
Abstract
This qualitative interview study explored older people’s experiences and perceptions around mental wellbeing and using digital technology in later life, and the relationship between the two. Twenty-three community-dwelling older people aged 65+ years took part in a one-to-one, semi-structured interview between January and March 2025. Reflexive thematic analysis led to the development of five key factors involved in maintaining older people’s mental wellbeing and digital technology’s double-edged role in each: psychological, social, cognitive, physical, and financial health. Reviewing the findings through a critical gerontology lens reveals the persistence of ageism impacting on older people’s digital experiences during a time of rapid digital shifts towards AI-based and online-only services. The need for a strengths-based approach to supporting older people’s digital inclusion and technology independence is discussed.
Introduction
In a post-Covid pandemic world in which some digital shifts remain permanent and the rapid advancement of artificial intelligence (AI) has an ever-growing presence in public discourse, it may be easy to assume that digital technologies have reached a level of global ubiquity and democratisation. However, digital exclusion persists despite the growing ‘digital by default’ nature of many essential services, from banking to education (Wilson-Menzfeld et al., 2025). Indeed, nearly one-third of the global population (2.6 billion people) were estimated to lack internet access in 2023 (International Telecommunication Union, 2023).
Digital exclusion is about more than just access: it also includes barriers to literacy, confidence or skills which lead to an inability to benefit from digital technologies and the services they confer (Wilson-Menzfeld et al., 2025). This multifaceted concept is also complex in its effects, to the extent that digital inclusion has been proposed as a ‘super social determinant of health’ due to its potential impacts on all other social determinants of health (Sieck et al., 2021). Older people are one population group known to experience digital exclusion (Mubarak and Suomi, 2022; Raihan et al., 2025). Existing research suggests an important relationship between digital exclusion and decreasing access to public services with age: in Aotearoa New Zealand (NZ), recent findings showed that over 40% of people aged 60+ years experienced barriers to accessing online government information and services, and self-reported confidence to use digital devices decreased with each decade (Citizens Advice Bureau New Zealand, 2022).
Age-related digital exclusion is an important challenge in a time of ageing populations, but the nature of this divide is dynamic and difficult to characterise (Mubarak and Suomi, 2022; Wilson-Menzfeld et al., 2025). Reasons for age-related digital exclusion have been theorised to involve a complex interplay among sociodemographic, physiological, and psychological factors (Ge et al., 2025). Digital exclusion has been associated with implications for older people’s wellbeing, including cognitive impairment (Wang et al., 2024), access to healthcare (Mubarak and Suomi, 2022), social exclusion (Ge et al., 2025), technology anxiety (Ge et al., 2025), and depressive symptoms (Wang et al., 2025). The term ‘technostress’, which has traditionally been used to study technology-related distress among workers, has more recently been applied to older populations to better describe their stress-related experiences with digital technologies (Nimrod, 2018). Dimensions of technostress include overload, invasion, complexity, privacy, and inclusion, and previous research has found a significant negative association between technostress and life satisfaction (Nimrod, 2018, 2022). However, the implications of technology use among older people are not fully understood, as other research has found positive mental health associations with internet use in people aged 50+ years (Luo et al., 2025).
Research on older people’s relationship with digital technology and its mental wellbeing impacts is further struggling to keep pace with the rapid advancement of machine learning technologies such as AI and the digital transformations that are already underway (Fritsch et al., 2022; Wong et al., 2025). While the ageing population may demonstrate an overall increase in digital adoption over time (Faverio, 2022; Mace et al., 2022), the persistence of digital exclusion may become more complex and challenging to address (Wilson-Menzfeld et al., 2025). Understanding the complexities of digital exclusion, from the perspectives of older people themselves, is increasingly important during a time of increased digitalisation (Wanka et al., 2023). This study explored older New Zealanders’ perceptions and experiences around mental wellbeing, digital technology, and the relationship between them. These perspectives are crucial in informing efforts to ensure that digital transformation is done equitably across the age spectrum and mitigates the potential psychological harms resulting from digital exclusion.
Methods
Positionality
We are a transdisciplinary team bringing a breadth of perspectives and experiences to the research. The first author (MS), a USA-born qualitative researcher and PhD candidate of European ancestry (referred to as Pākehā in Aotearoa New Zealand (NZ)), has a background in equity-focussed health services research and medical anthropology. Author (CLL) is a qualitative Kaupapa Māori researcher with a research background in health inequities and mental health. Author (VN) is a Pacific academic at the University of Auckland. He has extensively worked as a Pacific health researcher in New Zealand, the Pacific region, Australia, Hawaii, and the USA. RW is a Pākehā public health physician and long-term researcher in digital population health programmes. JM is a Pākehā public health researcher skilled in qualitative and survey design and analysis. RD is a Pākehā mixed methods digital health researcher and psychologist working both within the New Zealand public health service and the university.
This breadth of perspectives supported our aim to achieve a balanced interpretation of the data. This was particularly important at times when the first author lacked lived experience or expertise relating to, for instance, participants’ ethnic background or mental health experiences. When this occurred, targeted discussions were undertaken during the analysis with study team members having relevant lived experience or expertise to further contextualise the data and clarify interpretive decisions.
Study design
We conducted an observational study involving one-time, semi-structured interviews from January to March 2025 in Aotearoa NZ. We referred to the COREQ checklist to facilitate the reporting of this qualitative research (Tong et al., 2007). The study procedures and interview guide were developed with input from the transdisciplinary study team. Ethics approval was granted by the University of Auckland Human Participants Ethics Committee (Reference no. UAHPEC28518).
Study setting and participants
Inclusion criteria included being aged 65+ years, community-dwelling (not currently in residential care or hospitalised), comfortable participating in English, and consenting to participate. Current or prior history of diagnosed mental disorder was not a requirement to participate. Convenience sampling methods were used to recruit participants, who were unknown to the researchers prior to the study, leveraging the study team’s existing university and community networks. The study sample size was projected to include a minimum of 10 participants but was determined pragmatically during data collection based on data adequacy and pragmatic constraints (Braun and Clarke, 2021).
Study procedures
Flyers were distributed through relevant channels which provided researcher contact details. Potential participants were provided an information sheet and consent form in-person or via email and invited to ask the researcher any questions they had about the interviews before giving informed consent. Upon consenting to participate, one-time interviews took place via videoconferencing, phone, or in-person in a private setting with a female researcher (MS). Each participant was offered a NZ $30 gift card for participating and given the option to bring a support person to the interview. All interviews were audio recorded and detailed notes were taken by the interviewer. Interviews were transcribed and participants could request a copy of their transcript with an opportunity to provide corrections. Interviews lasted an average of 57 minutes (range = 41–85 minutes).
