
Abstract
This study examined associations between motives, self-regulation, and health behaviors and tested the factor structure of a healthy eating motives scale adapted from the Motives for Physical Activity Measure–Revised. Participants (N = 187) were primarily female (67%) and Caucasian, non-Hispanic (94%), with a mean age of 20.39 years (standard deviation (SD) = 1.58). Participants completed an online survey assessing physical activity, sedentary behavior, fruit and vegetable intake, and motivational constructs based on Self-Determination Theory (SDT). Exploratory factor analysis supported a four-factor structure for healthy eating motives (health, appearance, social, interest) with strong internal consistency. Multiple regression results showed intrinsic motives and autonomous regulation were positively associated with physical activity and vegetable intake and negatively associated with sedentary time. Cross-behavioral effects were limited, though autonomous regulation demonstrated consistent benefits across domains. Outcomes reinforce the importance of autonomous motivation in promoting health behaviors and provide psychometric support for an SDT-based measure of dietary motives.
Keywords
Introduction
Physical activity improves health (Mahindru et al., 2023), yet over 25% of U.S. adults are inactive and most spend one-third of time sedentary (Centers for Disease Control and Prevention [CDC], 2025; Matthews et al., 2021). Sedentary behavior independently harms health, even among active individuals (Young et al., 2016). Adequate fruit and vegetable intake reduces chronic disease and mortality (Aune et al., 2017). Health behaviors established during young adulthood persist with long-term disease implications. Promoting multiple health behaviors together supports lasting changes in physical activity, sedentary behavior, and diet (Geller et al., 2017). This study examined university undergraduates during this critical period.
The self-determination theory (SDT) distinguishes young adults’ motives to maintain a healthy lifestyle between intrinsic motives (inherent enjoyment or personal value) and extrinsic motives (external pressure and/or reward; Deci and Ryan, 2000). Among young adults, research consistently shows that intrinsic motives foster autonomy, supporting ongoing adherence to workouts and nutritious diets (Teixeira et al., 2012). Conversely, extrinsic motivators, such as appearance or social reward, may spark initial compliance but are difficult to sustain and eventually diminish in effectiveness (Teixeira et al., 2012). SDT-based interventions build intrinsic motivation, supporting long-term healthy behaviors in young adults (Ryan and Deci, 2017). Despite robust SDT research, motivational consistency across multiple health behaviors remains poorly understood.
SDT distinguishes autonomous self-regulation (personally valued, intrinsic) from controlled self-regulation (external, guilt-driven; Deci and Ryan, 2000). Autonomous motivation supports sustained adherence to healthy lifestyle behaviors (Hagger et al., 2014), while controlled motivation undermines maintenance (Maillet and Grouzet, 2022; Teixeira et al., 2012). Fostering autonomous motivation is critical for lasting change (Ntoumanis et al., 2021). Few studies have compared autonomous versus controlled regulation across multiple health behaviors.
Two objectives guided this study: testing an adapted healthy eating motives measure and examining motivational associations across multiple health behaviors. Greater intrinsic motives and autonomous regulation were expected to associate with increased activity and fruit and vegetable intake, and decreased sedentary behavior (Hagger et al., 2014; Teixeira et al., 2012). Findings aim to clarify the influence of motivational and self-regulatory processes across multiple health behaviors, extending SDT beyond single-behavior models in young adults.
Methods and measurement
Young adults aged 18–25 attending a Midwestern university were recruited via email invitation to participate in a 10-minute anonymous online survey at their convenience. The study received ethical approval from the appropriate institutional review board, and participants gave informed consent prior to participation. Participants provided covariate information, including gender, age, ethnicity, height, weight, and perceived health status. Self-reported height and weight were used to calculate body mass index (BMI): (weight (lb)/height (in)2) × 703. Perceived health status was assessed using a single item on a five-point Likert scale (1 = Poor, 2 = Fair, 3 = Good, 4 = Very Good, 5 = Excellent).
