
Abstract
To explore how the illness risk representation framework explains vaccination uptake in pregnant women. Pregnant women were recruited via hospitals and community groups. Semi-structured interviews with pregnant women, explored factors influencing vaccination uptake. Findings were analyzed using codebook approach to thematic analysis, and applied to illness risk representation framework (IRR). 43 interviews explored domains of the IRR showing good fit to vaccination beliefs of pregnant women. Identity beliefs focused on feelings of susceptibility to illness, beliefs about Cause related to exposure and prevalence to illness and feelings about immunity, Timeline beliefs included feelings about appropriate times to vaccinate, with some waiting to accept vaccinations. Beliefs about Consequences focused on perceived severity of illness and vaccine novelty, and Control beliefs included effectiveness of vaccinations, adverse effects and attempts to control exposure. Some domains of the IRR fit better than others, with estimates of likelihood and severity contributing to risk appraisals.
Introduction
Pregnant women and their unborn babies are at increased risk of serious complications from infectious diseases such as Influenza (flu), Pertussis (whooping cough) and Covid-19. Whooping cough is highly infectious and can cause severe health consequences and death in infants (Parsons et al., 2024). Pregnant women and their babies are significantly more at risk of complications from flu and Covid-19, including admission to intensive care and increased risk of death (Campbell et al., 2015; Heath et al., 2020; Knight et al., 2022; UKOSS, 2021; Villar et al., 2023).
Vaccinations are routinely offered to all pregnant women in the UK for flu and whooping cough, and more recently pregnant women are eligible to receive Covid-19 vaccinations. Flu, whooping cough and Covid-19 vaccinations are proven to be safe and effective during pregnancy(Lynch et al., 2012; Regan et al., 2015; Tamma et al., 2009; Villar et al., 2023).
Despite vaccinations being available for pregnant women in the UK uptake is low. Amongst women who gave birth in England in October 2021, 29.4% had received 2 doses of the Covid-19 vaccine (Gov.UK, 2022), compared to approximately 60.4% of the general population (Gov.UK, 2022). Uptake of the flu vaccination amongst pregnant women only reached 37.9% during the 2021/22 season (UKHealthSecurityAgency, 2021), and only 60.7% pregnant women in the UK had the pertussis vaccination in 2022–23 (UKHealthSecurityAgency, 2023).
A number of behavioral determinants exist. These include consequences, social influence and environment (Michie et al., 2008). When considering vaccination as a behavior, risk is considered a key determinant of behavior. Evidence has demonstrated that vaccination uptake is lower amongst people who felt unlikely to contract a disease, or those that believed the disease to not be severe (Bish et al., 2011).
Risk appraisals are defined as “people’s beliefs about a potential harm.” (Wright, 2010) Health Psychology theories (such as the Health Belief Model, (Rosenstock, 1974)) Protection Motivation Theory, (Rogers, 2010) and the Extended Parallel Processing Model (Witte, 2010) propose that the adoption of protective or healthy behaviors can be encouraged by increasing individuals’ beliefs about the risk of harm. Meta-analytic evidence shows that increasing appropriate risk appraisals may be an effective way to increase vaccination uptake (although the effects of this are small) (Brewer et al., 2007; Sheeran et al., 2014; Tannenbaum et al., 2015). Efficacy appraisals are perceptions made by an individual, consisting of response efficacy; the “ability of the recommended behavior in reducing the threat,” and self-efficacy; “beliefs about one’s ability to perform the risk-reducing behavior (Wright, 2010).”
In order to understand how to change behaviors, it is important to understand the beliefs that underly the perceptions of risk that an individual holds. Specifically, in order to understand what motivates pregnant women to accept vaccinations, there is a need to understand the beliefs underlying perceptions of risk for vaccinations, held by pregnant women.
One theoretical model addressing how cognitive factors influence illness coping behaviors is the ‘common sense’ model of illness representations, proposed by Leventhal (1980). The Common Sense model identifies factors involved in information processing about illnesses by a patient, to produce a lay view of the illness and how that guides behavior (Hagger and Orbell, 2003).
Individuals will create mental representations (illness representations) of their illness, to make sense and manage the problem. The interpretation of this information can lead to individuals seeking help for their illness, or engaging in coping or management strategies (Hagger and Orbell 2003).
One model used to explain the beliefs attributed to illness risk is the Illness Risk Representation framework which incorporates the illness representations of the Common Sense model.
In line with the Illness Risk Representation (IRR) framework (Cameron, 2003; Cameron, 2008), individuals make estimates of likelihood (how likely they are to be ill) and severity (how severe it would be if they did get ill) regarding an illness. According to theory (Rogers, 2010; Witte, 2010) increased perceptions of likelihood and severity are more likely to result in the adoption of the behavior. These estimates are underpinned by five illness representation domains, directly influencing health-related behaviors (Cameron, 2003). The IRR framework provides a more in-depth understanding of how individuals perceive a health threat, and proposes that information about health risks trigger beliefs about the risk of the illness, constructed from five domains: identity (beliefs about whether an individual considers themselves to be at risk of the illness based on personal characteristics and symptoms of the illness), cause (factors from personal and environmental sources that will cause the illness to occur), timeline (beliefs around the time of onset and the duration of the illness), consequences (perceptions about potential negative effects of the illness, including beliefs about pain and death as a result) and control (the extent that individuals feel they have control over the progression or cure of the illness) (Cameron, 2003; Cameron, 2008). In 2008 Cameron extended the domain of Control, to also include control over prevention (beliefs about actions that might prevent the illness) (Cameron, 2003). Beliefs of personal perceptions of illness risk are achieved by matching the illness representation with personal characteristics, to create an estimate of personal risk to the illness in question (Cameron, 2008).