Prior to commencing the interview, the researcher introduced herself and the purpose of the study. Participants were also asked to complete a short demographics survey. During the interview, the researcher asked a series of open-ended questions to understand participants’ thoughts on (1) mental wellbeing in later life; (2) experiences with/feelings about digital technology in their everyday life; and (3) how technology relates to older people’s mental wellbeing. The semi-structured interview guide is included as Supplemental Material.
Data analysis
Demographic information was summarised using descriptive statistics (means, ranges). Interviews were analysed using reflexive thematic analysis as described by Braun and Clarke (2019). Analysis was led by the interviewing researcher (MS) who first re-read each interview transcript and notes for familiarisation. Transcribed interviews were then coded inductively using NVivo 14 (Lumivero, 2023). A subsample of transcripts was double-coded by a second researcher (CLL) and discussed with the interviewing researcher and a third researcher (RD). Themes were then developed, reviewed and interpreted in a discussion with the wider study team (RD, VN, JM, RW). These steps were taken to encourage a deeper and more nuanced perspective on the data rather than seek consensus (Braun and Clarke, 2019). Themes were then finalised by the interviewing researcher. The analysis was influenced by the interviewing researcher’s theoretical assumptions including a prior scoping review around age-related digital exclusion and critical gerontology, which promotes the use of reflexive techniques to challenge strictly biomedical understandings of ageing as well as ageist social policies and constructions of ageing (Chong and Gu, 2021).
At the end of this process, participants were offered a summary of the findings for their feedback.
Results
A total of 23 participants took part in an interview. Demographic characteristics of all participants are presented in Table 1.
Participant characteristics (N = 23).
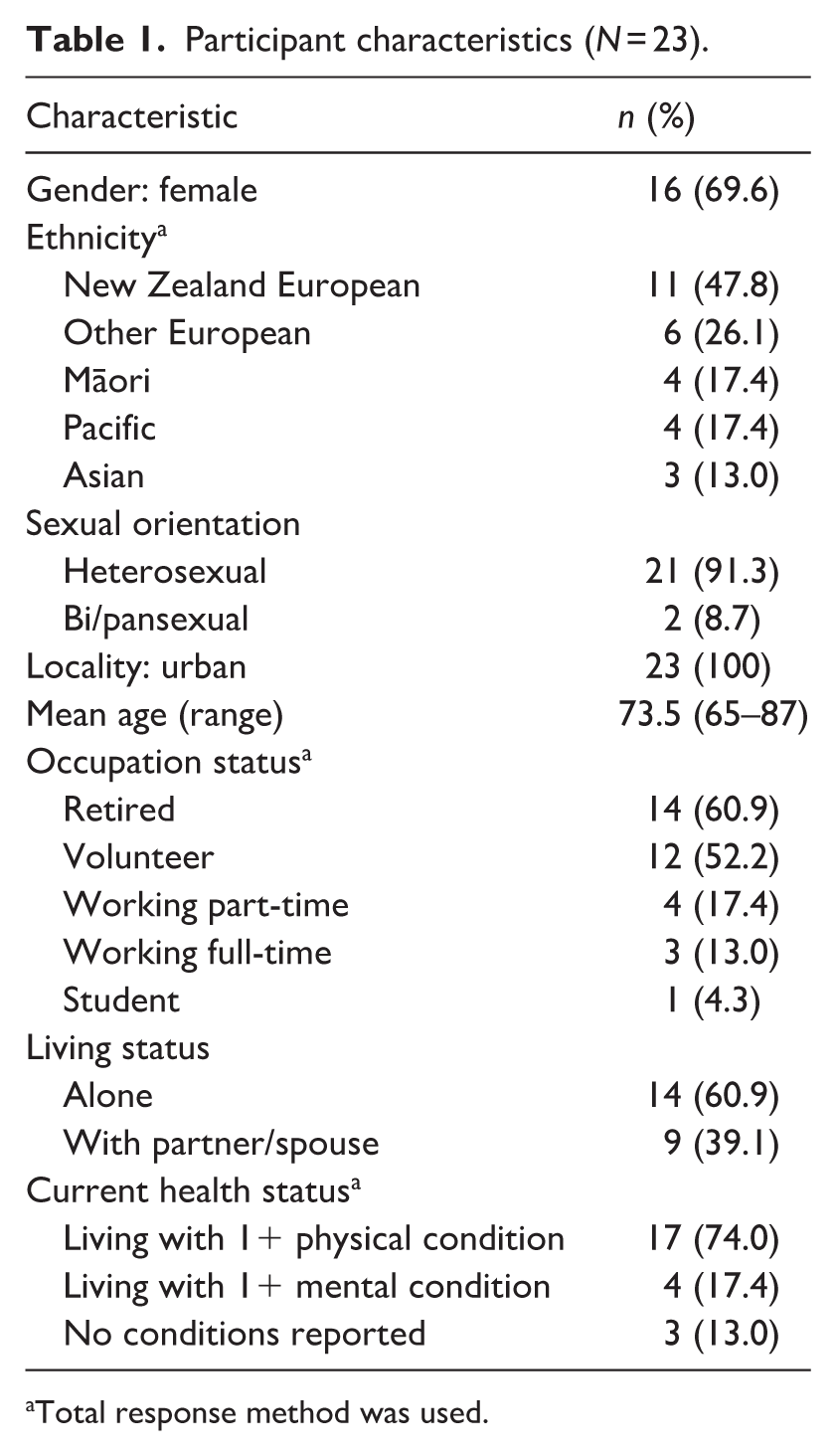
Total response method was used.
Most participants conceptualised their technology use as it related to ICTs such as mobile phones and computers/tablets, however several also noted other forms of digital technology they used such as a car with a touchscreen control panel or automated teller machines (ATMs). Participants’ experience and comfort levels with technology varied widely, spanning minimal use (e.g. essential communications via phone and text) requiring frequent support from friends or family members, to frequent independent use including use of emerging technologies (e.g. AI assistants). All participants felt that some degree of technology use and digital literacy are needed to function in today’s world and that technology could be beneficial or harmful to mental wellbeing depending on level of digital inclusion/exclusion. Most participants attributed the degree of technology use in their working years for their current level of comfort and digital literacy, as well as whether they had an intellectual interest in learning about digital technologies. Mental health experience also varied, with several participants having lived experience with a mental health disorder and/or professional experience in counselling or psychotherapy.
