
Abstract
Neonatal hypoglycaemia is the primary metabolic disorder affecting newborns. It has severe implications including cerebral injury when left untreated. Pacific newborns have the second-highest prevalence of risk factors for hypoglycaemia amongst all ethnic groups in New Zealand, and therefore disproportionately suffer its effects. However, Pacific voices remain largely unheard regarding experiences with at-risk infants. This qualitative study aims to amplify Pacific families’ stories. Nine interviews involving ten participants were transcribed and analyzed. Seven central themes were revealed: Teu Le Vā: Nurturing relationships by healthcare professionals, Complex circumstances, Family decision-making, Talanoa: Culturally congruent information sharing, Cultural beliefs related to medical care in pregnancy, Relevance of faith and spirituality, and Continued follow-up. The findings of this study highlight the pivotal role of healthcare professionals in nurturing Vā or relational space and underscore the necessity of culturally responsive practices to improve Pacific families’ experience of neonatal hypoglycaemia care.
Introduction
Hypoglycaemia is the most common metabolic disturbance of newborns (Abramowski, 2019). Of healthy infants, 39% will have one or more episodes of hypoglycaemia in the first five days after birth (Harris, 2020), and up to 50% of infants with recognised risk factors will develop hypoglycaemia (Harris, 2012).
Hypoglycaemia can lead to cerebral injury in babies if left untreated (Burns, 2008; Cornblath, 2000; Lucas, 1988; Rozance, 2016. Regular blood glucose monitoring, usually by repeated heel-prick blood testing, is recommended for those at risk to allow early detection and treatment. Babies experiencing hypoglycaemia not corrected by first-line treatment (increased feeding and dextrose gel rubbed inside the cheek) are usually admitted to the neonatal intensive care unit (NICU) for further therapeutic intervention, usually intravenous dextrose administration (a glucose drip) (Newborn Services Clinical Practice Committee, 2024). This results in separation of the baby from the family and can make establishment of breastfeeding more difficult.
There are no data about how families of babies born at risk of hypoglycaemia respond to and experience this care pathway in Aotearoa New Zealand. In particular, the voices and perspectives of Pacific families (kāinga/whānau/aiga/vuvale) have not been sought to guide management. Pacific peoples are disproportionately affected by risk of neonatal hypoglycaemia. An Aotearoa study found that 32.1% of neonates eligible for hypoglycaemia screening were born to Pacific mothers, the second highest amongst all ethnic groups studied (O’Brien, 2023).
The development of a national Aotearoa New Zealand guideline for management of neonatal hypoglycaemia is in progress. To ensure that this guideline will be appropriate and culturally responsive to the needs of all communities, we undertook this qualitative study to better understand Pacific families’ experiences of having a baby born at risk of hypoglycaemia. The findings of this study will be used to inform the panel, of which some authors are members, as they develop the guideline recommendations. We explored the experiences of Pacific families on receiving the news that their baby was at risk, as well as their encounters with detection, prevention, management, and follow-up processes.
Methods
This study was conducted between August and December of 2023 and is reported using the COREQ checklist for qualitative research (Tong, 2007) (Supplemental material 1).
Participant recruitment
Potential participants comprised families of children enrolled in the hypoglycaemia Prevention with Oral Dextrose (hPOD) trial between January 2015 and May 2019. The hPOD trial was a multicentre, double-blind randomized controlled trial designed to evaluate the efficacy of oral dextrose gel for the prevention of neonatal hypoglycaemia among infants deemed at risk (preterm, small or large birthweight, or infant of mothers with diabetes) (Harding, 2015). All potential participants had children who had participated in the follow-up assessment at 2 years of age, and some in the second assessment at 6–8 years, and had previously given consent for further contact for future research. Families of children or mothers who had died since enrolment in the hPOD study were not contacted.
Our intention was to ensure a diverse sample by recruiting participants from different Pacific Island nations, birth hospitals, and neonatal hypoglycaemia risk groups. Initially, eligible individuals were contacted via email (if address available), followed by a phone call or text message. Several eligible individuals were contacted by phone due to a preexisting relationship with a study team member (JR). The participant invitation email was written in English with translation of the opening greeting and some terms (e.g. neonatal hypoglycaemia) to Tongan or Samoan to acknowledge the family’s native language and to foster a sense of warmth and rapport. The email reminded the participants of their previous involvement in the hPOD trial and explained the purpose of the contact. Information about the study was provided through a shared link in the email, which included the participant information sheet containing study aims, participation, withdrawal process, data management protocols, and the research team. Recruitment ceased once data saturation was reached (i.e. few novel codes introduced with additional interviews), as agreed between study team members involved in data analysis (JR, KOG, OW, LR).
Data collection
Participants were offered the option of an interview in-person at our offices in Grafton, Auckland, online via Zoom, or by telephone. Although the mother served as the primary contact, other family members were invited to participate. Where multiple family members participated, they were interviewed together, but were asked to provide individual consent. A koha (voucher) was given to each individual family member who participated to recognize the gift of sharing their lived experience for the study. Additional reimbursement was offered for parking and travel costs.