Cameron also proposed that illness risk representations can lead to representations being made of procedures that could protect the health threat (Cameron, 2003). Procedure Representations are representations of coping processes that can trigger illness risk representations, and therefore activate the behavior (Cameron, 2003). When thinking about vaccination as a health behavior, Procedure Representations that are constructed around vaccinations are likely to be dependent on contextual information including the messaging and recommendations available to individuals.
The IRR framework has been used in the past to explain health behaviors such as skin cancer (Cameron, 2008), bowel cancer (Newby et al., 2017), cardiovascular disease (Claassen et al., 2010; Newby et al., 2020), and sexually transmitted infection (Newby et al., 2013). The IRR has also been used to describe vaccination behavior, including Covid-19 vaccination (Vollmann and Salewski, 2021), whooping cough vaccination amongst young children (Garg et al., 2018), flu vaccination (Bish et al., 2011; Salewski et al., 2017) and flu vaccination behavior amongst pregnant women (Parsons 2020), and as a framework upon which to develop an intervention for flu vaccination in pregnancy (Parsons et al., 2024). These examples show that the IRR framework is an appropriate framework against which beliefs influencing behaviors can be understood. This paper aims to use the IRR Framework to explain how pregnant women feel about flu, whooping cough and Covid-19 vaccination following the Covid-19 pandemic.
Aim
This qualitative study aims to explain pregnant women’s decision-making in regards to the uptake of flu, whooping cough and Covid-19 vaccination, using the Illness Risk Representation (IRR) Framework.
Materials and methods
This research is reported using the Standards for Reporting Qualitative Research framework (Supplemental material 1) (O’Brien et al., 2014), and in line with APA reporting guidelines (Association APAP, 2020). Data was collected using semi-structured interviews with pregnant women to explore their views and experiences of vaccinations, and the factors that influence their decisions to accept or refuse vaccinations, particularly since the Covid-19 pandemic. Full findings of these interviews are reported elsewhere (Parsons et al., 2024). The study was pre-registered on the International Standard Registered Clinical/social Study Number (ISRCTN) register (ID: researchregistry8679)
Sampling and recruitment
Participants were recruited to the study between March and June 2023. Participants were eligible to participate if they were pregnant at the time of recruitment, were over the age of 18 and had the capacity to consent. Participants were recruited to the study via two participating hospitals in one region of the UK, and via one community group. Interested participants were given information about the study from midwives (hospital recruitment) and group leaders (community recruitment), and these individuals passed on contact details of interested participants to the research team. Recruitment to the study has been reported elsewhere (Parsons et al., 2024).
Data collection
Semi-structured interviews were conducted remotely via telephone. Views on vaccinations and susceptibility to illness during pregnancy, factors influencing vaccination decisions, and the impact of Covid-19 on vaccination decisions were explored during interviews.
Semi-structured topic guides were informed by previous literature. To ensure the reliability and validity of findings, interview schedules were developed with consultation with healthcare professionals, Patient and public (PPI) representatives and the wider research team, and were developed iteratively as interviews progressed (Supplemental material 2). This was to ensure the schedule and the process were appropriate (Leung, 2015). Verbal or written consent was obtained prior to the start of all interviews (including consent for anonymized quotations to be included in reports). Interviews were conducted by two experienced qualitative researchers, and were audio recorded and anonymized and transcribed by a University approved transcription service. All transcripts were checked against the audio recording for accuracy. Steps were taken to ensure reliability and validity of the data collection and analysis. Two researchers conducted constant comparison and searched for deviant cases (Leung, 2015).
Only the two researchers conducting interviews had access to the audio files and transcriptions, and all files were saved with unique participation number to ensure confidentiality.
Data analysis
All interviews were analyzed using a codebook approach to Thematic Analysis (Braun and Clarke, 2021; Byrne, 2022; Clarke and Braun, 2021), which presents a flexible approach to the analysis of qualitative data, whereby a structured codebook was used, whilst also recognizing the interpretative nature of data coding (Braun and Clarke, 2021).
Thematic Analysis involves six steps (Clarke and Braun, 2021), and these were applied to the data. This consisted of (1) Familiarization of the dataset, (2) Coding, (3) Generating initial themes, (4) Developing and reviewing themes, (5) Refining, defining and naming themes, and (6) Writing up. An initial coding frame and themes were identified, and these were then used to map the constructs of the IRR framework onto, in an attempt to explore the fit of the framework in understanding and explaining vaccination uptake in this population. A deductive and semantic approach to analysis was taken (Braun and Clarke, 2006), as themes were mapped onto the five domains of the IRR (Identity, Cause, Timeline, Consequences and Control) (Cameron, 2003; Cameron, 2008), with sub-themes identified and illustrated with quotes. Assigning sub-themes to the IRR domains was completed by the two researchers conducting data analysis. Decisions were informed by the analysis previously completed and reported previously (Parsons et al. 2024), where in-depth analysis of the experience was conducted, and discussions about the fit of each in the context of vaccination in pregnancy were held. For example, factors related to timing were felt to appropriately fit within the domain of Timeline. It was decided that the domain of Timeline was relevant in relation to the timing that the vaccination was available (i.e. some vaccinations (such as flu) are available at several seasonal times of the year, whooping cough is available at a certain point in pregnancy), and decisions about vaccination that participants made based on the timing of the vaccination, or the gestation they were when offered it.
