
Abstract
Neonatal hypoglycaemia is the most common metabolic disorder of infants worldwide. In Aotearoa New Zealand, Asian infants are at increased risk due to predisposing factors, including maternal diabetes and low birthweight. Little is known regarding the experience of parents of infants born at risk for neonatal hypoglycaemia, including finding their infant is at risk, testing, treatment, and follow-up. This qualitative study aimed to explore Asian families’ experiences of having an infant born at risk of hypoglycaemia in Aotearoa New Zealand. Twelve interviews involving 14 participants were conducted and transcribed. Content analysis highlighted eight key themes that summarised families’ experiences of the care pathway: complex circumstances, adequate information sharing, varied attitudes towards neonatal hypoglycaemia, cultural openness, confronting testing, acceptable gel treatment, importance of support, and continued monitoring. Our findings demonstrate the importance of comprehensive and culturally sensitive care of neonates born at risk for hypoglycaemia and their families.
Introduction
Neonatal hypoglycaemia is a common metabolic disorder of newborn infants, affecting 5%–15% of all infants (Cornblath and Ichord, 2000) and up to 50% of those in recognised risk groups, including those born preterm, small or large birthweight, or to mothers with diabetes (IDM) (Harris et al., 2012). When severe or prolonged, neonatal hypoglycaemia can result in neurodevelopmental impairment (Harding et al., 2024).
In Aotearoa New Zealand, Asian infants are more likely to be born at risk of neonatal hypoglycaemia than European infants, due to the higher incidence of risk factors in this group. (National Women’s Health, 2022; O’Brien et al., 2023). However, to our knowledge no published study has reported Asian families’ experiences of the care pathway.
The aim of this study was to explore families’ perspectives of how they were informed their infant was at risk and any testing, treatment, and follow-up their infant received, to identify both positive aspects of their experience and areas for improvement.
Methods
This study, conducted from May to September 2023, is reported according to the COREQ checklist for qualitative research (Tong et al., 2007; Supplementary File 1).
Participant recruitment
We used a purposive sampling approach to recruit participants from a range of Asian backgrounds, birth hospitals, and neonatal hypoglycaemia risk groups.
Families of children who took part in the 2-year or 6–8 year hypoglycaemia Prevention with Oral Dextrose (hPOD) follow-up study and had given consent for further contact for future research were considered eligible (Harding et al., 2021). They were sent an initial email outlining the study and providing a link to the participant information sheet, available in English or Mandarin. The primary contact was typically but not always the mother, depending on available contact details, and other family members were invited to join the interview. If there was no response to the initial email, a study team member attempted to contact potential participants by telephone or text. Recruitment continued until data saturation was reached, as agreed upon by three research team members involved in data analysis (CU, LL, LR).
Data collection
Participants were interviewed according to their preferences, alone or with family members, and either in-person at research offices in Grafton, Auckland, or via online video conference, or telephone. Interviews lasted 25–60 minutes and were attended by one or two researchers (CU, JR, LL, LR) who facilitated a conversation in English or Mandarin based on a question guide (Supplementary File 2). Of the four interviewers, all were female, two had a medical background, and two had qualitative research experience.
Data analysis
Interviews were audio recorded and transcribed verbatim. Participants could review the transcript in the interview language before analysis.
Conventional qualitative content analysis was used to analyse transcribed interviews (Hsieh and Shannon, 2005). Transcripts were anonymised and imported into NVivo 14 (Lumivero, 2023). Two researchers (CU, LL, LR) coded each transcript independently and consensus was reached with a third researcher. Coding of the first two transcripts was discussed to standardise the approach. Codes were combined into themes and subthemes through iterative content analysis (Hsieh and Shannon, 2005). To avoid identification, participants were grouped into South Asian and East Asian.
To quantify the proportion of participants expressing a certain sentiment, we used ‘few’ for 1–3; ‘some’ for 4–5; ‘half’ for 6–7; ‘most/the majority’ for 8–13; and ‘all’ for 14.
Ethics statement
Approval for the study was granted by the Auckland Health Research Ethics Committee (#25449). All participants gave written informed consent. Participants received a small gift voucher and expense reimbursement for participation.