Interviews lasting 25–60 minutes were conducted by one or two members of the study team (JR, KOG, OW) who facilitated a conversation based on semi-structured interview questions (Supplemental material 2). The questions aimed to address families’ experiences with discovering their child’s risk of neonatal hypoglycaemia, along with associated testing, treatment, and follow-up processes. Employing a Talanoa-style approach empowered participants to take control over their shared story and perspective on pertinent study topics. The interview team was exclusively female with diverse qualitative research and clinical experience: medical student, medical specialist in Obstetrics and Gynaecology, and registered nurse with experience in qualitative research.
Data analysis
Interviews were audio-recorded and transcribed verbatim. Participants were invited to review their transcripts before analysis.
A qualitative content analysis process was used (Hsieh, 2005). Deidentified transcripts were imported into NVivo software (QSR, release 14.23.2 (46)) for coding. Two researchers (OW, LR) independently coded each transcript, reaching consensus through discussion. At least one additional investigator (JR, KOG) with expertise in Pacific culture reviewed the coding.
Codes were then iteratively organized into themes by the analysis team (OW, LR, JR, KOG). The frequency of similar ideas or sentiments among participants was quantified as: “few” for 1-2; “some” for 3-4; “half” for 5-6; “most/the majority” for 7-9; “all” for 10. Verbatim quotes were used to exemplify participants’ expression of identified themes.
Ethics statement
Ethical approval was granted by the Auckland Health Ethics Committee (AH25449). Written informed consent was obtained from participants, who also received compensation for their time and expenses, with the option to withdraw (self and data) at any time.
Results
Characteristics of participants
A total of 65 participants were invited to participate, of whom 53 (82%) did not respond and two ceased contact with the study team and were therefore not interviewed. Ten parents (nine mothers and one father) of nine infants at risk of hypoglycaemia participated in nine interviews. The participants identified as Samoan (4), Tongan (4), and Cook Islander (1). One mother who identified as NZ Māori and married to a Samoan man, was also included to represent a bicultural whānau. Infants (six girls and three boys) were born at Auckland City Hospital (8) and North Shore Hospital, Auckland (1). The most common reason for risk of neonatal hypoglycaemia was a mother with diabetes in pregnancy (six participants), with two having a low birthweight and two a high birthweight baby.
Seven themes emerged from the experiences of the participating kāinga/whānau/aiga/vuvale (families): (1) Teu Le Vā: Nurturing relationships with healthcare professionals, (2) Complex circumstances, (3) Family decision-making, (4) Talanoa: Culturally congruent information sharing, (5) Cultural beliefs related to medical care in pregnancy, (6) Relevance of faith and spirituality, and (7) Continued follow-up.
We used the Seitapu Framework of Cultural and Clinical Competency to inspire the visualisation of the above themes and how they interconnect (Agnew, 2004; Ioane, 2017) (Figure 1). This framework was developed to support Pacific and non-Pacific staff working with Pacific peoples (Agnew, 2004).
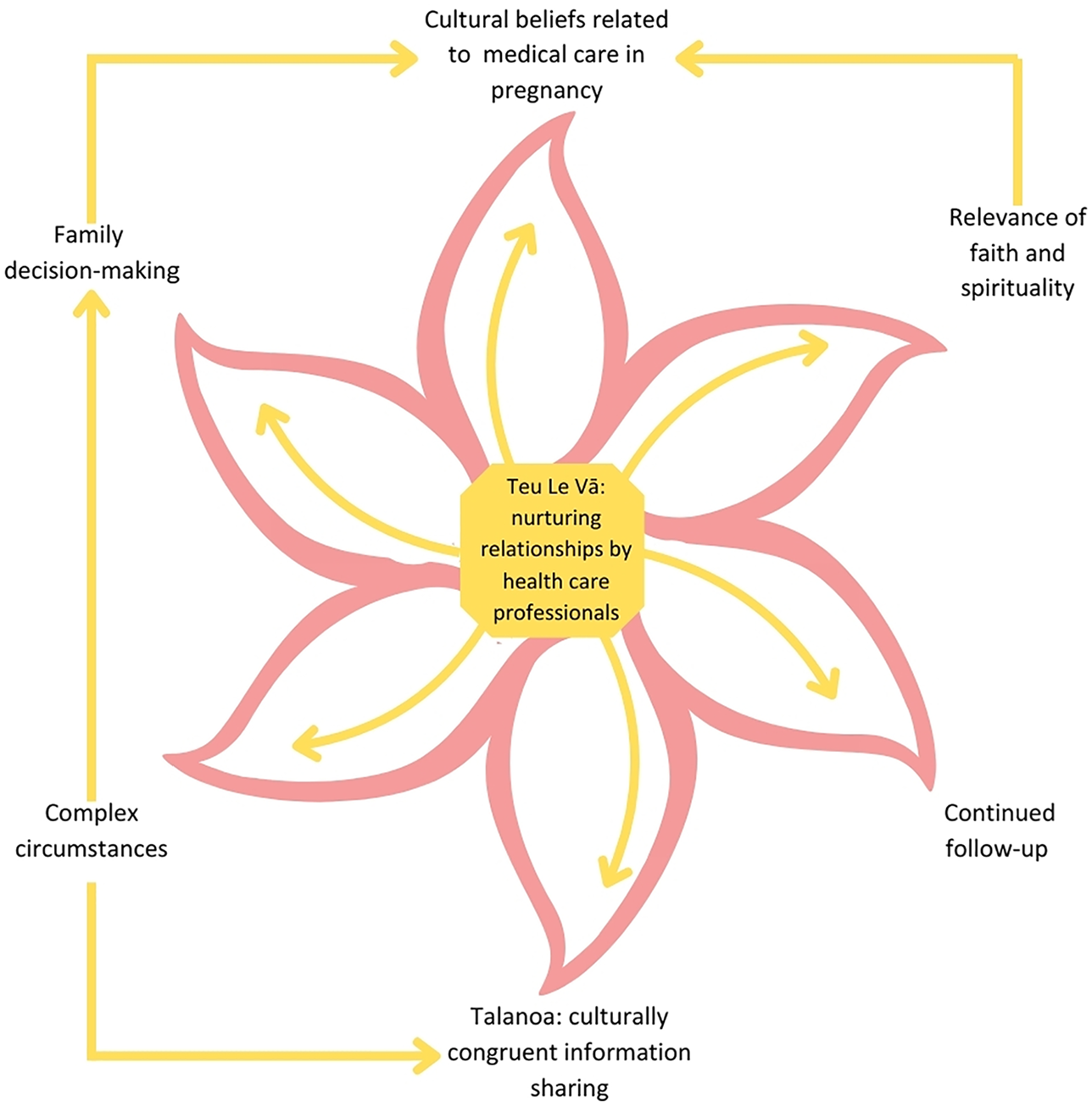
Key Themes depicted as inspired by the Seitapu framework (Agnew, 2004; Ioane, 2017).
Teu Le Vā : Nurturing relationships by healthcare professionals
