
Abstract
The preconception, pregnancy, and postpartum (PPP) periods represent a distinct life phase where women are particularly vulnerable to weight stigmatisation. While community members are often the primary source of weight stigma, little is known about their perspectives. This study aimed to explore community members’ perceptions of women’s body weight during the PPP periods, focussing on weight stigma and societal norms. We undertook 20 semi-structured interviews with community members residing in Australia. Interviews were transcribed verbatim and reflexive thematic analysis was conducted. Two main themes were identified: (1) societal value structures around PPP weight were evident with high value and continuous surveillance placed on women’s weight; and (2) conflicting discourse relating to PPP women’s body size was present with participants holding contradictory but simultaneous beliefs regarding women’s weight. Our findings provide valuable insights into specific social norms and beliefs that perpetuate weight stigma towards PPP women.
Introduction
Weight stigma, defined as negative weight-related misconceptions and stereotypes towards individuals based on their body size or weight, is commonly reported and often constitutes bias, discrimination, and social devaluation and exclusion (Puhl and Brownell, 2003). Individuals living in larger bodies are subject to stereotypes portraying them as lazy, unintelligent, unmotivated, and lacking willpower, a phenomenon that is largely socially acceptable (Puhl and Brownell, 2003). Weight stigma is experienced more often among women than men, with women reporting three stigmatising experiences daily, on average (Seacat et al., 2016). Previous studies have shown that the preconception, pregnancy, and postpartum (PPP) periods represent a distinct life phase where women are particularly vulnerable to weight stigmatisation (Hill and Incollingo Rodriguez, 2020) due to significant physiological and physical body size changes as well as pressure to meet societal body ideals (Hill and Incollingo Rodriguez, 2020; Incollingo Rodriguez and Nagpal, 2021; Leopold, 2025). Also, PPP women are held to high societal standards regarding responsibility for the health of their child, and their weight is explicitly blamed for negative outcomes in this domain (Bombak et al., 2016). Weight stigma experienced during this period is linked to worse reproductive healthcare quality and behavioural, anthropometric, and psychosocial outcomes, all of which have potential long-term negative impacts on both mother and child (Hill and Incollingo Rodriguez, 2020; Incollingo Rodriguez and Nagpal, 2021). For instance, experiencing weight stigma during pregnancy can contribute to premature birth, caesarean delivery, high birthweight (DeJoy and Bittner, 2015), and postpartum depression (Incollingo Rodriguez et al., 2019), which is often associated with breastfeeding challenges (Ahmadinezhad et al., 2024) and impaired mother-infant bonding (Gilden et al., 2020). Additionally, weight stigma can contribute to body dissatisfaction, disordered eating, and lowered self-esteem (Wu and Berry, 2018). For example, studies assessing women’s perception and navigation of body weight changes during the postpartum period highlight that many women feel dissatisfaction with their bodies, accompanied by self-judgement and guilt. These experiences are largely influenced by societal ideals, expectation and the desire to return to pre-pregnancy body weight, which can promote maladaptive eating behaviours (Gilmour et al., 2025; Lee et al., 2025).
PPP women report experiencing weight stigmatisation from multiple sources such as the community, media, healthcare, and workplaces (Hill and Incollingo Rodriguez, 2020). While experiences of weight stigma have been well documented from victims’ perspectives (Dever et al., 2025), insights from the perpetrator’s perspectives remain limited, particularly outside healthcare. In a foundational study, the most commonly endorsed sources of weight stigma by pregnant and postpartum women were society in general, the media, strangers, immediate family members, and healthcare (Incollingo Rodriguez et al., 2020). However, despite the general public being the most common source (Incollingo Rodriguez et al., 2020), very little work has systematically studied PPP weight stigma in the community or community members’ perspectives directly (Hailu et al., 2024; Hill and Incollingo Rodriguez, 2020). This is surprising given that a seminal conceptual model of weight stigma for women in the PPP periods (Hill and Incollingo Rodriguez, 2020) identified the community setting along with the influence of culture and society as critical socio-ecological drivers of weight stigma in the PPP period. Here we use the term ‘community’ to refer to members of the general public from every walk of life regardless of their weight status; this ensures a comprehensive picture of the existing cultural values, norms, and attitudes with respect to body weight and weight stigma (Stangl et al., 2019).
Community members are a powerful and problematic source of weight stigma as stigma is normalised and reinforced by societal norms (Brown et al., 2022). This is perhaps explained by socio-cultural theory (Polivy and Herman, 2004), which emphasises the dominant influence of society and culture in shaping attitudes and beliefs. In particular, societal ideals and cultural norms that stress the importance of appearance and body size influence how body size is perceived and evaluated often leading to stigmatisation (Nutter et al., 2021; Polivy and Herman, 2004). Understanding community members’ views, beliefs, attitudes, and perceptions about body weight therefore has critical implications for our understanding of societal weight stigma and informing tailored interventions. Across the literature on the pervasiveness of weight stigma (Puhl et al., 2021), to our knowledge, we conducted the only study from the perspectives of community members and found that, from cross-sectional data, community members held explicit and implicit weight bias and stigmatising attitudes towards PPP women living in larger bodies (Hailu et al., 2025). Yet, an in depth understanding of participants’ insights to complement the quantitative findings is essential. This gap in evidence may partly explain why weight stigma in community settings is seldom challenged by research and policy.
Given that weight stigmatising attitudes and beliefs in community settings are complex and can be shaped by broader socio-cultural norms, a detailed exploration of perceptions, insights, and existing norms surrounding women’s body weight is needed. Furthermore, given the unique susceptibility and experiences of weight stigma for PPP women, specific attention to community perspectives is important to contrast from general weight-related attitudes and beliefs. Therefore, this study explored community members’ perceptions of women’s body weight during the PPP periods, focussing on weight stigma, societal norms, attitudes, and beliefs regarding weight and body size.