Results
Participant characteristics
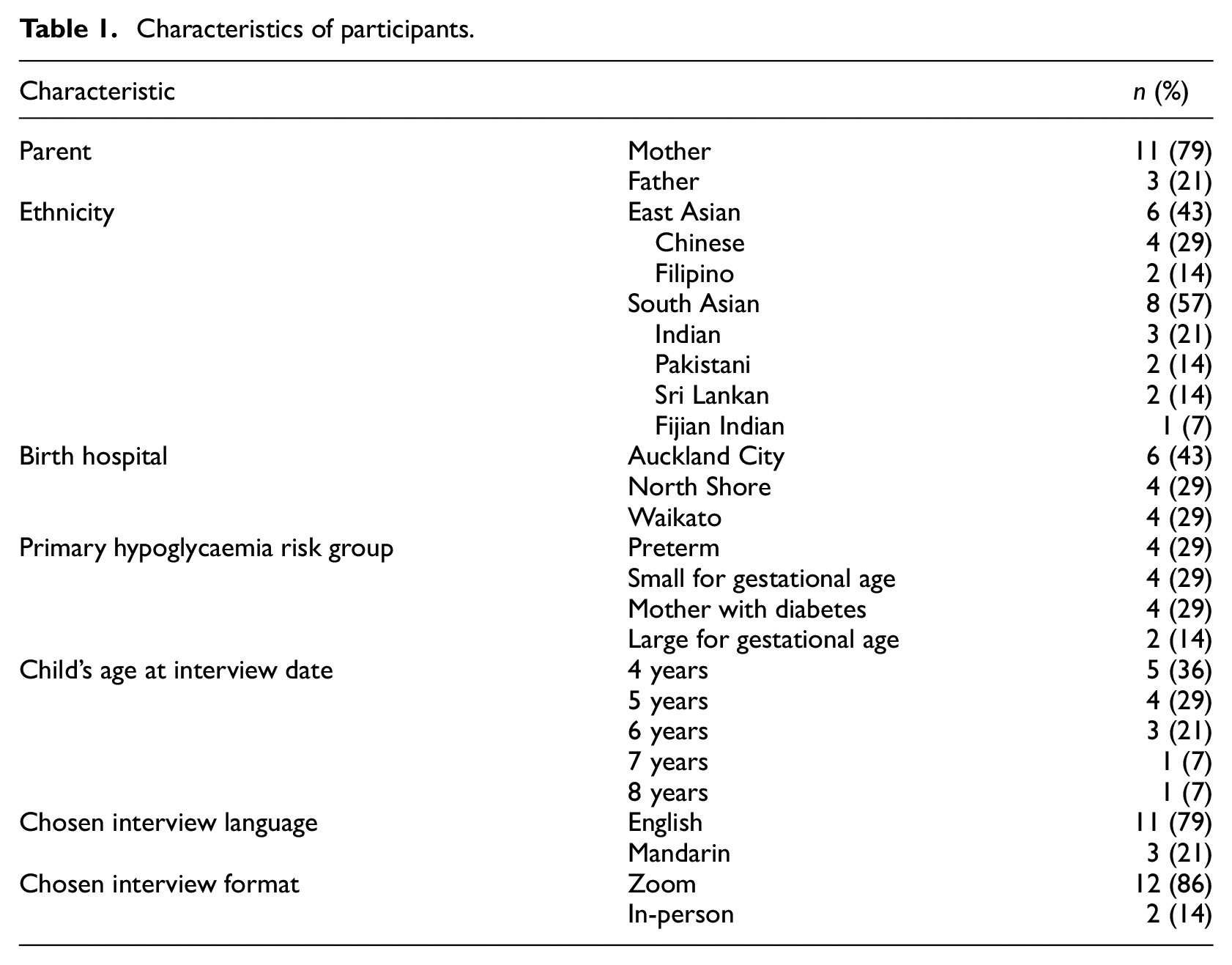
In total, 14 participants were involved in 12 interviews, of whom 11 were mothers and three were fathers. Two interviews involved both parents. Six participants (43%) were East Asian and eight (57%) were South Asian. Almost half of their babies were born at Auckland City Hospital (43%), with the remainder born at North Shore Hospital (29%) and Waikato Hospital (29%). Primary risk factors for hypoglycaemia were preterm birth, SGA and IDM each 29% and large for gestational age (LGA) 14% (Table 1).
Characteristics of participants.
Key themes
We identified eight interconnected themes in the experiences reported by parents interviewed: (1) Complex circumstances, (2) Adequate information sharing, (3) Varied attitudes towards neonatal hypoglycaemia, (4) Cultural openness, (5) Confronting testing, (6) Acceptable gel treatment, (7) Importance of support, and (8) Continued monitoring (Figure 1).
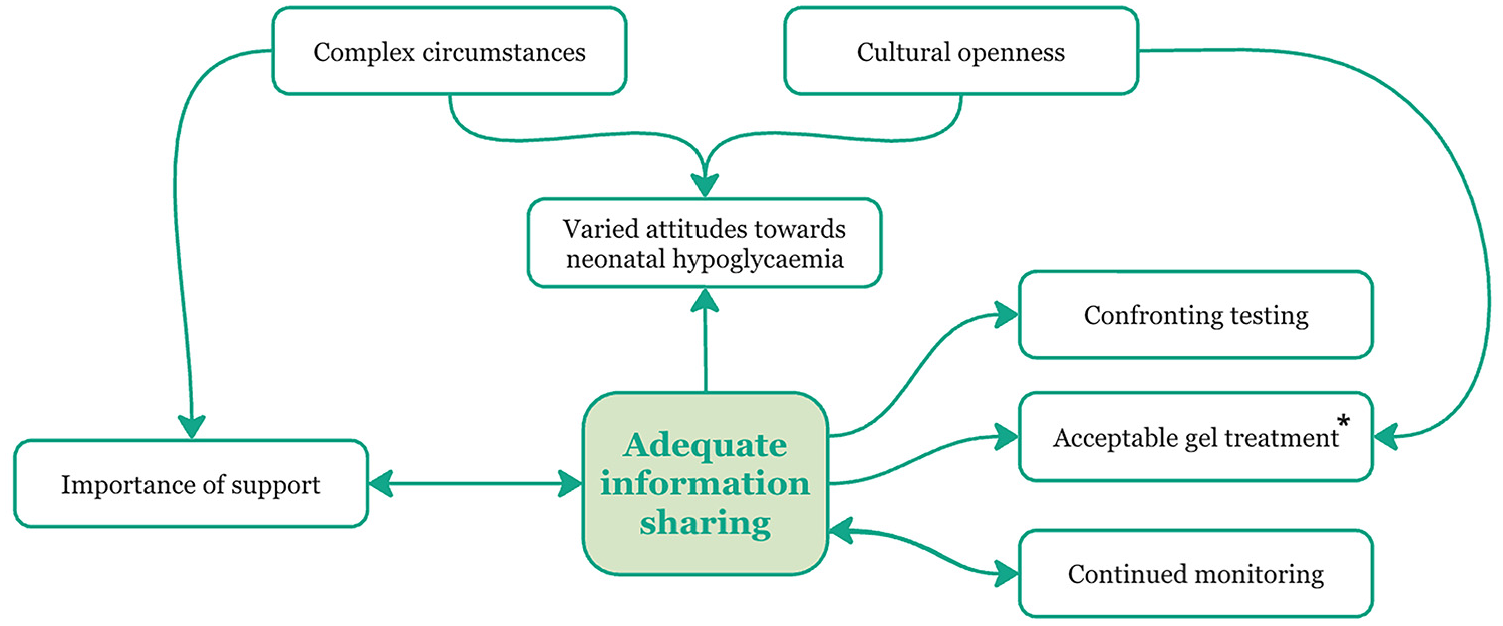
Visualisation of the eight themes summarising the experiences of Asian parents of infants born at risk of neonatal hypoglycaemia and the interconnectedness of these themes.
