
Abstract
Background
Pregnant women are at increased risk of complications from flu, but uptake of flu vaccination is below 75% targets. Evidence suggests that changing illness risk appraisals may increase vaccination behaviour. In 2018–2019, researchers, public health specialists, and pregnant women co-designed a short animation targeting (unhelpful) beliefs underlying pregnant women’s flu risk appraisals aiming to promote vaccination uptake.
Aims
This study aimed to examine effectiveness of a digital intervention (animation) in increasing flu vaccination among pregnant women through changing illness risk appraisals.
Method
A prospective study design was used, involving convenience sampling of unvaccinated pregnant women recruited via a Qualtrics Online Panel. Participants received small payments via the panel for survey completion. Risk appraisals and intention to vaccinate were measured at baseline and immediately after intervention presentation (follow-up one). Six months later, a further survey (follow-up two) was administered measuring vaccination behaviour.
Results
Baseline and first follow-up surveys were completed by 411 participants. Watching the animation led to increased appraisals of likelihood of getting flu while pregnant and severity of flu during pregnancy, and increased intentions to accept flu vaccination during pregnancy. Of the 67 respondents who completed follow-up survey two, 38 reported having the vaccination while pregnant.
Conclusions
This study provides evidence supporting the promise of the intervention. Randomized controlled trials are required to produce definitive efficacy evidence. Should such a study prove intervention effectiveness, it could be readily embedded within existing campaigns at national and local levels by public health organizations.
Influenza (flu) does not usually cause serious or long-term problems; however, its impact is heightened for those in at-risk groups including pregnant women. Pregnant women are at increased risk of hospitalization and death as a result of physiological and immunological changes that occur during pregnancy (Knight et al., 2014). Maternal flu also increases the risk of serious consequences to unborn babies, with increased rates of stillbirth, premature birth, and below average birth weight (Campbell et al., 2015; Legge et al., 2014).
Uptake of the flu vaccination during pregnancy is influenced by sociodemographic factors. Previous international literature has shown that women of non-Hispanic black origin, under 25 years of age, living at or below the poverty line were significantly less likely to have had the flu vaccination, than other pregnant women (Centre for Disease Control and Prevention 2013). Furthermore, pregnant women with higher educational achievements were more likely to receive the flu vaccination (Frew et al., 2013; Laenen et al., 2015). These sociodemographic factors associated with the uptake of flu vaccination in pregnancy are replicated in the United Kingdom, with white British women being more likely to accept the flu vaccination than ethnic minorities (Sebghati & Khalil, 2021). Furthermore, vaccination uptake is lower in more deprived areas (52.1%) than least deprived areas (69%) of the United Kingdom (Sebghati & Khalil, 2021), and pregnant women with higher levels of education are more likely to be vaccinated against flu during pregnancy (Sebghati & Khalil, 2021).
Since 2010, pregnant women in the United Kingdom have been categorized as a population at increased risk from flu, and therefore have been eligible to receive free flu vaccinations (Joint Committee on Vaccination and Immunisation [JCVI], 2010). The flu vaccination is proven to be safe to receive at any stage of pregnancy (Regan et al., 2015) and has a good record of effectiveness (Madhi et al., 2014). Despite this, uptake of the flu vaccination in the United Kingdom remains below the desired target of 75% (Public Health England [PHE], 2021). In England, for example, uptake was 43.7% in the most recent flu season for which data are available (winter 2019/20) (PHE, 2020). Reasons pregnant women do not accept recommended vaccinations include concerns over potential side effects of the vaccination, doubts over the effectiveness of vaccinations, and doubts about whether the vaccinations are necessary (Kilich et al., 2020; Sebghati & Khalil, 2021). Furthermore, uptake of flu vaccination is positively associated with vaccination recommendations from a health care professional (Kilich et al., 2020).
Changing individual’s risk appraisals of future illness is a potentially useful strategy for changing health behavior (Brewer et al., 2007; Sheeran et al., 2014; Tannenbaum et al., 2015). Risk appraisals are “people’s beliefs about a potential harm” (Wright, 2010) and are typically conceptualized as the product of likelihood estimates (how susceptible an individual feels to an illness) and severity estimates (how serious the individual considers the illness would be if they were to get it) (Wright, 2010).