The central theme in all stages of the neonatal hypoglycaemia care pathway was Teu Le Vā (nurturing relationships), placed at the core of all themes (Figure 1). Despite difficulty in recalling the whole hypoglycaemia journey in detail, families consistently emphasized the importance of their relationships with healthcare professionals.
Many spoke very highly of healthcare professionals: The care was amazing, and I’m so grateful…I was just so impressed with all the service of [name of hospital] like. It was gold star, in my opinion, like nothing could have been better – Mother with diabetes in pregnancy I think kudos to the to the midwives or nur- midwife nurses of Auckland. They’re really good. From my experience. – Parent of low birthweight baby
Despite several years since the baby’s birth, all participants vividly remembered healthcare professionals who gave their time and demonstrated genuine loving care, highlighting the importance of healthcare professionals nurturing Vā (relationships) with families.
But that that’s their love and their supporting for my daughter – Mother with diabetes in pregnancy
Most families felt their midwives nurtured relationships well. For most, their midwife was the primary informant about hypoglycaemia risk and crucial in providing emotional and practical support, sometimes across multiple pregnancies.
Yeah, because when my midwife tell me about that at that time I was crying, and then lucky because she stayed there and then… give me a hug and then just say, I’m gonna be alright. – Mother with diabetes in pregnancy
Most participants preferred carers who they trusted. A few women preferred care provided by their general practitioner due to an existing relationship.
I didn’t have a midwife, and that was by choice – Parent of low birthweight baby
The predominant reason for families reporting overall negative experiences of their hypoglycaemia journey was healthcare professionals not investing time to nurture Vā.
Yeah. just talk to me and explain it to me rather than just keep me in the dark with the whole thing… – Parent of high birthweight baby
This also applied to staff recruiting for the hPOD trial. One mother expressed extreme discomfort sharing her and her baby’s space with unfamiliar staff after the birth without any prior rapport building. The intrusion was viewed as disrespectful, given the sanctity of the space.
And you had no idea who it is, too. So, it’s like, you know. I don’t really want you in the room. I have no idea who you are. Parent of high birthweight baby
Complex circumstances
This theme encompassed all aspects of the hypoglycaemia journey. Most interviewed women described encountering some form of complex circumstance that affected them at various stages such as medical diagnoses in pregnancy (diabetes), Down syndrome risk, or previous gastric bypass surgery.
I had something a little bit different, I guess, in my case where I had diabetes, and I had a gastric bypass – Mother with diabetes in pregnancy Oh, your child is gonna be born with Downs syndrome – Parent of high birthweight baby
The most prevalent complex circumstance affecting half the interviewed mothers was diabetes in pregnancy. A few reported that their family struggled because the mother was recommended a Eurocentric dietary plan to manage her diabetes, without acknowledgement of Pacific food culture or involvement of the whole family. This often meant mothers were encouraged to eat foods they did not like while deviating from their family’s diet, and required additional preparation time. One father remembered being advised that the mother’s dietary change was for the benefit of baby’s health.