Positionality of the research team and reflexivity
The immediate research team consisted of two experienced qualitative researchers working in health sciences. The researchers are independent and not affiliated with any organization providing care to pregnant women. Both researchers have experience in conducting interviews on potentially sensitive topics.
Both researchers have backgrounds in Health Psychology research. The lead researcher has conducted previous research into vaccinations in pregnancy. Both researchers are female and have experienced pregnancy. It is acknowledged that personal views or experiences with vaccinations may have impacted on researchers’ approach to the research. However, as analysis was conducted by two researchers, it was a collaborative and reflexive process, reducing the potential for bias and allowing a deeper and richer interpretation of the data. Reflexivity was considered by the two researchers with ongoing discussions about potential meaning and interpretation of findings. The wider research team has a varied background and expertise, including healthcare professionals, and were involved in discussions about the meaning and interpretation of findings.
Results
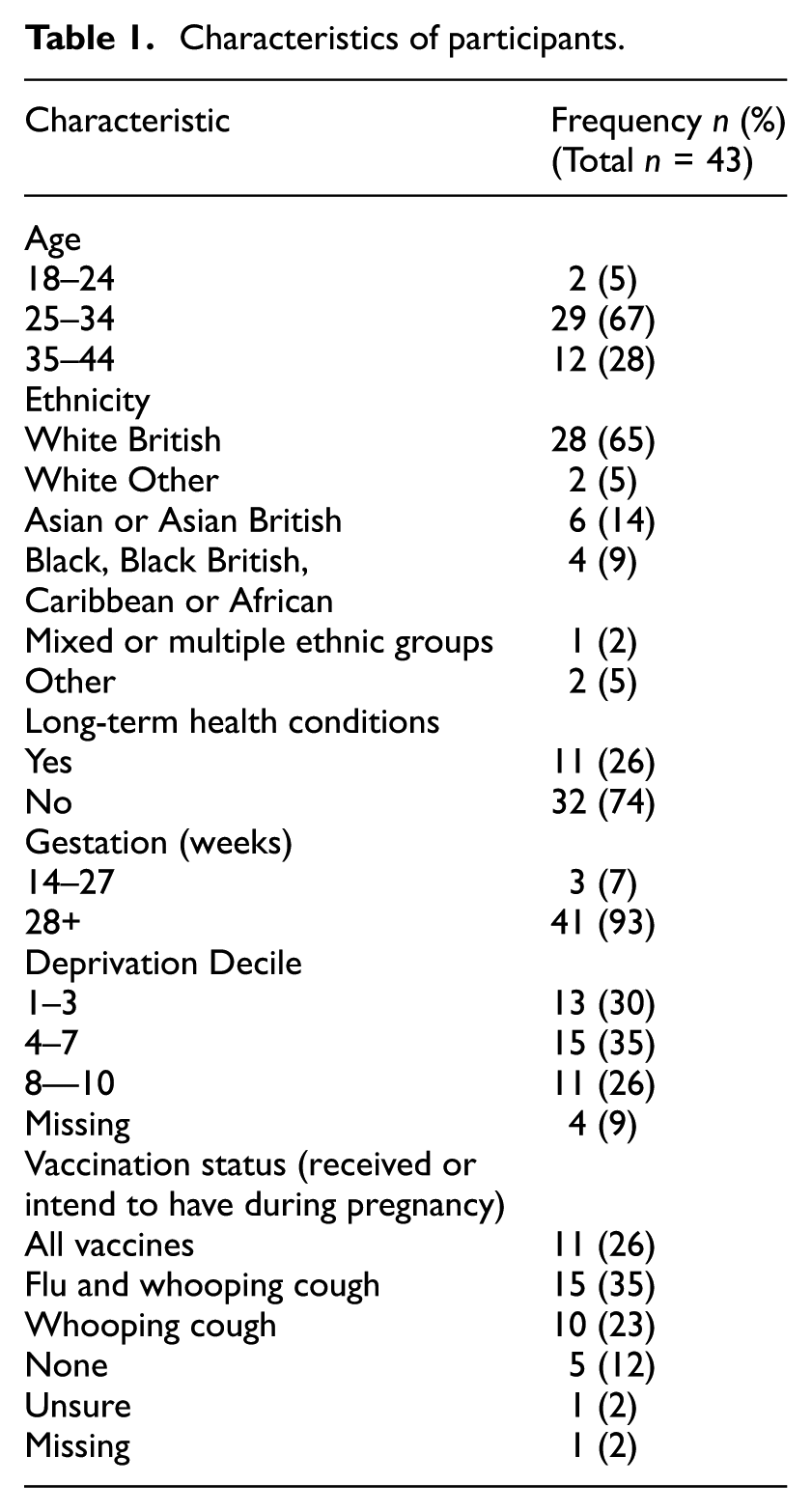
Interviews were conducted with 43 pregnant women. The majority of participants were aged between 25 and 34, and were of White British ethnicity. Characteristics of participants can be found in Table 1. Participants presented with a range of vaccination history during their current pregnancy. No vaccination criteria was placed on the recruitment of participants, with some having received all the available vaccinations, and many combinations of vaccination history. Many participants reported being in favor of vaccinations during pregnancy, yet were still cautious about receiving Covid-19 vaccinations.