Meta-analyses have found that interventions containing risk messages have a significant positive effect on behavior, when examining the role of risk in health behavior change in general (e.g., Sheeran et al., 2014; Tannenbaum et al., 2015), and vaccination specifically (e.g., Brewer et al., 2007; Sheeran et al., 2014).
While this review-level evidence indicates that risk-based interventions can have a positive effect on changing behavior, how best to do this for health behavior in general, or for vaccination behavior in particular, is unclear. As concluded by Tannenbaum et al. (2015), including strong risk and efficacy messages are likely to be important. Other potentially important considerations are using images and visual components to communicate risk (French et al., 2017; Parsons et al., 2018), content being produced by a trusted and respected source (Briñol & Petty, 2009; Kumkale et al., 2010), and providing clear and meaningful explanations of how the pathogen (e.g., flu) causes harm and of how the proposed action (e.g., vaccination) works to reduce or remove that harm (Bishop et al., 2005).
Development of the Intervention
In November 2018, an intervention aiming to increase the uptake of flu vaccination among pregnant women was developed as a result of a collaboration between behavioral scientists, pregnant women, midwives, clinicians, and public health professionals. The animation is approximately 4 minutes long, is informed by Intervention Mapping (Bartholomew Eldredge et al., 2016) which ensured that it was based on theory and evidence, as well as being grounded in the needs and preferences of the target population. It addresses beliefs about the risk of flu and the efficacy of the vaccination, using animated messages and relatable characters to convey information to pregnant women. The animation informs pregnant women about the risks of flu to themselves and their unborn baby (risk appraisal). Estimates of severity are targeted by describing the consequences it can have on both themselves and their unborn baby, and likelihood is targeted by clearly explaining why pregnant women are at increased risk of complications. The animation also informs pregnant women about the effectiveness of the flu vaccination by showing how the vaccination works to protect pregnant women and unborn babies from flu. In addition, messages about the ease of vaccination are communicated by demonstrating visually how the vaccination is administered.
The content and the messages within the animation were informed by a qualitative study, which identified knowledge gaps across a sample of 24 pregnant women recruited from community and hospital settings. This qualitative research identified that pregnant women underestimate their vulnerability to flu, underestimate the severity of flu to themselves and their unborn baby, and identified that pregnant women thought the flu vaccination was a live vaccine (Parsons, 2019). The animation was designed to target all of these knowledge gaps. Despite this qualitative study aiming to recruit a diverse range of pregnant women, the majority of women were white British, and therefore the beliefs targeted by the animation reflect the demography of the qualitative sample (Parsons, 2019). A detailed description of the intervention and its development can be found elsewhere (Parsons et al., 2021) but is described briefly here. Screenshots of the completed animation can be found in Supplemental Appendix 1.
The animation was specifically designed to provide lay explanations, and simple visual demonstrations of the processes involved in the pathogen infecting pregnant women, and how the flu vaccination works to disrupt it. Straightforward descriptions of ingredients in the vaccination, how it is manufactured, and how it works to protect pregnant women and unborn babies were also provided in an attempt to demystify the processes, rectify any misconceptions and reassure pregnant women about the safety and effectiveness of the vaccination.
The Study
This study aimed to examine the effectiveness of the animation in increasing risk appraisals and subsequent flu vaccination uptake among pregnant women using a prospective study design. This design was chosen for pragmatic reasons (such as time and financial restraints), but care was taken to make appropriate choices with regard to the timing and type of measures used to avoid errors associated with using correlational data to examine the association between risk and behavior (Weinstein et al., 1998). The intention of this study was to contribute to understanding about what works to increase risk appraisals, and also to the broader body of evidence about the relationship between risk and behavior.
Aims
To examine whether the animation is effective in increasing pregnant women’s appraisals of the severity and likelihood of flu and their intention to have the flu vaccination while pregnant.
To examine whether watching the animation leads pregnant women to have the flu vaccination during their pregnancy.
Method
Surveys
The intervention aimed to increase vaccination behavior through changing pregnant women’s risk (conceptualized as likelihood and severity) and efficacy (conceptualized as self-efficacy and response-efficacy) appraisals. The survey was designed to measure the main targeted behavioral determinant only (risk).
