
Abstract
Research indicates relationships can support post traumatic growth (PTG) following spinal cord injury (SCI). However, knowledge of this area is limited. Thus, the study aimed to explore the role of relationships and perceived support in PTG development. Eleven semi-structured interviews were conducted with participants who had acquired SCI in adulthood. Constructivist Grounded Theory was utilised for analysis. Tracy’s qualitative markers were used to ensure quality and rigour. Findings showed SCI can disrupt core beliefs, triggering cognitive and behavioural re-evaluation processes to rebuild beliefs, and experience PTG. Three inter-related themes of how relationships support these processes were revealed: ‘a safe place to get back on your feet’; accepting and valuing me and enabling learning and independence. Relationships can support PTG processes through providing emotional safety, enabling exploration of self and supporting self-acceptance. A tentative theoretical model is provided, with implications for PTG theories and recommendations for clinical practice.
Keywords
Introduction
Spinal cord injury (SCI) is a life changing event, bringing substantial physical, social and psychological impacts on the individual (Ahuja et al., 2017). Not only are individuals required to adapt to considerable physical changes in mobility and function and manage multiple physical health complications (Ahuja et al., 2017), they also face psycho-social losses and challenges (Dickson et al., 2008). However, in adjusting to SCI there is potential for positive psychological changes and personal growth (Byra, 2016; January et al., 2015). Calhoun and Tedeschi’s (2001), Tedeschi and Calhoun’s (2004), Tedeschi et al.’s (2018) model of post traumatic growth (PTG) proposes that trauma or highly challenging events, such as that experienced by people with SCI, represents a significant disruption to life goals and core beliefs about the self, world and others, and triggers deliberate and ruminative processes as the individual attempts to make sense of their experiences and rebuild core beliefs. PTG is predicted to occur in several domains, including appreciation of life, sense of priorities, relationships, sense of personal strength, recognition of new possibilities, spiritual development and personal narrative (Tedeschi et al., 2018; Tedeschi and Calhoun, 2004). Evidence is accumulating that it is possible to experience growth in all domains post-SCI (Byra, 2016).
Research shows SCI can lead to the rupture of the fabric of everyday life resulting in disruption of identity, described by Bury (1982) as ‘biographic disruption’ (Bourke et al., 2015; Dickson et al., 2008). SCI can impede the individual’s participation in social, leisure, work and daily activities, which can cause disruption to the individual’s perception of self (Dickson et al., 2008). SCI can also lead to movement of ‘one social world to another’ (Denzin, 1992), as the individual suddenly becomes a member of a new social minority group: people with disability (Dickson et al., 2008). Therefore, the individual is required to explore and determine how their self-concept has been impacted, as part of reconstructing their identity (Adler et al., 2021) or core beliefs (Tedeschi et al., 2018). Qualitative studies have shown the process of reconstructing identity to be a central pathway to PTG following SCI (Crawford et al., 2014; Griffiths et al., 2012; Wang et al., 2017).
The notion of ‘self’ is defined as a concept constructed through reflexive interactions with others (Clarke and James, 2003). Calhoun and Tedeschi (2001) also recognise the role of social factors in PTG development. Consistent with this, research indicates relationships could be important in supporting PTG processes, such as by providing opportunities for self-disclosure, enabling coping, supporting exploration of capabilities post-SCI and providing continued acceptance (Chun and Lee, 2010; Griffiths et al., 2012; Wang et al., 2017). Advice from a lived experience perspective has also been shown as supporting PTG through providing information about how to manage challenges, enabling the individual to live well and influencing beliefs about future possibilities (Khanjani et al., 2017).
Aims of present study
Studying PTG, and its processes, is clinically relevant in providing insights into how individuals adapt and rebuild following life-changing events. Growing evidence indicates relationships play an important role in supporting PTG processes and highlights the need to ascertain relationship factors following SCI (Chun and Lee, 2010; Griffiths et al., 2012; Kennedy et al., 2013). Therefore, the aims of this qualitative study are:
To investigate the role of relationships, including romantic, familial, friendships and peers with lived experience of disability, and perceived support in PTG development following SCI;
To explore the interaction between relationships and cognitive processing in PTG development.
Method
Constructivist Grounded Theory (CGT; Charmaz, 2006, 2014) was utilised as the research aims, to understand how the individual’s experience of PTG is supported and constructed within their relationships, were congruent with the theoretical underpinnings of social constructionism of CGT. CGT culminates in theory building suited to future research and clinical understanding (Charmaz, 2014), which was also deemed useful.
Recruitment
The study was approved by Cardiff University ethics committee. Participants were recruited via a SCI charity website and social media page. Potential participants made contact via email and were provided an information form, and email or phone call to assess eligibility and facilitate informed consent.
Inclusion criteria were utilised to assess eligibility: (1) over 18 years; (2) living with SCI; (3) able to communicate in English; (4) at least 1-year post-SCI; (5) sustained injury in adulthood (16 years+) and received rehabilitation input from adult services and (6) reports experiencing growth from adjusting to SCI. Exclusion criteria were also applied: (1) significant cognitive difficulties inhibiting informed consent or recall of lived experiences and (2) sustained injury during childhood.