Methods
We used qualitative research methods to address the aim and reported the findings per the Standards for Reporting Qualitative Research (O’Brien et al., 2014; Supplemental File section 1). In this study, the terms preconception, pregnancy, and postpartum broadly refer to the periods before conception, during pregnancy, and following childbirth, respectively, and are used to frame the exploration of weight stigma across these distinct periods.
Ethical statements
This study was approved by the Monash University Human Research Ethics Committee (approval no. 36876) on October, 26, 2023. Written informed consent was obtained from all the participants.
Participants and recruitment
Members of the community or general public aged 18 years and older, who could read, write, and communicate in English, and who resided in Australia were eligible. Participants were ineligible if they had no access to the internet and a device such as a mobile phone or computer, or were unable to provide informed consent. A convenience sampling technique was used to recruit individuals based on their availability and willingness to participate. Interviews were conducted until no new information or themes were observed and data saturation was reached (Hennink and Kaiser, 2022). The final sample size of 20 was therefore determined based on data saturation, aligned with evidence indicating saturation can be reached between 9 and 17 interviews (Hennink and Kaiser, 2022). Potential participants were recruited via advertisements using flyers on social media such as Facebook and X (formerly Twitter), and public places such as libraries and Shopping Centres in in Melbourne, Australia. Interested participants scanned the QR code or clicked a link to access the explanatory statement containing the aim of the study and participation details and then completed the consent form. Individuals who fulfilled the inclusion criteria and provided their informed consent and email addresses were contacted to schedule an interview at their convenience. All participants received AUD$30. Recruitment occurred between November 2023 and January 2024.
Data collection
Semi-structured interviews were conducted via Zoom (Zoom Video Communications Inc, 2024) and lasted 20–50 minutes (mean = 33). The interviews were conducted by PhD students (HH, MD) or a research assistant (HK), all with research expertise in weight stigma, experience conducting interviews and after receiving training in qualitative research and interview methods. To minimise bias, a piloted semi-structured interview guide was used by all the interviewers. The first three interviews served as a pilot to assess language, clarity, question flow, and unforeseen issues. As no modifications were required following the piloting of the interview guide, the data from these interviews were included in the final analysis (Ismail et al., 2017). Additionally, the interview guide incorporated open-ended probing questions and clear instructions to promote consistency across interviewers and reduce interviewer bias. This included guidelines for interviewing, examples of supportive comments, and background information on ethical interviewing, such as an exercise to reflect on one’s own biases, all of which were consistently utilised by the three interviewers. All interviews were conducted exclusively in English due to resource constraints. All interviews were audio recorded using the Zoom recording function and transcribed verbatim using otter.ai (Otter, 2024). The transcripts were cross-checked with the recording for accuracy by HH. Transcripts were not reviewed by participants to avoid introducing bias (e.g. social desirability bias) after reflecting on and potentially wanting to change responses, as well as to minimise additional burden. A semi-structured interview guide, with eight open-ended questions and probing prompts, (Supplemental File section 2) solicited demographic information and delivered questions designed to elicit participants’ own views and reflections on societal perceptions of body weight, weight stigma, and societal norms pertaining to PPP women. The interview guide was developed based on prior literature (Faucher and Mirabito, 2020; Hailu et al., 2024; Hill and Incollingo Rodriguez, 2020; Incollingo Rodriguez et al., 2020) and input from researchers and Lived Experience Experts, including the steering and advisory groups of an Australian Research Council (ARC) Discovery Project Grant (DP220101107). Contributors had expertise in weight stigma, maternal health, public health policy, body image, and health psychology. Personal details mentioned during the interview were removed from the transcripts to protect confidentiality.
Data analysis
Reflexive thematic analysis was used to analyse the data (Braun et al., 2023). This method offers an accessible and theoretically flexible approach to comprehensively identify, analyse, and interpret the meaning in the data (Braun et al., 2023) and therefore was appropriate. We followed Braun and Clarke’s six-step analysis process to develop themes inductively (Braun et al., 2023; Byrne, 2022). In step 1, HH did data familiarisation and immersion via reading and re-reading of the transcripts and listening to the recordings. In this phase, the researcher attained in-depth contextual understanding of the data and noted initial observations and insights. In step 2, labels or codes related to our research questions were rigorously assigned to the data to capture the meaning in the data. This was applied to the entire data set in numerous rounds by the first author with ongoing debriefing and discussion with the senior author. NVivo software (QSR International, 2024) was used to code all transcripts. In step 3, HH, BH, and ACIR identified the patterns of meaning across codes and categorised the codes into initial potential subthemes and themes. This process was supported by using an online data visualisation platform, Mural (Mural, 2024) that facilitated the categorisation and depiction of relationships between codes and identification of main ideas, potential subthemes, and themes. In step 4, HH, BH, and ACIR held several online and in-person meetings with the author team to discuss the coding and potential themes and whether the themes accurately reflect the codes and the overall meaning in the dataset. At this stage, some subthemes were compiled and themes were refined. Following this, in step 5, themes and subthemes were discussed, defined, and named from the codes following wider team discussions and feedback. At this stage the themes were clearly defined reflecting the story of the data along with establishing distinctiveness and clear relationship between each theme. Finally, in step 6, the report (manuscript draft) was produced with careful refinement of the themes to tell the overall analysis story. This has been done by depicting the narrative of each theme per the study objective, supporting it with relevant data, and presenting the overall findings with contextual basis in the existing literature.