Because for us when we wake up in the morning we can for our breakfast we can eat the leftover food from yesterday, but here is the… cause I can’t tell her the truth, that I wake up in the morning, and I just eat food in the morning for breakfast, but she could tell me, just have two toasts brown bread with porridge or weetbix – Mother with diabetes in pregnancy It’s really hard cause… she wants to eat the food she liked, but what the midwife said, it’s not good for him, for the baby. So, it’s kind of hard because we got our food made already prepared for us. We have to make another food for her even though she doesn’t like it – Mother with diabetes in pregnancy
Some experienced complications after the birth (including epidural effects, infant tongue tie and postpartum haemorrhage). A few expressed distress when complications prevented immediate contact with their baby.
I was quite sick. I had lost a lot of blood with her. So yeah, I didn’t get to see her till the night – Mother with diabetes in pregnancy
Complex circumstances arose where family members could not provide support. Some resided in the Islands, and others were dealing with other family medical issues. Consequently, some mothers felt much needed family support was lacking during childbirth.
He (baby’s father) was having surgery um heart surgery as well – Mother with diabetes in pregnancy
Some participants reported these complex circumstances led to a renewed sense of gratitude, in that they were simply thankful for the birth of a live baby.
I’ll be just grateful if we can all survive this, it will be okay – Mother with diabetes in pregnancy
Poor access to hospital negatively impacted the experience of some, making engaging with care difficult and stressful.
When it was really difficult to find parking, but I needed to be there for the appointment. It was just a whole bunch of stuff that was happening around me - Mother with diabetes in pregnancy
Easy access to the hospital for follow-up visits enhanced mothers’ willingness and ability to actively engage in appointments, resulting in a more positive overall experience.
It just happened to be I worked in the city, so I worked 5, 10 min away from the hospital where all my appointments were so… but actually everything worked out well. Wasn’t much of an inconvenience. But yeah, regular appointments. But I didn’t mind. - Parent of low birthweight baby
Family decision-making
Some participants felt unable to share the decision-making with their husbands or extended family and struggled with the sole responsibility of making final decisions during baby’s hypoglycaemia journey. This was exacerbated by mothers feeling separated from important family supports (eg residing on their home island).
She (Grandmother) is in Samoa – Mother with diabetes in pregnancy Yeah, especially Dad as well, I think [husband], he also was overwhelmed with everything that was going on, but I usually take on the… information – Mother with diabetes in pregnancy
Some participants with a healthcare background or previous pregnancy experiences felt comfortable with their own decision-making.
I learned from my first one – Mother with diabetes in pregnancy I think because I have a health background. Um I it was easy for me to understand – Mother with diabetes in pregnancy
For others, not involving their family in decision-making put significant strain on relationships with other family members, particularly between husband and wife, mother and daughter. A few participants took full responsibility for information about their child’s risks to avoid burdening their partner or family.
It’s so hard at that time… I just keep it to myself, because how he’s working…. I don’t want him to be. I just want him to be focused on his work. So, it’s just I didn’t tell him straight away. – Mother with diabetes in pregnancy
Some participants suggested that healthcare professionals should offer to involve the wider family to share the responsibility for decision-making. Many reported their family’s unfamiliarity with neonatal hypoglycaemia, stating that the family would have benefited from knowing how they could provide support and be involved in the treatment, prevention, and post-birth care for better outcomes.
You go a little bit further, because for in terms of the dynamics and the logistics around the family. That is how that is the most important information of how everyone is going to, you know, arrange themselves or arrange the situation with the home to be able to match the information that you’re giving us, so that we can actually work effectively, efficiently and appropriately so that, you know we get the best outcomes for not just for me, as a woman, my baby, but also for my husband, and also because we’ve also got all the other children as well. – Mother with diabetes in pregnancy
Talanoa: Culturally congruent information sharing
The majority of participants were dissatisfied with adequacy of information sharing and this negatively impacted their experience of the neonatal hypoglycaemia care pathway.
Firstly, many felt that insufficient information was provided during pregnancy and in hospital for the birth.
A few mothers attributed avoidable confusion and heightened family anxiety to inadequate information about test results and the required treatment.
The result of that thing. I never get it, and nobody explained to me. what did they get? What’s the result they get out of it? – Parent of high birthweight baby
Several mothers still had unanswered questions regarding the purpose of testing, even years later. Few remembered why their baby was at increased risk of hypoglycaemia. This added more distress when their baby had to be tested multiple times.
Do they prick every Pacific Island baby or is just every baby? – Parent of high birthweight baby
A few mothers also felt that the implications for their child’s future health were not well explained.
Not fully as far as the future implications – Mother with diabetes in pregnancy
Secondly, the communication style of many healthcare professionals was not seen to foster trust or respect. Many participants perceived information delivery as dictatorial, leading mothers to feel overwhelmed and disempowered.