Seventeen individuals expressed interest. One person did not meet inclusion criteria (less than 1 year post-SCI), two expressed interest only, one cancelled their interview and two made contact after data saturation was reached and recruitment had closed. Eleven individuals took part.
Data collection and procedure
Semi-structured interviews were utilised to enable the researcher to co-construct the interview with the participant and to support reaching data saturation by adapting the questions to make links between participants’ accounts (Charmaz, 2014; Foley et al., 2021). Interviews were completed by the first author via Skype (n = 10) or telephone (n = 1). Participants reviewed a consent form and were able to ask questions before providing verbal consent. Participants completed a demographic form and post-interview psychometric measures. Interviews were audio recorded and lasted 39–66 minutes (mean 55.33). To safeguard participants, verbal and written debriefs were provided, and a risk assessment pathway followed.
Measures
Demographic and psychometric information was obtained to situate the sample (Elliott et al., 1999). In combination, these measures evidenced the diversity of the sample and ensured transparency regarding participants’ self-reported mental health and experience of growth after SCI. The Posttraumatic Growth Inventory Short Form (PTGI-SF, Cann et al., 2010) measures self-reported growth in Tedeschi et al.’s (2018) domains. This measure consists of 10 items rated from 0 (I did not experience this change) to 5 (I experienced this change to a very great degree). It provides a score out of 50, with higher scores representing more growth. The Patient Health Questionnaire-2 (PHQ-2, Kroenke et al., 2003) measures depressed mood and the Generalised Anxiety Disorder 2-Item (GAD-2, Kroenke et al., 2007) measures anxiety; with each measure consisting of two items rated from 0 (not at all) to 3 (nearly every day). Scores greater than 3 out of 6 indicate the possibility of clinical levels.
Interview schedule
An interview schedule (Appendix 1) was developed based on implications and gaps in existing research and literature, in line with methodological guidelines (Charmaz, 2006). This was co-constructed in consultation with an individual living with SCI to assist reflexivity and evaluate accessibility and resonance.
Participants
Participants included four women and seven men of White ethnicity, aged 24–86 (mean 43.82). Nine participants were British, one participant Irish, and one defined themself as Mixed. Ten lived in the UK, and one lived in Ireland. Participants had acquired SCI between 17 and 82 years of age (mean 35.91) and were 1–28 years post-SCI (mean 7.91). Three participants experienced non-traumatic SCI and eight traumatic, including sports injury (4), motor accident (3) or fall (1).
PTG inventory scores ranged from 16 to 40 (mean 28.82), with factor scores lowest for spiritual change and highest for relating to others. PHQ-2 and GAD-2 scores varied between 0 and 6 (PHQ-2 mean 1.18; GAD-2 mean 1.09) with most participants scoring below clinical threshold. The demographic characteristics and range of scores situating the sample reflect heterogeneity in participant lived experience (Table 1).
Participant demographics.
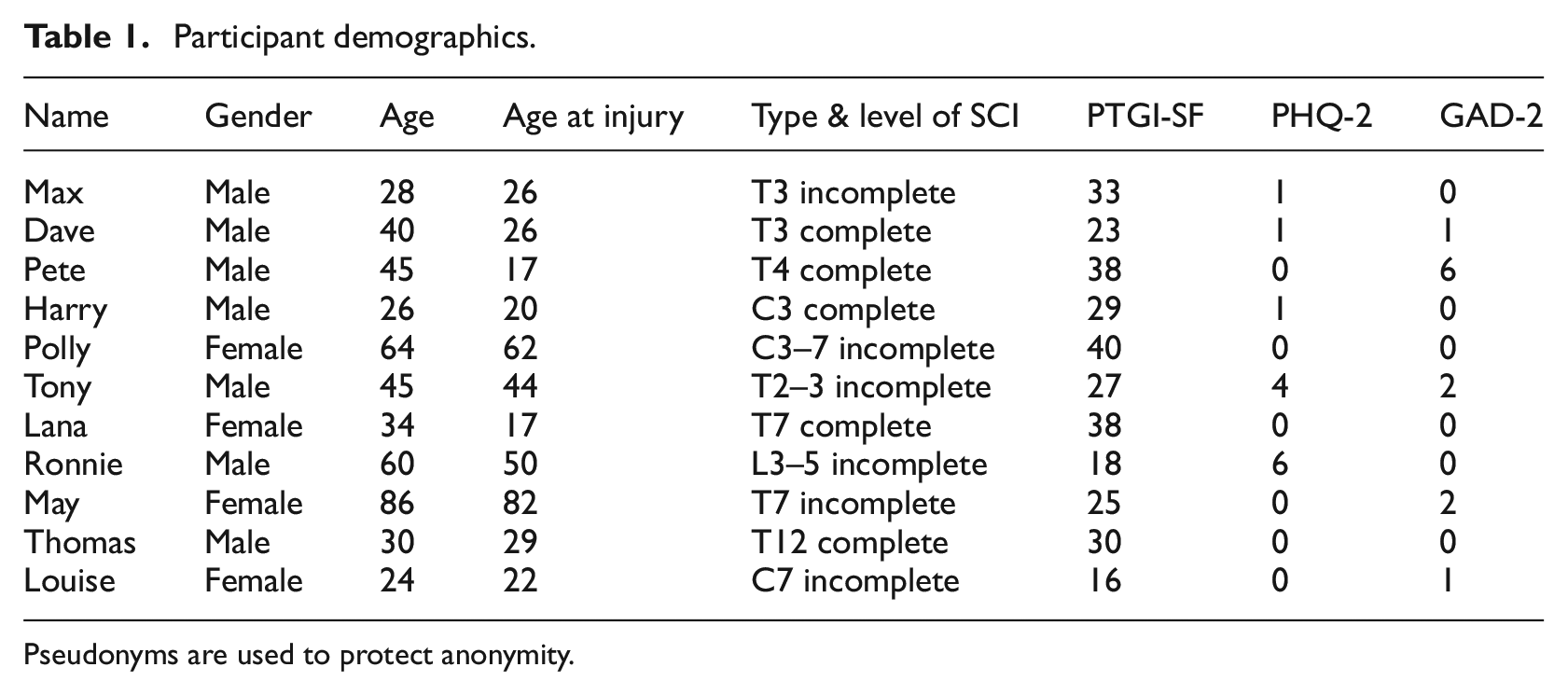
