
Abstract
Research examining how psychological and relational experiences differ between parents of dependent children living with curable or incurable cancer is limited. This study presents a secondary analysis of longitudinal data examining the impact of cancer on mental health and relational wellbeing of parents with dependent children. Participants’ free-text responses were analyzed using a convergent mixed-methods design. Qualitative content analysis identified three categories, which were coded as present or absent for each participant: The emotional and personal burden of cancer, Impact of cancer on families, couples, and social relationships, and The role of healthcare in supporting or undermining well-being. Category frequencies were statistically compared between parents with curable and incurable cancer. Psychological and relational experiences were similar across groups, particularly regarding emotional, relational, and healthcare-related challenges. These findings suggest that such challenges may be shaped more by parental role, life context, and access to systemic support than by disease curability.
Keywords
Introduction
A cancer diagnosis is a life-altering event that often brings significant physical and psychological challenges, not only for the individual but also for their close relationships and family (Arès et al., 2014; Borstelmann et al., 2022). For parents with dependent children, cancer is experienced not only in their role as patients but also in their role as caregivers, as these challenges are amplified by the dual responsibility of caregiving and managing the uncertainties of illness and treatment (Romare Strandh et al., 2025). In this context, cancer may threaten parents’ ability to fulfill parental roles and to protect their children’s emotional and practical needs.
Symptoms such as anxiety and depression are prevalent among cancer patients and may persist even after treatment ends (Erdoğan Yüce et al., 2021). Elevated parenting concerns (Romare Strandh et al., 2024), alongside factors such as female gender, older age, high symptom burden (Erdoğan Yüce et al., 2021), and financial worries (Dee et al., 2021) contribute to psychological distress. These findings suggest that psychological distress in cancer is shaped not only by medical factors, but also by social roles and responsibilities, including parenthood. In a previous study of individuals with early-stage cancer, approximately 42% reported clinically significant psychological distress (Lu et al., 2025). In this group, low social support and being aged 40–59 were associated with depression, while having children was related to higher levels of both anxiety and depression (Johannsen et al., 2022; Lan et al., 2022). In another study, approximately 41% of palliative care patients also experienced emotional distress (Pérez-Cruz et al., 2025). Among individuals with advanced cancer, religious beliefs and financial hardship are associated with increased levels of depression, while higher educational attainment and continued employment relate to elevated anxiety symptoms. In this population, death anxiety frequently coexists with depression, anxiety, and a greater symptom burden (Su et al., 2022). Taken together, these findings indicate that psychological distress in cancer patients may vary according to illness stage and personal circumstances, such as caring for dependent children.
The impact of cancer frequently extends to the family, disrupting routines, shifting roles, and affecting emotional well-being over time (Coyne et al., 2020; Perak et al., 2024). Partners of parents with cancer often report high levels of depression and anxiety symptoms (Borstelmann et al., 2022), while children may exhibit declines in well-being and behavioral changes (Romare Strandh et al., 2025). For parents, concerns about their children’s emotional security, development, and long-term adjustment may constitute a source of distress, particularly when illness compromises parental availability. For instance, despite efforts to maintain a sense of normalcy and present a posture of strength, parents with advanced cancer often express concerns about the effect of their illness on family functioning and the co-parent’s ability to provide both practical and emotional support, particularly for the children (Caparso et al., 2023).
Couple relationships may also be affected by cancer (Borstelmann et al., 2022). Contributors to relationship strain and dissolution include elevated partner anxiety and lower relationship satisfaction (Nalbant et al., 2021). Physical changes due to cancer and its treatment can negatively impact sexual functioning (Sousa Rodrigues Guedes et al., 2022), sexual identity, body image, and self-confidence (Olesen et al., 2023). Commonly reported cancer-related sexual dysfunctions include dyspareunia, reduced desire, and difficulties with arousal and orgasm (Ljungman et al., 2018, 2019; Olesen et al., 2023; Wettergren et al., 2022). Because couple relationships may serve as emotional and practical resources for parents with dependent children, disruptions in intimacy and relationship functioning may undermine individual psychological well-being and strain family dynamics. While fertility-related concerns and treatments may create emotional and sexual intimacy strains, in some instances, facing these challenges together can strengthen the couple’s bond and foster relationship growth (Hawkey et al., 2021).
Cancer encompasses a broad range of diagnoses, with prognosis varying among different cancer types (Wang et al., 2019). A commonly accepted clinical standard for considering cancer cured is the achievement of complete remission lasting 5 years (Wang et al., 2019). However, prolonged survival rates are becoming increasingly common among patients with incurable cancer, defined as no longer treatable with curative intent, leading many to live extended periods with the disease (Stegmann et al., 2021). From a conceptual standpoint, prognosis may represent a critical marker that shapes expectations regarding survival, future planning, and perceived continuity of life roles, including parenthood. Over half of caregivers hold misconceptions about the likelihood of cure for the patient (Gray et al., 2021). Accurate prognostic awareness in patients with advanced and incurable cancer has been associated with greater emotional distress (Arai et al., 2021; Pérez-Cruz et al., 2025), and around one-fifth believe their illness is curable despite its incurable nature. Patients who acknowledge and accept their incurable prognosis also tend to experience a stronger sense of being a burden to others compared to those with inaccurate prognostic awareness (Tang et al., 2016).