Health behavior measurement
Physical activity was measured using the International Physical Activity Questionnaire (IPAQ; Craig et al., 2003), which assessed participants’ weekly minutes of moderate and vigorous physical activity. A single item assessed daily sedentary minutes spent on screen activities (TV, social media, video games). To evaluate fruit and vegetable consumption, participants were provided with standardized serving size definitions: a serving of vegetables was defined as 1 cup of raw, cooked, frozen, or canned vegetables; 2 cups of raw leafy salad greens; or 1 cup of 100% vegetable juice. A serving of fruit was defined as 1 cup of fresh, frozen, or canned fruit; ½ cup of dried fruit; or 1 cup of 100% fruit juice (U.S. Department of Agriculture, n.d.). Participants then reported their typical daily servings of fruits and vegetables.
Motives for health behavior
Participants’ motivations for engaging in health-promoting behaviors were assessed using two instruments grounded in SDT. Physical activity motives were evaluated with the Motives for Physical Activity Measure-Revised (MPAM-R), a 30-item questionnaire that examines 5 dimensions: enjoyment, competence, appearance, fitness/health, and social motives. Each item is rated on a seven-point Likert scale ranging from 1 (Not at all true for me) to 7 (Very true for me; Ryan et al., 1997). The MPAM-R has demonstrated robust validity across diverse populations to understand motivational factors influencing physical activity participation (Gonçalves and Alchieri, 2010).
The MPAM-R was adapted for healthy eating by paraphrasing items to reference diet. Authors with SDT expertise developed items, which were reviewed with students and pilot tested (n = 10), resulting in minor revisions. The Motives for Eating a Healthy Diet scale measures individuals’ motivations for maintaining a healthy diet across the same five subscales: enjoyment, competence, appearance, fitness/health, and social motives. Participants indicate the extent to which each motive applies to their dietary habits using the same seven-point Likert scale (Ryan et al., 1997). Although this adaptation has been used in nutrition research to assess motivations for healthy eating across five domains (Trudeau et al., 1998), preliminary evaluation of the factor structure and psychometric properties is needed.
Self-regulation of health behavior
The Treatment Self-Regulation Questionnaire for Exercise (TSRQ) assessed participants’ self-regulation for exercise and eating behaviors. The TSRQ for Exercise (TSRQ-E) evaluated motivations related to maintaining regular physical activity, while the TSRQ for Diet (TSRQ-D) focused on sustaining a healthy diet. Fort both instruments, participants responded on a seven-point Likert scale, ranging from 1 (Not at all true) to 7 (Very true), with 4 representing “Somewhat true.” The TSRQ is designed to measure three types of motivational regulation: autonomous regulation, controlled regulation, and amotivation (Levesque et al., 2007).
Statistical analysis
Data were analyzed using IBM SPSS Statistics Version 29.0. Only complete data were included in analyses. SDT measurement scales were first evaluated for factorial validity and refined for optimal model fit using exploratory factor analysis (EFA) with principal axis factoring and oblimin rotation. Factor retention was determined using multiple criteria, including eigenvalues greater than 1.00 (Kaiser, 1961), item factor loadings ⩾0.40 on a single factor in the pattern matrix (Gorsuch, 1983), cumulative variance explained, and conceptual interpretability of the solution. Criterion validity was evaluated through gender differences and health behavior associations.
Descriptive statistics were calculated for the full sample and stratified by gender (male, female). Gender group comparisons evaluated criterion validity by assessing whether the motivational constructs differentiated groups in theoretically consistent ways. A one-way ANOVA tested group differences with 95% confidence. Single linear regressions assessed associations between observed covariates and health behaviors; those statistically significant at p < 0.05 were retained for subsequent models. Separate regression analyses examined each behavior and motivation. Physical activity motives and regulation related to activity and sedentary minutes, eating motives and regulation to fruit/vegetable servings. Cross-behavioral models tested between-behavior associations. Adjusted R2 indicated variance explained.