This was a prospective study design. Prior to receiving the intervention (baseline), and immediately afterward (follow-up one), participants were asked to complete a short survey measuring risk appraisals. Approximately 6 months later, a further short survey (follow-up two) was administered to measure vaccination behavior. Single-item measures of study variables (severity, likelihood, and vaccination intentions and behavior) were employed to keep the survey short in an attempt to maximize recruitment and retention. The surveys were delivered via Qualtrics survey software. Items used in all surveys can be found in Supplemental Appendix 2.
Participants
To take part, individuals had to be signed up to the Qualtrics participant pool (people who have expressed an interest in taking part in research). The inclusion criteria were as follows: female, over the age of 18, pregnant, living in England, and not having received the flu vaccination during that flu season. Pregnant women who had already had the flu vaccination that season (due to pregnancy or other at-risk factors) were not eligible to participate, and therefore did not complete the survey or view the animation.
Recruitment and Procedure
All those who met the inclusion criteria were invited by Qualtrics to participate in the study.
Informed consent was obtained using an online consent form. Participants were required to confirm that they had read and understood the participant information sheet, seen immediately prior to presentation of the consent statements, that they met the inclusion criteria, and that they agreed to participate.
Qualtrics distributed the baseline survey to all eligible participants (during October and November 2019). They were then asked to watch the animation. This was followed immediately by the first follow-up survey. Six months later (during March and April 2020), participants were sent a link by Qualtrics to the second follow-up survey.
Statistical Analysis
All analysis was performed using SPSS. Data were initially analyzed descriptively. Differences between baseline and follow-up one scores were examined using paired t tests, and effect sizes were calculated using Cohen’s d (Lakens, 2013). There were significant nonnormal distributions in all the independent variables so bootstrapping within SPSS was used when performing the analysis.
The follow-up two data set was analyzed initially with frequencies and percentages before being analyzed alongside the baseline/follow-up one data set. In the follow-up two survey, those who were no longer pregnant answered the question, “Did you have a flu vaccination while you were pregnant?,” and those who were still pregnant at the time of follow-up answered the question, “Have you had the flu vaccination so far during your pregnancy?” Answers were combined into one dichotomous variable “had vaccination in pregnancy” which was used as the dependent variable in the multivariate statistics. The follow-up one values of likelihood of getting flu (measuring perceived likelihood), seriousness of flu during pregnancy (measuring perceived severity), and intention to get vaccinated during pregnancy were used as predictors in a univariate logistic regression to find individual odds ratios. Values significantly predicting behavior (having had the vaccination at follow-up) were then entered into a multivariate logistic regression. Using the power calculation defined by Cohen (1992), for sufficient power of 0.80, for multiple regression with two independent variables, a minimum of 67 were required in each group (i.e., those who had the vaccination and those who did not).
Assumptions of linearity (Box & Tidwell, 1962) (Supplemental Table S1) and multicollinearity (Variance Inflation Factor (VIF) and tolerance levels; Supplemental Table S2) were tested within SPSS prior to performing the logistic regression (Supplemental Material). In addition, residuals were checked for outliers and influencing cases (Supplemental Table S3). Relationships between the variables from the regression model were analyzed using mediation analysis in SPSS with the PROCESS macro (Hayes, 2018).
Ethical Approval
Ethical approval was granted by Coventry University ethics (project reference: P96086).
Results
The baseline and follow-up one surveys were completed by 411 participants, and of these, 67 (16.3%) went on to complete the follow-up two survey.