Pseudonyms are used to protect anonymity.
Data analysis
Consistent with CGT procedures (Charmaz, 2006, 2014), the researcher completed open coding, working systematically across the dataset examining the transcript line by line and assigning codes that described segments of the data and remained close to participants own words. Next focused coding was applied, taking the initial codes from a descriptive to conceptual level using the most frequent or significant codes. The researcher then looked across datasets to group together focused codes and create conceptual categories. Memo writing was used to capture thoughts and make comparisons and connections between categories. This supported the identification of themes and subthemes and thus supported the development of conceptual categories into an explanatory framework; consistent with CGT procedures (Charmaz, 2006, 2014).
Data analysis and collection occurred contiguously to allow reflection on emerging ideas from the data and refinement of the interview schedule. Data collection was paused after six interviews to allow the researchers to reflect on how the schedule was enabling the analytic process, and no changes were deemed necessary. However, ideas from the first round of interviews provided further prompts to deepen or find contrasting narratives, to support development of conceptual categories as part of theoretical sampling. Data collection continued until interviews were felt not to provide new insights, indicating data saturation, rather than aiming for a pre-determined sample size (Bowen, 2008).
Tracy’s (2010) key markers were applied to uphold research quality (Appendix 2). The first author conducted the analysis, and the steps were verified by the research team. The researchers discussed emerging ideas and themes throughout the analysis process, enabling the first author to explore and expand on emerging ideas, and understand the relevance to clinical practice observations (Tracy, 2010). The research team facilitated the reflexivity process through reflection about the influence of their values and assumptions on interpretation of the data, enhancing the main researcher’s awareness of how the findings were being co-constructed with participants (Tracy, 2010). The researcher kept a journal, commenting on the influence of their values and assumptions (Charmaz, 2014). A reflexive statement from the researchers is provided (Appendix 3).
Results
Data analysis revealed how SCI initiated PTG processes. SCI was described as a ‘traumatic event’ (Harry) that ‘shakes up everyone’s life’ (Max). This shook beliefs about intended life course, relationships, and worldview, and thus could result in disrupted self-identity. It triggered examination of significant changes to the physical self and re-evaluating life, relationships, sense of self and future possibilities through cognitive (deliberate self-reflection, information seeking and unconscious appraisal processes) and behavioural (exploring limitations and capabilities) processes. Participants described learning from challenges of living with SCI through these processes, enabling them to reconstruct ideas about self, world, others and disability and identify ways they experienced growth. Emotional coping and acceptance of self with disability appeared to support these processes.