Five key themes regarding age-related contributors to mental wellbeing in later life and technology’s mediating role were developed from the analysis.
Psychological factors involved in mental wellbeing
Participants described several key psychological factors that are important to consider for maintaining their mental wellbeing as they aged (Table 2). Most participants spoke about the importance of recognising that life’s ups and downs are normal and that mental wellbeing is not the result of an absence of difficulties, but rather an ability to cope through them. Related to this, participants expressed mixed views about whether happiness should be the goal or if this is overrated or unrealistic. Mental wellbeing was largely considered to require intention and effort, that self-management skills do not come naturally, and that finding a sense of purpose and belonging post-retirement is critically important. Volunteering was frequently endorsed as a way to achieve a sense of purpose as paid employment and family obligations eased.
Key themes as related to psychological factors and illustrative quotes.
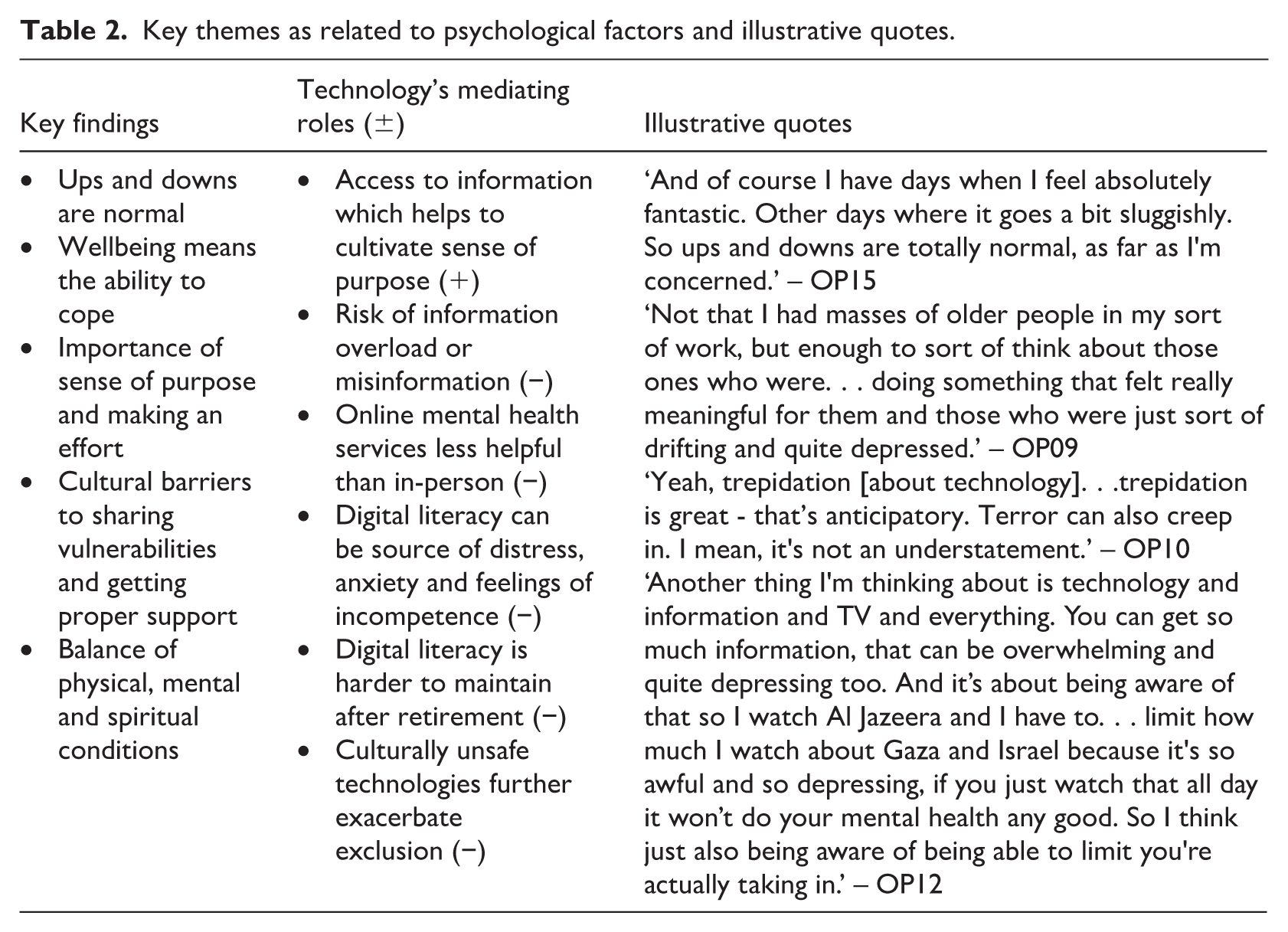
Several participants also spoke about the need to consider mental wellbeing as part of a larger balancing act between physical, mental and spiritual wellbeing. Pākehā or Western culture was perceived to devalue the importance of this holistic view and discourage people from sharing their vulnerabilities and struggles with growing older. Conversely, several participants also described positive feelings of peace that were perceived to come naturally with age and an increased sense of freedom to pursue hobbies, such as planning travel, gardening, or choir music.
Technology’s role in psychological factors
Technology was perceived to mediate on these factors in both positive and negative ways. In a positive sense, technology was viewed by most participants as a crucial method for accessing information that facilitates cultivating a sense of purpose and connection to the world. Examples of this included using Google and YouTube to explore hobbies and learn. Conversely, the risk for information overload and misinformation were perceived to have a negative impact on participants’ mental wellbeing, particularly the ability to access the news 24/7. Further, many participants expressed that challenges using technology could be a major source of distress, frustration or feelings of incompetence. Participants similarly shared concerns about exclusion as the difficulty of ‘keeping up’ with technology post-retirement if they previously had a job that required digital literacy. Nearly all participants felt that digital technologies are not developed with older people in mind, with reasoning that older people are not a high-profit demographic for tech companies. Several participants also expressed scepticism about technology-based mental health services, as these lack the ability to read body language or provide the psychological benefits of human-to-human connection. Cultural insensitivity was also noted by several participants, such as mispronunciation of text-to-voice for places with Te Reo Māori (Māori language) names, further exacerbating a feeling of exclusion from the digital world.