Reflexivity statement
Reflexivity is the self-appraisal of how one’s social position and personal experiences influence the research process and outcomes (Berger, 2015). All researchers identify as women and are experts in public health. The senior author (BH) self-identifies as having moved from a weight-centric approach to women’s health research to a weight-inclusive approach while applying a pragmatic lens to address weight stigma amongst real world problems. Also, all interviewers would like to acknowledge that they do not identify as living in larger bodies and are aware of their positionality as an ‘outsider’ to this experience; interviews and analyses were conducted primarily from an ‘outsider’ perspective. Also, some of the authors have children and have had the experience of being preconception, pregnant, or postpartum women. Despite being mindful to remain objective when interacting with the participants and conducting analyses, we acknowledge that we may not understand the depth of weight stigma from a lived experience perspective. However, the interviews focussed on the perspectives of community members, which often takes an ‘outsider’ perspective. Furthermore, a reflexive journal was kept by the first author who was present through each step of the study. The first author documented the team reflexivity, reflections during each interview, and data analysis steps to make sure the findings were not influenced by researcher beliefs and assumptions.
Trustworthiness
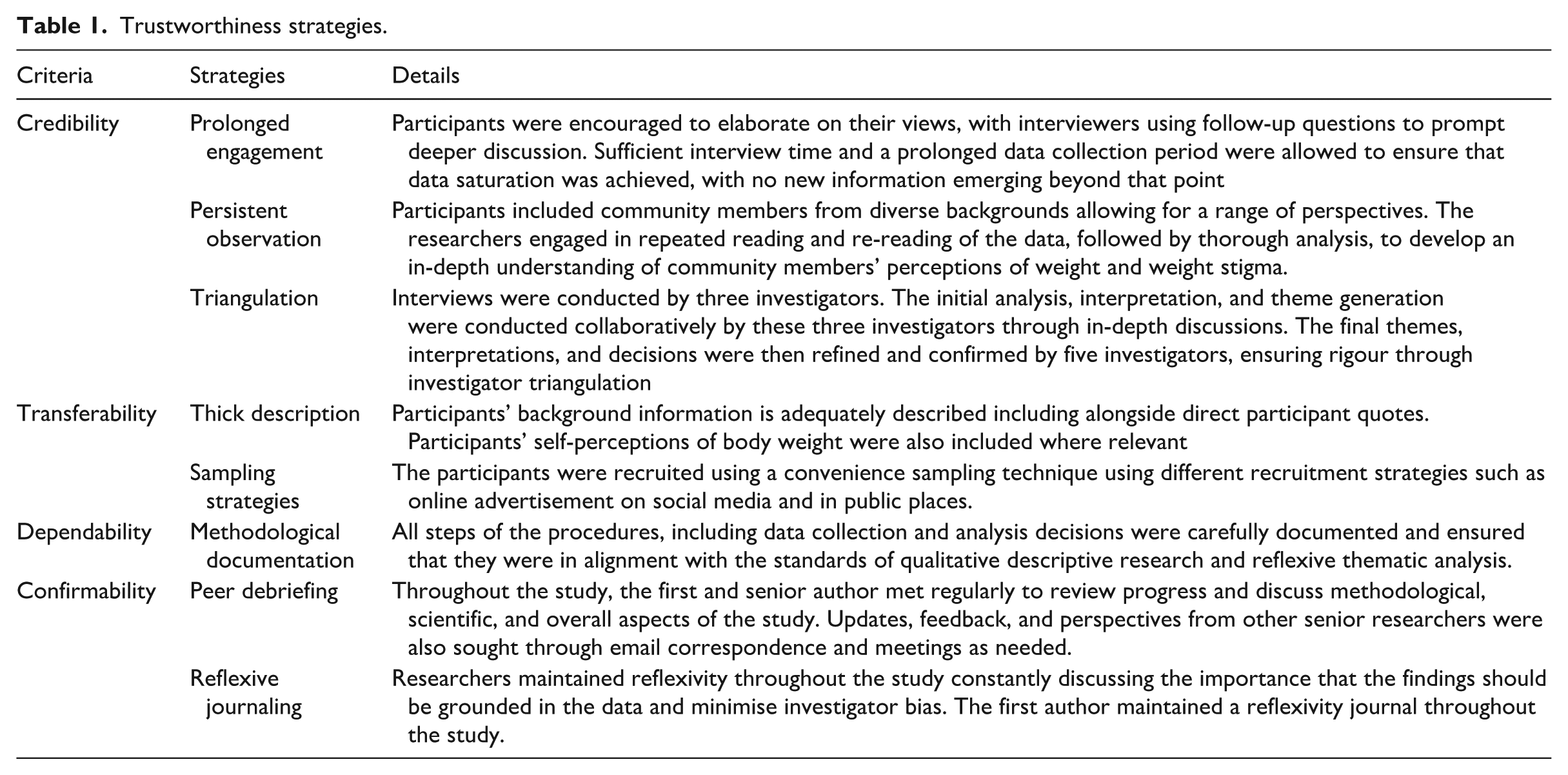
We sought to ensure our research was trustworthy using the key criteria of credibility, transferability, confirmability, and dependability (Table 1; Ahmed, 2024; Korstjens and Moser, 2017).
Trustworthiness strategies.