Characteristics of participants.
Findings are categorized into the five domains of the IRR Framework (Identity, Cause, Timeline, Consequences and Control), to explain how pregnant women perceive the likelihood and severity of illness, influencing their vaccination decisions. A summary of themes and sub-themes can be found in Table 2.
Themes and sub-themes.
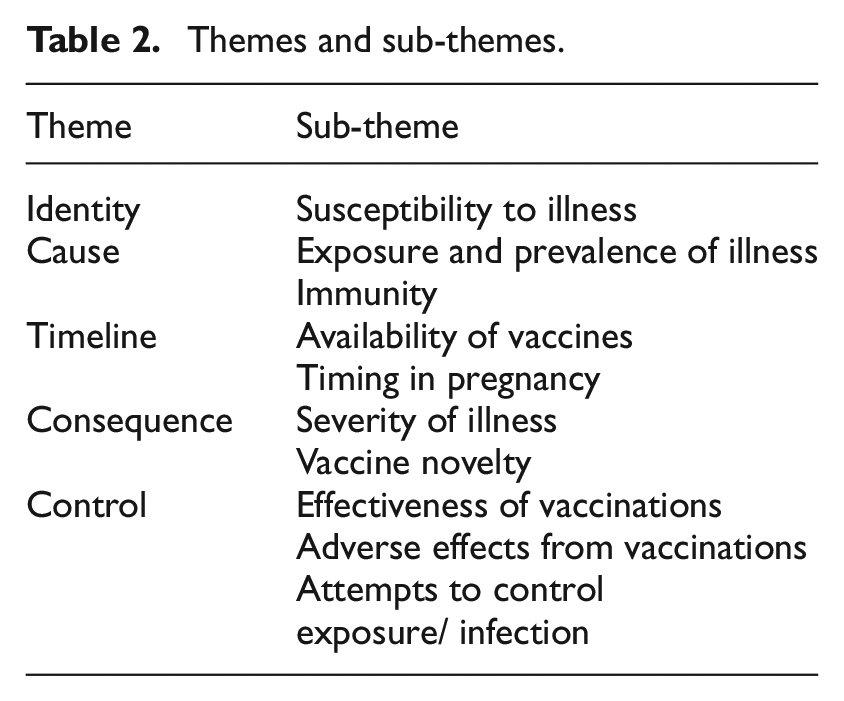
Figure 1 shows how the themes map to the domains of the IRR.
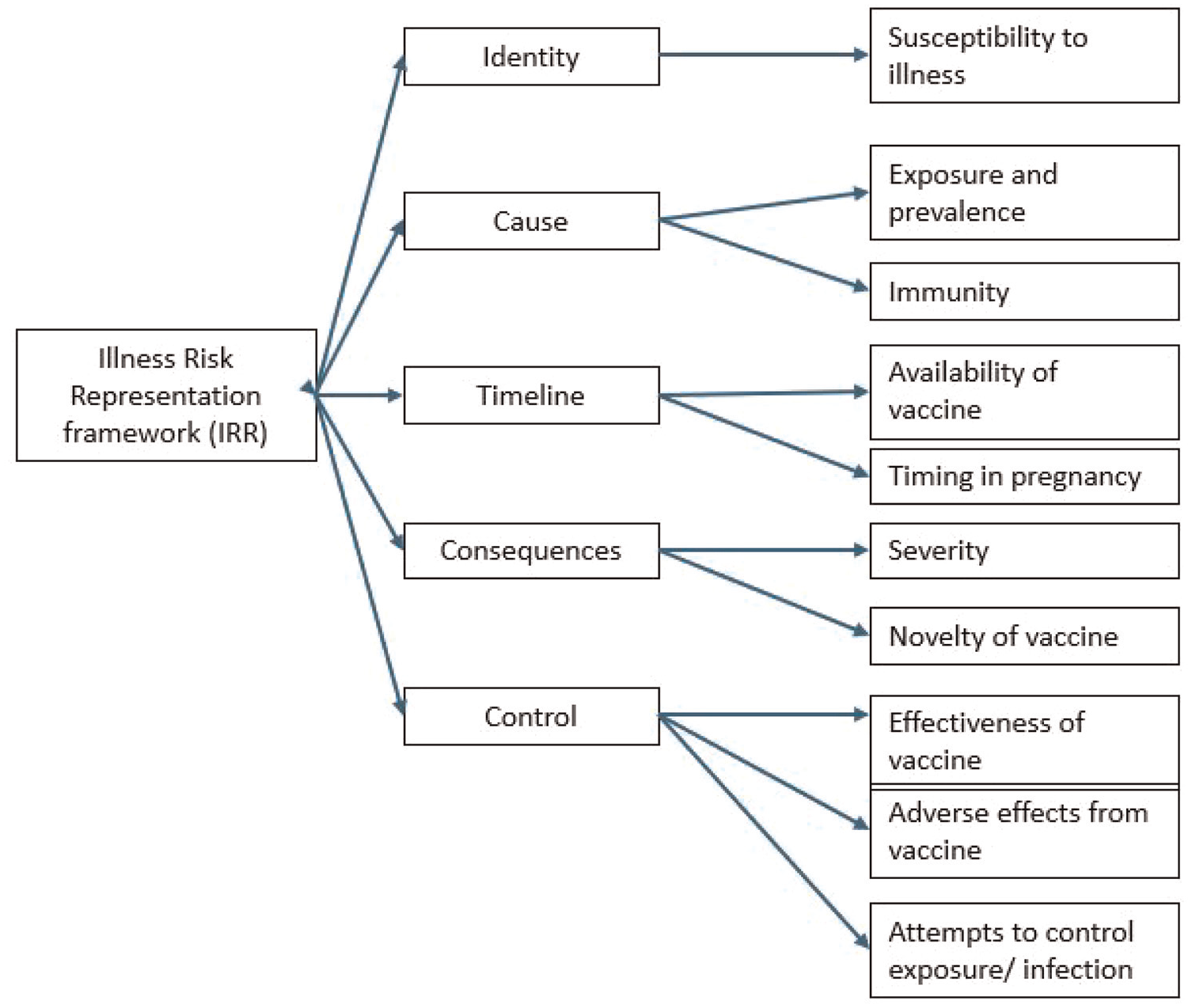
Themes mapped to the IRR.