Social factors involved in mental wellbeing
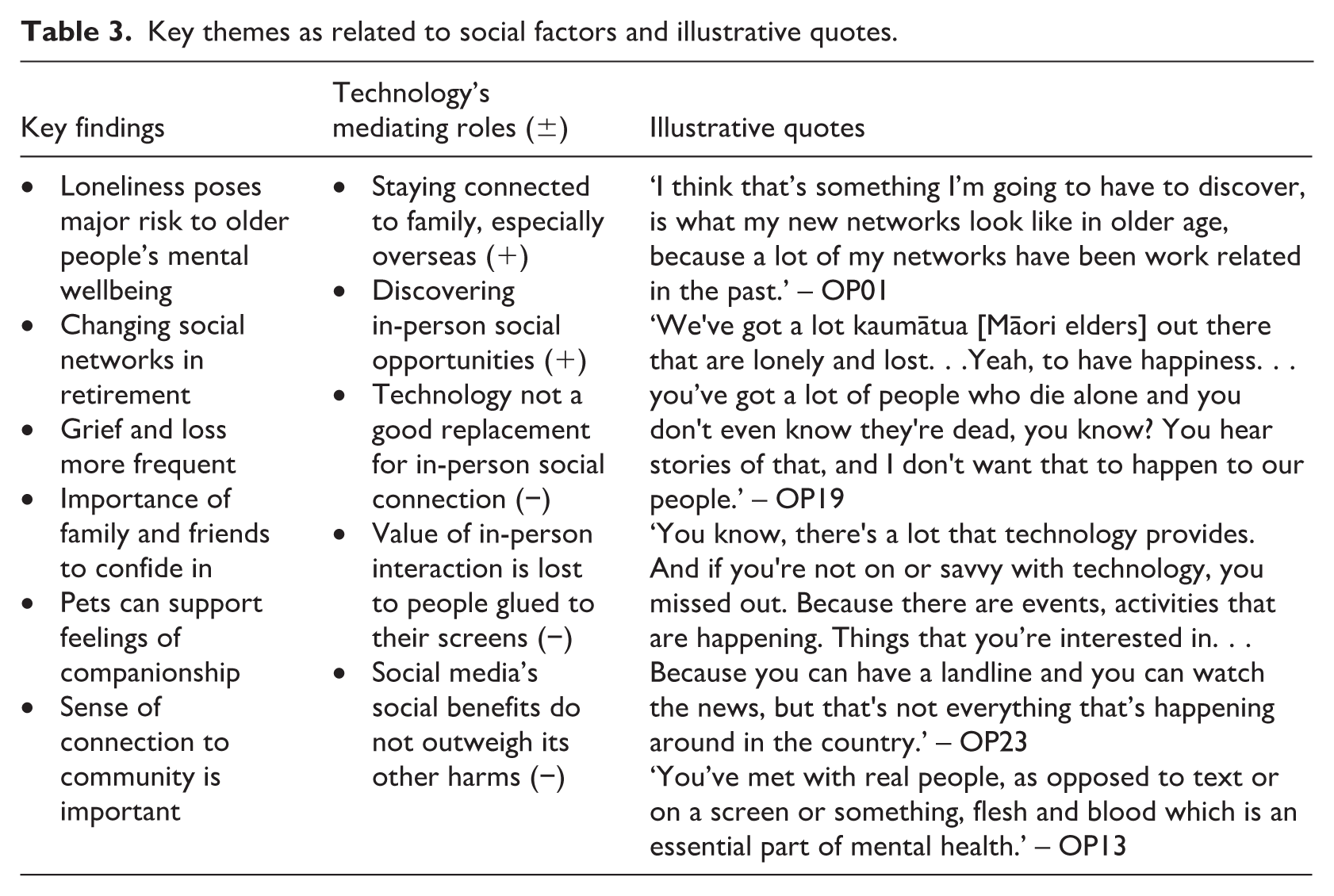
Loneliness and social isolation were described by participants as some of the most important issues among older people with significant implications for mental wellbeing (Table 3). Close relationships were seen as vitally important in that they provide a person to confide in when struggling mentally or grieving a loss. Maintaining social connection was perceived to require more effort in later life but could also be more meaningful when focussing on quality time with family and close friends. For participants living alone, pets were also perceived to fill an important companionship role and sense of feeling needed. Several participants also spoke about the importance of feeling connected to their community and that even surface-level interactions with acquaintances like neighbours and store clerks are also important. Some participants felt that Pākehā or Western culture overvalues independence at the expense of strong family relationships and devalues the wellbeing benefits of intergenerational households.
Key themes as related to social factors and illustrative quotes.
Technology’s role in social factors
Technology was seen as having a positive effect on participants’ social wellbeing in keeping them connected to loved ones. Several participants mentioned that FaceTime played an important role in being able to connect with loved ones regularly even if they had moved overseas. Technology was also seen as the primary method for organising in-person social activities and finding local social groups to join. Participants often spoke about the value of technology for sharing and storing memories, such as videos from their grandchildren. Despite these benefits, all participants felt that technology is not an adequate replacement for human connection. Many also shared observations of technology having a detrimental impact on in-person interactions, such as dinner table conversations being disrupted due to people being glued to their phone. Several participants also described a generational divide around technology and a resultant social disconnection, with some participants describing efforts to use apps like Pokémon Go solely to maintain connection with grandchildren. Nearly all participants expressed concern about social media and felt it did not provide enough social benefits to outweigh its downsides and associated distress, particularly around misinformation, scams, and excessive advertising.