Complex circumstances
Most parents experienced complexity before and around the time of birth. For example, some infants were expected to be born SGA, meaning parents needed to attend repeated appointments to closely monitor growth. A few parents had high-risk pregnancies with medical complications that meant they were grateful for their infant’s birth. Two felt a sense of displacement, one having hoped to give birth in a birthing centre but instead being in a hospital due to the infant’s high-risk status, with another experiencing their first birth in a hospital away from their home country. The theme of importance of support was pivotal for these mothers.
We were displaced in the sense…that I had to stay in hospital for about a week or more than that…We were thinking that we’d go into like a birthing centre, and all of that. So there were so many changes and so many things. And so yeah, lots of things going through our minds. (Participant 6, South Asian) My experience with [hypoglycaemia] was not [laughs] very impacting, because her birth by itself was a not normal, like, you know, in the whole scenario because I wanted to see her alive. (Participant 9, South Asian)
For some, memories of the events around this time were blurry, with complex family dynamics, medication effects, or many appointments for medical complications. This meant information processing was difficult at the time and poorly recalled at the interview.
I can’t really remember because I had so many… because I had a backpain. So I have a back injury. So, because of that, I had a lot of doctors [laughs] like. And this is a lot of people. So, I can’t really remember who exactly told me. (Participant 13, South Asian) So yeah, it was. It’s sort of like a blur. And at that time, because of my current situation. Yeah, it’s quite difficult to process things. (Participant 6, South Asian)
Lifestyle changes during pregnancy were difficult to accept. For example, some mothers were diagnosed with gestational diabetes, with most understanding this to increase the risk of hypoglycaemia. Responses varied, especially in their attitude towards neonatal hypoglycaemia; a few expected the diagnosis due to similar experiences from friends, and a few felt shocked, afraid, depressed, or guilty about the impact of their own health on their unborn child.
I am still a little bit afraid. I don’t even remember what it was like at first. Uh, I really don’t remember very much, I was just a little shocked. (Participant 2, East Asian) I don’t have any specific feelings, because I know others, my friends, who have had a similar experience. It appears that this can happen sometimes. (Participant 3, East Asian)
A few mothers found it challenging to control their blood glucose concentrations during pregnancy due to a traditional diet of high carbohydrates. Uncertainty existed, for a few mothers, surrounding strict blood glucose control benefits for their unborn infant.
Participant: Managing blood sugar within a controllable range during pregnancy was challenging. Interviewer: You had to test it every day, right? Participant: Yes, three times a day. It’s quite challenging for us Chinese; I feel like even eating a steamed bun could cause a spike in blood sugar. Participant 3, East Asian I don’t know that they it had any benefit to it. In fact, my suspicion is it didn’t really work for either of us. (Participant 14, South Asian)
Shortly after birth, feeding the infant became an additional complicating factor for a few mothers who experienced issues with lactation.
I only give her like the only few drops. It’s like the colostrum is like only maybe not even a teaspoon, I cannot… (Participant 7, East Asian)
Adequate information sharing
Most participants recalled first hearing about their infant’s risk of hypoglycaemia during pregnancy or childbirth, but a few did not remember hearing about it. Among those who could remember, about half thought the conversation occurred in the third trimester, and half recalled learning about it at their infant’s birth.
Towards the end, when they were planning for induction of labour…that was the time that I was told that, you know, there could be chances of hypoglycaemia. And yeah… that was a time that I was given kind of more information. (Participant 5, South Asian)
Few participants could recall who informed them about their infant’s risk of hypoglycaemia, with the midwife being the most common source and one parent learning from an obstetrician. For some, the intensity of the birth made it difficult to remember who shared the information when being told around this time.
I don’t know who told us the midwife, or I think it’s the nurse. We had a nurse there…and my midwife was also there. Yes. (Participant 9, South Asian)
As indicated in Figure 1, this theme is interconnected with all other themes since it appears information sharing impacted the whole experience, including how supported parents felt by medical staff while in hospital and how reassured they felt surrounding their infant’s development when leaving the hospital. Two subthemes illustrate parents’ experiences of information sharing: (1) Language barriers and (2) Communication style.