Identity
Beliefs about identity contribute to estimates of likelihood, impacting on how at risk from illness an individual feels.
Susceptibility to illness
Some pregnant women acknowledged that they felt at greater risk of flu and Covid-19 as a result of being pregnant. This was attributed to a perception that they were potentially more vulnerable whilst pregnant, as a direct consequence of the pregnancy and therefore it was more likely that they could become ill, often influencing the view to accept vaccinations.
But because I’m pregnant, I’m just a bit more aware. And … my husband is very aware as well. Like, if we’re, go somewhere, and there’s anyone who’s ill, we’ll both, like, not … like, keep away or not go. (P11) And really without pregnancy I would not take. But in pregnancy, because you’re more aware you’re vulnerable and also for baby, I will take it to be on the safe side. (P29) Like, I didn’t look into it massively but, like, people have been having the flu jab for a very long time and I already know that I can’t fight the flu as well while pregnant because my body’s not working for me, it’s working for the baby. (P26)
For other pregnant women, being pregnant did not make them feel more at risk from getting ill from flu or Covid-19, as they did not consider pregnancy to make them more vulnerable than pre-pregnancy. This feeling was often justified with a belief that their general health was good, and this was not changed by being pregnant. This belief that they were not susceptible to illness contributed to decisions not to accept vaccinations.
I’m not … I don’t feel I’m more at risk because I’m pregnant, unless there is some reason why. But normally, pregnant women tend to be in the high-risk group. Yeah. So … but I didn’t feel … really, that’s why the reason is, also, that I didn’t feel like I needed to have the COVID vaccine as well. (P34) I’m not in any of the danger zones for flu, so I’ve never been offered the flu vaccine before I got pregnant. And so I think that was another thing. If I’d been … If I’d had asthma, or if I’d been susceptible to the flu, then that may have changed my mind, because I would be more likely to get it. (P11) Yeah, I think I feel less at risk of being ill because as I say, positive changes …. on my health, yeah, as a result of it (P35).
Cause
Beliefs about Cause contribute to estimates of likelihood, impacting on how likely individuals feel they will become ill, based on how they perceive the illness is caused.
Exposure and prevalence of illness
Pregnant women’s appraisals of likelihood were influenced by the prevalence of a disease at a specific time, leading to perceptions about how likely it was that they would come into contact with it. Experience of the illness themselves, or seeing other people ill contributed to their perception of how visible the illness was, as well as how much the illness was being talked about in the media. When they perceived a greater risk due to a high prevalence of the illness, participants felt more at risk and this increased adherence to vaccination recommendations. However, when the prevalence of an illness was considered to be less, or they did not feel it was likely they would come into contact with the illness themselves, pregnant women felt less at risk of being exposed to it, and were less concerned and less motivated to receive a vaccination.
I mean, particularly the COVID one, yeah. That was, I mean, it was everywhere, and so that’s why I had those, those jabs. (P8) But yeah, I, I don’t really feel like we’re in it, really … now, myself, especially… even being pregnant, in the hospital and things like that. It doesn’t feel like … (P9)
Feelings about Covid-19 appeared to be particularly impacted by visibility, with some pregnant women reporting that they did not feel at risk of Covid-19 as it was perceived as not being as prominent as previously. Hearing less about Covid-19 from others and in the media reduced the visibility and in turn the perception of risk for some participants.
I know that COVID’s a thing, but … I don’t know, I feel like it was all blown up and then, kind of, it’s kind of died down. Yeah. I don’t know. It’s not … I, I don’t think … On a day-to-day basis, I’m not like, Yeah, it’s not quite as, as, ’cause everywhere there was, there was tonnes of place wasn’t there to go and get them at one stage and, yeah, I haven’t, I haven’t been offered or heard or had it mentioned at all really. (P28) And I have, like, anxiety with, like, germs and all things like that. So, I would … it’d probably panic me at the beginning, but as we’ve gone on, I’ve gotten a bit more relaxed about it. (P31)
Immunity
Existing immunity impacted whether pregnant women felt they would get ill. Some felt that they had already built up immunity (from being ill previously or from previous vaccinations) so were not at risk of illness, others felt pregnancy reduced their natural immunity and put them more at risk.
So, I feel that my body has naturally produced… that immunity, and the anti-bodies to fight the infection anyway. So I, I just didn’t want to then put anything more into my body. (P1) Obviously, at the minute, I’ve not really got an immune system, because baby’s taken it all. (P23) I think, yeah, because like, because of, I think when you’re pregnant your body, like, your, your immune system will be lower. (P5)
Timeline
Pregnant women did not discuss views around how long the illness would last or time of onset, but did express issues about the availability of vaccinations, and timing of accepting vaccinations based on their gestation.