Cognitive factors involved in mental wellbeing
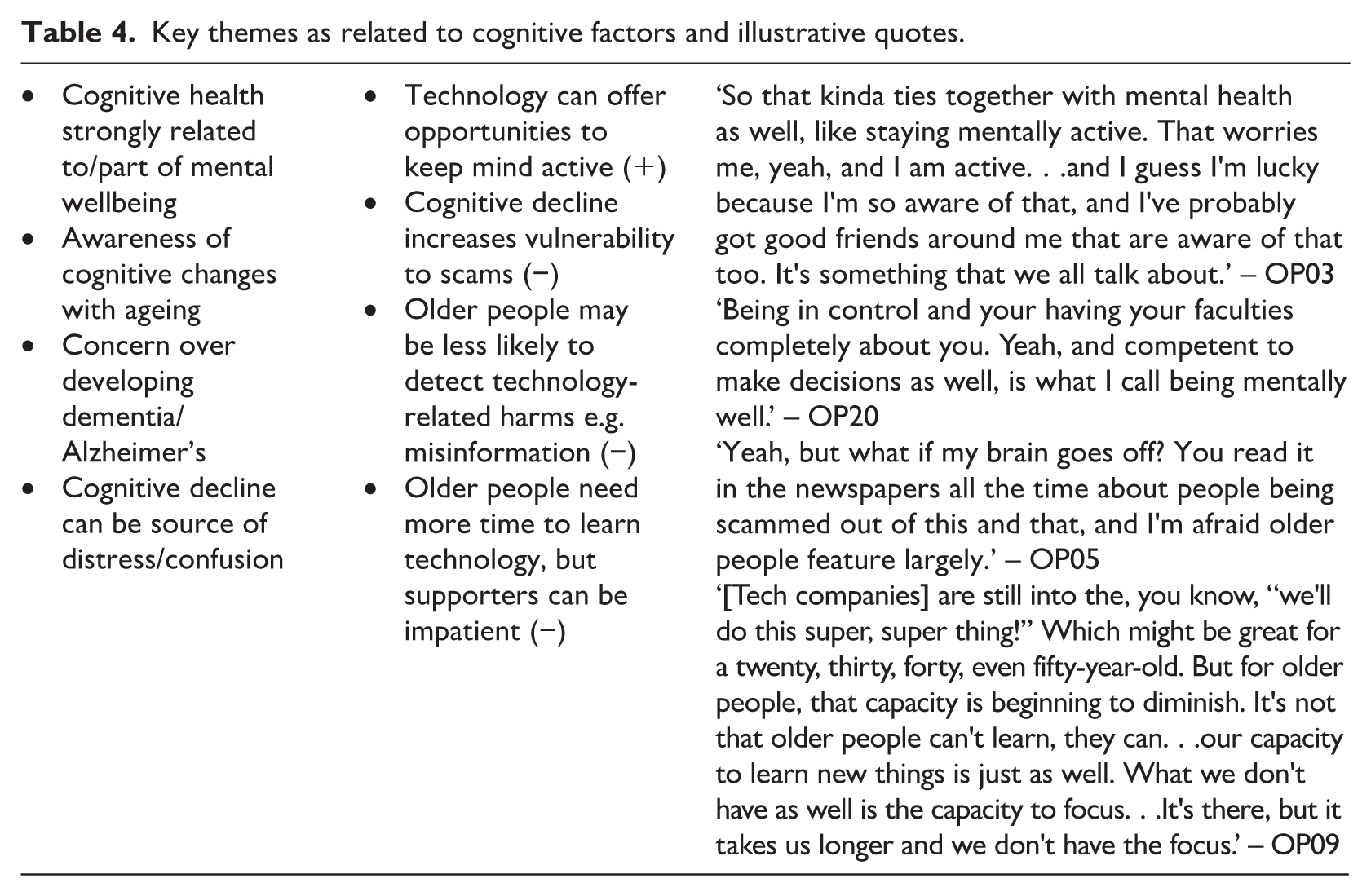
Cognition was another important wellbeing factor among participants (Table 4). Many expressed an awareness of their cognitive abilities changing as they grew older, such as having more difficulty remembering people’s names, and feared the possibility of cognitive decline in the form of dementia or Alzheimer’s. Many participants had observed the effects of dementia and cognitive decline among family members and feared the associated mental distress due to confusion and loss of independence. Most participants thus felt it was vitally important to maintain their cognitive health. This was perceived to become more difficult in retirement as cognitive challenges were less inherent in everyday life and instead needed to be sought. Some participants gave examples of ways they tried to keep mentally active, such as joining a bridge club or learning a new language.
Key themes as related to cognitive factors and illustrative quotes.
Technology’s role in cognitive factors
Participants saw technology has having potential benefits for participants’ cognitive health in the opportunity to keep their minds engaged through online games such as Wordle, learning about new topics, and upskilling in digital technology itself. However, there was a perceived point of diminishing return, as cognitive decline could make it more difficult for older people to learn or maintain their technology skills and reduce their ability to detect some of technology’s harms, such as scams and misinformation. Participants also described an increasing need to critically analyse everything they consumed online, and a growing sense that people can no longer take everything they read at face value.
These challenges could contribute to symptoms of distress. For instance, some participants noted stressful experiences when trying to complete a complicated online-only pension application or struggling to re-learn how to use their email app after unexpected updates to the interface. Most participants asserted that older people need more time to learn or master digital technologies and that patience is thus required. However, this patience was not always seen as being provided by their usual support people (e.g. customer services, family, friends) which could further exacerbate feelings of distress or incompetence. Some participants also described concern about burdening their family members with technology issues when their time together was already limited. Many participants were aware of community-based technology support services and endorsed these as a way for older people to receive in-person support from patient individuals with proper training.
Physical factors involved in mental wellbeing
Physical health was seen as integrally linked to mental wellbeing for participants, despite a common feeling that physical and mental health are siloed by the health system (Table 5). Participants frequently discussed increasing physical health issues as they grew older, which could limit their capacity to maximise on the freedoms that come with retirement. Physical disability was also linked to loneliness, with some participants citing issues such as hearing and vision loss which make it more difficult to participate in community activities and result in disengagement. Nearly all participants emphasised the importance of looking after their physical health to maintain their mental wellbeing. This included staying physically active with exercise, good nutrition, and having regular visits with a general practitioner (GP) they trusted. Several participants recounted first-hand experiences of the mental wellbeing impacts when physical health is lost, such as having a heart attack or feeling distress over uncontrolled diabetes.
Key themes as related to physical health factors and illustrative quotes.