Results
Participants (N = 187) were primarily female (67.4%) and identified as Caucasian, non-Hispanic (94.1%). The mean age was 20.39 years (standard deviation (SD) = 1.58). Average self-reported perceived health was 3.81 (SD = 0.76) on a five-point scale, indicating ratings between “good” and “very good.” The mean BMI was 23.11 (SD = 3.56). Table 1 provides descriptive statistics and results of group comparisons. Gender differences emerged across several variables. Males reported significantly more weekly minutes of moderate and vigorous physical activity (ps < 0.01) and greater daily sedentary time (p < 0.05) than females. Compared to males, female participants reported stronger appearance and fitness motives for physical activity (ps < 0.05), as well as higher health, interest, and appearance motives for healthy eating (ps < 0.05). For healthy eating, females demonstrated greater autonomous self-regulation (p < 0.05) and lower amotivation (p < 0.01) compared to males.
Descriptive statistics and gender differences in behaviors, motives, and self-regulation.
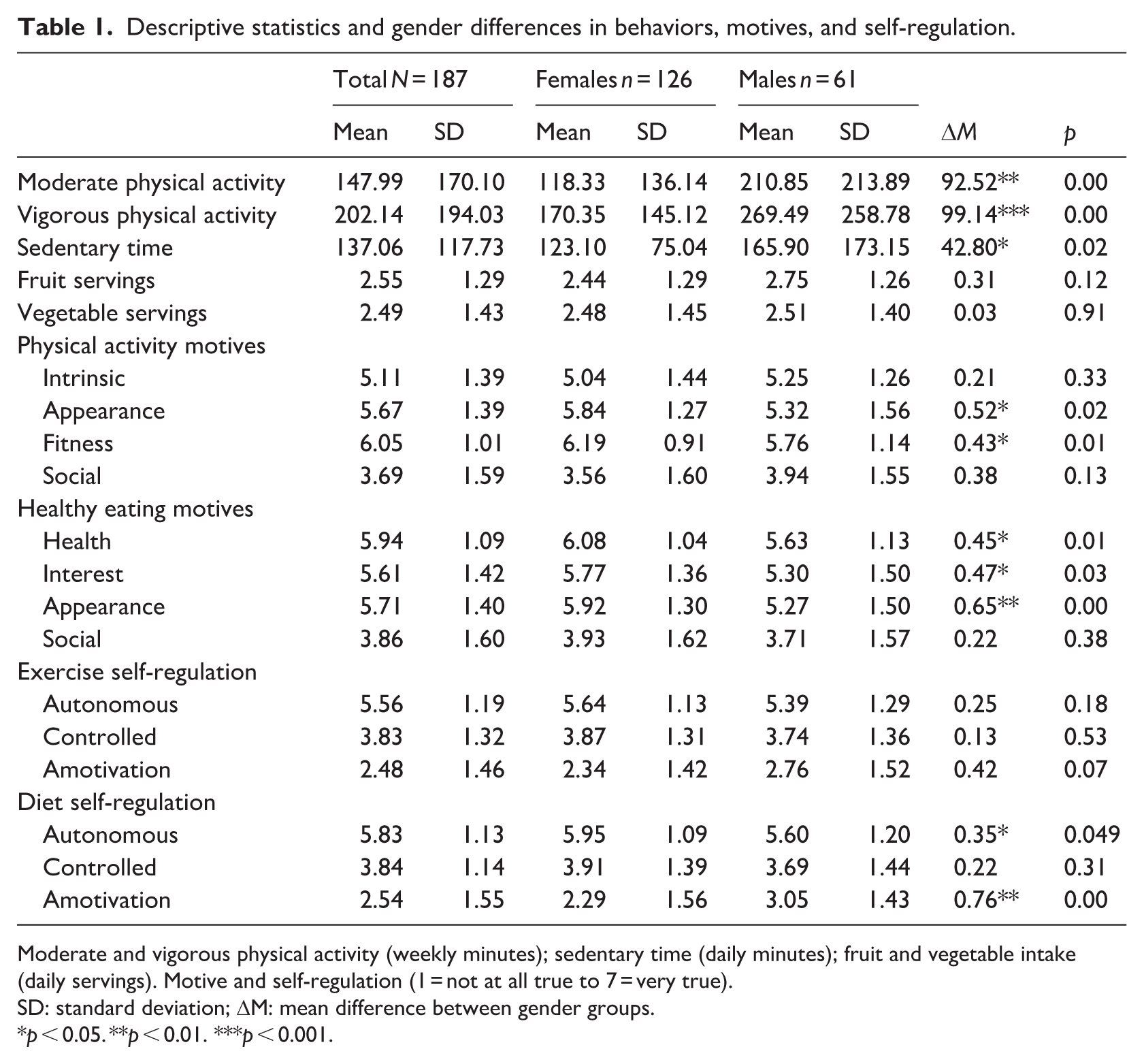
Moderate and vigorous physical activity (weekly minutes); sedentary time (daily minutes); fruit and vegetable intake (daily servings). Motive and self-regulation (1 = not at all true to 7 = very true).