Individuals with cancer report unmet needs, in particular regarding psychological domains (Erdoğan Yüce et al., 2021). While psychosocial support is frequently perceived as most beneficial immediately following diagnosis, many continue to face emotionally overwhelming cycles of surviving and confronting mortality throughout the illness (Buiting et al., 2019). Although well-being is a multidimensional construct, it is commonly understood to encompass emotional, relational, and existential dimensions, all of which may be challenged by cancer and its prognosis (World Health Organization, 2021). Despite increasing attention to the psychosocial challenges of living with cancer, there is limited research examining how psychological and relational experiences differ among parents depending on whether their cancer status is considered curable or incurable. Given the specific responsibilities, future-oriented concerns, and relational contexts associated with parenthood, this distinction warrants special attention. Therefore, the aim of this study was to explore how parents with cancer experience their psychological and relational well-being, in relation to whether their cancer was described as curable or incurable.
Material and methods
Study design
This study employed a convergent mixed-methods design, using data from a longitudinal study conducted between 2023 and 2024. The present study represents a secondary analysis of data from this longitudinal dataset, the overall aim of which was to investigate how cancer impacts the mental health and relational aspects of parents with cancer who have dependent children (Romare Strandh et al., 2024).
In the convergent design, qualitative and quantitative data were collected simultaneously from the same sample, analyzed separately, and then integrated to provide a comprehensive understanding of the psychological and relational well-being among parents with either curable or incurable cancer. The study protocol was approved by the Swedish Ethical Review Board (Reference number: 2022-03088-01), and the reporting adheres to the GRAMMS guidelines for mixed-methods research (O'Cathain et al., 2008).
Participants and recruitment
Participants were recruited through social media advertisements, patient organizations, and posters displayed in oncology clinics across Sweden. Detailed information about the recruitment process has been published elsewhere (Romare Strandh et al., 2024). Inclusion criteria were being aged between 25 and 60 years, having been diagnosed with any type of cancer in the past 5 years at the time of enrollment, and having at least one child aged 18 years or younger. For this specific study, only participants who self-reported their current cancer status (curable or incurable) and provided responses to the open-ended questions about psychological and relational experiences were included. Curability was intentionally conceptualized from the patient’s subjective perspective, as our primary interest was in how individuals understand and make sense of their illness rather than in medical prognosis per se.
Data collection
Data were collected via online surveys accessible through the project website and managed using REDCap electronic data capture tools (Harris et al., 2019). Detailed information about the study and the research team was available on the project website. Data collection occurred at two time points: at inclusion (T1) and 1 year after inclusion (T2). However, the present analyses focus on cross-sectional patterns in parents’ experiences rather than on temporal change. Participants received a gift voucher upon completing the survey at each time-point (equivalent to approximately 21 USD).
At T1, participants provided background information including socio-demographics (e.g. gender, age, educational level, relationship status and duration, number of children, and age of the youngest child), and health-related information such as cancer status (curable or incurable), time since diagnosis (years), cancer diagnosis, and perceived need for support during the cancer trajectory (individual support and couple support during the cancer trajectory). For participants who had not provided information about cancer status at T1 but did so at T2, the T2 response was used (n = 21). Cancer status reported at T1 and T2 was also compared to assess any changes over time.
Self-rated health was collected assessed using a single item: “How would you rate your general health?,” with five response options ranging from very good to very poor. Following prior research, responses were dichotomized as good (good and very good) or poor self-rated health (neither good nor poor, poor, and very poor; Roelsgaard et al., 2016). Before responding to open-ended questions on experiences of psychological and relational well-being, participants were asked about their perceived need for support (“Have you experienced a need for support for your mental well-being after being diagnosed with cancer?” and “Have you experienced a need for support for your couple relationship after being diagnosed with cancer?”). Response options were Yes, Partially, and No. For analysis, Yes and Partially were combined and categorized as Yes.
Qualitative data consisted of free-text written responses to two open-ended questions: “Is there anything else you would like to tell us about your mental health and need for support in relation to the cancer illness?” and “Is there anything more you would like to tell us about your couple relationship in relation to the cancer illness?.” These study-specific items were intended to capture participants’ experiences and aspects of psychological and relational well-being that may not be fully represented by structured questionnaire items, allowing parents with cancer to elaborate on issues of personal relevance. These questions were asked at both T1 and T2, resulting in a total of four questions per participant (two at each time point). To enhance the breadth of the material and maximize inclusion, responses from both T1 and T2 were compiled and analyzed together. If a participant responded to the same question at both time points, both responses were included. Participants who were not in a relationship at the time of the surveys were still eligible to respond to questions concerning psychological well-being. This approach allowed the inclusion of participants who responded at only one time-point and/or were single parents, consistent with the study aim of exploring the experiences of parents with cancer rather than changes over time.
Each free-text field allowed for responses up to 65,535 characters. The length of responses varied considerably, ranging from brief statements of a few words to extended narratives spanning several sentences.
Data analysis
Descriptive statistics were used to summarize participant characteristics (socio-demographic and health-related characteristics, and needs for support) and are reported as median and interquartile range (IQR) or count (n) and percentages (%). Group differences between participants with curable versus incurable cancer were analyzed using Chi-Square test or Mann-Whitney’s test, depending on the type of variable. No statistical testing was performed for subcategories with small group sizes.