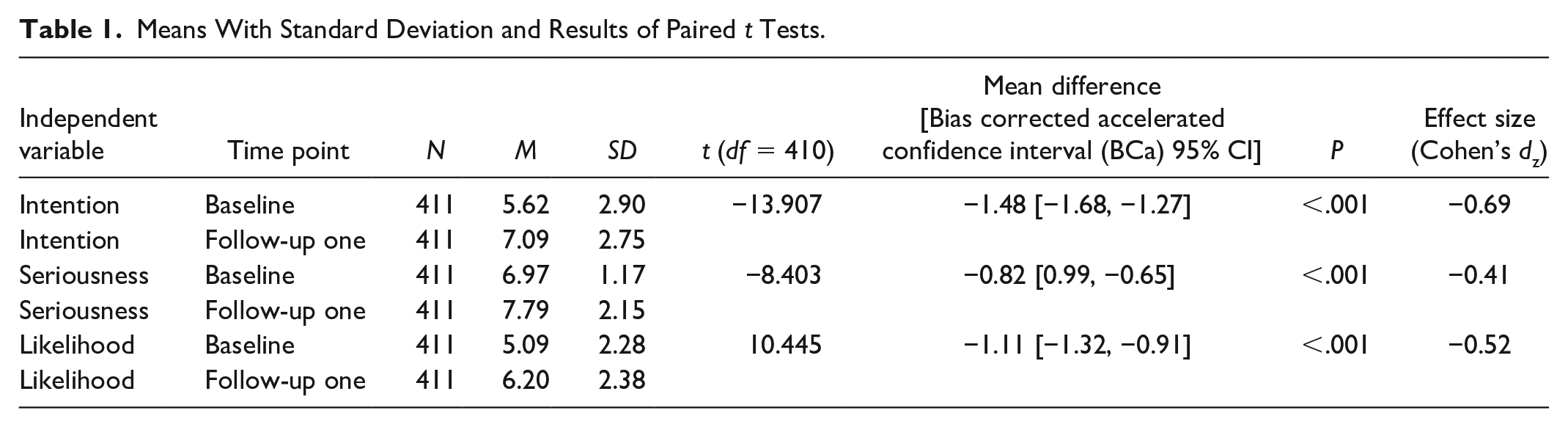
Results of paired t tests showed that intention to have the flu vaccination during pregnancy was significantly higher after watching the animation (Table 1). Participants’ perception of the likelihood that they would get flu while pregnant significantly increased after watching the animation, as did their perception of the severity of flu while pregnant.
Means With Standard Deviation and Results of Paired t Tests.
Follow-Up Data Descriptive Statistics
Sixty-seven participants completed the follow-up survey at time two. Of these, 43 reported that they were no longer pregnant, and a total of 38 (57%) received the flu vaccination. Of the women who were no longer pregnant, 23 (53.5%) reported having the vaccination, and 20 (46.5%) had not. Out of the 24 women who were still pregnant at the time of completing the follow-up survey, 15 (62.5%) had received the vaccination, and nine (37.5) had not. Of the nine who had not at that point had the vaccination, three (33.3%) reported that they did not plan on having it, four (44.4%) said they