Results
Participant characteristics
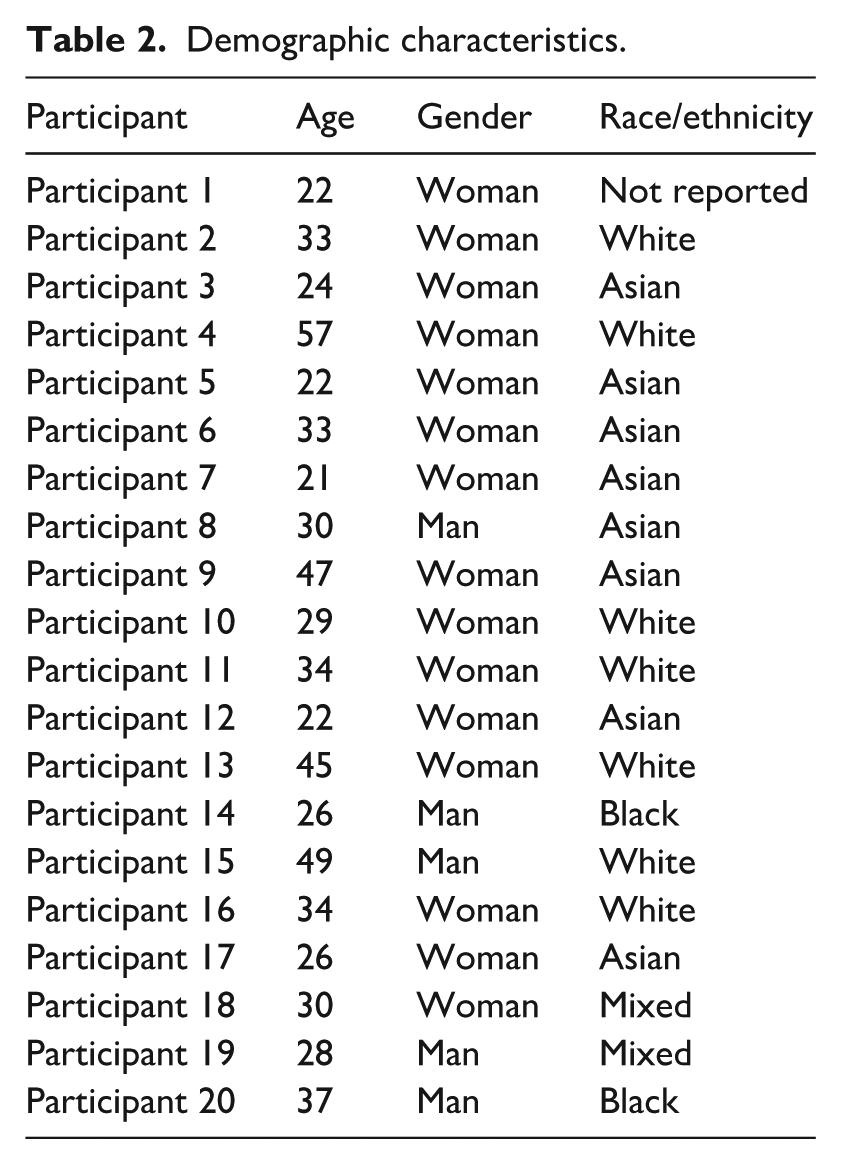
We interviewed 20 participants who were 32.5 ± 10 years old (range: 21–57; Table 2). The majority of the participants identified as women (n = 15), Asian (n = 8), and white (n = 7). While we did not collect quantitative data on participants’ body weight self-perception, almost all described their own body weight or size during the interview; this information is reflected in quotes where pertinent. We also did not collect data on participants’ experience of pregnancy or parenting, but this emerged in nine interviews.
Demographic characteristics.
Themes
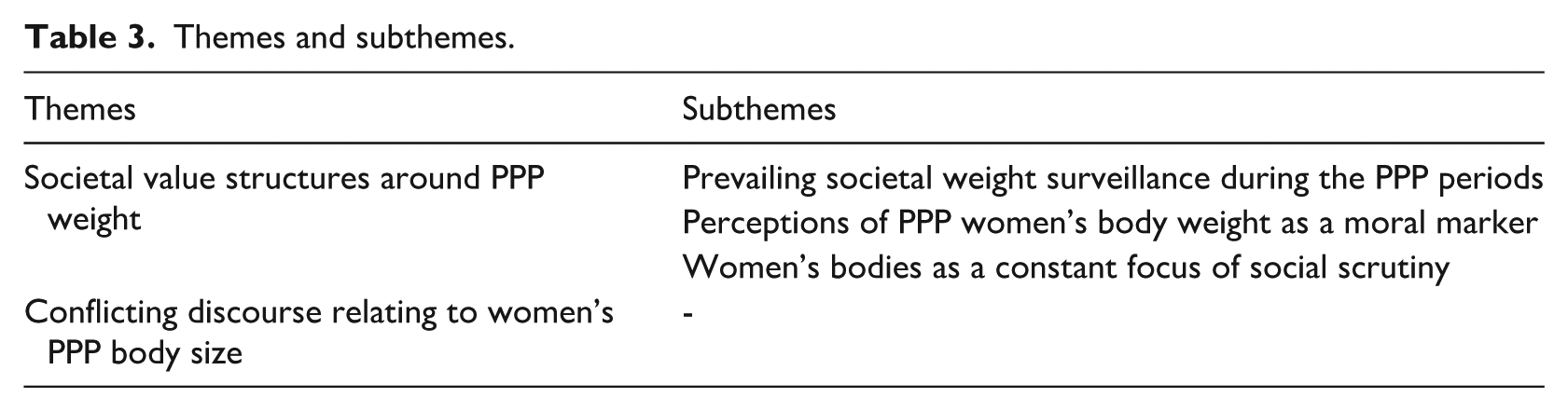
Two themes, with three subthemes on the first theme, were generated during analysis that encompassed participants’ perceptions and societal norms of women’s body weight during the preconception, pregnancy, and postpartum periods (Table 3).
Themes and subthemes.