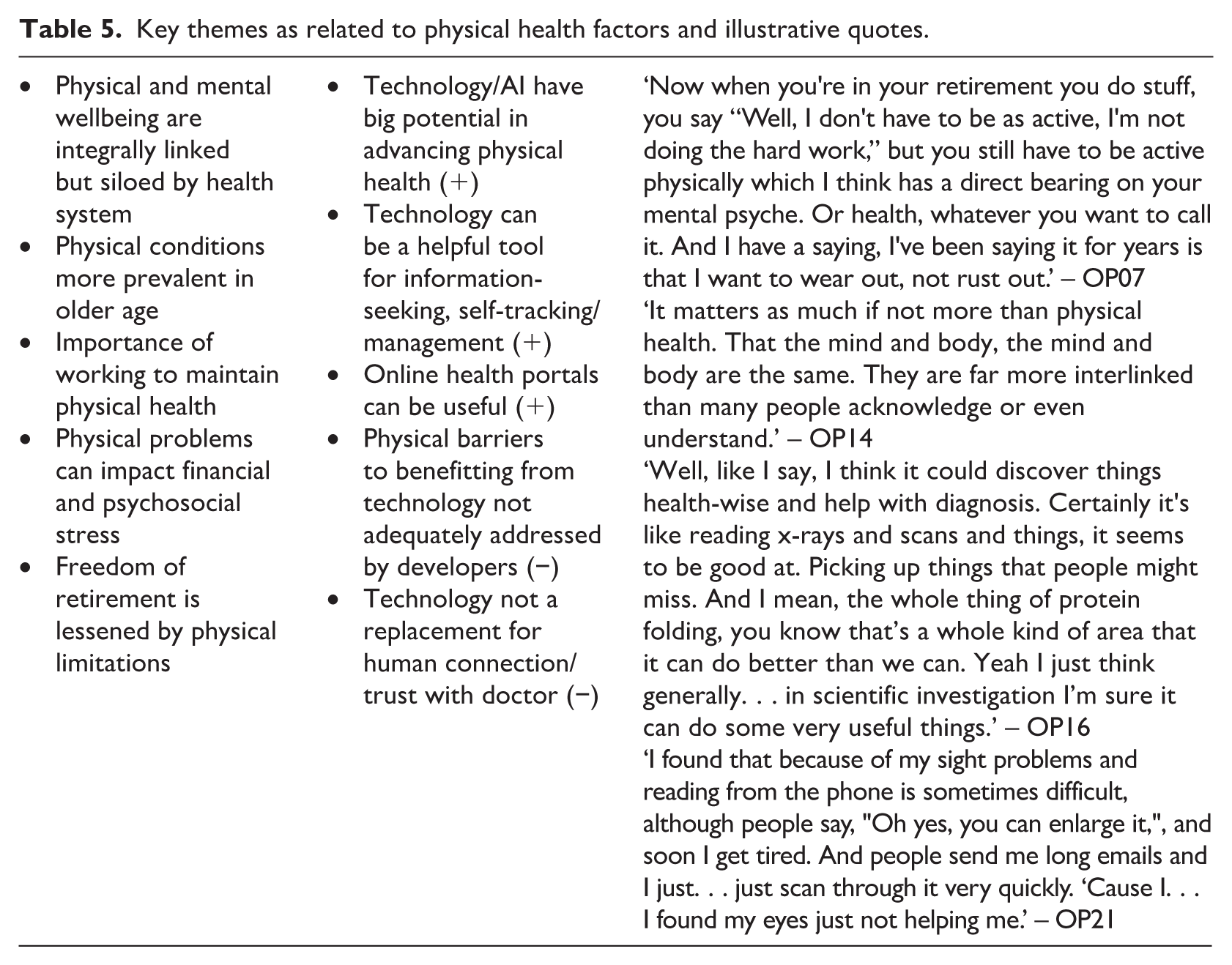
Technology’s role in physical factors
Technology was perceived to have several positive implications for participants’ physical health. While participants were generally doubtful about AI’s societal impacts, advancements in physical health were viewed as the area where AI has the greatest potential for benefit to society. Several participants with higher levels of knowledge expressed optimism about AI’s potential to improve areas such diagnostic image reading and drug discovery. Apart from AI, some participants used health apps or wearables, such as a Fitbit or a continuous glucose monitor, which they viewed as helpful tools. Many participants also used Google and YouTube to seek health information which they highly valued but noted that a critical eye was necessary to identify credible sources. While most participants still preferred to phone their health provider, many also saw great value in using an online health portal to view test results quickly and schedule appointments at their convenience.
Participants frequently expressed that digital technologies do not provide enough accessibility options for their physical needs. For example, participants with vision loss felt that text size customisations on their phone were often impractical for reading long passages and text-to speech-options were not always convenient or culturally appropriate for Aotearoa NZ. All participants also expressed a strong preference to continue seeing their GP and health professionals in-person due to a perception that the quality of the interaction is lost in a phone or video appointment. Several participants saw potential benefits in telehealth for people with disabilities and they appreciated the ability to transition to telehealth during Covid outbreaks. Many participants recounted experiences of trying to use an online health portal and finding it overly complicated as compared to simply phoning a receptionist. For some participants, the possibility of transitioning to virtual/digital-only healthcare delivery, particularly in areas with existing workforce shortages, was viewed with great concern for Māori and other priority groups who already face inequities, access barriers and mistrust. These downsides to technology represented a source of frustration for most participants and for some exacerbated a feeling of losing control over their physical health.
Financial factors involved in mental wellbeing
All participants spoke about stress related to financial security in later life, particularly following retirement, and the significant impact this could have on their mental wellbeing (Table 6). Participants frequently described feelings of unpreparedness and anxiety about retirement and managing the associated change in income. Financial stress was especially salient for participants living alone. Several participants living alone spoke of the need to downsize or seek housing support after retiring, experiences which caused strong feelings of grief or anxiety. Getting care for physical or mental health conditions was also noted to be costly and added a stressful age-related financial burden. As a result, these financial stresses posed a barrier to participants’ ability to benefit from the freedoms they hoped to experience in retirement.
Key themes as related to financial factors and illustrative quotes.