SD: standard deviation; ΔM: mean difference between gender groups.
p < 0.05. **p < 0.01. ***p < 0.001.
Physical activity and healthy eating motives
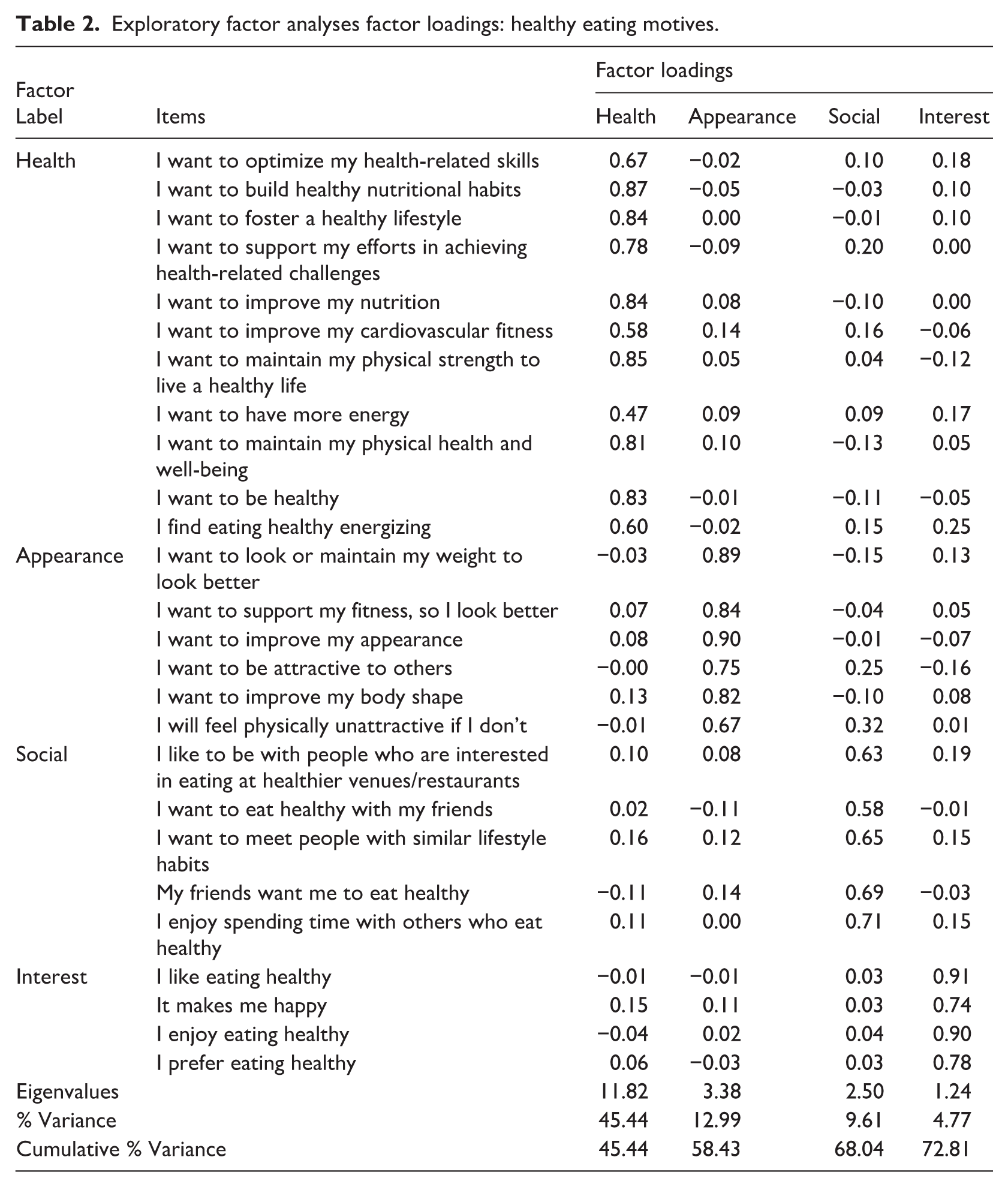
EFA revealed a four-factor structure for both physical activity and healthy eating behaviors, differing from the theoretical five-factor model (Ryan et al., 1997). Intrinsic items loaded onto a single factor, reflecting shared variance in pursuing physical activity for enjoyment and personal interest. The physical activity motives model accounted for 70.87% of variance, with factors: intrinsic (14-items, α = 0.96), appearance (6-items, α = 0.93), fitness (5-items, α = 0.88), and social (5-items, α = 0.93). Inter-factor correlations ranged from r = 0.03 to 0.51. All 30-items had strong and exclusive loadings (pattern coefficients >0.40). The healthy eating motives model explained 72.81% of variance, comprising: health (11-items, α = 0.95), appearance (6-items, α = 0.93), social (5-items, α = 0.84), and interest (4-items, α = 0.93), with inter-factor correlations from r = 0.16 to 0.63. Table 2 presents the EFA results for the valid measurement model, including all measurement items.
Exploratory factor analyses factor loadings: healthy eating motives.