Theme 1: Societal value structures around PPP weight
The first overarching theme ‘societal value structures around PPP weight’ describes the societal, and individual perceptions, beliefs, and norms regarding women’s body weight during the PPP periods. Overall, interviews revealed that women’s body weight held significant social value, with pervasive expectations for weight loss regardless of individual circumstances, prompting negative societal attitudes towards higher weight. This high value placed on thin body size for PPP women was explicated by the three sub-themes: (1) prevailing societal weight surveillance during the PPP periods; (2) perceptions of PPP women’s body weight as a moral marker; and (3) women’s bodies as a constant focus of social scrutiny.
Prevailing societal weight surveillance during the PPP periods
This subtheme illustrates the existing weight surveillance and expectations regarding the appearance of women’s bodies to be deemed ‘normal’ and hence ‘worthy’ of reproduction that is free of complications and is generally healthy. It emphasises the pressure placed on PPP women to lose weight and meet the socially valued thin body size regardless of where they are on the reproductive continuum and its physiological requirements. The participants narrated their own and societal expectations of women’s body weight across the transitions - before, during, and after pregnancy.
In preconception, participants felt that women are expected to avoid weight gain and, in many cases, to lose weight before conceiving. This expectation was perceived as a requisite in order to prepare their bodies for pregnancy and there is no justified cause for weight gain during this period. Participants also believed that losing weight helps prevent adverse outcomes such as infertility, reflecting the broader societal belief that equate larger bodies with poorer health. One participant mentioned: ‘. . .weight gain or body weight before pregnancy is controllable, especially if you are having or if you’re thinking to have a baby, I think you should definitely do something about it. You should maybe work on it before you get pregnant.’ (Participant 14, 26 years old, man, Black)
In pregnancy, all participants conveyed a belief that weight gain is inevitable for well-known reasons, such as the baby’s weight. However, the majority mentioned the prevailing expectation that women should ensure they conform to the recommended weight gain during pregnancy or avoid excessive weight gain. This expectation was understood not only as a means to minimise perceived health risks but also as a way to avoid societal judgement as to why they may have gained too much weight. When this expectation is unmet, society often provides lifestyle advice to women for controlling weight implying that amount and location of gestational weight gain is controllable. This was explicated in the following quote: ‘I think people expect some weight change to happen during pregnancy, like, that’s normal. But I think if you gain too much weight during pregnancy, then people. . . will view that negatively and be like, Oh, why she gained so much weight so quickly? So, people will definitely judge a woman’s body when she’s pregnant. Like they expect her obviously, to get a belly. But if she puts on more weight than that, I think people can be like, judgmental, and start giving tips (laughing) unsolicited advice about weight gain and pregnancy.’ (Participant 16, 34 years old, woman, White)
In the postpartum period, all the participants described that ‘bouncing back’ to pre-pregnancy body weight is challenging. Nonetheless, the majority felt that women should work to return to their ‘normal’ physical appearances and function as they did before pregnancy. Participants talked about returning to pre-pregnancy weight as ‘doable’ and that women ‘need to do it’. Further, the idea emerged that not only should women be able to lose weight, they in fact seek out excuses if they do not, highlighting the societal expectation for women to lose weight in spite of the reproductive phenomena happening in their lives.
‘. . .I think a lot of women blame being pregnant on their weight. . . I think they say, well, you know, I’ve gained weight during pregnancy and I can’t lose it, I tried all the diets and everything but maybe they haven’t really changed their lifestyle. And it’s easier to blame the pregnancy weight than to say, Okay, well, I’m not eating correctly, or, I’m not exercising or doing what I need to do.’ (Participant 4, 57 years old, woman, White)
While the majority of the participants felt that women should make an effort to ‘bounce back’ despite its difficulty, all participants acknowledged pervasive societal pressure for rapid postpartum weight loss. Generally, the consensus was that such pressures were mainly influenced by media and unrealistic standards from celebrities with postpartum weight loss resources. Some participants shared that such messaging perpetuates societal thinness ideals leading to an expectation for women to minimise weight or weight gain. Consequently, participants expressed that many women may feel compelled to adhere to these standards, sometimes prioritising thinness at the expense of their health.
Perceptions of PPP women’s body weight as a moral marker
This sub-theme unpacks the existing societal perceptions and stereotyping of women’s bodies that lead to association of larger bodies with moral failure. It emphasises the high value placed on thin body size and frames a higher body weight as a problem that needs to be solved. For PPP women, these negative stereotypes led to marking larger bodies as ‘unacceptable pregnant or reproductive bodies’ and thin as ‘acceptable pregnant or reproductive bodies’. Perceptions of larger body weight as a moral failure appears consistent across the various ethnic backgrounds and genders of our study participants. Participants discussed their perceptions of women’s body size/weight, highlighting general unacceptability of larger bodies in society. One participant explained ‘I think we don’t value larger bodies at all as a society’. (Participant 1, 22 years old, woman, race not reported).
The majority of participants mentioned the commonly held societal assumption that women living in larger bodies are unattractive, less healthy, lacking self-appreciation, and less competent, but some participants mentioned not necessarily believing this to be true. The participants felt this assumption promoted unfavourable treatment of women living in larger bodies, impacting how they are perceived and navigate daily life, as in the following quote: ‘I know that a lot of people also judge those women because they question their ability as mothers to be caretakers because it’s like, Oh, you’re so unhealthy. How are you going to raise a child or you’re so unhealthy, you’re going to make your child also unhealthy.’ (Participant 17, 26 years old, woman, Asian).