Availability of vaccines
Acceptance of vaccinations was sometimes dependent on external factors, such as when the vaccinations are available. This was due to the seasonal nature of some vaccinations (particularly flu vaccination), recommendations of when vaccinations should be taken (such as whooping cough being recommended between 16 and 30 weeks pregnant) and also due to some vaccinations not being available when they wanted them (including changes in Covid-19 vaccination programmes).
I would’ve definitely considered it a bit more. I think if I, like, if I was having a winter baby, for example, then, yeah, I probably would’ve thought about it a bit more … than … I don’t think I would’ve taken the COVID vaccine, but I would’ve considered the flu or the whooping cough. I think, because it’s summer …Yeah. I think I felt a bit more relaxed about it. (P19) So, that was basically mentioned. I think it was, like, in my booking, or in my twelve-week scan by a midwife, had done, I think there was a certain time you had to have it done. I think it was, like, 26 weeks or something P27).
Timing of vaccines
Some participants reported that they had decided to wait until later in their pregnancy, as they perceived the risk from adverse effects from vaccinations to be less, as their pregnancy progressed. Some also reported that they had decided to wait until after their baby had been born to accept vaccinations, as this was perceived to be a safer time to be vaccinated.
I’m not against, like, 100%, like, you know, like, it’s not because I’m against the vaccines and, you know … it just … I’ve already, you know, come this far enough, so I just … Yeah. So, I think …I’ll wait until I have baby, and then maybe I’ll have my booster. (P34) But also, I think they kind of … Like, I was pregnant … in October, I think I found out I was pregnant. So I was very early in pregnancy, and I think I wouldn’t have taken any, any, kind of, vaccination until after I was at least 12 weeks (P19).
Consequences
Beliefs about the consequences of the illness, and how severe they would be are influential in the decision to adopt healthy behaviors (i.e. vaccinations). For pregnant women, consequences to both themselves and their unborn baby are influential in their vaccination decisions.
Severity of illness
There was evidence of fear from pregnant women around the illnesses being discussed. This was a result of seeing other people seriously ill or die from illnesses, fear triggered or exacerbated through the media and society more generally (often perceived by participants as scaremongering), and from recommendations from healthcare professionals that made them feel more at risk of serious outcomes from the illness. This fear often acted as a trigger to accept vaccinations when offered them.
I’ve seen people worse who didn’t have vaccines. Even with the vaccines getting, you know, like, poorly. The risk of COVID, how much people can get sick through COVID. (P34) I’ll be honest, I think it’s of pushed on you, personally. I do think it’s a very pushed, pushed thing, injections, and you’re kind of always told negative things that can happen. (P14)
Pregnant women often underestimated the seriousness of Covid-19, which made them less inclined to accept vaccination recommendations. For these women, the perceived consequences of Covid-19 were not considered enough to impact on their decisions.
I’ve never worried about myself having COVID, I’ll be honest. I’m, I’m a fit, healthy person, and I just … I don’t, I don’t know. I was never somebody who was, kind of, scaremongered, in my opinion, at the start. I didn’t, I never, I never saw it like that. It was a, a, not a nice time for those who, obviously, suffered and died from it, but it wasn’t something I was personally worried about. (P14) Yeah. And I didn’t feel like, I, I, I certainly wasn’t concerned about it to the point that I didn’t want to go to work or I didn’t want to go and be around people. I think it was just, kind of, like, I just, I just felt it was a bit inevitable. Like, “Well, it’s gonna happen. Just need to get it and get it over with,” and just hope that it was mild. (P17)
When participants did recognize the potential seriousness of Covid-19 consequences it was influential in their vaccination acceptance, making them more likely to receive them.
I’ve always been quite aware of, sort of, different illnesses and how it can, you know, sort of, the symptoms associated with it. But I think it just … I think, having seen the pandemic and some pregnant women get really poorly during COVID, when I fell pregnant then … And I, and I suppose, before I even fell pregnant, every time a symptom, sort of, arises, like, it was sort of, “Well, what is this?” I think it did just, sort of, make me, make me a bit more aware …. of what it could be, and start questioning, “Well, what is this? Do I need to be concerned?” (P21) Yeah, ’cause I didn’t really know much about what it’d do to the baby. So when I caught COVID, I was more panicking that, like, “What, what’s gonna happen?” (P25)
Vaccine novelty
The newness of the Covid-19 vaccination meant that participants were concerned about the unknown consequences it may have on themselves and their unborn baby. Long-term evidence on safety was needed by many before they would be happy accepting the Covid-19 vaccination (or any new vaccination proposed).
So, with the existing vaccines like the flu and whooping cough, I know they’re long standing, they’ve had lots of trial testing, sorry trials and tests and things. But with the COVID because, so I was, gosh how, I think I was five months pregnant when, when they started rolling out Pfizer, I think it was, and they initially didn’t confirm whether it was safe and then when they did, it because it was so new I, I wasn’t comfortable, sort of, having it. But that was the main reason to be, as I say, I have had the vaccine since, but yeah, not, just mot while I was pregnant … to protect my, my, my unborn baby really … just in case. (P10) I think that does make an impact, because I … I did, kind of, look into the whooping cough and how long it’s been, been given to pregnant women and that kind of thing, just for my own, my information, really. And you can see it’s been given for a, a number, whole number of years. And so it does cross your mind with COVID, like, there’s not many babies that have been born since the COVID vaccinations, and so there can’t have been that much research on any long-term effects. (P11)
Control
The IRR was extended in 2008, and Control was also considered to include control over prevention (things that can be done to prevent the illness) (Cameron 2008). Beliefs about control relate to how well vaccinations are considered to prevent the illness (their effectiveness), actions individuals feel they can take to control the spread of infection, and things they can do to control their exposure to the illness.