Language barriers
Some parents explicitly stated or implied that they faced language barriers during interactions with midwives or hospital staff. English was a second language for most, and none mentioned receiving support from staff speaking their first language. As a result, a few felt they missed out on information or didn’t fully understand what was happening with their infant.
Maybe it’s because my midwife is a foreigner, so maybe we missed a lot of information… this is the only midwife I’ve ever seen, and I don’t have any Chinese midwife… (Participant 4, East Asian)
A few mothers had to relay information to their partners who could not understand what was said. One Mandarin-speaking parent did not recall being informed about their child’s risk of neonatal hypoglycaemia and notice a language barrier with her English-speaking midwife. Despite this, she and her partner regarded the medical staff highly and trusted them to act in their infant’s best interest.
I don’t really remember… there may be some problems in communication… we were not sure what she said at the time. But because we thought they were qualified and we trusted them, then we agreed. Because we were also afraid that it would not be good if the child had symptoms of hypoglycaemia or something. (Participant 4, East Asian) English is a second language, I mean, for all of us. So I think, sort of, I would have processed the information better than him. (Participant 6, South Asian)
One participant described feeling nervous and helpless experiencing motherhood for the first time without having a strong grasp of the language spoken by hospital staff.
Yes, at that time, because I was a mother for the first time, I was also very nervous, and then I couldn’t speak the language. In fact, I was really helpless. (Participant 4, East Asian)
Communication style
During pregnancy and the hospital stay, parents received a plethora of information, not just about neonatal hypoglycaemia. Most participants struggled to recall information shared during pregnancy or birth, with a few noting they needed repeated interactions with the information to process and understand it. Without this, parents often left feeling confused and uninformed.
Maybe a second visit or a second time, you know, just a sort of a little bit of time to process information, and then information be shared with you again, or information be summarised… Just sort of probably two occurrences…that might be useful. Yeah well, that for me, that would have been useful, because…my pregnancy, and just the birth of my son like that time was very overwhelming. So yeah, it was uh, it was difficult for me to process like everything that was happening at that same time. (Participant 6, South Asian)
One participant mentioned briefly hearing about the long-term risks of hypoglycaemia from her midwife. When she and her partner learned that hypoglycaemia could affect their infant’s brain, they were concerned and requested more information. She acknowledged that not everyone would want such detailed information and that the midwife might have been cautious about causing unnecessary worry.
I think at that time, I think, with the midwife explaining to us, and even the doctors like whoever was there like I can’t remember like, because they were giving us lot of information, and then they were saying, No, because we were like asking what else? What like? We wanted to know the like other things so, but other than that, even if they say like, there will be a risk. They say, No, no, this is very common. And then they were trying to like give us all the positives. I think that was a good thing. (Participant 13, South Asian)
Half of the participants expressed that it was important that both parents were kept informed, and that efforts are made to ensure both parents absorb and understand the information. Participants understood this wasn’t always possible, particularly when the mother was incapacitated, such as after surgery. However, instances existed where both parents could have been informed, but only one was, which hindered their ability to make shared decisions about their infant’s care.
My husband said that [we were told that our son was at risk] when he was born, it was when my child was first born. But you know a mother is tired after giving birth. It’s all my husband told me. In fact, maybe he knows these [details] better than me. (Participant 4, East Asian) I was in the bed, but they first told [father], and he told me. Yeah, the nurse didn’t directly speak to me. (Participant 9, South Asian)
Half of participants had specific preferences for how they received information about neonatal hypoglycaemia. Some remembered only receiving written information and would have preferred a face-to-face conversation. Others appreciated informative conversations but would have appreciated a supplementary leaflet or short video to review later. A few suggested a follow-up visit to their home to summarise the information and ensure it was understood.
Maybe if they were able to show like a … little video and say, look…this is what’s going to happen. This is how it’s going to be done and so forth. And then having some yeah, I guess, reassurance that you know… what benefits that would have for my son. (Participant 6, South Asian) But I was just given actually a leaflet to read through it. Um but nobody explained that. (Participant 5, South Asian)
Varied attitudes towards neonatal hypoglycaemia
Of those who remembered being informed about their infant’s risk of hypoglycaemia, half felt nervous or guilty, while the other half did not recall being strongly affected. One parent felt nervous, as they had no idea how small the infant would be and the possibility of an emergency caesarean section. Another mother felt guilty, knowing her diabetes put her infant at risk.
I was quite nervous, actually, when I found out that that yeah, my children were under, I mean, especially with the first one. (Participant 5, South Asian)
Parents who weren’t strongly affected often had complex circumstances around the birth that took precedence, linking to that theme. As a result, a few parents didn’t fully process the information at the time or were simply hopeful that their infant would be born alive. For one couple, after struggles with conception and multiple miscarriages, having an infant was a blessing, and they accepted any complexities that would arise.
I wanted to get [baby] out…my bilirubin was high because of …., my um …. markers were high and I was on a particular medication. I don’t know. I forgot that. So, all that wanted me for me was to… so hypoglycaemia I didn’t even understand…I just want to see my baby, that’s all. (Participant 9, South Asian) My son has come after a lot of struggles and all of that. So I’ve already had like miscarriages, and all of that kind of stuff. So for us, just to have a child was, you know, the most biggest blessing, and it didn’t really matter what else was accompanied with it. Yeah. (Participant 6, South Asian)
This theme is closely ties to ‘Adequate information sharing’, as variations in how the risk of hypoglycaemia was communicated clearly affected parents’ attitudes. Only one participant mentioned being informed about the implications of hypoglycaemia for their infant’s development. Lacking this information likely affected how concerned the parents were for their infant’s health and development.