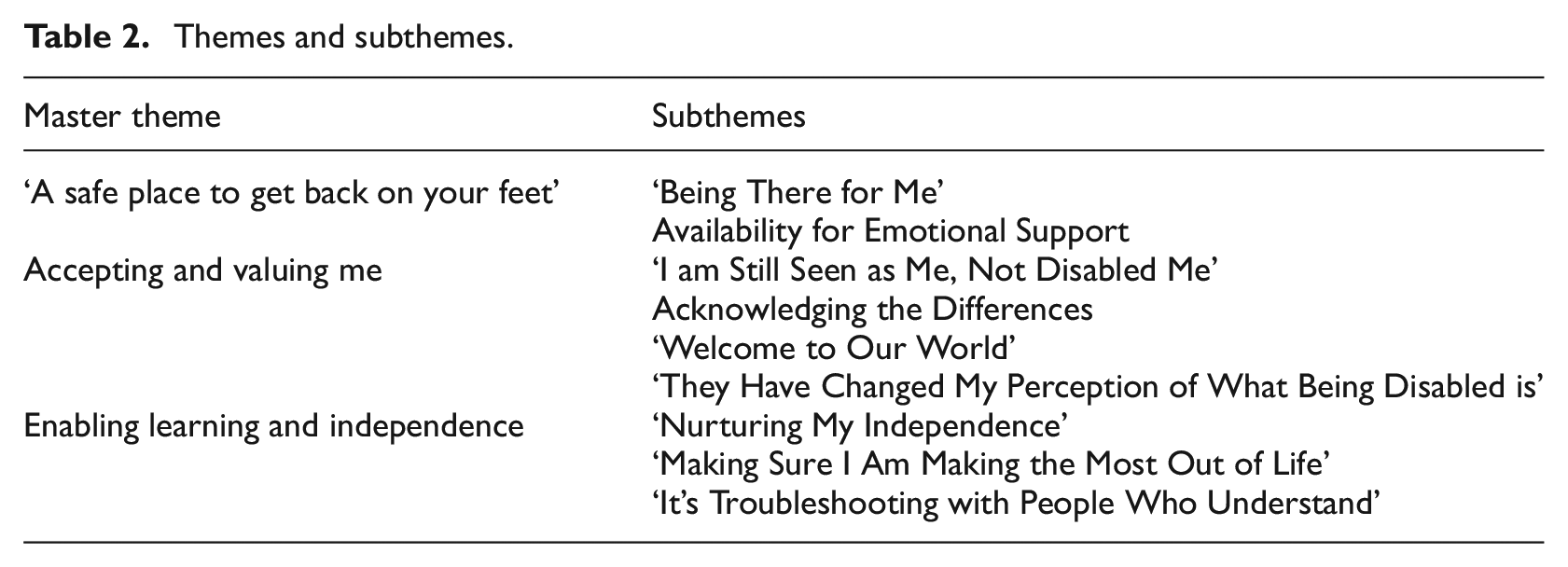
Data analysis revealed three inter-related themes representing how close relationships and peer interactions influence PTG processes: (1) a safe place to get back on your feet; (2) accepting and valuing me and (3) enabling learning and independence. Themes and subthemes are shown in Table 2.
Themes and subthemes.
‘A safe place to get back on your feet’
This theme captures the role close relationships play in providing emotional support and comfort following SCI. Participants discussed initial feelings of loss and being in states of ‘survival’ (Louise). Close relationships could provide feelings of safety and comfort during this period, as well as providing ‘space’ (Dave) to come to terms with the impact of SCI, thereby enabling cognitive processes of PTG. For some, close relationships provided opportunities to discuss experiences of loss and emotional struggle, allowing them to process these experiences in a supportive environment.
‘Being there for me’
This sub-theme reflects the importance of close others providing support and comfort following SCI both in the early stages and as a continued source of support, in facilitating PTG. Participants discussed how traumatic events leading to SCI, or sudden news of life-changing circumstances could lead to more open displays of affection (such as, making life changes to be with the person or rushing to the person’s side), which helped to provide a sense of comfort and soothe emotions: ‘Having brain injury and drug induced delusions and I really couldn’t make sense of the world…the people around me I suppose just helped at that point, helped me be where I was easier, more comfortably’ – Max
It was also helpful to know that although ‘a lot of things are going to change, some things are not’ (Harry), suggesting that others being there for them in the early stages helped to create feelings of safety and protect against further losses: ‘By having no concern that [my wife] would be there and would just deal with whatever because that’s how I would be with her it makes coming home and trying to deal with things easier, you are not worried about the little things’ – Thomas
Having people around them that provided comfort and practical support, enabled participants to feel in a more ‘settled place’ (Dave) and helped to soothe emotions and facilitate cognitive processing as part of PTG processes.
Some recalled how others’ demonstration of love and choices to ‘stick by you’ (Dave) could lead to increased ‘closeness’ (Polly), ‘sense of oneship’ (Ronnie) and understanding of what we ‘meant to each other’ (Thomas), enabling PTG within relationships: ‘It’s an acid test is a spinal cord injury…there’s a yes or no question that is implicitly asked, do you want to be with me yes or no? And everyone, your friends, your partner, everyone makes that choice…it means that I know that everyone in my life really wants to be’ – Max
Availability for emotional support
Participants described the importance of close relationships being available to provide emotional support and support coping. Participants talked about the importance of knowing they could express emotions or talk about experiences in facilitating opportunities to process loss and make sense of changes: ‘Happy to talk about my emotions and stuff, if I feel like crying I will just cry, I don’t care, and I have been quite open about that, especially amongst my closest friends, how I deal with stuff or when I have had a rubbish day’ – Thomas
Being able to express difficult experiences and emotions was important for participants in being able to manage emotions. However, being prompted to use coping strategies which helped to avoid or reduce emotional intensity was also felt to be important when emotions felt overwhelming: ‘Points where I was like I really can’t be bothered to go on living…having people be like “no, shut up, here let’s go out, let’s go and do this”, or “didn’t you love painting in hospital lets go and buy some art stuff, let’s go start painting”, you know having those people around at the right time is everything’ – Harry
Pete’s experiences provide insight into the impact of a familial environment where close others were felt not to be able to flexibly provide opportunities for both types of coping: ‘He would find me asleep in the kitchen just absolutely slaughtered and just tell me to go to bed and now I wish he had spoken to me about it, why was I going out and getting hammered’ – Pete
His family’s avoidance of emotional experiences seemed to endorse the sole use of avoidance coping strategies, blocking his ability to manage emotions and make sense of the impact of his injury. Pete told of how he struggled with SCI for many years. His engagement with peers, rather than family, was the turning point in the development of PTG.