For me working with Pacifica people giving too much information is so overwhelming, and it can make the person feel really bad about the information that you’re giving, which is not the intention. But you know I can easily see how explaining the implications can be…um… like overwhelming – Mother with diabetes in pregnancy I feel like it was kind of forced. And it’s like, a non-negotiable thing. It doesn’t come across like it’s a choice – Parent of low birthweight baby I think it was just more the reassurance of like the baby’s not gonna remember it and trying to outline the advantages of why they get it done – Parent of low birthweight baby
A few participants suggested adopting a conversational, culturally acceptable approach such as Talanoa because this empowers people to ask questions and gain a clearer understanding of hypoglycaemia.
Interviewer: “I think I’ll just let you talanoa sometimes it’s the easiest way to do it” Participant: “Cool!” – Parent of low birthweight baby “It’s just been able to draw it out in a way that’s more like a conversation, so that it has meaning for me.. and the family receiving the information um rather than just a whole bunch of ideas as to how this could be implicated” – Mother with diabetes in pregnancy
A few participants felt information was provided in a set format, neglecting multiple perspectives of a Talanoa-style discussion. They expressed a desire for information sharing to be accompanied by reassurance, hope and optimism.
I’m quite optimistic. So, I’m not like. I think… I prefer not to hear bad news – Parent of low birthweight baby
Most participants stressed the need for effective information sharing throughout the hypoglycaemia journey, to facilitate families’ understanding. Some participants suggested that a “normal” test result still required a conversation to provide reassurance and understanding about the blood tests and implications for baby’s health.
If they say something happened, they should come back at the end and tell me, why … that’s not the result… why they were wrong – Parent of high birthweight baby
Thirdly, timing of provision of information was crucial. Many described difficulties recalling information about their baby’s risk and being asked to consent to treatment or research while drowsy from pain medications.
I can’t remember and I was highly drugged as well – Parent of high birthweight baby
Some participants proposed that information would be better accepted if delivered by a trusted health professional. A few participants expressed that it can be difficult for mothers to trust information from a stranger, as described in the Teu Le Vā theme.
I did not believe them. I tell my husband they are liars! - Mother with diabetes in pregnancy
Importance of receiving information with support from family and friends
Some mothers reported that fathers were not always present when they were informed about the risk of hypoglycaemia. Most felt they needed support during these appointments, as the information given was often emotional and shocking, negatively impacting them. However, a few mothers did not require a support person, and felt they coped well in these appointments alone.
Yeah, I cried, because it’s, it’s hard – Parent of high birthweight baby It was devastating because you don’t want that for your child – Mother with diabetes in pregnancy You’re in shock and you look around and its only yourself – Mother with diabetes in pregnancy Interviewer: Hmm! So, what helped you get through? Participant: I… I bring my parents over. – Parent of high birthweight baby No, I think I looked at it more logically than anything it’s like. It’s like, you know, just like a mama. You have the problem. You just have to deal with it – Mother with diabetes in pregnancy
For some, addressing the challenges of their diabetes diagnosis overshadowed the implications for their baby. Whereas in families where the mother did not have diabetes, neonatal hypoglycaemia risk was the primary focus. This highlights the necessity for tailored provision of information and support depending on the family’s context.
When I had this gestational diabetes. It was just part of the package – Mother with diabetes in pregnancy
Some participants had experienced extensive familial trauma from diabetes. Talking about diabetes in pregnancy and infant hypoglycaemia evoked traumatic memories of the premature passing away of parents or family members from diabetes.
Yeah, yeah, when [midwife] told me that I was thinking for my parents. But no, my parents pass away, both of them pass away – Mother with diabetes in pregnancy And then she told me I need to use the insulin, so I use that. When she told me first, I’m so scared to use it– Mother with diabetes in pregnancy
A few participants were confused about the connection between the mother’s diabetes diagnosis and the baby’s risk of neonatal hypoglycaemia. One mother believed that the hypoglycaemia risk implied that her baby would be born diabetic, indicating misconception arising from a lack of information.
I just thought that um they’re at risk of getting diabetes like me – Mother with diabetes in pregnancy
Native language communication
For some, the absence of someone able to speak their family’s native language was a barrier to culturally congruent information. It often was left to the mother to communicate all health information to her family, as other family members spoke only in their native language.
No, I feel if I had, if I needed help to do that, and could have done it in Samoan, then I would have – Parent of low birthweight baby For me is that like I would have loved someone of my own culture that will come and explain it to me in my language, so I could understand more about it. Because in science they have their own scientific words which I don’t understand. – Parent of high birthweight baby
Cultural beliefs related to medical care in pregnancy
Acceptance of treatments
Some participants expressed concerns about taking medications or supplements during pregnancy, fearing harm to their baby. Consequently, some mothers experienced anxiety around prescribed medications and would have preferred an alternative management option instead of tablets.