Cultural openness
Participants had diverse ethnic and geographic backgrounds and varying cultural preferences for their pregnancy and childbirth. Some had strong preferences for cultural openness and awareness, while most had no specific preferences.
Um… I think cultural. I I wasn’t. No, I wasn’t nothing that I had really…I wasn’t too fussy about anything. (Participant 5, South Asian)
Some participants voiced challenges related to their cultural experiences. One found childbirth in Aotearoa New Zealand to be a culture shock, while another sensed a lack of cultural support, which made them feel isolated from their support systems back home. They suggested that culturally open healthcare could better support parents through their reproductive journey.
Cause I’m a migrant like, I don’t have a cultural support system. So I felt like I was really alone…Just even like a bit of knowledge about, you know, what happens in Asian countries. Or…kind of what are the supportive things that might help Asian mothers, you know, even if they’re not [country of origin]… When I read about like, you know, Māori support kind of things that, you know, just even understanding that, and or having someone… it’s like just a gap between what the medical system can provide and what could make you feel supported and less anxious and resolve your issues. (Participant 14, South Asian)
Few participants experienced cultural openness in hospital which left a lasting impression. For example, a few participants stated that Muslim tradition involves honey being placed in the infant’s mouth immediately after birth to bring prosperity. Being permitted to do this brought a lot of happiness to a few parents, despite clinicians’ preference that dextrose gel should first be administered for the prevention of hypoglycaemia. This links to the acceptable gel treatment theme.
It’s amazing because the doctor and nurses told me yeah it’s good we can give the first this [gel] but I say no I give the honey first so they’re all doctors and nurses and discussions like honey or [gel] and I say no honey is going first. (Participant 11, South Asian)
Other preferences for improving the birthing experience for Muslim parents included having a female staff member present to support the mother and provide information during procedures, such as the infant’s blood glucose testing.
My most vivid memory is when the doctors came to visit us, and that’s when the tests were done in hospital. It would have been good to have for me just going through that process having a female doctor coming in, or a nurse or a support staff, you know, sort of coming in, and just sort of accompanying um that process and just sort of letting me know what’s happening. I kind of felt that things kind of happened very quickly, and I wasn’t really prepared for you know what it meant…I just kind of felt that if there was a female, that was accompanying, then…that would have been good yeah. (Participant 6, South Asian)
One parent also would have appreciated being asked if they would like to perform any cultural practices such as prayer after their child was born.
I think that would be good if doctors can ask the clients. They can ask the patient that if you prefer a cultural thing that you can do it…there are specific things when they’re born. So we like, say something like, maybe it takes 10 to 15 min. But if they put right away to the incubator or something like that. So how can we do that? It’s not possible. (Participant 11, South Asian)
Confronting testing
For most parents, the heel prick test was the most vivid memory from their initial hospital visit and reported feeling distressed, upset, and shocked by seeing blood drawn from their infant’s foot, with some seeing more blood than expected. Some remembered several heel pricks, with one likening their infant’s foot to a pincushion. A few parents were not negatively affected or did not witness the procedure as the infant was taken to another room.
She is the first child, and she [child’s mother] remembers being very distressed, very distressed. (Participant 2, East Asian) Seeing the blood… I know that my husband he kind of felt a little bit uneasy about, you know… seeing, you know…our newborn, you know, having to go through that. Yeah, it was a bit confronting…they said that it was a prick, but you know, when you see the blood coming out there was quite a lot of blood. And so that was, that was a bit. Yeah, unexpected for us. (Participant 6, South Asian)
One parent, on reflection, felt sorry for their infant due to the pain caused by the heel pricks, especially as he developed into a child with nervous temperament.
Cause he was quite a nervous little baby, and I didn’t really know at the time, but I guess just in hindsight. When I think about how nervous he is now about anything I can just imagine getting those pricks must have been I don’t know. Kind of kind of awful for him. (Participant 14, South Asian)
A few parents were surprised at the method, finding the ‘large needle’ used on a tiny infant distressing and suggesting a less stressful alternative blood collection method. One mother took a few months to recover.
They need to check the sugar level. So, if there’s any other way aside from pricking because it stresses out the baby and the parents. (Participant 8, East Asian) Yeah, it’s been like few months to recover my mind. My heart. (Participant 11, South Asian)
A similar number of parents believed that the heel prick was optional, and regretted consenting to it, implying they were not aware that the process was standard care for infants born at risk of hypoglycaemia.
If I were probably you know to have to be told that, you know we want to do it again, or you know on, on my, on a second child…I would probably decline the process. Um and then just sort of do a wait and watch, and just see if you know anything comes up later as symptoms. (Participant 6, South Asian)
Few parents felt adequately warned about the testing process, with mothers able to breastfeed or either parent holding the infant skin-on-skin during testing, for comfort. Advanced warning and the ability to comfort their infant improved the experience for those parents.