Treatment self-regulation questionnaire for exercise (TSRQ-E) and diet (TSRQ-D)
EFA revealed a three-factor solution for both the TSRQ-E and TSRQ-D measurement models (eigenvalues > 1.00), encompassing autonomous, controlled, and amotivation regulation factors. The TSRQ-E model explained 63.73% of the variance, with factor correlations ranging from r = −0.13 to r = −0.48. The TSRQ-D model accounted for 68.14% of the variance, with factor correlations between r = −0.10 and r = −0.45. Both models retained all six original items for autonomous and controlled regulation factors (pattern coefficients > 0.40; α = 0.81–0.91). One amotivation item was removed from both scales due to low and cross-loadings (“It is easier to do what I am told than think about it”). The revised amotivation factor retained two items, explaining an additional 8.84% (TSRQ-E) and 9.53% (TSRQ-D) of the variance, with acceptable internal consistency (α = 0.60 and α = 0.74).
Multiple linear regression
Multiple regression models are presented in Table 3. Only significant results are reported.
Motives, self-regulation, and multiple health behaviors.
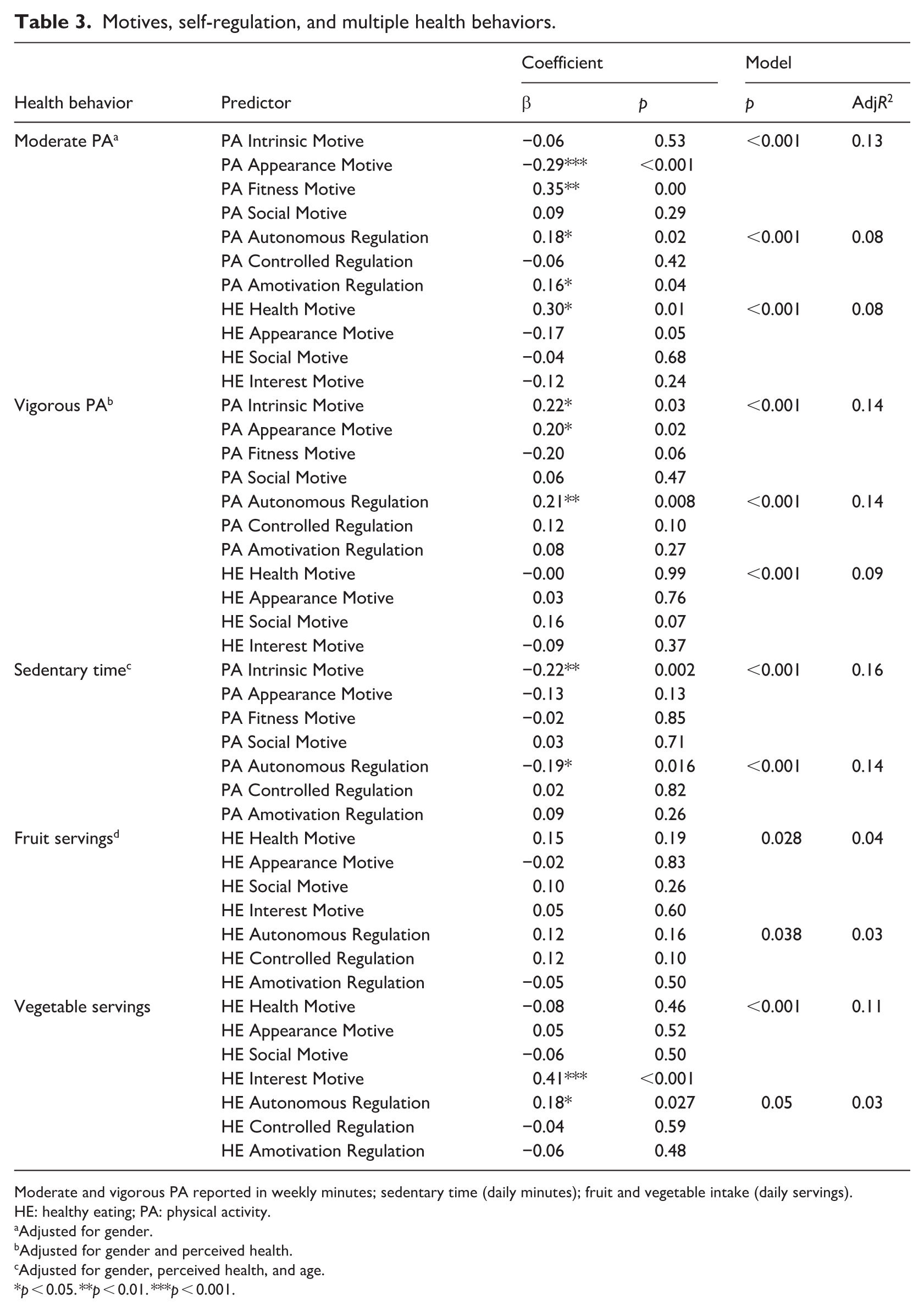
Moderate and vigorous PA reported in weekly minutes; sedentary time (daily minutes); fruit and vegetable intake (daily servings).
HE: healthy eating; PA: physical activity.
Adjusted for gender.
Adjusted for gender and perceived health.
Adjusted for gender, perceived health, and age.
p < 0.05. **p < 0.01. ***p < 0.001.
Moderate physical activity weekly minutes
The motives model (F(5, 178) = 6.35, p < 0.001) significantly explained 13% of the variance in moderate physical activity, revealing that fitness motives positively and appearance motives negatively predicted activity; the self-regulation model (F(4, 179) = 5.11, p < 0.001) accounted for 8% of variance, with both autonomous regulation and amotivation associated with higher activity; and the healthy-eating motives model (F(5, 178) = 4.36, p < 0.001) also explained 8% of variance, with health motives predicting increased activity (p = 0.01).
Vigorous physical activity weekly minutes
All three models significantly predicted weekly vigorous activity: the physical activity motives model (F(6, 177) = 5.75, p < 0.001, R2 = 14%) showed positive associations for intrinsic and appearance motives (ps < 0.05), the self-regulation model (F(5, 178) = 7.03, p < 0.001, R2 = 14%) indicated autonomous regulation predicted increased activity (p < 0.01), and the healthy eating motives model (F(6, 177) = 4.07, p < 0.001, R2 = 9%) also reached significance.