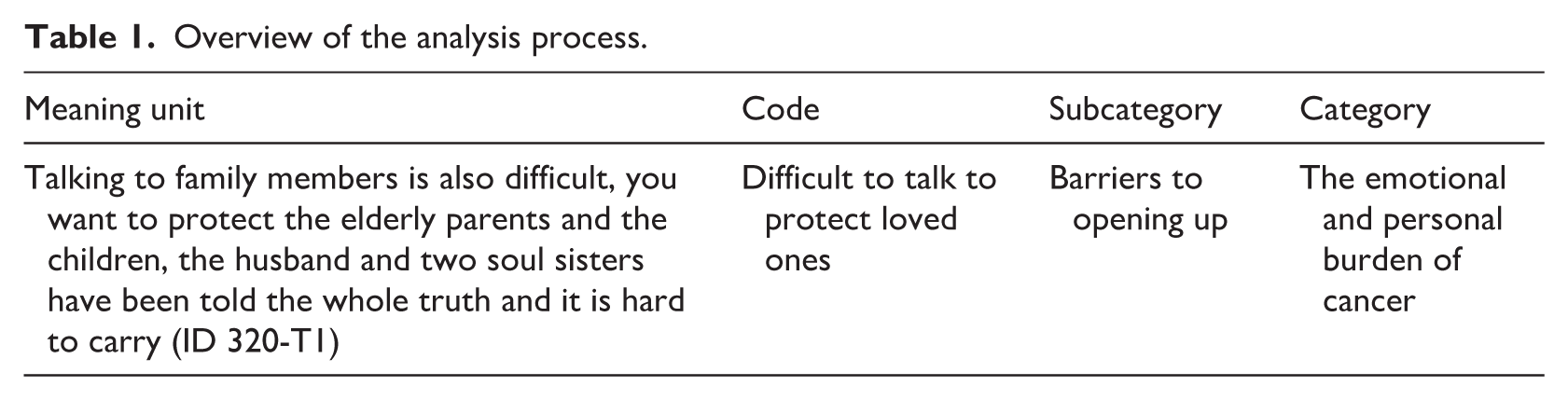
A qualitative content analysis (Lindgren et al., 2020) was conducted to explore participants’ experiences of psychological and relational well-being in the context of cancer. All free-text responses were compiled into a single unit of analysis. Meaning units were identified and, when appropriate, condensed. These were then coded using a manifest content approach, focusing on the explicit content of the text without deeper interpretation. The qualitative analysis was descriptive in nature and aimed to identify shared patterns in reported experiences, rather than provide an in-depth interpretative analysis of meaning. All responses were included in the qualitative analysis regardless of length. Shorter responses were treated as meaningful but limited expressions of participants’ experiences, while longer responses provided greater contextual detail. Codes were organized into subcategories based on similarities in content. Related subcategories were grouped into broader categories, representing a higher level of interpretation. Initial coding was performed by the first author and validated by the second author. The development of subcategories and categories was also reviewed collaboratively by the final two authors. Subcategories and categories were identified based on patterns across responses rather than the length or depth of individual contributions. Any disagreements were resolved through discussion until consensus was reached. An overview of the analysis process is illustrated in Table 1.
Overview of the analysis process.
In the mixed methods analysis, the first step involved data transformation (Creswell and Clark, 2017), where qualitative data from both T1 and T2 were merged and treated as a single unit of analysis per participant. These qualitative data were then transformed into numerical form to enable subsequent quantitative analyses. Codes in each subcategory and category was then quantified using binary coding, indicating whether it was present or absent for each participant, regardless of whether it appeared at T1, T2, or both. Thus, participants were only counted once per code, and not multiple times based on frequency. Frequencies of subcategories and categories were then stratified between participants with curable and incurable cancer. The qualitative findings were not only used as input for the data transformation but also served an interpretive function within the mixed methods design. While the qualitative analysis identified content and meaning of parents’ experiences, the quantitative analyses examined whether these qualitatively derived experiences differed by cancer status.
Three participants were excluded from this analysis due to inconsistencies in their self-reported cancer status between T1 and T2. Group differences at category level were analyzed using Chi-square tests. However, due to the small group sizes within certain subcategories, those comparisons are presented descriptively only. All statistical analyses were conducted using IBM SPSS Statistics version 28.0 (IBM Corp., Armonk, N.Y., USA).