Accepting and valuing me
This theme relates to how relationships and interactions can help shape beliefs about the impact of SCI on self-identity in ways that enabled the individual to learn and experience PTG. This was discussed in the context of societal beliefs of disability as representing vulnerability and incapability, which could threaten continuity of self and feelings of acceptance within their social world. Participants described the importance of close relationships in seeing ‘a continuation of the same person’ (Harry), which appeared important in maintaining a continued sense of self and self-acceptance following SCI. It was also important for close others to accept and acknowledge a changed physical body so the individual could be open to the impact of SCI on self and relationships. Peers were also seen as important catalysts in enabling acceptance, and in providing opportunities to reconstruct beliefs about disability and rebuild identity. Relationships and interactions appeared to be important in facilitating acceptance of self with a disability, providing a foundation for growth and living well.
‘I am still seen as me, not disabled me’
This sub-theme reflects how beliefs about self were ‘shaken’ (Max) due to the unexpected acquisition of SCI and social label as a disabled person. For many this brought to the surface unconscious beliefs about disability as representing vulnerability or incapability, which could present as a perceived threat to identity and acceptance by others. Participants were therefore required to make sense of how these beliefs might impact on self and social identity. Close relationships were an important source of information in this process: ‘They just treated me like I was me, because I was, I am still me, just because I’ve broken my spinal cord doesn’t mean that I’m a different person…the first time that I realised I was going to be ok was when one of my best mates came into hospital to see me and was like of course it’s you that’s broken your neck Harry, honestly you always like attention’ – Harry
Continuity of relational dynamics, humour in Harry’s case, could be helpful in shaping beliefs about the impact of SCI on the self, such as by learning that ‘my body is not me’ (Lana). It could also shape ideas about how participants might be perceived by others. Harry’s friends appeared to signal to him that others felt comfortable around him and saw him as someone who was emotionally resilient and able to handle the changes, rather than someone who needed to be protected. Thomas also shared how his friends describing him positively to others revealed to him how others saw him ‘as a strong individual rather than just a disabled man’.
In contrast, close others interacting with participants differently had the potential to highlight a changed self or ‘disabled me’, which could undermine PTG: ‘Just trying to do daily things they were really worried, and I get why because I’m sort of almost could be seen as maybe like a bit of a broken human…I was like no, I’m going to tell you to F off in a minute, just kind of that really, making sure I am still seen as me, not disabled me’ – Thomas
Other participants described this in terms of ‘people having very low expectations of you’ (Lana), ‘infantilising you’ (Louise) or ‘fussing over me’ (May). These interactions appeared to highlight a disabled self which could precipitate a negative self-image and undermine PTG. However, in Thomas’s case being able to navigate this within a safe relationship through open discussion helped protect his self-image.