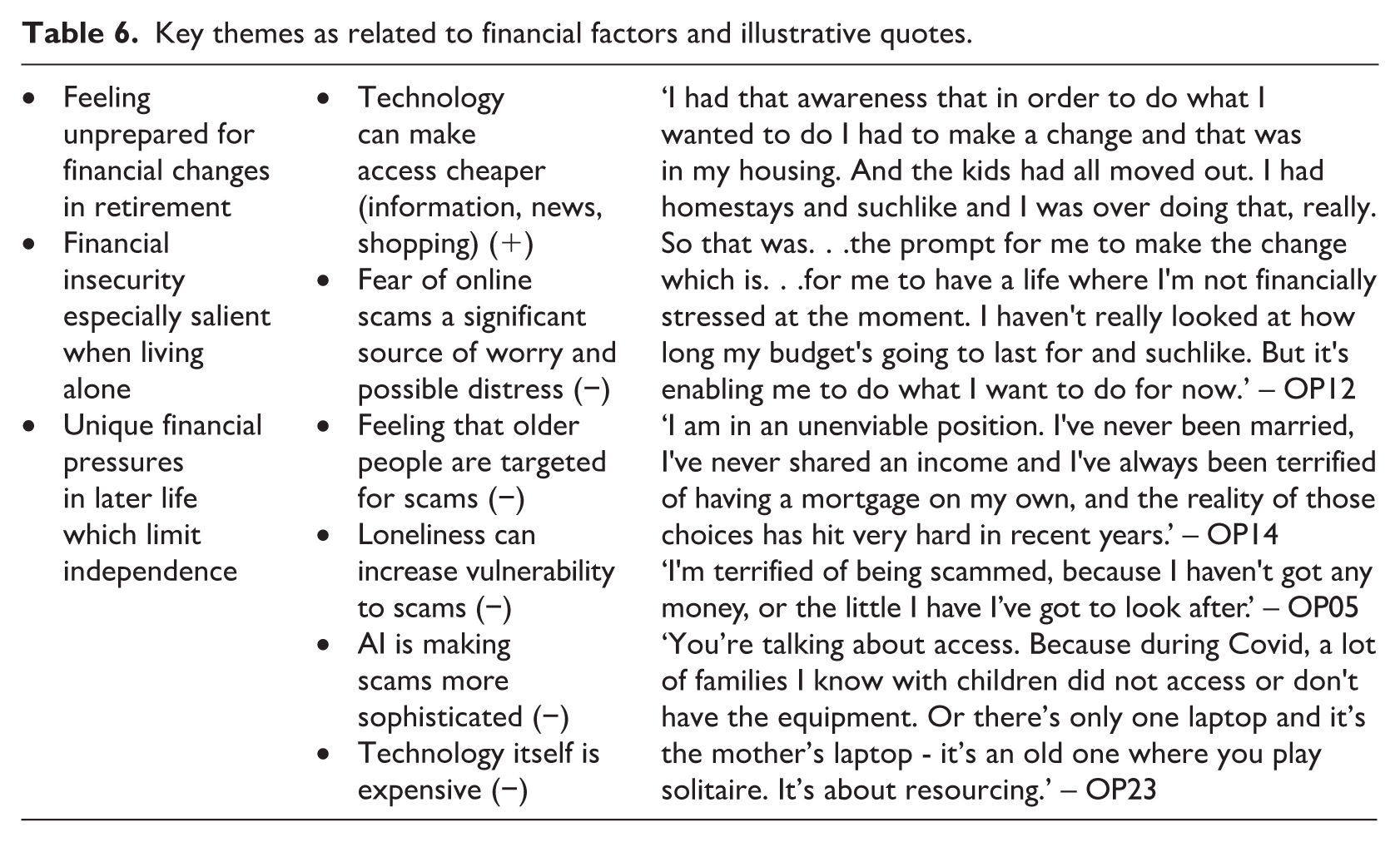
Technology’s role in financial factors
Technology was viewed positively in terms of participants’ ability to access information, news, and shopping at low or no cost. For example, one participant spoke with enthusiasm about their low-cost subscriptions to multiple global online newspapers spanning Europe, Asia and the Pacific. Another participant spoke of the benefits of being able to find low-cost health and nutrition products online which would have otherwise been out of budget. However, many participants noted that staying up to date with digital technologies themselves is extremely costly and often out of reach for older people, exacerbating a feeling of disconnection and inability to benefit from the latest devices.
Fear of online scams or data breaches were also reported to have an important role in participants’ sense of mental wellbeing. Regardless of digital literacy, participants were unanimous in feeling that older people are targeted for scams and that AI is making these scams more sophisticated and difficult to detect. Online engagement was also perceived as reinforcing an increasingly consumerism-driven online world, with advertising becoming sneakier and more targeted in commonly accessed services like YouTube, Google, and Facebook. While many participants said they relied on family members for support in addressing suspected scams, several also noted that family members can themselves be capable of fraud, particularly when they are given access to an older person’s online banking details. Several participants were emphatic that falling victim to a scam or data breach could lead them to financial ruin, particularly if living alone, and that this prospect was a source of anxiety. Online banking in general was met with mixed views, as many participants shared concerns that the loss of in-person banking options and real-time customer services caused them to feel less in control over their finances. Several participants also pointed out that ATMs are frequently updated and that the changes can cause confusion for older people who still rely on cash, particularly in areas where cash is still a commonly used payment method.
Discussion
This study explored older New Zealanders’ perspectives on mental wellbeing and digital technology, and the relationship between the two. Results from the qualitative interviews suggest that digital technology plays a complex but important mediating role in each of the factors impacting older people’s mental wellbeing. On a practical level, all participants expressed technology-related distress and fear, such as being targeted for online scams or losing the cognitive ability to successfully keep up with technology. However, participants also acknowledged that when digital inclusion is achieved, technology has unique benefits which can support older people’s wellbeing and independence. This ‘double-edged sword’ conception of digital technology is not new (McLean et al., 2025) but reflects an unresolved tension between older people’s increasing need for digital engagement and the risk of harm and distress that may coincide, reaffirming the importance of understanding technostress and its impacts (Nimrod, 2022). It also builds on the proposition of digital inclusion as a super social determinant of health, where digital technologies may play an overarching and crucial role in the trajectory of health disparities – including those related to mental wellbeing (Sieck et al., 2021).
While the dimensions of mental wellbeing developed in this study provide a useful conceptual model to clarify the critical role of digital inclusion in key areas of older people’s subjective wellbeing, the complexity of digital exclusion and its impacts will inevitably demonstrate fluctuating interdependencies and nuances that must be considered in the interpretation of these findings. Ongoing engagement of older people to understand their experiences will be crucial as services continue to undergo digital transformation to ensure that older populations are brought forward equitably in this process (Ge et al., 2025). Participants contributed valuable counterarguments to the ongoing demand for developers to innovate and services to digitise, and to consider the psychological impacts of ignoring end-users’ needs and preferences. Participants also provided an important reminder about what may be lost in the process of digitalisation: vital human-to-human connections that technology cannot replace. Participants belonging to priority equity groups further emphasised that the most underserved community members will not benefit from even the most well-intended developments, such as online patient portals, if they cannot afford the required devices or infrastructure, do not see value in this modality, or have concerns about their data privacy. It may therefore be more useful to think about older people’s reasons for distress or frustration around digital technology, rather than barriers to acceptance, which may place too much emphasis on individual deficits and under-recognition of the problems stemming from blind adoption at the societal level (Zhang, 2023).