Even iron tablets, we never take any tablets when we were pregnant in the island – Parent of high birthweight baby
Most participants strongly preferred natural birth. The prospect of a caesarean section created anxiety, stress, and, occasionally, anger. Some mothers stressed the importance of health professionals clearly explaining why a caesarean section or induction of labor may be necessary.
My mum said they gonna cut you open to take the baby out because of, I said na I’m going to push my baby out – Parent of high birthweight baby Honestly. I was so angry I was so angry…. why did they take me earlier (for c-section) – Mother with diabetes in pregnancy I really just wanted to birth naturally. And then I was worried about recovery – Mother with diabetes in pregnancy
Few women raised concerns regarding themselves and their family members about preventative treatments given to the mother during pregnancy or to their newborn child. They felt these may cause unnecessary harm.
My mum, who obviously has a big influence, you know, with me having kids. Um I remember she was a bit hesitant, which then sort of led me to be, you know. This is, I’m sure if kids were born and they’re healthy then why did they need to add in this preventative measure/ just in case type thing if they don’t need it? – Parent of low birthweight baby
All participants opted to breastfeed their infants either exclusively or partially. Most preferred exclusive breastfeeding to formula as treatment for neonatal hypoglycaemia. A few used formula after discussing and understanding why it was needed as ‘breast is best’ is strongly encouraged. It was important to them to first discuss the reasons for supplementing with formula.
They told me to give her formula, but I never give my babies, all from the first one to the last one. I never give them a formula. I just breast feeding them – Mother with diabetes in pregnancy They recommend me to use both formula and breast. But I said, no, I prefer to breastfeed my baby. I never allow formula same as all my kids. I never give them formula – Parent of high birthweight baby
All mothers were happy with the use of oral dextrose gel and reported that the information provided on the use of gel was sufficient and appropriate.
I’m grateful for the gel like it was, you know, thorough…the information that was presented to me – Mother with diabetes in pregnancy
Confronting neonatal blood testing
Mothers strongly recalled heel prick blood testing of their baby, with most expressing distress at witnessing it. Some mothers felt that their baby was too young for testing and were cognizant that they were experiencing pain.
It’s so hard at the time, because when they come and do it I’m always crying, cause I just feel sad for him when he’s crying– Mother with diabetes in pregnancy Interviewer: Did you hold her while they’re doing that? Participant: Yeah I did while they were doing that and she cry, I cry. – Mother with diabetes in pregnancy The baby is still young, and they feel pain as well. – Parent of high birthweight baby
Half of the mothers were offered the opportunity to breastfeed during the test or warm baby’s foot before testing. Mothers felt that having skin-to-skin contact with baby on the breast was the most effective way of soothing their baby. A few mothers were concerned that others were not offered the same opportunity. One mother who wasn’t present during the heel prick test was grateful that her baby’s father could provide skin-to-skin in her absence.
So, we know the value of skin to skin right? So, I was really happy with the idea that my husband would be able to do that for my daughter, cause I wouldn’t be able to do that – Mother with diabetes in pregnancy They warmed up the foot in some nice warm water, and they warmed it up, massaged it as well… I learnt after [baby 1] and [baby 2] that I prefer to keep them on my breast while they had it done. Yeah so I don’t know if another Mama would know that - Mother with diabetes in pregnancy And that would have been much better if there was time taken for her to have some comfort while that was happening.– Mother with diabetes in pregnancy
Insufficient warning of the test and inadequate information exacerbated negative experiences.
I was woken up from a nap. I was still sleeping; I saw the one of the nurses. They were doing that one on her leg, the one on her foot, and I heard her crying – Mother with diabetes in pregnancy
Some mothers experienced significant distress when their baby required multiple tests, due to insufficient discussion or understanding about the necessity for extra testing.
And they said that they wanna do it again because maybe they missed something and I said no, I don’t wanna do it again. – Parent of high birthweight baby
Relevance of faith and spirituality
Faith holds great importance in Pacific families’ lives. Prayer emerged as a crucial faith practice for most participants in the hospital setting.
Some mothers highlighted the deeply personal nature of prayer time. During prayer, participants expressed the desire for the inclusion of all family members, underscoring the sacredness of the shared space engendered by prayer. These mothers expressed preference for prayer before giving birth or any procedures as it provides comfort and strength for all.
We prayed before my birth. My husband did a little prayer. Just me, my husband and baby - Mother with diabetes in pregnancy And we’re so lucky that we have a big family, and that’s they only thing they do, they’re praying in the morning and afternoon– Mother with diabetes in pregnancy And yeah we just embraced it. And that was really lovely. Yeah, and it lifts up our spirits too, and make us feel special – Mother with diabetes in pregnancy
Most families felt supported in using prayer in hospital. Other faith-based practices (receiving holy communion, visit from a priest or clergyman) were less accessible. Some families who had strong religious faith would have appreciated these.