Not only were PPP women in larger bodies accused of moral failure, but the stigma and discrimination they faced was attributed to their own self-consciousness. This underscores the societal blame placed on PPP women both for their larger bodies and the weight discrimination they face. For example, one participant shared: ‘I think it would be more maybe the [women in larger bodies] themselves, lacking confidence in their bodies, or maybe not look the way they want to, so they kind of start to not go out as much or that kind of thing.’ (Participant 19, 28 years old, man, mixed race)
Women’s bodies as a constant focus of social scrutiny
This sub-theme illustrates that participants observed higher body ideal standards imposed on women compared to men, as evidenced by the constant scrutiny of women’s bodies and suggestions geared towards achieving thinness ideals. Participants mentioned that PPP women are subjected to more stringent body weight ideals or standards, including societal expectations for women to be smaller in size and occupy less space. One participant highlighted: ‘I think it’s probably worse for women because I think women were held to this really high standard of beauty standards anyway, you’ve got to be outstanding. . ., you know, there’s this huge, massive beauty expectation on women.’ (Participant 10, 29 years old, woman, White)
Participants noted that PPP women experience unique pressure to lose weight, often equated with becoming healthy, while men are not held to these expectations while preparing for parenthood. This is exemplified in the following quote: ‘. . .I think there’s extra pressure in some sense for [sic] obese women, to now suddenly become very healthy quickly, you know, because they have a child. But at the same time, for example, a father who’s like a smoker and has always been a smoker, I don’t see that pressure.’ (Participant 17, 26 years old, woman, Asian).
Also, participants mentioned that this societal expectation and pressure start at a very young age and persist throughout women’s lives. They further noted that they perceived women as a group have internalised these ideals, resulting in ongoing concerns about their weight and efforts to take corrective measures. One participant emphasised that these experiences are not only exclusive, but body size is often the first thing noticed and commented on for women: ‘Like, when I talked to my guy friends they just never had that happen to them, you know, like, a relative by pointing out Oh, looks like you gained weight or something like that. And just, so I feel like it’s kind of women’s experience. Like, specifically.’ (Participant 7, 21 years old, woman, Asian).
The overall narrative for this sub-theme suggests the pervasiveness of continuous dialogue and scrutiny of women’s body weight in society. This perspective is supported by the parallel and prevailing idea that thinness should be a woman’s goal for her to fit into any role she assumes in society.
Theme 2: Conflicting discourse relating to women’s PPP body size
This theme captures conflicting thoughts reported by participants regarding PPP women’s body weight. It emphasises the attitudes, beliefs, and assumptions held by participants (i.e. within the same participant and often within the same sentence) regarding PPP women’s body weight that were contradictory but simultaneous. These disparate but simultaneous narratives included: (1) the belief that body weight is determined by multiple factors versus individual responsibility to control weight; (2) being respectful versus using stigmatising language; (3) having versus not having feelings of sympathy or empathy based on weight loss attempts; and (4) the belief that PPP women should be treated fairly versus justification of negative treatment or stigmatisation.
Although the participants acknowledged that body weight is influenced by multiple factors including genetic, environmental, and medical factors, they reported a dominant narrative that it is mainly determined by behavioural factors, reflecting the internalised societal belief of individual controllability. Interestingly, this understanding was commonly presented when participants acknowledged genetic or medical causes of obesity while simultaneously expecting that women address this and achieve control of their body weight with active approaches to weight management. This was exemplified in the following quote: ‘I think potentially like eating more calories than you’re burning probably contributes more, but there’s obviously definitely people who have like medical issues that cause them to be [sic] obese and overweight, but I think calories in and calories out and the knowledge around that is probably what mostly causes people to be overweight or [sic] obese.’ (Participant 16, 34 years old, woman, White)
Similar discourse persisted regarding being respectful, or nonjudgmental, versus the use of stigmatising language. Although participants described that they do not condone the stigmatisation of women based on body weight, they used stigmatising words such as ‘obese’ or ‘grossly overweight’, as well as ‘othering’ phrases such as ‘those women’ and ‘such people’. This highlights the deeply ingrained and normalised nature of weight stigma in community settings. One participant mentioned: ‘I’m not a very judgmental person. I still don’t judge them [PPP women in larger bodies], but I just hope they’re aware. And they’ve done something about it.’ (Participant 14, 26 years old, man, Black)
Furthermore, conflicting discourse was observed when participants reported feelings of sympathy or empathy based on the assumption that women may have attempted to lose weight. This is conflicting because as it suggests that participants’ sympathy or empathy is conditional, extending only when women are perceived to have attempted weight loss, reflecting an underlying belief that moral worth is tied to weight control. This is highlighted by the following quote: ‘Well, I just feel for such people [women in larger bodies], because I’m sure they would be wanting to be like, skinny and slim, but they must also be trying to work hard doing exercises, and, you know, come from a diet, but if it doesn’t work, you know, I feel for them, because it’s not easy.’ (Participant 9, 47 years old, woman, Asian)
While the participants reported feelings of sympathy, pity, or empathy, the latter was primarily reported by those who self-identified as living in larger bodies, reflecting the importance of lived experience and advocacy. One participant who self-reported as living in a larger body mentioned: ‘I feel like I probably have heightened empathy, in the sense that I understand what it’s like and I know that it might not necessarily be because they’re lazy or if they have issues like I can appreciate those other issues going on’. (Participant 10, 29 years old, woman, White)