Acknowledging the differences
It was important that close others acknowledged a changed physical self and were ‘willing to adapt, do something different’ (Max) to support social inclusion, and acceptance of a changed physical self: ‘Moving forward I have to have people who can accept that you know I’ve got problems and I can’t just pop out with them’ – Polly ‘I used to have to circle back constantly [to the accessible bathroom] to be able to keep up with my friends and it was interesting because at that time I would have let bouncers or my friends or whoever lift me up stairs to get somewhere that everyone was going…you are so grappling with not wanting to be different that you will conform to just do whatever’ – Lana
Disability going unacknowledged seemed to lead to the individual struggling to accept and learn to work with physical changes, meaning some participants felt they had to try to ‘live life like an able-bodied person’ (Pete) to retain relationships. This seemed to have negative implications for making sense of the impact of SCI on self-identity, hindering PTG: ‘I didn’t identify as having a disability because all my friends were mobile, were able-bodied and they saw me as I was before. It was fairly easy to pretend that my identity hadn’t changed that much. It was when I moved at the point, it was the first time that people saw my wheelchair before they saw me’ – Lana
‘Welcome to our world’
This sub-theme describes the value of connecting with peers, who have lived experience of SCI and ‘know what it’s like’ (Polly), in reducing feelings of isolation and cultivating a sense of belonging and acceptance in a social world often felt to be disabling: ‘It was really refreshing at that time, to meet someone else who was like what the hell is wrong with this world’ – Lana
For some this community of peers enabled them to find acceptance of disability, and acknowledgement of the difficulties they faced with access and disablement. Pete had strongly held beliefs about disability and societal acceptance from the working community he grew up in, which initially caused him to reject engaging with a community of peers. However, when he began to integrate into this community, he was able to start to challenge ideas about his own acceptability. This was the catalyst of his experience of PTG: ‘I met a load more people with disabilities, if one of us had a bowel accident we all laughed about it, the banter just made it more acceptable for having a disability’ – Pete
‘They have changed my perception of what being disabled is’
This sub-theme represents how meeting others with disability prompted participants to re-assess beliefs about current circumstances, disability, and potential future. Some participants described how stereotypes represented in the media could influence ideas about future opportunities and societal acceptance. Both Lana and Thomas observed reporting of the Paralympic movement had created a ‘superhuman’ (Lana) identity for disabled individuals. This was contrasted with ideas about ‘angry wheelchair users’ (Lana) or ‘those who moan…and complain’ (Thomas). These stereotypes were seen as reductive and could act to narrow aspirational possibilities: ‘It can create a bit of an unrealistic level, most people don’t aspire to climb mountains all the time, or be TV presenters and stuff, you know actually like if you’ve had a spinal cord injury you just want to live a normal life…it’s by speaking to everyday people living with a spinal cord injury where I have learnt the most’ – Thomas
Participants described how meeting others with physical impairment living everyday lives was helpful in challenging negative beliefs about possibilities and starting to understand how life could be: ‘I was amazed that she could have what appeared to be almost a normal life with this spinal injury…it was completely affirming that life can go on’ – May
Enabling learning and independence
This theme refers to the ways in which close others helped them to learn to live well following SCI through enabling independence, exploring boundaries, and connecting with valued hobbies. This was important in enabling the behavioural processes of PTG and revising beliefs. Peers were also important in empowering participants to manage SCI more independently, scaffolding them to make gains.
‘Nurturing my independence’
Participants described how close others helped to support independence, particularly in the early stages. This was thought to be helpful in exploring and understanding physical and psychological capabilities, and in starting to rebuild their life and self-identity: ‘Washing, ironing, cooking, cleaning as best as I can and stuff like that, so yeah its taught me that I have got, I’ve learnt about myself how more determined I can be’ – Tony ‘[my husband] was reluctant to share any chores with me because he knew he could do it better and he just wanted me to be looked after…I knew I could do these things but there’s a difference between having to do them and knowing you can’ – May
May felt her ability to exert autonomy and contribute to the household was hindered by her husband’s wish to care for her. She described surprise at what she could do when she was able to explore this, enabling her to reconstruct beliefs about self and disability as part of her experience of PTG.
‘Making sure I am making the most out of life’
This subtheme refers to the role of close others in encouraging and enabling participants to connect with valued activities through physical support, encouragement and creative adaptations. This appeared important in understanding physical capabilities and limitations, as well as rebuilding beliefs about self-identity.
‘Friends who helped me go on stupid adventures and things like that, who have in their own way got over their own squeamishness and help me with things that we would not normally ask’ – Louise ‘A really good friend of mine who is a very talented music tech spent about a year and a half trying to invent an instrument that I could play, that was pretty special, didn’t quite get it to work in the end but you know it was sort of the thought of that and the effort’ – Harry
Encouragement and enablement to find new ways to connect with valued activities could reinforce a continued sense of self whilst allowing exploration and acceptance of limitations. Lana shared how her parents enabling her to continue pursuing horse riding, despite knowing it was unlikely to be possible, was important in facilitating acceptance and growth: ‘It was all part of the process of trying to do it and then accepting that it wasn’t going to happen in the same way, if I had rushed that process I think it would have just shattered that old sense of who I was…interrupted that growth’ – Lana
‘It’s troubleshooting with people who understand’
This sub-theme reflects how interactions with peers can support with learning how to live well with SCI by eliciting advice and information about overcoming problems. Participants described shortfalls in NHS services, such as finding information inaccessible, inconsistent, or too ‘clinical’ (Thomas). Information from peers was seen as more valued due to a shared skill set, purpose and vocabulary: ‘All the personal information that they give you, it’s a wealth of information…you get help if someone has been through it before’ – Tony
Learning from peers was seen as important in PTG development as it ‘arms you with the knowledge’ (Thomas) to navigate NHS systems and ‘helps people do what they need to do’ (Max), empowering participants to manage SCI. Participants also described learning about how they could connect with valued activities from peers: ‘He was travelling all around South America…so it was cool to talk to him and see how he did that to see how I would do that kind of thing in the future’ – Louise
Participants described wanting to use learning to help peers, which appeared important for PTG as it enabled participants to turn something difficult, and the learning from this, into ‘something positive’ (Thomas).