Results
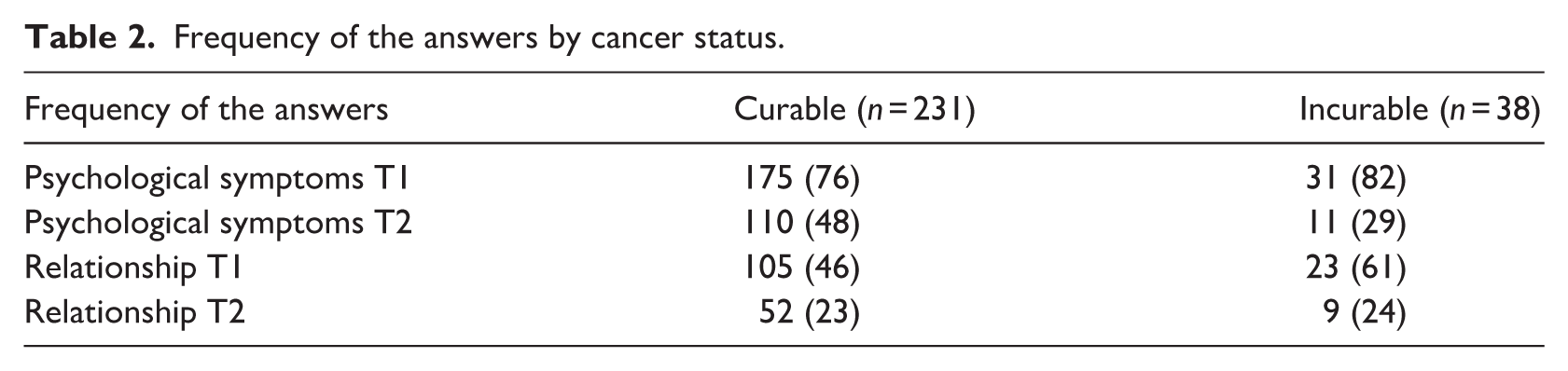
Of 406 participants who enrolled in the study, 269 (66%) responded to at least one of the open-ended questions at either T1 or T2 and were included in the analyses (Table 2). Among these, 231 (85%) had curable cancer and 38 (14%) had incurable cancer. The majority of participants were mothers (96%), had a post-secondary education (87%), and were in a partnered relationship (83%). The most common type of cancer was breast cancer (70%), followed by pelvic cancer (15%). Approximately half of the participants rated their health as good. The only statistically significant difference between participants with curable and incurable cancer in terms of sociodemographic or health-related characteristics was the perceived need for couple support (p = 0.02), with a higher proportion of participants with incurable cancer reporting a need for such support. A detailed overview of participant characteristics is presented in Table 3.
Frequency of the answers by cancer status.
Participant characteristics at inclusion by cancer status.
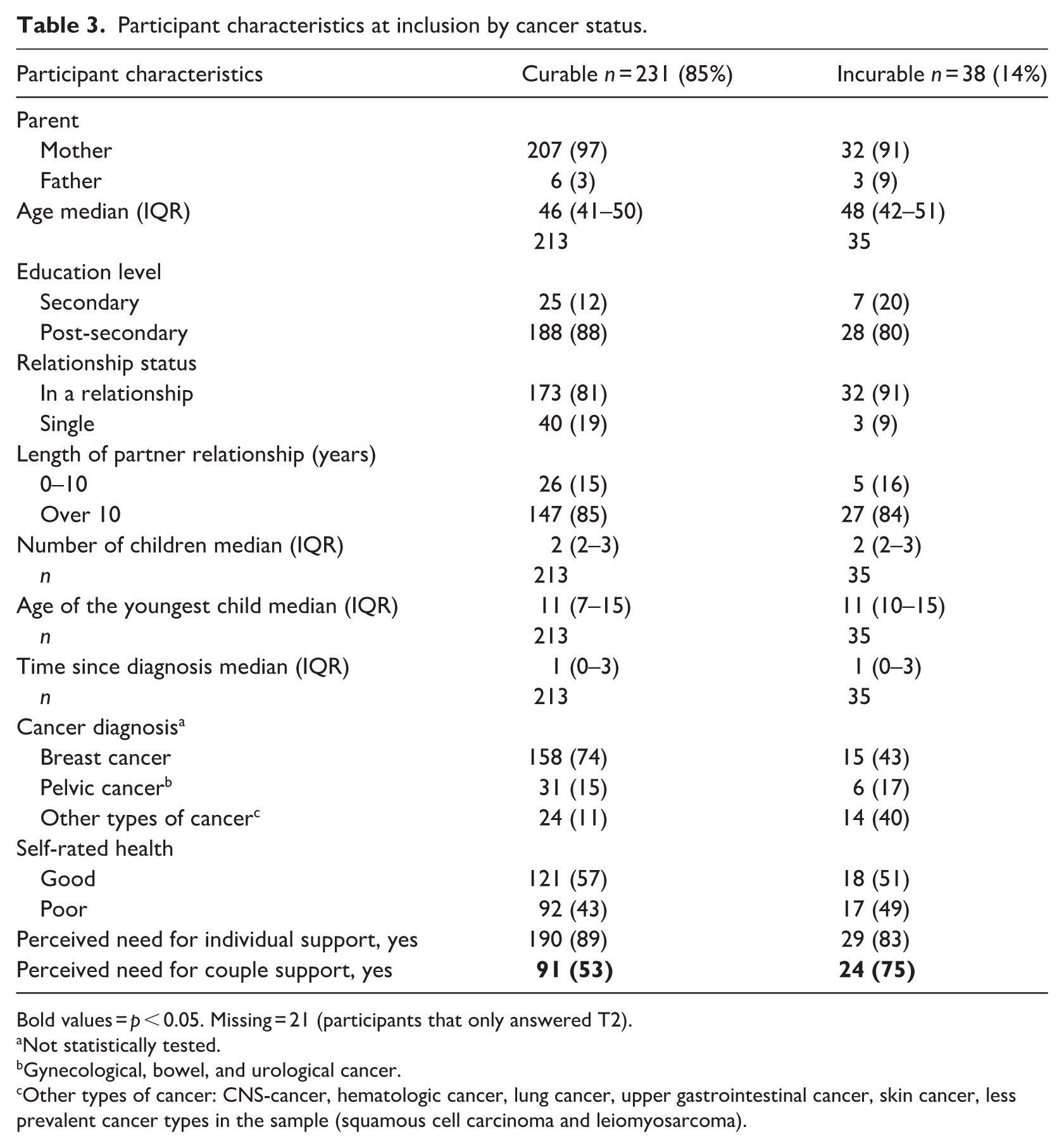
Bold values = p < 0.05. Missing = 21 (participants that only answered T2).