I did tell them I would like to have my baby on skin-to-skin while they perform the blood sugars. So yeah, so they did…they did agree with that and carried on the same way. So yeah, and baby was, I think, yeah, comfortable just feeding. And yeah, they just made sure that whatever I like, my choice was respected… I felt that way. (Participant 5, South Asian)
A few parents felt the heel prick process was transactional or lacking in preparation of the infant and the parents. Few remembered any pre-test care, like warming the infant’s heel or encouraging skin-to-skin contact. One mother had the infant taken from her and given to her partner, but her partner was not prepared to see blood and was upset. The mother wished to have the choice of having skin-to-skin.
I think the first blood sugar they did one of the midwives they came and they asked my husband to hold the baby and I did have a Caesarean I was in the recovery room. Um rather than … my baby was on me doing the skin to skin but they asked my husband to hold the baby. He had already freaked out…I think baby bled quite a bit, and the blood was all over like the clothes of my husband. So it just really upset him…But I think I did try to tell them I think we could just do the blood sugar while baby was on me on skin to skin, baby wasn’t really feeding but they actually took the baby off me and asked my husband to hold a baby so… (Participant 5, South Asian) I guess maybe more educational… I don’t know how to say more training to the staff to make sure that… to warm baby’s foot, I think. Because the next time …somebody warmed the baby’s foot, because the first time…one of the midwives…they didn’t really warm and baby did have some bruising on the foot. (Participant 5, South Asian)
Most parents who were adversely affected by the testing wished for a longer discussion with hospital staff about the process and the choice of providing comfort to infants both prior and during testing. Parents wanted more information on the rationale, benefits of testing, the impact of hypoglycaemia on the infant’s health, and how testing is done. Some couldn’t recall receiving test results, and one parent who did felt reassured knowing their infant’s blood sugars were normal.
I think probably a little bit more time given to the whole process around it. Just yeah for us to understand. You know what it required and what it would mean, and then…how it would benefit us. (Participant 6, South Asian) Interviewer: Do you happen to remember if they told you whether he had hypoglycaemia or not? Participant: No, I don’t. (Participant 3, East Asian)
Acceptable gel treatment
In general, the gel treatment recollection was less vivid than the heel prick testing. For some parents, the gel was considered acceptable at the time. No adverse response to the gel was reported; few parents noted that their infant seemed to enjoy its sweetness.
I think that was fine? That was … I don’t remember? Yeah, I think kids like sweet stuff anyway, from memory and breast milk is quite sweet. So there wasn’t any issue there. (Participant 1, East Asian)
Some participants felt well-informed about the gel treatment, though few recalled receiving written information, and others thought they were only informed verbally. Some parents understood that the benefits of the gel treatment outweighed the potential harm, while others felt the discussion about the gel was rushed and wished for more time to be informed. One parent, facing a language barrier, agreed to the gel out of fear for their infant’s health despite not fully understanding the information provided.
Then midwife will have her own protocol to follow. The nurse will have a whole protocol to follow. They want to finish off. Tuck, chuck, chuck, chuck, chuck! They want to finish off this protocol and then send the baby to the ward. (Participant 9, South Asian) They talked about this series of information, told us about these aspects, and then asked us if we would like to participate. Because first, we were not sure if it was true, second, we did not know the information, and third, we might not understand it well. But because we are worried our son will have this problem. In addition, we think they are professional, so we trust them. Because we have confirmed that it will not have any harm on our son, so we agreed to participate at that time. (Participant 4, East Asian)
Having a health background helped one parent weigh up the gel treatment’s risks and benefits, whereas few parents had unanswered questions. For instance, one parent was sceptical about the gel’s long-term effects, and another wanted more details on the long-term effects of untreated hypoglycaemia.
We saw the risk and the benefits. So for us the benefit we thought having the gel benefited more than the risk. And even though at that stage we didn’t know what will happen if a baby is born hypoglycaemic and is untreated. (Participant 9, South Asian)
Importance of support
Most mothers were accompanied by their partners to the appointment, where they learned of their infant’s risk of hypoglycaemia. Many participants found continued partner support crucial, especially with complex information surrounding the hypoglycaemia journey, linking to the theme complex circumstances. Having informed partners helped parents make decisions and plans together. Partner support was particularly important for those experiencing stress due to their infant’s at-risk status or a complicated birth away from family. Some mothers felt better informed about the childbirth process and hypoglycaemia than their partners, often being the main source of information in the family. One mother wished her partner was present at the antenatal appointment to receive the information simultaneously and provide emotional support, linking to our previous theme of adequate information sharing.
No, it was only me and my husband. So yeah, so it’s only both of us doing all the things. And because baby was actually so, my parents were gonna come, but because the baby was born little bit early. So they were not here yet. (Participant 13, South Asian) Oh, just my husband. Yeah, just my husband with me. He didn’t understand a thing, anyway, so he said, well, I just told him that maybe needed to have blood sugar monitoring. And he asked me, what was that? (Participant 5, South Asian)
Some parents also noted strong support from their midwife and hospital staff. High-quality care and competent hospital staff provided comfort and reduced stress. One parent mentioned her midwife’s advice on managing gestational diabetes, while another recalled a good balance of information with positive reassurance from their midwife.
But yes, I think it started from our midwife. So she’s the one who say when the baby’s born, there are risks like this. And then she started explaining to us because we were bit worried because it’s our first baby. So she’s the one who’s mostly no, no, we can do this and try to help us through. (Participant 13, South Asian)
However, a few parents felt that hospital support could have been improved, such as more care around the heel prick process to make it feel less procedural. One parent thought more follow-up support was needed post-birth to make the hospital environment more conducive to the wellbeing of the family and infant. One mother mentioned how the hypoglycaemia process negatively impacted her mental wellbeing after her infant’s birth and believed more holistic care could have improved her experience.