Effectiveness of vaccinations
For many, vaccinations were considered to be the most effective choice to make as a way of preventing illness. Views on whether vaccinations were effective at controlling illness were mixed, with some feeling that they would be an effective way of preventing getting ill, whilst others doubting their effectiveness.
No, because I got it straight after so if I’m, I’m not going to have something if it’s not really going to prevent from getting it. (P20) But I’ve never, never had the flu vaccine before. I’ve suffered with flu once, and yes it was horrible, but I don’t know, I always, I have my reservations about the flu vaccine purely because people seem to get ill after the flu vaccine. So, I have my reservations. But yeah, that’s why I had it, because I was pregnant, that was the only reason I had it. (P38)
Adverse effects from vaccinations
Some participants were concerned about adverse effects from the vaccinations rather than from the illness themselves. Concerns about side effects of vaccinations, to either themselves or their baby often influenced the decision not to vaccinate during pregnancy.
No, no. Just, I’m worried that, I don’t know how my body will react, and, of course, my baby. P22 every time I took the vaccines for COVID I had really bad, like, leg pain for like a week or two, like for two weeks, whatever reason, it left my legs and stuff …. so, I was in a doubt about if I would get it in this pregnancy, because … I, afford the pain again because all three times I took the vaccine, I had the same symptom. (P29) I think the only worry was getting ill when I had the flu vaccine and the whooping cough, I suppose…. Getting a cold and, yeah, being ill. (P12)
Attempts to control exposure/ infection
Some pregnant women felt that they could control the risk of illness, by reducing their exposure to illness by maintain alternative precautions such as increased hand washing, social distancing, or mask wearing. This led them to feel less at risk, and therefore did not feel a vaccination was necessary, as they were controlling their exposure and therefore their likelihood of illness.
yeah, it definitely makes you think more about just protecting yourself and what you could be putting yourself in, situations with COVID or … even with the flu, because I didn’t have the flu jab… I was then extra careful about not being near anybody who was ill, or using sanitizer and masks. (P11) I used to have my flu vaccine routine. You know, we would get given them often, the same working in the hospital… So I never really, like, thought anything of it either way. Like, so, but it’s more so since I’ve thought, no, no, I’m in control of my own health, and I would rather do it through, like, exercising and eating healthily and looking after myself… And then I, then I’m well enough and equipped to fight something that I might get, rather than giving myself something, vaccine, that I don’t know. (P7)
Discussion
Summary of findings
This study shows that knowledge about the risk of illness and effectiveness of vaccinations during pregnancy amongst women was mixed. Pregnant women based their appraisal of risk of infectious diseases on a number of factors. Not feeling vulnerable because of being pregnant, not feeling that there is a lot of the illness around, underestimating the seriousness of the illness, belief in other methods of protection and underestimating the safety and effectiveness of vaccinations were all associated with reluctance to accept vaccinations.
The Illness Risk Representation (IRR) Framework overall appears to provide a good framework to understand the beliefs underlying the risk perceptions held by pregnant women about vaccinations. Some domains fit the beliefs associated with vaccination better than others, but estimates of both likelihood and severity contribute to appraisals of risk.
From the findings of this study “Identity” can help explain reluctance to accept vaccinations amongst this population. Many participants did not feel they were at risk, solely based on their status as a pregnant women. The lack of previous long-term risk factors led to the perception that they were at no greater risk of serious illness than they previously were, with pregnancy alone not always increasing perceptions of risk.
“Cause” helps to explain pregnant women’s acceptance of vaccinations, based on perceptions of how much of the illness is around, and whether women feel they have any immunity to it already, and whether they feel the need vaccinations. “Consequences” contributed to explanations of vaccination acceptance and refusal, with some pregnant women underestimating the severity of illness, whereas others were more aware of the seriousness of becoming ill whilst pregnant.
“Control” helps to understand vaccination decision amongst this population, as participants in this study often believed that vaccinations were not effective at protecting them from illness, and in many cases contributed to decisions not to accept vaccinations whilst pregnant. “Timeline” was the domain that explained vaccination decisions the least in this study, mainly referring to factors outside of anyone’s control, but some pregnant women reported believing that it was safer to wait until later in the pregnancy to accept vaccinations, or even once the baby had been born.
Some of the illness risk representations pregnant women hold appear to have influenced procedure representations (representations or perceptions about the vaccination), and visa versa, making it complicated and difficult to separate at times. This complex interplay between illness and procedural representations is not surprising when many messages and campaigns pregnant women receive about vaccinations and illness, convey messages that merge aspects of the risks of illnesses and efficacy and safety of vaccinations, again making it difficult to look at illness representations and procedure representations in isolation from each other.
Strengths and weaknesses
This study has increased understanding of beliefs underpinning appraisals of risk related to vaccination uptake amongst pregnant women, and provided information about the useability and suitability of the IRR framework in understanding vaccination beliefs and decisions amongst pregnant women. The quality and robustness of the qualitative data analysis was increased by the involvement of two experienced qualitative researchers. The recruitment of a good proportion of participants from non-white British ethnicity is a strength, given that women from black and ethnic minorities are disproportionately affected by low vaccination uptake (Nichol et al., 2023), and serious consequences of illness as a result of the illnesses for which vaccinations are available during pregnancy.