Not statistically tested.
Gynecological, bowel, and urological cancer.
Other types of cancer: CNS-cancer, hematologic cancer, lung cancer, upper gastrointestinal cancer, skin cancer, less prevalent cancer types in the sample (squamous cell carcinoma and leiomyosarcoma).
Qualitative analysis
The qualitative content analysis resulted in three categories: The emotional and personal burden of cancer; Impact of cancer on families, couples, and social relationships; and The role of healthcare in supporting or undermining well-being. A summary of the subcategories, categories and illustrative participant quotes are presented in Table 4.
Subcategories, categories, and quotes from the participants.
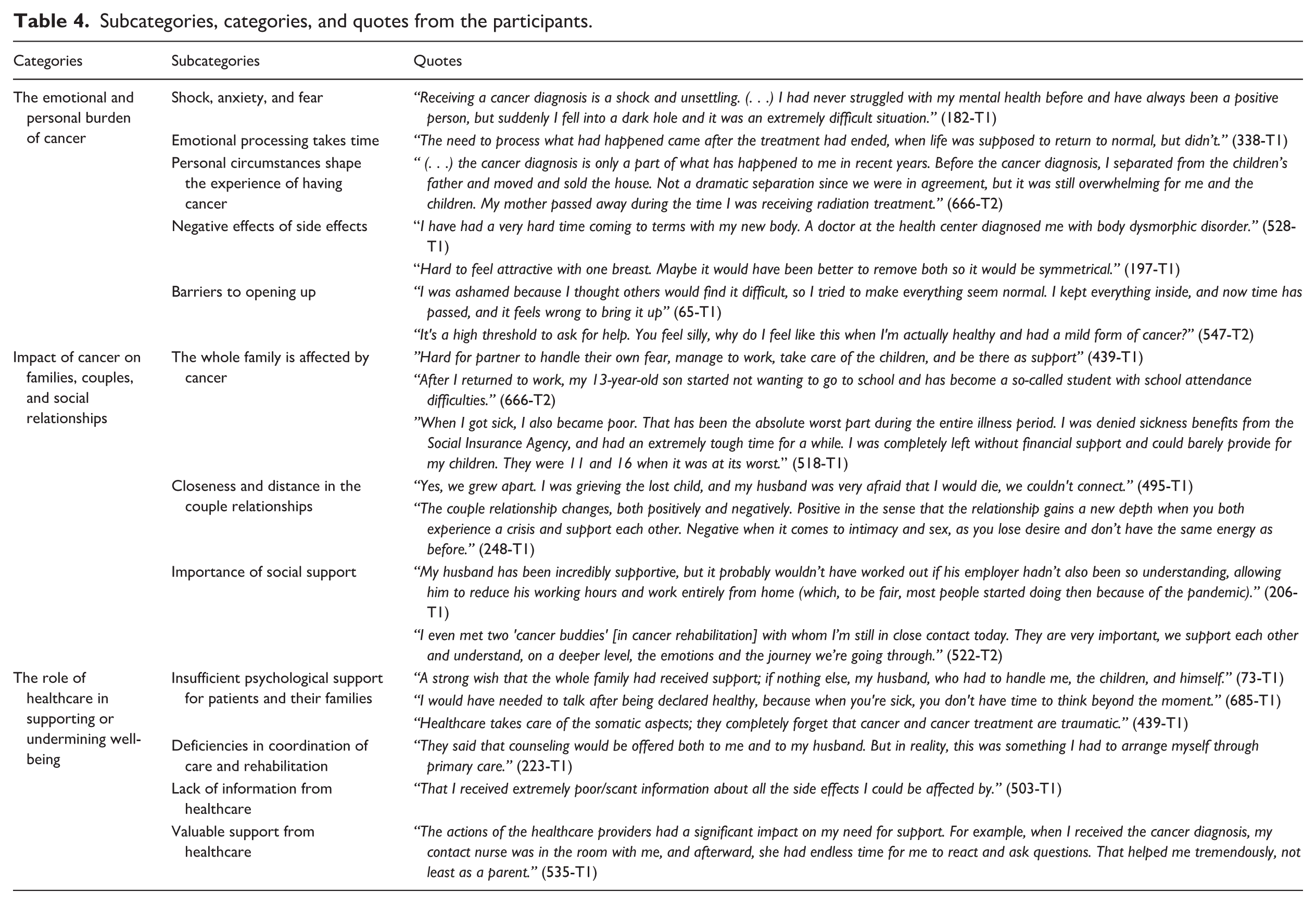
The category The emotional and personal burden of cancer includes parents’ experiences of how cancer affected them on an individual level. This category consists of five subcategories “Shock, anxiety, and fear,” “Emotional processing takes time,” “Personal circumstances shape the experience of having cancer,” “Negative effects of side effects,” and “Barriers to opening up.” Parents described feeling shocked and fearful upon receiving the diagnosis. Parents also expressed that the psychological impact of cancer persisted long after treatment had ended or surfaced later in the illness trajectory. Personal life circumstances, such as bereavement, relationship dissolution, or concurrent stressors, were described as influencing parents’ coping and psychological well-being. Physical side effects, including changes in the body, body image, cognitive functioning, and sexuality were also reported as negatively affecting well-being and, for some, their intimate relationships. Some also noted difficulties in expressing their emotions or seeking support, even when experiencing emotional distress. Barriers to opening up included difficulties in asking for help and a wish not to burden loved ones.