We’ve all had our holy communions. So that would have been lovely – Mother with diabetes in pregnancy I did. I try to cry it out to the Lord and…walk on, walk strong, and don’t look back. Whatever happened – Parent of high birthweight baby
One participant expressed that being faced with such a challenging experience made them question where God was when they needed him. However, for most participants, this emotionally challenging time strengthened the connection of their whānau with God. Practising their faith while in hospital brought them great comfort and peace. Most participants wanted the hospital to be a safe place to be able to express their faith without judgement from staff or visiting family members.
I just feel sometimes God hasn’t been there for me… I just thought that God has failed me sometimes in life… You need to open your heart to God but I’m like, I’m trying. How can I? How can I open my heart more? – Mother with diabetes in pregnancy I know it’s so hard, like I said, that time is so hard at that time. But we thank God, he help us a lot – Mother with diabetes in pregnancy
Continued follow-up
No families were informed about post-discharge monitoring of the child. All families expressed satisfaction with their inclusion in the hPOD study follow-up, as that was their only experience of follow-up besides routine visits by Plunket (Well-Child) nurses or midwives to assess baby’s growth. Most families were interested in tracking their child’s progress and development via the study.
No, everything was great. Yeah. I have nothing negative to say. – Mother with diabetes in pregnancy I thought that was interesting just to see how he was and where he was – um and there were no problems with him at any of those times. – Parent of high birthweight baby
Half of the participants desired more regular and frequent follow-up and monitoring opportunities post-discharge. Some expressed the need for specific guidance regarding the care required for infants born at risk of hypoglycaemia.
You guys too with the following up because we didn’t know about the follow up until the first one … you know. It’s very helpful for us, and we…pray that … people take notice – Mother with diabetes in pregnancy It would be better if the follow up will be happening like every year – Parent of high birthweight baby I don’t know if that was something to be you know…follow up after having been informed that a child might have had low blood sugar like what sort of care the child might need after that – Mother with diabetes in pregnancy
Half of the participants preferred community-based follow up over hospital settings. Families fondly recalled their child’s school visits (hPOD trial follow-up assessment). A few preferred home-based follow-up.
And just maybe a follow up at home instead of the hospital. – Parent of high birthweight baby I remember the lady came with some books and stuff. Yeah…she was really good. – Parent of high birthweight baby They’ll organise it through the school, through the teacher. So, all of that was… was well explained. I had no problems – Parent of low birthweight baby
The prospect of their baby being at risk of hypoglycaemia heightened mothers’ awareness of their child’s diet in terms of sugar intake and weight as they grew. Some recalled having anxiety regarding their child’s health issues such as dental problems, weight gain, or hearing difficulties, fearing a link with neonatal hypoglycaemia. This was the case for some mothers whether the children did or did not develop hypoglycaemia at birth.
Because after that, every little thing that is wrong with the child it’s like…oh is this relevant? – Mother with diabetes in pregnancy
However, most families were content with their child’s health, perceiving them to be thriving and achieving all developmental milestones satisfactorily.
Oh, my gosh, she’s okay, never! She never sick. She’s healthy. Very healthy- Mother with diabetes in pregnancy I had no problems with it whatsoever. I didn’t feel like it affected her, anyway, or, you know sort of. No, she’s fine. She’s met all her milestones still very active now, does gymnastics. – Parent of low birthweight baby
Discussion
This study explored Pacific families’ lived experience of having a baby born at risk of neonatal hypoglycaemia. We found seven connected themes to represent the experiences of participants. We used the Seitapu Framework, which was designed to foster cultural competency for Pacific and non- Pacific health providers when working with Pacific families (Agnew, 2004). Drawing on the four principles of Seitapu: Family, Language, Tapu (sacred religious and cultural beliefs) and Community, we created a framework that visualizes the interconnectedness of our seven themes. This framework represents how the Pacific families involved in this study would like to be supported through the neonatal hypoglycaemia care pathway. This approach is likely to be helpful for other health professionals involved in providing care for Pacific families in the future, encouraging a shift from assuming care is culturally responsive to actively engaging with families about their unique needs and preferences. By emphasizing that healthcare should be a collaborative and culturally informed process, our findings emphasize the importance of ensuring that the care provided is not only respectful but truly aligned with cultural values and expectations. This is relevant, and indeed crucial, not just for neonatal hypoglycaemia care in New Zealand, but for a broader spectrum of health challenges in any location to improve the healthcare experience for Pacific families.
The central theme, at the centre of the Sei (flower) is
Within the theme
Broadly within our theme
Findings under the theme
The theme
The theme of
Lastly,
Although the sample size in this study was relatively small, it reflected the unique group targeted for recruitment, which inherently limited the eligible population. One recruitment challenge was the time that had elapsed since the parents of children at risk of neonatal hypoglycaemia had experienced these events, so some families approached had put their experiences behind them and did not wish to discuss them. Despite these challenges, the study team observed consistent themes emerging across participant interviews after just 10 interviews, suggesting data saturation had been reached. While the small sample size may constrain the generalisability of the findings, the depth and richness of the findings offer valuable insights into the lived experiences of these parents. More research is required to provide additional insight on other Pacific groups, and in different healthcare settings, to establish if these findings are applicable in a broader context.