One potential limitation of this study is the focus on recruitment from one geographical area. Despite the area being demographically diverse, one area alone is unable to reflect demographics from the whole of the UK. Additionally, the timing of this study might impact on the views and beliefs underlying perceptions of risk. Interviews were conducted in a largely post-pandemic time, where restrictions and rates of infection were reduced. It is likely that views may have been stronger in the middle of the pandemic, and therefore findings might differ.
It is noted that findings about Covid-19 and the Covid-19 vaccination were analyzed separately to other vaccinations, as it was felt that Covid-19 was such a unique time period and due to the newness of the Covid-19 vaccination, perceptions would potentially differ to that of more routine vaccinations. However, we acknowledge that the Covid-19 pandemic is likely to have influenced pregnant women’s feelings about the more routine vaccinations and their health more widely, so this should be considered when interpreting the findings. This is discussed in more detail elsewhere (Parsons et al., 2024).
There may be some overlap between how findings from this research can map onto domains of the IRR. For example, adverse effects of the vaccination have been attributed to the domain of control (specifically representing control over prevention), whereas they may be considered to be consequences. As consequences within this paper referred more to perceived consequences of the illnesses being examined, it was felt that effects of the vaccination fitted better as a factor within Control over prevention. Again, this links to the point earlier about procedure representations, where separating illness representations and procedure representations in the context of vaccinations is complex.
Comparison to previous literature
Previous research has also shown appropriateness of the Illness Risk Representation Framework in explaining health protecting behaviors. This includes adolescents cardiovascular disease (Newby et al., 2020), Covid-19 protective behaviors (Alegria et al., 2021) and Covid-19 vaccination acceptance (Vollmann and Salewski, 2021). Limited evidence exists explaining vaccination behavior of pregnant women using the IRR, but research examining IRR framework in explaining beliefs about maternal views of whooping cough vaccination reported findings similar to the current study; beliefs related to the domain of control included beliefs that vaccinations are not always effective, and that other prevention or treatment (such as antibiotics) can effectively manage or prevent illness in place of vaccinations (Garg et al., 2018). Systematic review evidence examining factors associated with uptake of pandemic flu vaccination showed results consistent with the current study (albeit not specifically in pregnant women). Low or no perceptions of risk from the effects of flu resulted in lower uptake of flu vaccination, low perceptions of the severity of flu, or that it would only have mild threat to health also resulted in lower uptake or intentions to accept the flu vaccination (Bish et al., 2011). These findings reinforce the use of the IRR in explaining beliefs that contribute to vaccination decisions.
Implications for research and practice
Pregnant women are underestimating their risk of illness, based on beliefs that are unfounded. Interventions to address uptake of vaccinations need to consider and address these beliefs. Interventions should target providing appropriate information about vulnerability and susceptibility to infectious diseases (flu, whooping cough, and Covid-19) during pregnancy, and the seriousness of consequences of infection. Conveying up-to-date and consistent messages about vaccination is essential, including messages about the effectiveness and safety of vaccinations, and making sure healthcare professionals both receive, and relay these messages to pregnant women is paramount. These findings can help ensure appropriate guidance for midwives is available. In line with the Illness Risk Representation Framework (Cameron, 2003), clear and consistent messages, and informed healthcare professionals offering reliable recommendations will also help to activate Procedure Representations which in turn will activate illness risk representations and increased acceptance of vaccinations.
Conclusion
The Illness Risk Representation framework has shown to be a helpful theoretical framework in explaining and understanding how pregnant women make decisions about vaccinations. This framework will be helpful in developing a future theoretically- informed intervention, aiming to target an increase in vaccination uptake amongst this population.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251329680 – Supplemental material for How can the illness risk representation framework be used to explain flu, whooping cough and Covid-19 vaccination uptake amongst pregnant women? A qualitative study
Supplemental material, sj-docx-1-hpq-10.1177_13591053251329680 for How can the illness risk representation framework be used to explain flu, whooping cough and Covid-19 vaccination uptake amongst pregnant women? A qualitative study by Jo Parsons, Cath Grimley, Louise Clarke and Sarah Hillman in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053251329680 – Supplemental material for How can the illness risk representation framework be used to explain flu, whooping cough and Covid-19 vaccination uptake amongst pregnant women? A qualitative study
Supplemental material, sj-docx-2-hpq-10.1177_13591053251329680 for How can the illness risk representation framework be used to explain flu, whooping cough and Covid-19 vaccination uptake amongst pregnant women? A qualitative study by Jo Parsons, Cath Grimley, Louise Clarke and Sarah Hillman in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank Dr Jeff Lambert for his advice and expertise in reviewing a draft of this manuscript, as part of the study advisory group.
Data sharing statement
Data associated with this study are not publicly available. Due to consent and ethical limitations, full transcripts for this study are not available to be shared.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study/project is funded by the National Institute for Health Research (NIHR) [Research for Patient Benefit (NIHR203598)]. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethics approval
Ethics approval was obtained from the Yorkshire & The Humber - Sheffield Research Ethics Committee (REC 22/YH/0283).
Informed consent
Verbal or written consent was obtained prior to the start of all interviews (including consent for anonymised quotations to be included in reports).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.