When asked about their perception of how women living in larger bodies are treated in society, participants mentioned that women are often treated poorly because of their body weight. However, some participants justified this societal reaction, suggesting that it stemmed from a perceived sense of care and concern aimed at encouraging women to become healthier. Notably, the terms ‘healthy’ and ‘losing weight’ were used analogously. The overall narrative implied that offering unsolicited advice or negatively treating PPP women will motivate them to lose weight. The following quotes exemplify this: ‘Well, I don’t think it’s [negative societal attitude] a necessarily negative thing because having a healthy weight is what everyone should aspire to. But certainly, people shouldn’t be bullied if they’re overweight. I mean as to how society should approach it, I think, society should promote a healthy weight because it [overweight or obesity] can cause a lot of problems in the long run.’ (Participant 6, 33 years old, woman, Asian) ‘. . .They [the society] want to change them [PPP living in larger bodies] positively.’ (Participant 3, 24 years old, woman, Asian)
Despite the above conflicting thoughts on societal treatment of larger bodied PPP women, the participants explained that women living in larger bodies should be treated with the same fairness and respect as others. Simultaneously, they noted the importance of additional support recognising their needs. One participant shared: ‘I definitely acknowledge there may be times where equity is more important than equality . . . For example, if you’re exercising, there might be things that someone in a larger body can’t do. . .So, I think equality is good until there’s those points where you know, treating someone with a bit of extra respect or support might actually provide that equity’. (Participant 10, 29 years old, woman, White)
Discussion
This is the first study to qualitatively explore community members’ perceptions and societal norms of weight stigma and women’s body weight during the PPP periods. The results of this study provide a unique and richly contextualised insight into prevailing societal norms as well as individual perceptions and beliefs regarding women’s body weight and weight stigma during the PPP periods from the firsthand perspective of perpetrators of weight stigma – community members. Two overarching themes generated from the participants’ own perceptions and recounts of societal perspectives were ‘societal value structures around PPP weight’ and ‘conflicting discourse relating to PPP women’s body size’. The societal value structures around weight were demonstrated by prevailing societal weight surveillance during PPP periods, and a perceptions of PPP women’s body weight as a moral marker. Conflicting discourse relating to PPP body size captured contradictory but often simultaneous thoughts reported by participants regarding the controllability of body weight, being respectful versus the use of stigmatising language, feelings of sympathy or empathy, and treatment of PPP women living in larger bodies. Our study adds to the literature by providing insight into both the societal value structure around women’s bodies from the rarely sought views of community members across the PPP periods and the most common areas of conflicting yet simultaneous beliefs about women’s bodies and weight stigma. Hence, our findings go beyond women’s self-reported experiences of weight stigmatisation to the first-hand views of weight stigma perpetrators.
Our findings indicate prevailing societal weight surveillance across the PPP continuum. We found this to be consistent with the perspectives shared by PPP women who have a lived experience of weight stigma (Dever et al., 2025; Hill and Incollingo Rodriguez, 2020). This finding is concerning given it implies that society holds the view that women have total control over their weight and can manipulate it as needed, which is not supported by scientific evidence, (Hailu et al., 2025; Westbury et al., 2023). Preconception, pregnant, and postpartum women not only experience this societal pressure and weight stigma but they tend to internalise it (Nagpal et al., 2022). Evidence indicates this internalisation can lead to engaging in unhealthy actions such as consuming unnecessary diet pills, starving behaviours, or vomiting/purging to try to lose weight (Himmelstein et al., 2018). These actions have significant health consequences for both the woman and their (potential) child including increased risk of gestational diabetes, postpartum depression, suboptimal breastfeeding outcomes, and avoidance of reproductive health services (Dieterich et al., 2022; Incollingo Rodriguez et al., 2019; Nagpal et al., 2021).
Given the high value that society often places on thin body size, PPP women with higher body weights were automatically labelled with negative stereotypes and framed as a problem that needs to be solved. Terms relating to higher body weight were used interchangeably/equivalently with ‘being unhealthy’. These stereotypes are consistent with the general weight stigma literature (Westbury et al., 2023). Our study further identified additional negative characterisation of PPP women, such as doubts about their mothering abilities and ‘mother blame discourse’, which refers to a perception that women are putting their child at risk because of their weight (Bombak et al., 2016). This negative stereotyping translates into inequities for larger bodied women in employment, healthcare, education, and daily interactions. Furthermore, it also impacts weight stigma intervention efforts because it creates the misperception that it is the ‘women in larger bodies’ that need to be targeted for change and not the community that is perpetrating weight stigma (Westbury et al., 2023).
Moreover, by bringing the community’s perspectives, our findings confirmed commonly held beliefs previously reported by victims that women are held to higher thin body ideal standards compared to men and are disproportionately affected by weight stigma (Selensky and Carels, 2021). Body ideals for women are a standard by which all women are evaluated against and judged. Men, on the contrary, are allowed more flexibility in body size, and ideals trend to muscularity rather than thinness (Leopold, 2025). These body weight ideals apply to women regardless of their age or reproductive milestones, despite the fact that reproduction is known to contribute to further weight gain and impose unrealistic expectations on women (Rodgers et al., 2024). Further consequences include negative body image and eating disorder symptoms which are also associated with an increased risk of psychosocial and physical health problems and increased economic cost to society more broadly (Gilmour et al., 2025; Streatfeild et al., 2021). In addition to impacting women’s health, weight stigma also affects women socioeconomically due to discrimination in employment and educational settings (Sohier et al., 2025). This cumulative disadvantage likely contributes to poor quality of life and poverty with overall economic and public health implications (Lawrence et al., 2022; Westbury et al., 2023).