Study limitations and future research
Our study findings have limited generalizability, as most participants were mothers of babies at risk of hypoglycaemia recruited to a clinical trial, and only one father’s perspective was obtained. Due to the geographical concentration of New Zealand’s Pacific population, with 64% residing in Auckland in 2013 (Auckland Council, 2019) all study participants had infants born in hospitals located in Auckland. Our limited sample size also did not include all Pacific nations. Additionally, the most common risk factor for neonatal hypoglycaemia was infant of a mother with diabetes. This is primarily due to diabetes in pregnancy being more prevalent among Pacific than NZ European women (Chepulis, 2022; Health Quality and Safety Commission, 2019). Our findings show that having diabetes in pregnancy alters a mother’s experience with neonatal hypoglycaemia risk. This is because mothers are often informed about their diabetes diagnosis (gestational diabetes) before or at the same time as their baby’s risk of neonatal hypoglycaemia. Their diabetes diagnosis then competes for focus and the implications for the baby may not be well understood. Our findings also showed that mothers with a diabetes diagnosis prior to being informed about neonatal hypoglycaemia risk were less shocked and were able to approach the situation more logically.
Although we have presented our findings as a homogenous group, we recognise that each Pacific Island has a unique cultural identity that was not fully explored by our collective analysis approach. Furthermore, several years had passed since their experiences of neonatal hypoglycaemia, so families’ recollection of events and impressions maybe incomplete. Lastly, our research team’s inability to conduct interviews in all Pacific languages may have hindered inclusivity and more comprehensive data collection.
However, our study has several strengths. To our knowledge this is the first study to explore Pacific families’ experience of having a baby born at risk of neonatal hypoglycaemia. We employed a validated analysis method, and recruited participants from the main Pacific Island ethnic groups who reside in Aotearoa. We offered in-person, telephone, or online Zoom interviews to accommodate diverse circumstances including residence outside Auckland, limited time availability, or lack of transport or internet access. Some participants were greeted in their own first language (Tongan and Samoan) on the invitation letter and one study team member was available to interview Samoan participants in their own language. We implemented a prespecified interview question guide comprising open questions to minimize interviewer bias, but also encouraged participants to share in a Talanoa to make interviews more culturally appropriate.
Conclusion
In exploring the experiences of Pacific families facing the challenges of having a baby born at risk of neonatal hypoglycaemia, we found that the healthcare professionals have a pivotal role in nurturing the Vā, or relational space, which profoundly influences Pacific families’ experiences of the neonatal hypoglycaemia care pathway. Key strategies for nurturing the Vā were highlighted, including involvement of the whole family in care decisions, culturally appropriate communication through Talanoa-style discussions, healthcare staff speaking Pacific languages, and acknowledgement of religious and spiritual beliefs. Integration of these more culturally responsive practices into care of Pacific families whose infant is born at risk of neonatal hypoglycaemia is likely to improve their overall experience of neonatal hypoglycaemia care.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251331290 – Supplemental material for Experiences of Pacific parents of infants born at risk of neonatal hypoglycaemia in New Zealand
Supplemental material, sj-docx-1-hpq-10.1177_13591053251331290 for Experiences of Pacific parents of infants born at risk of neonatal hypoglycaemia in New Zealand by Orla Walsh, Lily F Roberts, Karaponi Okesene-Gafa, Jenny A Rogers and Jane E Harding in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053251331290 – Supplemental material for Experiences of Pacific parents of infants born at risk of neonatal hypoglycaemia in New Zealand
Supplemental material, sj-docx-2-hpq-10.1177_13591053251331290 for Experiences of Pacific parents of infants born at risk of neonatal hypoglycaemia in New Zealand by Orla Walsh, Lily F Roberts, Karaponi Okesene-Gafa, Jenny A Rogers and Jane E Harding in Journal of Health Psychology
Footnotes
Acknowledgements
For their guidance on the design of this study we would like to acknowledge the Neonatal Hypoglycaemia Guideline Governance Group.
Definitions
Talanoa: To tell a story or have a conversation in Pacific Culture.
Koha: An acknowledgement of the time, knowledge and experience that a person has gifted.
Vā: The space in relationships that relates, holding two separate entities in unity.
Author contributions
OW: administration, conceptualisation, data collection, analysis, writing. LFR: administration, analysis, writing. KOG: conceptualisation, data collection, supervision. JAR: conceptualisation, data collection, analysis. JEH: conceptualisation, supervision, writing.
Data sharing statement
The datasets used and analysed are confidential and cannot be shared as a condition of ethics approval for this study. All material that can be shared is included in the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Ministry for Business, Innovation and Employment and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health (NIH; grant R01HD091075). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NICHD or the NIH.
Ethics approval
This study was approved by the Auckland Health Research Ethics Committee (reference number 25449).
Informed consent
All participants gave written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.