were unsure whether they would have it, and two (22.2%) said that they did plan on having it (see Figure 1 for flowchart). For those completing follow-up two, 28 of 49 (57.1%) who reported a higher intention to have the vaccination (score ≥ 6 out of 10) at follow-up one went on to have the vaccine. At baseline, 21 of the 27 (77.8%) participants reporting a higher intention to vaccinate (score ≥ 6 out of 10) who participated in follow-up two went on to have the vaccine.
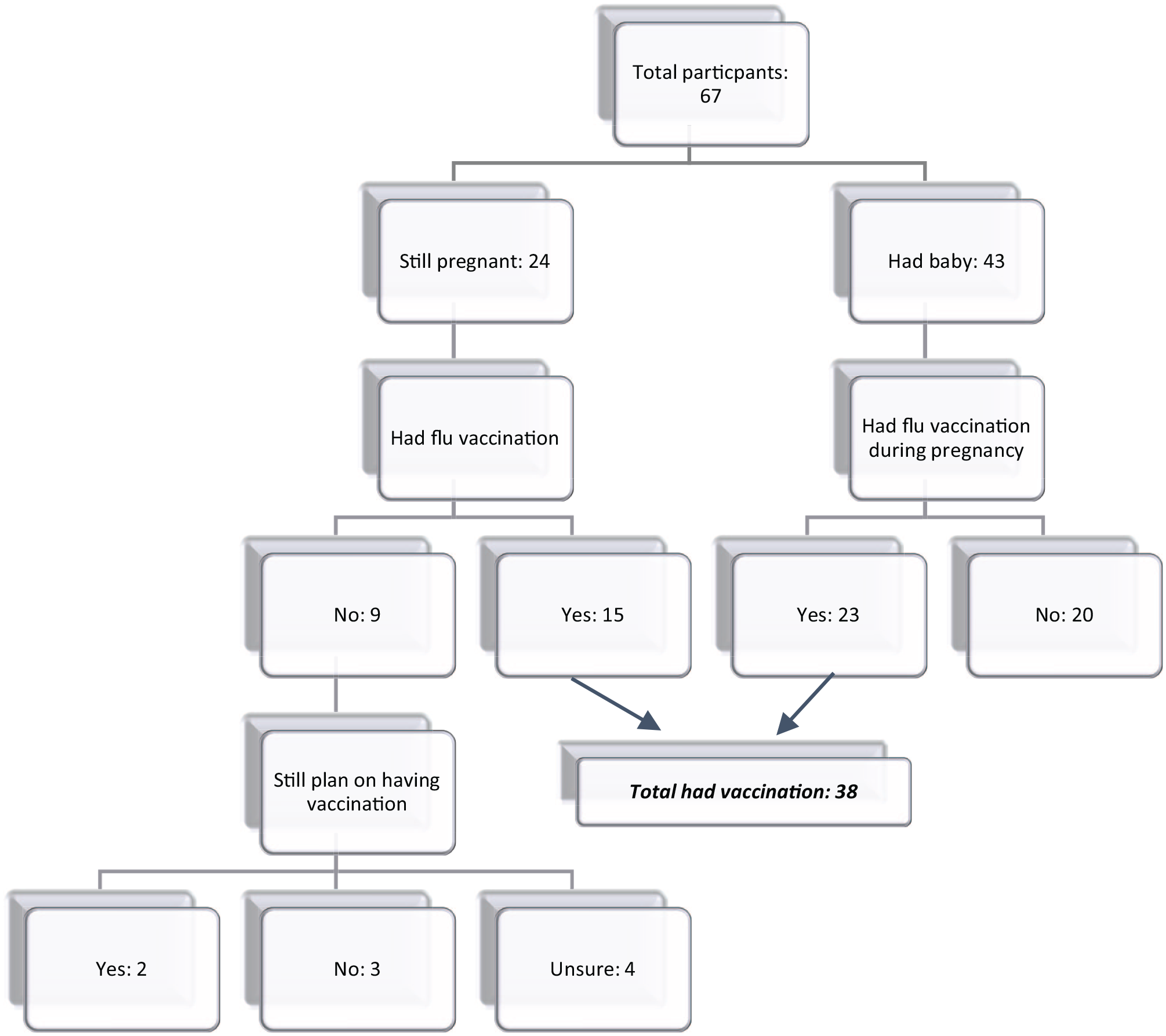
Follow-up two participants’ responses.
Prediction of Flu Vaccination From Postintervention Variables
Univariate logistic regression was performed on the three postintervention variables. Likelihood of getting flu during pregnancy and intention to have the flu vaccination both significantly and positively predicted having the flu vaccination (Table 2). There was no relationship between perceived severity and vaccination behavior (Table 2).
Univariate Logistic Regression on Predicting Flu Vaccination.
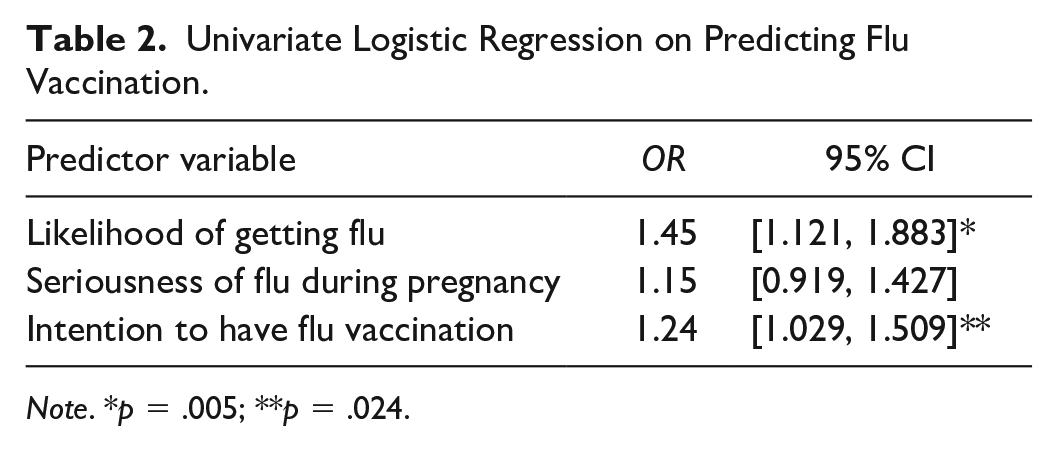
Note. *p = .005; **p = .024.