The category Impact of cancer on families, couples, and social relationships reflects the effects of cancer on family members, couple relationships, and the importance of social support throughout the cancer journey. This category comprises three subcategories: “The whole family is affected by cancer,” “Closeness and distance in the couple relationships,” and “Importance of social support.” Parents described the toll cancer took on their children and partner, sometimes accompanied by financial concerns. Changes in family roles and dynamics were also reported and many prioritized the needs of their children. Parents indicated that their couple relationship was negatively affected, particularly in the presence of pre-existing issues. Relationship difficulties emerged when roles shifted, with some expressing feelings of being a burden or not feeling understood, for example, regarding fatigue. They reported reduced sexual activity, emotional disconnection, and grief over changes in their intimate lives. Some noted that their relationship had been deprioritized and experienced more frequent conflicts. Despite the challenges of cancer, some parents shared that their relationships had strengthened following the diagnosis. The importance of receiving social support from partners, family, and friends was consistently emphasized. Feelings of loneliness were reported when such support was lacking, while connecting with others who had lived experience of cancer was also highlighted as especially valuable.
The category The role of healthcare in supporting or undermining well-being illustrates how the quality and availability of the healthcare services influenced parents’ during and after cancer treatment. This category includes four subcategories: “Insufficient psychological support for patients and their families,” “Deficiencies in coordination of care and rehabilitation,” “Lack of information from healthcare,” and “Valuable support from healthcare.” Parents reported that healthcare services did not adequately address their individual or family needs, particularly with regard to psychological support. They perceived the healthcare system as being primarily focused on medical treatment, often overlooking the emotional aspects of living with cancer. Access to psychological services was described as inconsistent and limited by geographical disparities, resulting in unequal availability of care. Parents also reported deficiencies in the coordination of care and rehabilitation, which created barriers to accessing appropriate support. While some parents received useful information, for example about side effects of cancer treatment, long-term consequences, fertility, and how to access psychological or rehabilitation services, others reported receiving little or no information from healthcare providers. Despite these shortcomings, many parents shared that when support was available, interactions with healthcare professionals were meaningful and had a positive impact on their well-being.
Mixed-method analysis
In the mixed methods analysis, a greater proportion of participants with curable cancer were represented in the category The emotional and personal burden of cancer, although this difference was only bordering statistically significant (p = 0.08). No significant group differences were found in the analyzed subcategories within this category (Shock, anxiety, and fear and Personal circumstances shape the experience of having cancer). Similarly, no statistically significant differences were observed between the curable and incurable cancer groups in the categories Impact of cancer on families, couples, and social relationships (p = 0.28) or The role of healthcare in supporting or undermining well-being (p = 0.23). No group differences were found in the subcategories under the category Impact of cancer on families, couples and social relationships, or in the subcategory Insufficient psychological support for patients and their families under the category The role of healthcare in supporting or undermining well-being (Table 5).
Categories and subcategories derived from qualitative content analysis and by cancer status.
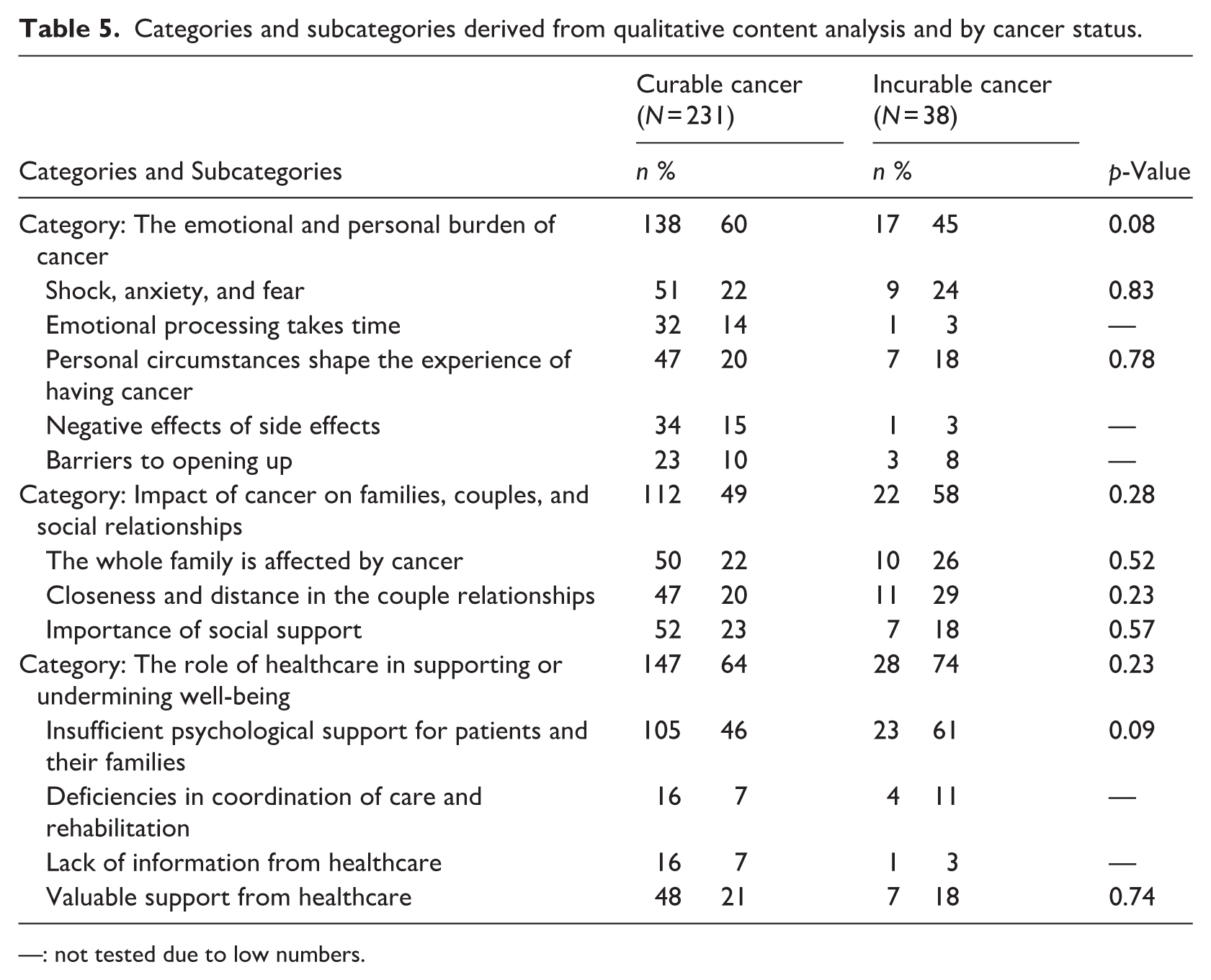