Sedentary daily minutes
Both models were significant for daily sedentary minutes: the physical activity motives model (F(7, 179) = 5.99, p < 0.001, 16% variance) indicated that higher intrinsic motives were associated with lower sedentary time (p < 0.01) and the self-regulation model (F(6, 180) = 6.10, p < 0.001, 14% variance) showed greater autonomous regulation led to decreased sedentary behavior (p < 0.05).
Daily fruit and vegetable servings
Both the healthy eating motives model (F(4, 182) = 2.79, p < 0.05, 4% variance) and the self-regulation model (F(3, 183) = 2.87, p < 0.05, 3% variance) significantly associated with daily fruit servings. For daily vegetable servings, the healthy eating motives model (F(4, 182) = 6.44, p < 0.001, 11% variance) and the self-regulation model (F(3, 183) = 2.87, p < 0.05, 3% variance) were also significant. Greater interest (p < 0.001) and autonomous regulation (p < 0.05) associated with increased vegetable intake.
Discussion
This study applied SDT to examine motivational and self-regulatory determinants of multiple health behaviors in young adults and provides an initial psychometric evaluation of an adapted Motives for Eating a Healthy Diet scale. The four-factor Motives for Eating a Healthy Diet scale demonstrated strong factor loadings, high internal consistency, and evidence of criterion validity through sensitivity to expected differences and associations. Further evaluation of the factor structure is needed using confirmatory factor analysis and measurement invariance across sex/gender, ethnicity, and broader settings.
Gender differences in motives and self-regulatory processes provide evidence of criterion validity for the adapted Motives for Eating a Healthy Diet scale. Compared to males, females reported greater autonomous healthy diet regulation and stronger health, interest, and appearance motives. This aligns with evidence that women demonstrate greater health and weight consciousness in dietary decision-making (Wardle et al., 2004). Females also reported higher appearance and fitness physical activity motives, consistent with evidence that women’s activity motivation often includes a blend of autonomous and controlled components (Egli et al., 2011).
Autonomous motivation predicted healthier behaviors, consistent with theory and prior research. Stronger autonomous motivation was associated with greater physical activity, less sedentary behavior, and higher vegetable consumption. Results support research linking autonomous motivation to exercise (Teixeira et al., 2012), healthier diets (Maillet and Grouzet, 2022), and reduced sedentary time (Esmaeilzadeh et al., 2022). Notably, amotivation was positively associated with moderate physical activity. Moderate physical activity (e.g. walking, chores) may accumulate through habit despite low reflective motivation (Hopkins et al., 2022). Future research should examine how habit, context, and intensity moderate motivation-behavior associations.
Motivational processes differed for fruit versus vegetable intake. No specific healthy eating motives or self-regulatory styles associated with fruit consumption, consistent with evidence that fruit intake is opportunistic and environmentally driven by cost, availability, and convenience (Larson et al., 2012). Conversely, greater healthy eating interest and autonomous self-regulation associated with higher vegetable intake, a more effortful dietary behavior (Coumans et al., 2022), emphasizing intrinsic motivation is required to sustain this more effortful behavior requiring preparation.
Cross-behavioral analyses revealed selective motivational spillovers. Health motives for eating correlated with increased moderate physical activity, suggesting health-oriented motivations transfer across behavioral domains (Lee et al., 2021). Physical activity autonomous regulation also correlated with lower sedentary time, indicating high-quality motivations co-occur across behaviors (Carraça et al., 2024). Given the cross-sectional design, causal inferences cannot be drawn; longitudinal research is needed to examine directionality of these associations.
Limitations include self-report measures and single-item sedentary assessment. The homogenous sample limits generalizability, and small male subsample reduced power. Future research should employ diverse samples and objective measures. Interventions are needed to establish causal mechanisms for sustainable lifestyle change.
Footnotes
Ethical considerations
The current research was approved by Miami University’s Institutional Review Board, Oxford OH. Exempt Research Certificate Number: 00447e. Data were collected via an anonymous survey platform.
Consent to participate
Informed consent to participate was obtained electronically from all participants before they began the online survey. Participants gave digital consent prior to the first survey question.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available at request by contacting the corresponding author.*