Multivariate binary logistic regression was performed (n = 66) with having had the flu vaccination during pregnancy versus not having it as the outcome variable (Table 3). The predictor variables entered into the model were intention to have the vaccination and the likelihood of getting flu if not having the vaccination. The model significantly predicted having the flu vaccination, chi-square=10.149(2), p = .006. The model accounted for between 14% and 19% of the variance in having a flu vaccination, with 78.9% of those having a vaccination being correctly predicted, 46.4% of those not having a flu vaccination being correctly predicted, and 65.2% overall. Only the likelihood variable was a significant positive predictor of having the flu vaccination, so that as perceived likelihood of getting flu increased so did the likelihood of having the flu vaccination, B = .32 (p = .026) 95% BCa CI [−.029–0.78], OR = 1.37 95% CI [1.012–1.861]. Examination of residuals revealed no outliers or significant influence of individual variables in the model (see Supplemental Table S3).
Logistic Regression Model for Predicting Having the Flu Vaccination.

Note. R2 = .143 (Cox & Snell, 1989); .192 (Nagelkerke, 1991). Model χ2 =10.149, p = .006.
Mediation analysis showed a significant indirect effect of intention to vaccinate on having the vaccination through its relationship with the likelihood of getting flu, b = 0.16, BCa CI [0.01, 0.39]. Figure 2 shows the mediation model.
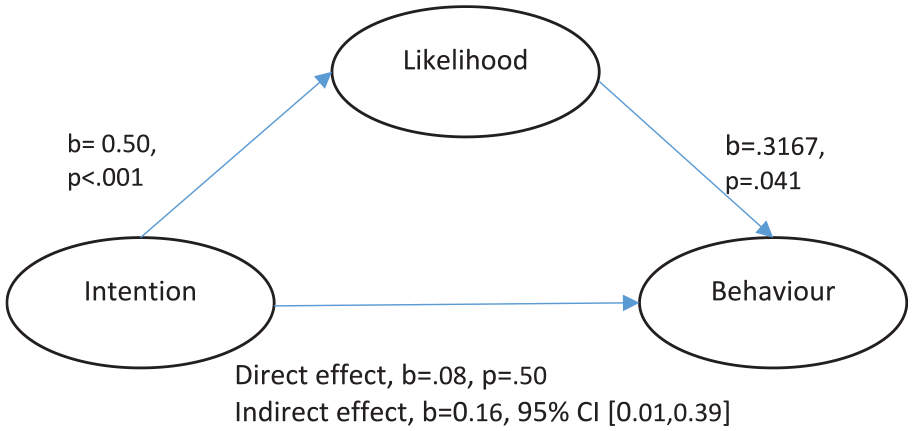
Mediation model.
Discussion
Summary of Main Findings
This study shows some promise of the intervention. It suggests that watching the animation may have contributed to an increase in participants’ appraisals of the likelihood of getting flu while pregnant, their appraisals of the severity of flu during pregnancy, and also their intentions to have the flu vaccination during their pregnancy. Of the 67 respondents who completed the second follow-up survey, 38 reported having had the vaccination while pregnant. This equates to 57% of the follow-up sample receiving the flu vaccination, which is higher than the latest uptake figures for pregnant women of 43.7% reported for the 2019/2020 flu season (PHE, 2020). However, it is likely that recruiting participants from a Qualtrics pool (individuals that have expressed an interest to participate in research) may not be representative of the general pregnant population of the United Kingdom.
The results showed that vaccination behavior was predicted by participants’ appraisals of the likelihood of getting flu while pregnant and also their intentions to get the vaccination. The higher these values, the higher the likelihood of having the vaccination. Furthermore, women’s perceptions of the likelihood of getting flu without the vaccination was a mediator and explained the relationship between intention to have the vaccination and then having the vaccination. Overall, these findings provide a signal of efficacy in support of the intervention as an effective tool for increasing pregnant women’s appraisals of the risk of flu, and then in turn, in increasing vaccination behavior.
Strengths and Limitations
The findings of this study should be interpreted in the context of its limitations. First and foremost, a prospective study design was used instead of an experimental design. This means that it is not possible to infer causality from the results. The risk appraisals and vaccination decisions of women taking part in the study may, for example, have been influenced by factors other than the intervention, such as local public health campaigns operating in parallel. It is also possible that recording participants’ intentions to vaccinate, severity, and likelihood immediately after exposure to the intervention introduces the potential for bias in the results. These results however are interesting as this provides evidence of the process of change (i.e., a change of vaccination intention through a change in risk appraisals).