—: not tested due to low numbers.
Discussion
This study explored how parents with cancer experience their psychological and relational well-being, with particular focus on whether these experiences differ based on cancer status (curable vs incurable). The mixed methods analysis revealed no statistically significant differences between groups across the three categories: The emotional and personal burden of cancer, Impact of cancer on families, couples, and social relationships, and The role of healthcare in supporting or undermining well-being. While the mixed-methods analysis included statistical comparisons between parents with curable and incurable cancer, these analyses examined differences in the prevalence of qualitatively derived categories rather than differences in how parents made sense of these experiences. The absence of significant group differences does not imply that parents with curable and incurable cancer have identical experiences. Rather, the findings suggest that similar challenges may arise across cancer trajectories, and that psychological and relational challenges may be shaped more by their role as parents and partners, life context, and systemic support than by cancer status alone.
Parents described emotionally challenging experiences, reflecting the personal and relational burden of cancer, and aligning with previous research on its psychological impact (Erdoğan Yüce et al., 2021; Rainbird et al., 2009). These experiences highlight how emotional well-being may be influenced by parenting-related responsibilities and life-context, rather that curability status alone. Some parents with curable cancer noted that these challenges intensified after the end of treatment, a period often marked by reduced clinical contact and limited psychosocial support. Our findings are in line with previous research indicating that emotional vulnerability can persist or increase after treatment, depending on baseline distress and individual coping resources (Cook et al., 2018; Lotfi-Jam et al., 2019). For some, this period may represent a turning point, where attention shifts from physical survival to processing the emotional impact of the illness. Within the parenting context, the emotional distress may be influenced by contextual and personal factors, such as role demands and responsibility for others rather than the cancer status alone.
The present results indicate that parents viewed cancer not only as a personal health crisis but as a shared family experience. They emphasized the impact on children, partner, and household dynamics. Previous research has shown that adaptive family communication, emotional openness, cohesion, and effective conflict resolution serve as protective factors in families of patients with advanced cancer (Chen et al., 2022). While the threat of loss may be more immediate for those with incurable cancer, the uncertainty, role changes, and emotional demands faced by parents with cancer suggest the importance identifying families at risk of emotional distress, regardless of curability status.
Experiences within couple relationships were mixed: while some described strengthened emotional bond, others reported increased tension and emotional distancing. These findings are consistent with research showing that cancer can lead to either increased intimacy or heightened anxiety within partnerships (Valente et al., 2021). Avoidance of emotional topics, in particular, has been associated with poorer psychological outcomes among couples managing illness and parenting responsibilities (Valente et al., 2021; Wikman et al., 2025). Physical decline and changes in sexual function have also been identified as additional stressors, especially among those with incurable cancer (Loughan et al., 2022). Nonetheless, in some cases, increased dependence on loved ones may deepen bonds with partners and children (Loughan et al., 2022). Taken together with earlier research, our findings suggest that interventions should support families with open communication and acknowledge both the emotional, physical and relational toll of illness, to promote better adaptive strategies and relational well-being (Coyne et al., 2020).