I know, like… there’s not that many people you know that are around like everyone’s busy. But I guess like just being a first-time mum and having haemorrhaged and everything having gone on so late. I guess maybe it might have been good if people could check, maybe, or just help a little bit. (Participant 14, South Asian) I think probably the main thing is just, for you know, the physicians to be just really aware of what the what the mum is going through at that time. Just in terms of their mental wellbeing you know the sort of the whole sort of holistic, the hauora of the of the person… it just kind of felt…very procedural, I guess, at that time. (Participant 6, South Asian)
Continued monitoring
Few parents recalled receiving any written information about hypoglycaemia upon hospital discharge. One received many documents in English, not her first language, and didn’t remember reading them so was unsure whether any were about hypoglycaemia. In contrast, one parent was well prepared by her midwife who advised signs of hypoglycaemia to watch for. This theme linked bidirectionally to the theme of adequate information sharing as both themes impacted one another.
I was quite nervous. But my midwife had prepared me well for that and just. I did have some plans in terms of making sure that he was like, you know, just to watch for signs of hypoglycaemia. (Participant 5, South Asian)
After discharge, all parents had only routine follow-up visits, such as from a Plunket (Aotearoa New Zealand well child health services charity) nurse or midwife to check infant’s growth. Half of the participants expressed no concerns about hypoglycaemia, feeling reassured that the infant’s blood glucose levels were normal upon leaving hospital. A few didn’t see the need for continued monitoring if their infant wasn’t exhibiting abnormal symptoms.
Think it was all good, because there, because I think it will be different if that baby was having some like a low blood sugar, or something like that. I think there would be different, like people involved and different follow up sessions. But I think because she didn’t have it so. It was like it went back to like usual, like, it was just meeting the midwife, the Plunket nurse, and those things. Yeah, so it was all good. (Participant 13, South Asian)
However, around half of the participants expressed a wish for more monitoring of their infant’s health after birth. One mother with type one diabetes mellitus was concerned about her child inheriting the condition and wanted more routine blood sugar monitoring. A few would have appreciated a follow-up appointment to review their infant’s risk of hypoglycaemia at birth and discuss future implications, as they found it difficult to retain information during the stressful time of childbirth.
No, actually. I understand, I’ve been reflecting on my own health condition during that period, particularly when I gave birth to my child. This has triggered concerns about whether my child might inherit any potential issues in the future. I’m wondering if children with a background similar to mine should receive more extensive monitoring, beyond just the usual routines. (Participant 4, East Asian) in the first sort of year, having…a follow-up or something like that just around…this is what happened…your child was at risk um but the gel was given, and then these. This is what will happen, you know, in a during… you know the course of the child’s life…But if you experience da da da da da, or something, you know, just to give somebody a call, or, you know, just to let somebody know or contact your GP, or something like that…it might be reassuring. (Participant 6, South Asian)
Discussion
To our knowledge, our study is the first to give a voice to Asian families who experienced the care of infants born at risk of neonatal hypoglycaemia. We found eight main interlinking themes: complex circumstances, adequate information sharing, varied attitudes towards neonatal hypoglycaemia, cultural openness, confronting testing, acceptable gel treatment, the importance of support, and continued monitoring (Figure 1).
The reasons why infants are considered at risk of neonatal hypoglycaemia are associated with mothers and infants at high risk of other conditions such as pre-eclampsia, polyhydramnios, and emergency caesarean section (Kouhkan et al., 2021). This is reflected in our findings that families experienced complex circumstances through pregnancy and at the birth of their infant, including lifestyle adaptations as a result of gestational diabetes.
Lack of services in the consumer’s preferred language is a well-recognised barrier to healthcare for culturally and linguistically diverse Aotearoa New Zealand communities and leads to misinformation (Bartholomew, 2013). A recent survey showed 47.9% of Asian patients using Aotearoa New Zealand health services lacked cultural or language support (Asian Family Services, 2021). Our study found similar issues; participants felt their communication preferences were often ignored and they faced language barriers, missing crucial information. Participants suggested alternatives to verbal communication, like written pamphlets or videos, be considered. A Cochrane review found that combining written or verbal information improves satisfaction and knowledge for parents being discharged with their children from hospital (Johnson and Sandford, 2004). In our study, communication style and effectiveness likely influenced participants’ variation in attitudes towards neonatal hypoglycaemia. Some families did not understand the implications of neonatal hypoglycaemia, while for others, the inability to communicate effectively with staff may have contributed to unresolved fear or guilt.
Cultural openness and culturally appropriate healthcare, such as recognising cultural identity and language, are important factors across global Asian communities (Ragavan et al., 2018). Ethnic-specific service delivery has previously been recognised in Aotearoa New Zealand as an action that can bolster health and disability services to reduce social and economic inequalities (Ministry of Health, 2002). Our findings suggest that receptiveness to cultural preferences is of utmost importance to some Asian families. We found that the birth of a child is met with particular rituals, particularly among South-Asian families, and that the neonatal hypoglycaemia care pathway should recognise and accommodate these in order to meet the expectations of consumers. This is similar to a study looking at traditional Asian practices surrounding the peripartum period, which reported acknowledging, integrating and trying to understand beliefs and traditions surrounding this period allowed providers to deliver culturally competent care rather than reducing the available choices (Withers et al., 2018).