Critical gerontology offers a useful lens to consider these findings within the wider societal and cultural systems at play. Older people’s experiences of digital exclusion described in this study reflect many of the ageist and deficits-based social constructions that have been observed elsewhere, including assumptions about older people’s willingness and ability to engage with digital technology safely and independently (Choi et al., 2020; Figueiredo et al., 2025; Mace et al., 2022; Manor and Herscovici, 2021). Ageism is a multifaceted concept that is theorised to manifest both implicitly and explicitly and on multiple levels, including individual/internalised, interpersonal/social, and institutional/cultural (Iversen et al., 2009). All three levels of ageism were identified in the discussions that took place in this study. Individually, internalised ageism was evident among participants who worried their age made them inherently more vulnerable to scams despite acknowledgement that scams are becoming increasingly sophisticated and universally difficult to detect. Self-blame for perceived digital incompetence was also common among participants, despite demonstrated proficiency in other forms of technology. Interpersonally, participants recounted experiences of unexpectedly dismissive, impatient responses from their usual sources of support regarding technology challenges, which further exacerbated feelings of incompetence, fear, and frustration. On the institutional level, participants were emphatic that digital technology is not designed with older people in mind and described a feeling of being ‘left behind’ from the digital sphere when they retired, despite the ongoing expectation, including from government services, to engage with technology for completion of everyday tasks. The presence of ageism in the digital space must not be ignored, as greater exposure to ageism has been found to be associated with decreased internet use (Choi et al., 2020; Gudynaite et al., 2025) and has implications for health and wellbeing that are avoidable (Stephens and Flick, 2010).
Implications for practice, policy, and research
Taking a strengths-based approach may offer promising future directions and recommended next steps which both address digital exclusion and the ageism present within it (Stephens and Flick, 2010). Although participants were appreciative of family members who provided support with technology, defaulting to reliance on family was not always viewed as the optimal way of promoting older people’s digital inclusion, nor did it necessarily build their confidence and independence as technology users. Participants instead endorsed the availability of more community-based support with skilled, patient coaches; real-time, human support from customer services who are trained in age-friendly practices; and digital device/connection companies being more transparent with older customers about their choices around equity products. Although some participants acknowledged these solutions may exist to some degree, they were not perceived to be widely available or promoted. These recommendations are supported elsewhere in the literature as ways of increasing older people’s digital access, autonomy and independence (Baluk et al., 2021; Barrie et al., 2021; Figueiredo et al., 2025; Manor and Herscovici, 2021; Matenga-Ikihele et al., 2023; Tsai et al., 2017).
Participants also had suggestions with policy and industry-level relevance to improve the way digital technologies are developed and distributed. Participants were emphatic that the increasing complexity of ICTs is often unnecessary, causing undue stress for end-users to un-learn and re-learn constantly and that digital solutions should never be implemented as a replacement for human expertise and interaction, but rather as a tool in their toolbox. Instead, participants endorsed companies providing more choices to consumers when it comes to adoption of unnecessary device or app updates and service innovations, including older people earlier in the design and implementation of mainstream technologies, and systematic discounts on devices and data plans that acknowledge the financial constraints of older people. These recommendations are echoed in the literature (Money et al., 2024; Wilson et al., 2021) and suggest an imperative for governments to treat digital inclusion as a right that warrants regulatory protections for citizens rather than a luxury in the hands of for-profit companies. Health and social care institutions also have an opportunity and indeed an obligation to implement digital equity policies for older patients and staff alike, particularly in contexts like Aotearoa NZ where digital transformation of the health system is receiving substantial government investment (McBeth, 2025). Digital inclusion action plans such as that developed in the UK may provide a promising first step in introducing policy frameworks to progress equity efforts alongside transformation (Digital Inclusion and Skills Unit, 2025).
This study contributes usefully to the literature around the complex nature of the relationship between digital technology and older people’s wellbeing in Aotearoa NZ. This is a dynamic topic area in which much is at stake for populations who may be digitally excluded (Mace et al., 2022; Wilson-Menzfeld et al., 2025) and warrants ongoing participatory engagement with older populations to improve digital equity efforts. In particular there is limited research specifically exploring older people’s knowledge and perceptions about AI, though emerging evidence, similar to the current findings, has found that older populations may have more concerns than younger age groups about AI’s growing presence which must be better understood (Fritsch et al., 2022; Wong et al., 2025). The depth of perspectives reported here reflect a particular sociocultural context but may be useful for informing research undertaken in other settings or with different sample characteristics.
Limitations
This study is not without limitations. Defining older age as beginning at 65 years may not reflect the experiences of priority equity groups who exhibit earlier onset of age-related conditions (Aker et al., 2024; Hayanga et al., 2024). Additionally, the mean age in this study was 73.5 years and representation from advanced-age older people (aged 80+ years) was lower. However, similar findings have been reported in research with older samples (Money et al., 2024).
Conclusion
This qualitative study explored the complex relationship between digital technologies and mental wellbeing among older people. Participants revealed key areas in which technology acts as a double-edged sword in terms of supporting or harming their psychological, physical, psychosocial, financial, and cognitive health. Participants overwhelmingly felt that digital technologies are not designed with older people in mind and may reflect the persistence of ageism in this area. Future research should seek to clarify how to best support older people to be technologically independent and improve access to digital technologies that are age-friendly by design.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261429653 – Supplemental material for Exploring the relationship between technology and mental wellbeing in later life: A qualitative study
Supplemental material, sj-docx-1-hpq-10.1177_13591053261429653 for Exploring the relationship between technology and mental wellbeing in later life: A qualitative study by Melanie Stowell, Cinnamon Lindsay Latimer, Vili Nosa, Judith McCool, Robyn Whittaker and Rosie Dobson in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to thank the participants who took part in in this study and the team at the University of Auckland Centre for Co-Created Ageing Research (CCREATE-AGE) for their support.
Ethical considerations
Ethics approval was granted by the University of Auckland Human Participants Ethics Committee (Reference no. UAHPEC28518).
Consent to participate
All participants gave written or verbal informed consent to participate in the study.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
MS contributed to the study’s conceptualisation, methodology, data acquisition, analysis, project administration, visualisation, writing – original draft, writing – review and editing. RD contributed to the study’s conceptualisation, methodology, supervision, analysis, writing – review and editing. JM contributed to the study’s conceptualisation, methodology, analysis, supervision, writing – review and editing. VN contributed to the study’s conceptualisation, methodology, supervision, analysis, writing – review and editing. CLL contributed to the study’s analysis, writing – review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data can be made available from the corresponding author on request and assuming the completion of a data-sharing agreement.
Supplemental material
Supplemental material for this article is available online.