Social support emerged as a central across both groups. Many parents emphasized the value of connecting with others facing similar experiences, consistent with previous research showing that approximately one-third of patients with non-advanced cancer seek peer support (Ferrari et al., 2019). In our findings, no differences were found between participants with curable and incurable cancer. While social support cannot eliminate all challenges, it may provide emotional and practical resources for everyday life (Perak et al., 2024), potentially serving as a stabilizing factor for parents with cancer, regardless of cancer status.
Parents within both groups described similar concerns regarding healthcare interactions, highlighting the role of healthcare in shaping emotional well-being. Some perceived a narrow focus on medical treatments, with insufficient attention to psychological and relational needs. This finding aligns with previous results showing that disengaged healthcare encounters can exacerbate feelings of hopelessness and emotional distress among cancer patients (Meggiolaro et al., 2016). Geographic disparities were also noted, with some participants reporting limited access to psychological services depending on their location. While geography alone may not determine distress levels, it can create logistical barriers that exacerbate that compound emotional burden (Loughan et al., 2022; Watts et al., 2016). Our results point to the importance of accessible care that acknowledges parents’ psychological and relational needs across the cancer trajectory, regardless of cancer status.
Clinical implications
Parenting while living with cancer introduces unique challenges that may transcend distinctions between curable and incurable disease. The shared call for improved access to psychological support, both during and after treatment, points to the need for family-centered care models that address the specific needs of parents with cancer. Integrating early screening for psychological distress and relationship difficulties into routine care may help identify need of additional support, prevent long-term emotional suffering and promote overall well-being.
Strengths and limitations
The mixed-method design applied in this study allowed for the exploration of psychological and relational well-being among parents with curable and incurable cancer. Focusing on parents with cancer enhanced the relevance and credibility of the findings for this specific population. The large sample size and the involvement of multiple researchers with theoretical and clinical experiences, are also strengths (Graneheim et al., 2017). However, a number of limitations must be acknowledged. The sample was predominantly composed of highly educated mothers with breast cancer in long-term partnered relationships, fluent in Swedish, which limits transferability to fathers, other cancer diagnoses, single parents, and those from diverse cultural or socioeconomic backgrounds. Accordingly, the findings primarily reflect mothers’ experiences, and conclusions should be interpreted with caution when considering fathers with cancer. Additionally, cancer status was self-reported, introducing the possibility of misclassification. For example, some participants on long-term hormonal therapy may have self-identified as having incurable cancer, despite their condition not being immediately life-limiting. Research suggests that nearly one-fifth of patients with incurable cancer misunderstand their treatment intent, which is also associated with higher levels of anxiety (El-Jawahri et al., 2020). Because the present study focused on participants’ experiences of psychological and relational outcomes, the subjective understanding of their illness was considered particularly relevant, as such perceptions may shape emotional responses and coping processes. Such variation in illness perception may partly explain the lack of observed differences between groups.
The survey did not include child-reported outcomes, and children’s experiences were therefore not directly assessed. However, the focus of the present study was on parents’ experiences of living with cancer while caring for dependent children. Parenting context was captured through demographic and clinical variables and through qualitative data reflecting parents’ perspectives of how cancer affected family life and parenting.
The order of survey questions may also have influenced responses. Participants answered items on perceived support needs before reflecting on psychological and relational well-being, which could have shaped their responses. As qualitative data were collected through open-ended questions embedded in a broader survey, this method may have limited the depth of responses. Nonetheless, the absence of an interviewer may have reduced social desirability bias and enhanced the authenticity of the responses. The optional nature of the questions likely empowered participants to share on their own terms, further contributing to the authenticity of the material. However, the small sample size in certain subcategories limited the feasibility of group comparisons at that level. A larger sample might have revealed more nuanced differences between curable and incurable cancer groups.
Conclusion
The psychological and relational experiences of cancer among parents with curable and incurable cancer appear to be similar, particularly in terms of emotional, relational, and healthcare-related challenges. This study highlights a need for equally attentive psychosocial care across the cancer continuum. Support should be tailored to individual emotional needs and family situations, regardless of whether the cancer is curable or incurable. Future studies should explore the experiences of younger parents, single parents, fathers with cancer, broader sample of diagnoses, and individuals from underrepresented cultural and healthcare contexts.
Footnotes
Acknowledgements
The authors would like to thank all participants for their valuable time and contribution to this study.
Ethical considerations
The study protocol was approved by the Swedish Ethical Review Board (Reference number: 2022-03088-01).
Consent to participate
All participants received written information about the study and provided written informed consent prior to participation.
Consent for publication
The written informed consent, provided by all participants, confirms consent to publish.
Author contributions
AHE: Formal analysis, visualization, writing – original draft; AMG: Formal analysis, Writing – review and editing, MRS: Data collection, writing – review and editing; AK, KS, FV, RE: Writing – review and editing; LL: Conceptualization, methodology, formal analysis, writing – review and editing; AW: Conceptualization, methodology, formal analysis, writing – review and editing, supervision, project administration, funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Cancer Society [grant number 20 0824 Pj and 23 2632 Pj]; and the Swedish Research Council [grant number 2020-02080 and 2023-01950].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data cannot be shared publicly due to ethical restrictions and participant, confidentiality under Swedish regulations. Data are available from the principal, investigator, Prof. Anna Wikman (