Our study indicated the presence of conflicting and yet simultaneous thoughts and beliefs regarding body weight, weight stigma, and related issues. The conflicting belief held by community members about the controllability of body weight is problematic. This is because the belief that body weight is under an individual’s control is the strongest predictor of negative attitudes and weight stigma towards people living in larger bodies (Luck-Sikorski et al., 2017). Our finding has an implication that mere awareness of environmental and genetic causes of body weight may not suffice to improve one’s beliefs and decrease weight stigmatisation, as there are many nuances involved in changing and maintaining beliefs and behaviours (Ajzen, 1991; Kwasnicka et al., 2016). Furthermore, the fact that participants mentioned that they are not judgemental towards PPP women in larger bodies while simultaneously engaging in stigmatising discourse may perhaps indicate that the participants are harbouring implicit weight bias (inherent biases or stereotypes that are unconsciously activated (Elran-Barak and Bar-Anan, 2018). At the same time, conflicting discourses may suggest the beginnings of a shift in societal attitudes, from overtly biased and stigmatising, to incorporating more equitable attitudes. This may indicate the growing awareness of the harms of weight stigma and potential early stage readiness signals for change.
Evidence of all these components is useful in considering theoretical guides for interventions aimed at curtailing stigmatising behaviours. For instance, The Theory of Planned Behaviour posits that subjective norms or beliefs, attitudes towards the behaviour, and perceived behavioural control influence behavioural intention and change (Ajzen, 1991). This may suggest that weight stigma interventions that target perpetrators’ stigmatising behaviours may need to incorporate strategies that shift subjective beliefs or norms and attitudes in addition to awareness creation. Additionally, empathy generally has been reported to alter negative stereotypes towards individuals living in larger bodies and empathy evoking has been considered a weight stigma reduction strategy (Talumaa et al., 2022). In our study, we primarily found feelings of pity or sympathy, which were based on a precondition that PPP women living in larger bodies had attempted to lose weight but were unsuccessful. The exception to this was empathy in those who have experienced living in a larger body. Hence, pity and sympathy may not effectively reduce weight stigmatisation because, even though well-intentioned, they may reinforce othering, facilitate inferiority, and negatively impact the self-esteem of the people experiencing stigma (Murray et al., 2024).
One of the main strengths of our study is that participants from relatively diverse ethnic backgrounds and age groups took part. However, most of our participants were women which may be attributed to the difficulty of recruiting men for qualitative studies (Onyeze-Joe and Godin, 2022). This challenge may be even greater in studies focussed on weight and/or PPP women. This lack of gender diversity might limit our full understanding of the perception of other gender groups, albeit we did find similar views across the men and women interviewed. Furthermore, data collection was guided by concurrent reflexive thematic analysis, which allows for the recursive development of themes interactively throughout the interview process. In terms of limitations, it is possible that individuals with a specific interest in the study topic were more likely to respond to the advertisement, potentially limiting the diversity of views. Furthermore, participant responses might have been influenced by the interview guide given the socially complex nature of weight stigma, despite the guide being carefully designed to be neutral and having undergone piloting. Also, in our study, given the sensitive nature of the issue of weight stigma, we did not ask participants if they perceived themselves to be living in a larger body. This protocol allowed participants to express their opinions without feeling negatively judged or pressured. However, some participants naturally disclosed their body size self-perception. Lastly, given data were collected over Christmas and New year period—often characterised by increased dialogue around food and weight, there is a chance that participants responses might have been influenced by seasonal attitudes despite the interview’s focus on broader societal norms and weight stigma towards PPP women.
Conclusion
This study is the first to provide qualitative insight into community members’ perspectives of women’s body weight, societal norms, and weight stigma across reproductive years—that is, those who commonly perpetrate weight stigma. We found disproportionately high value placed on women’s weight, manifesting through continuous surveillance of PPP’s body weight regardless of reproductive milestones and overall acceptability of higher body weight as marker of moral failure. Also, the study highlights common conflicting and simultaneous beliefs regarding PPP women’s body weight and weight stigma held among community. Characterising perpetrator perceptions enhances our understanding of specific social and cultural norms and beliefs that perpetuate weight stigma in community settings. By doing so, it underscores a needed shift in responsibility away from PPP women living in larger bodies to challenge existing norms and stereotypes. Furthermore, targeting weight stigma in the community setting has potentially far-reaching advantages due to its tendency to influence other societal domains such as employment, healthcare, and media settings. Generally, our findings have implications for future research and policy to identify strategies that address not only the intentional but also the inherent stereotypes, beliefs, and weight stigma towards PPP living in larger bodies. As such, it will ultimately contribute to the improvement of health and social wellbeing of PPP women and their children.
Supplemental Material
sj-docx-1-jes-10.1177_13591053251404190 – Supplemental material for Australian community members’ perceptions of women’s body weight, societal norms and weight stigma towards preconception, pregnant, and postpartum women: A qualitative study
Supplemental material, sj-docx-1-jes-10.1177_13591053251404190 for Australian community members’ perceptions of women’s body weight, societal norms and weight stigma towards preconception, pregnant, and postpartum women: A qualitative study by Haimanot Hailu, Angela C. Incollingo Rodriguez, Helen Skouteris, Michelle Dever, Helia Khalesi and Briony Hill in Journal of Health Psychology
Footnotes
Acknowledgements
The authors sincerely thank all the participants for taking part in this study.
Ethical considerations
This study was approved by the Monash University Human Research Ethics Committee (approval no. 36876) on October, 26, 2023.
Consent to participate
Written informed consent was obtained from all the participants who took part in the study.
Consent for publication
Written informed consent was obtained from all the participants to have the findings published.
Author contributions
Conceptualisation: HH and BH; Methodology: all authors; Analysis: all authors; Writing–original draft preparation: HH; Writing–review and editing: all authors; Supervision: BH, ACIR, and HS. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by an Australian Research Council Discovery Project grant (DP220101107). HH acknowledges MGS and MITS scholarships from Monash University. BH is funded by an Australian Research Council Discovery Early Career Researcher Award (DE230100704).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study’s findings are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.