Furthermore, the fact that demographic information was not taken from participants is a further limitation of the study and makes it impossible to examine demographic considerations of the uptake of flu vaccination as a result of the animation. However, due to the nature of recruitment, this study was able to recruit pregnant women from anywhere in the United Kingdom, rather than one health center, or one geographical area, thus increasing the potential to reach a varied sample of pregnant women.
The low number of women who took part in the follow-up survey should also be considered. Only 67 of 411 participants responded to the follow-up survey, resulting in the analysis being underpowered to detect small effect sizes in intervention risk variables on behavior. It is possible that with an increased follow-up data set available, the study would have been sufficiently powered to also detect a relationship between perceived severity of flu and flu vaccination uptake, as it almost reached the significance value. Furthermore, insufficient numbers of participants in the follow-up meant that there were too few participants who were still pregnant and had not yet had the flu vaccination but still intended to vaccinate, to run analyses to determine whether the intention to vaccinate at follow-up had been influenced by the intervention.
This intervention is aimed at targeting an increase in flu vaccination among pregnant women who are hesitant about vaccinations, ambivalent, or undecided, rather than those who have strong feelings against vaccinations. One limitation of this study is the inability to determine views about vaccinations among the survey sample. It is likely that participants had favorable feelings about the vaccination, which motivated them to participate. However, as this study has obtained measures of likelihood, severity, and intention to vaccination both before and after viewing the animation, we can directly observe the change in these scores, to provide a reasonable measure of effectiveness of the animation.
A number of choices were made to minimize participant burden and in doing so maximize recruitment and retention but which present limitations to the study. The study did not control for prior behavior. Ideally, participants should have been asked about whether they had had the flu vaccination within any prior pregnancies and for this to have been controlled for in the analysis. Prior behavior has the potential to influence both the size and the direction of the relationship between measures of likelihood and behavior. Given that past vaccination behavior is likely to have differed within the participant sample, it would have been preferable to control for this. In addition, the survey used did not measure efficacy appraisals, despite the animation targeting both risk and efficacy appraisals. As discussed earlier, simultaneously targeting risk and efficacy appraisals increases the likelihood of interventions being effective (Rogers, 1983; Rosenstock, 1974; Witte, 1992). While failure to measure efficacy appraisals does not undermine the findings obtained, and potentially explains for the increase in participant’s intention to vaccinate after watching the animation, it does present a missed opportunity to examine what works to increase these beliefs and also their relationship with risk and behavior. Finally, single-item measures of all constructs were used which are less reliable than composite measures (van der Velde et al., 1996). It would also have been useful for increasing understanding of factors that heighten intention to vaccinate during pregnancy, to have asked participants at follow-up whether watching the animation had led them to have the vaccination, or whether their decision had been influenced by discussions with, or advice from health care professionals.
Nonetheless, the prospective design used, the measurement of risk before and after presentation of an intervention, and the use of conditional measures of likelihood are all design considerations recommended when examining the relationship between risk and behavior using correlational data (Weinstein et al., 1998) and as such increase confidence in the observed findings.
Implications for Research and Practice
This animation appears to be a useful tool, which shows promise in increasing pregnant women’s intention to have the flu vaccination, perceived likelihood and perceived severity, which have shown to increase the uptake of flu vaccination among this population.
The animation looks promising as an intervention to be easily implemented into existing campaigns, or as a standalone piece aiming to provide pregnant women with the information needed to make their vaccination decisions. It is anticipated that the animation will be implemented into campaigns at both national (delivered by Public Health England) and at local levels (within local authorities), predominately delivered digitally through web content and social media messaging. This animation is ideally suited to distribution as part of these campaigns and would benefit from being endorsed by these bodies. The development of the animation was completed in conjunction with public health experts at local and national level and midwives, to ensure accuracy of the content. This enabled the animation to be developed in a way that would make it suitable for future endorsement. Embedding this animation within campaigns is technically simple, as it can easily be hosted on publicly accessible websites, with links embedded within relevant websites and social media posts.