Tentative theoretical model
Consistent with CGT methodology, a tentative, theoretical model is offered. The model, shown in Figure 1, represents the psychological re-evaluation (cognitive and behavioural) processes of PTG found in the study, and how these might be triggered by the ‘shaking’ of the individual’s world, core beliefs and identity following SCI. The model further demonstrates how relationships might interact with and support these processes through providing safety, acceptance, and enablement. Further testing, empirically and cross culturally, is needed to understand the relevance of the model to a wider SCI population, and chronic health conditions.
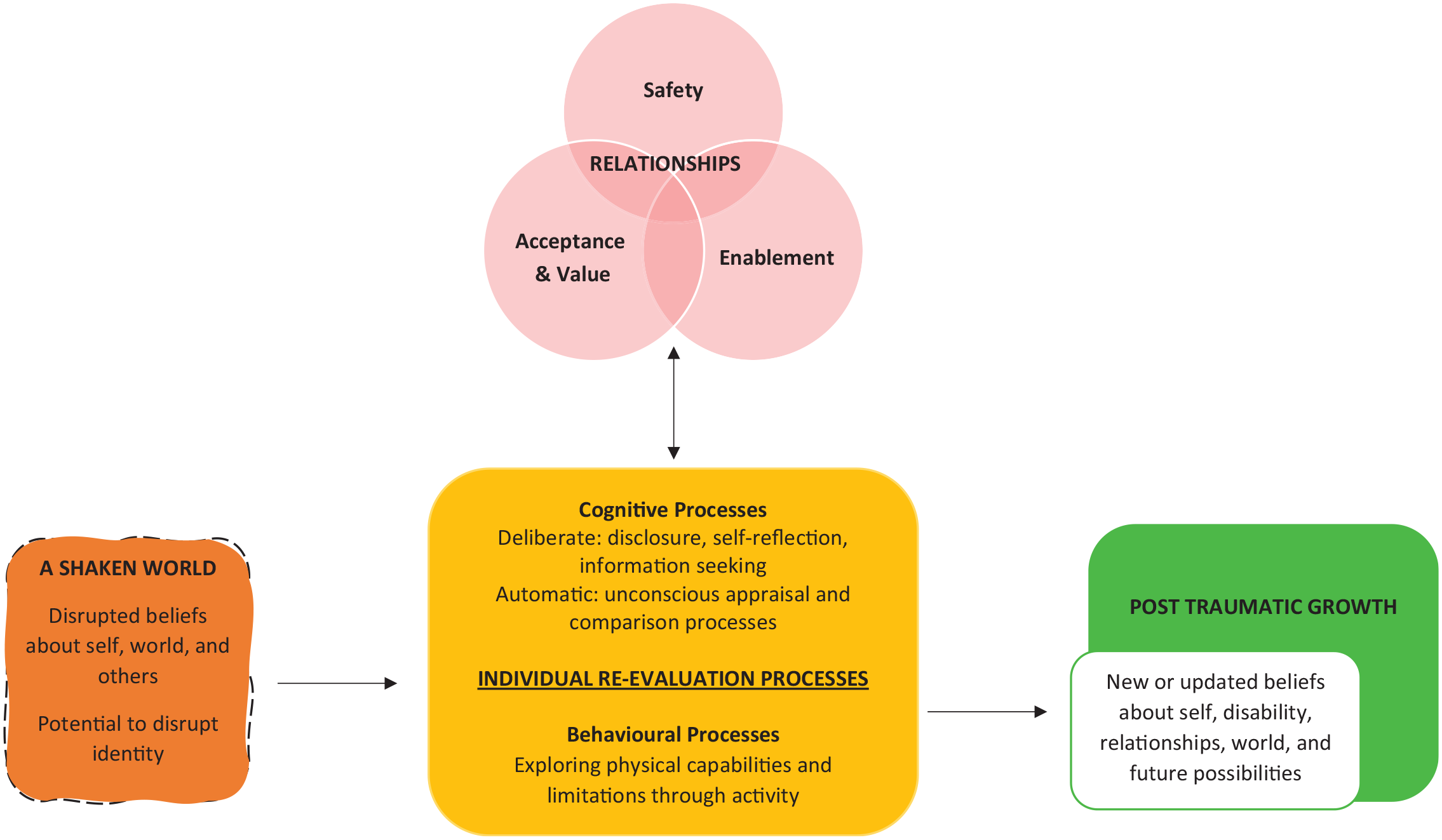
Tentative theoretical model.
Discussion
The study explored the lived experience of SCI, with specific focus on relationships and perceived support in PTG development. The findings provided insights into PTG processes and how these might be supported by relationships through safety, acceptance, and enablement of independence.
The study showed PTG processes to be triggered by the “shaking" of the individual’s life and world as they faced life-changing injuries and confronted beliefs about disability; in line with Bury’s (1982) concept of ‘biographic disruption’. This appeared to result in ‘shaken’ beliefs about self, relationships, and imagined future, leading to cognitive and behavioural re-evaluation processes as the individual rebuilt beliefs. In rebuilding beliefs participants could experience PTG in many areas; consistent with Tedeschi et al.’s (2018) model.