The heel prick technique for collecting blood from newborns has previously been met with negative reactions from parents including increased maternal stress (Kasem et al., 2022). Our findings are consistent with these, as most participants had vivid recollections of this procedure. Our findings also highlighted the desire of parents to have methods to comfort the baby during this challenging time. A study found that 55% of parents were not advised how to comfort their infant (Franck et al., 2001). This theme was interlinked with ‘adequate information sharing,’ with participants not understanding the purpose or significance of the test, and not having enough warning. Another study also found that parents would have preferred to learn about the heel prick test around 2–3 weeks before birth (Bartholomew, 2013). In contrast, the use of oral dextrose gel was generally deemed acceptable by participants, who were participating in a trial of prophylactic dextrose gel and therefore may have been provided with more information than in typical routine care. Some parents felt they were able to weigh up benefits and harms of the treatment, whereas others were unsure they were informed of potential harms, linking once again to the theme of ‘adequate information sharing’.
The importance of support was a key theme, with care from both staff and family integral to a positive experience through the neonatal hypoglycaemia pathway. Others have reported that having family visitors in the hospital played an additive and important role, leading to improved patient satisfaction, length of stay, pain, depression and anxiety (Fakhry and Mohammed, 2022). Support in the form of cultural openness was particularly important to our study participants as they navigated complex circumstances, such as experiencing a foreign healthcare system for the first time.
Current Aotearoa New Zealand hospital clinical guidelines indicate that infants born at risk of neonatal hypoglycaemia are typically not followed up after discharge from hospital (Harding et al., 2021; Mills, 2016). Our study involved parents whose infants were followed up as part of the hPOD trial, and we found that this opportunity to receive developmental reports was appreciated. Parents felt there was a gap in regular postnatal check-ups and would have valued the opportunity to ask questions and check the infant’s health after having low blood glucose concentrations after birth. This concern is not unreasonable, given evidence that infants born at risk of neonatal hypoglycaemia are at high risk of later neurocognitive impairment, whether or not they actually experience hypoglycaemia (Edwards et al., 2022; Shah et al., 2021).
This study had several strengths. It involved participants from diverse Asian backgrounds from several birthing hospitals and included perspectives of both parents. We interviewed families whose infants were at risk of neonatal hypoglycaemia for different reasons and reduced the barrier to participation among Mandarin-speaking participants by inviting and interviewing them in their first language. We implemented a prespecified interview question guide using open questions that minimised interviewer bias and leading questions. Double coding each transcript with two independent researchers established confirmability. Sharing transcripts with participants for feedback enhanced credibility.
This study also had limitations. Our study sample was not randomly selected and only involved participants of the hPOD study. Therefore, findings may not be transferable to families less involved with the health system. This recruitment method also limited our interviewees to the North Island of Aotearoa New Zealand. We were unable to offer interviews in a language other than Mandarin or English, so this may have limited our participant sample to those proficient in either of those two languages. There was also potential for recall bias since 4–8 years had lapsed since the birth of the affected infant.
Conclusion
Asian families in Aotearoa New Zealand with infants born at risk of neonatal hypoglycaemia often face difficult circumstances that complicate their pregnancy and childbirth. Repetitive information sharing and dissemination in various forms, as well as embracing cultural practices around the time of birth, may improve their experiences. Negative experiences with the heel prick test contrasted with positive experiences of oral dextrose gel treatment. Continuous support, encompassing familial and cultural connections, is crucial and follow-up care post-discharge was identified as lacking. These Asian families’ voices highlight the need for a culturally sensitive care pathway for managing infants at risk of neonatal hypoglycaemia in Aotearoa New Zealand.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251330087 – Supplemental material for Infants born at risk of neonatal hypoglycaemia in Aotearoa New Zealand
Supplemental material, sj-docx-1-hpq-10.1177_13591053251330087 for Infants born at risk of neonatal hypoglycaemia in Aotearoa New Zealand by Caitlyn Ulyatt, Lily F Roberts, Orla Walsh, Jane E Harding, Jenny Rogers and Luling Lin in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053251330087 – Supplemental material for Infants born at risk of neonatal hypoglycaemia in Aotearoa New Zealand
Supplemental material, sj-docx-2-hpq-10.1177_13591053251330087 for Infants born at risk of neonatal hypoglycaemia in Aotearoa New Zealand by Caitlyn Ulyatt, Lily F Roberts, Orla Walsh, Jane E Harding, Jenny Rogers and Luling Lin in Journal of Health Psychology
Footnotes
Acknowledgements
For their guidance on the design of this study, we would like to acknowledge the Neonatal Hypoglycaemia Guideline Governance Group.
Author contributions
CU: data collection, analysis, writing. LFR: administration, data collection, analysis, writing. OW: administration, conceptualisation. JEH: conceptualisation, supervision. JR: conceptualisation, data collection, supervision. LL: conceptualisation, data collection, data analysis.
Data sharing statement
The datasets used and analysed are confidential and cannot be shared as a condition of ethics approval for this study. All material that can be shared is included in the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Ministry for Business, Innovation and Employment and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health (NIH; grant R01HD091075). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NICHD or the NIH. LL is funded by the Aotearoa Foundation (9909494).
Ethics approval
This study was approved by the Auckland Health Research Ethics Committee (Reference Number 25449).
Informed consent
All participants gave written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.