Strengths of this type of intervention lie in the fact that it is an inexpensive approach to deliver at scale and meets the current appetite for video content on social media. The main disadvantage to this type of intervention is that the flow of information to pregnant women is one directional, with no opportunity for misunderstandings to be corrected, and no opportunity for any questions to be answered. This however is no different to other materials currently being included in campaigns.
Future testing of the animation’s effectiveness should include a full randomized controlled trial (RCT) to establish whether increases of flu vaccination among pregnant women are directly attributable to watching the animation itself. Previous literature has shown that efficacy (in addition to risk) needs to be high in order for risk to have a positive effect on changing behavior. For this reason, further experimental research involving participants being shown a version of an animation about vaccination, which manipulates risk alone, an animation that manipulates efficacy alone, and an animation that manipulates both risk and efficacy appraisals, will allow for further exploration of the relationship between risk and efficacy on changing vaccination behavior. It would also be beneficial to explore with participants which elements of the animation they feel works to influence their perceptions of vaccination and their intentions to receive the vaccination. A qualitative study to determine which elements of the animation were most influential would be a useful next step to better understand the role and effectiveness of such interventions.
This study provides evidence to suggest the promise of the intervention. Future research on the effectiveness of the animation, such as the proposed RCT would confirm whether this is an appropriate intervention to increase the uptake of flu vaccination during pregnancy. It will help researchers to understand why only 57% (n = 38) of pregnant women in follow-up two reported having the flu vaccination following the intervention, despite 75.4% (n = 310) expressing the intention to vaccinate at follow-up one. This would increase understanding of the factors involved in pregnant women’s vaccination decision making and would help to understand the gap between vaccination intention and eventual behavior within this population (Webb & Sheeran, 2006). This intervention is aimed at people who are vaccine hesitant or ambivalent rather than those with anti-vaccination views. An RCT would be beneficial as it would help to increase understand the differences in factors affecting vaccination decisions of pregnant women who are generally in favor of vaccinations, those who are strongly against vaccinations, and those who are ambivalent to vaccinations.
Should future testing prove the animation to be effective, it would be easily and cost-efficiently embedded into existing social media campaigns delivered at national and local levels by public health organizations in the United Kingdom. This would allow practitioners to provide pregnant women with a resource to accurate and appropriate information that will inform them of their susceptibility to flu and the seriousness of the consequences of flu. Ultimately, increases in uptake of flu vaccination among this population has benefits for pregnant women, unborn babies, and the wider health care system, both in health and mortality of pregnant women and the cost of consequences from flu to the UK National Health Service (NHS).
Should this animation prove to be an effective intervention to increase flu vaccination in pregnancy, it can offer valuable learning about the use of such interventions in targeting other vaccinations in this population, for illnesses such as COVID-19 given the increased risk that pregnant women are considered to be in (UK Obstetric Surveillance System (UKOSS), 2021). Furthermore, this type of intervention could also be useful in targeting vaccination behavior in other populations (such as other age groups at risk from COVID-19).
Supplemental Material
sj-docx-2-heb-10.1177_10901981221077935 – Supplemental material for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women
Supplemental material, sj-docx-2-heb-10.1177_10901981221077935 for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women by Joanne Parsons, Catherine Grimley and Katie Newby in Health Education & Behavior
Supplemental Material
sj-docx-3-heb-10.1177_10901981221077935 – Supplemental material for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women
Supplemental material, sj-docx-3-heb-10.1177_10901981221077935 for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women by Joanne Parsons, Catherine Grimley and Katie Newby in Health Education & Behavior
Supplemental Material
sj-docx-4-heb-10.1177_10901981221077935 – Supplemental material for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women
Supplemental material, sj-docx-4-heb-10.1177_10901981221077935 for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women by Joanne Parsons, Catherine Grimley and Katie Newby in Health Education & Behavior
Research Data
sj-xlsx-1-heb-10.1177_10901981221077935 – for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women
sj-xlsx-1-heb-10.1177_10901981221077935 for Effectiveness of a Digital Intervention in Increasing Flu Vaccination–Related Risk Appraisal, Intention to Vaccinate and Vaccination Behaviour Among Pregnant Women by Joanne Parsons, Catherine Grimley and Katie Newby in Health Education & Behavior
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by an internal award from Coventry University to demonstrate impact of the team’s research for REF purposes.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.