Consistent with Chun and Lee (2008, 2010) and Wang et al. (2017) the findings showed close relationships and interactions with peers could play a multi-faceted role in supporting PTG development. Relationships could function to enable PTG processes through the provision of support, as well as influence the rebuilding of beliefs in the implicit meaning taken from interactions; supporting Tedeschi et al.’s (2018) model.
The first relational theme showed how close relationships can promote coping and provide a source of comfort and safety in times of uncertainty and distress. This was shown to enable cognitive processing through the management and soothing of emotional distress. Tedeschi et al. (2018) recognise how social support can provide sources of comfort following trauma, however expansion of how comfort supports PTG is not articulated. Close others were also shown to directly facilitate cognitive processing through opportunities for emotional disclosure in a safe environment; consistent with Tedeschi et al.’s (2018) model.
Tedeschi et al. (2018) see deliberate rumination as a core facilitator of PTG. However, the findings show this may play a lesser role following SCI than the model predicts. Updating beliefs about self, world and others appeared to occur in less deliberate ways as participants interacted with their social world and engaged with behavioural processes of exploring physical capabilities. Relationships were seen as important in facilitating behavioural processes through encouraging independence and exploration of physical boundaries, and in understanding capabilities and limitations post-SCI. Consistent with previous research (Crawford et al., 2014), this was seen as important in connecting with the previous self and in developing new beliefs about self, disability, and future possibilities. Peers could also provide information from a lived experience perspective enabling individuals to better manage disability and rebuild beliefs about the future; similar to Chun and Lee (2008, 2010).
The findings showed SCI could trigger unconscious beliefs about disability, requiring the individual to make sense of the impact of a ‘disabled me’ on beliefs about self, world and others. This was shown to occur as the individual interacted with their social world and took implicit meaning from interactions. Close relationships played a significant role in how participants made sense of acquired disability on the concept of self. Continuity of relational dynamics and ‘being seen as the same’ as pre-injury was important in continuity of self. Previous research shows loss of sense of former identity can contribute to negative psychological outcomes (Dickson et al., 2008), whereas PTG has been associated with retaining or ‘finding the previous self’ (Griffiths et al., 2012; Wang et al., 2017). Therefore, arguably being able to retain elements of previous self is important in protecting against negative outcomes and establishing a basis for understanding change and potentiating growth. Relational dynamics were also important for reinforcing ideas about personal strength versus vulnerability, which appeared to enable participants to challenge beliefs about how they would be perceived with visible impairment and develop PTG in terms of beliefs about inner strength.
Finally, acceptance of self with disability was found to be important in readying the person to explore and make sense of changes, thus enabling reconstruction of beliefs as part of PTG. Byra (2016) argues acceptance creates the foundation for PTG as it provides readiness to reduce one’s emphasis on physicality as a feature of one’s own value, opening people up to appreciate other qualities. Relationships were shown to be important in supporting acceptance processes when close others acknowledged a changed physical self, were open to talk about this and willing to accommodate the individual’s needs. Whereas peers could support this process by demonstrating future possibilities, thus facilitating new beliefs about disability. Peers could also create feelings of acceptance in a world that often felt disabling, enabling reappraisal of the problem as an external societal issue rather than internalising self as unacceptable. These findings extend previous research.
Several limitations are recognised, indicating areas of future research. Firstly, the research provided rich insights into the lived experience of SCI. However, all participants were of White ethnicity and predominantly British, thus the results might be culturally specific. Further research exploring relational dynamics and PTG in other cultures is indicated.
Additionally, the study explored PTG from the perspective of the individual living with SCI. However, the impact of SCI has been described as rippling beyond the individual to the family (Dorsett, 2001). Further qualitative research from the perspective of couple dyads or families would aid understanding of PTG processes, relationships challenges and co-constructed meaning making processes within family systems.
The lived experiences of SCI discussed in this paper may resonate with the experiences of individuals living with other chronic conditions. However, further research is needed to understand whether the findings and recommendations extend to wider settings.
The findings have implications for SCI practice. The study shows it could be beneficial for rehabilitation professionals to support people with SCI to explore unconscious beliefs about disability and how these influence beliefs about self to facilitate positive adaptation. Psychological interventions could draw on Cognitive Behavioural Therapy and/or Acceptance and Commitment Therapy techniques to explore and change cognitive and behavioural patterns, as part of rebuilding a positive self-image and meaningful life.
Inpatient rehabilitation settings should be proactive in facilitating opportunities for close others to ‘be there’ for the individual, mobilising existing relationship orientated strengths, and acknowledging relationships challenges. Family Therapy or psychoeducation could be beneficial in creating an environment where the individual is enabled to feel safe, accepted, and express independence. Individual psychological work supporting the individual to navigate relational difficulties, such as Interpersonal Therapy, might be considered.
Moreover, opportunities to learn how to adapt positively from peers (including support groups, mentoring and sports/leisure groups) should continue to be offered, and strengthened, in inpatient and community settings in collaboration with the third sector. Services should look to highlight stories of everyday achievements as part of celebrating diversity in ways of living with SCI. The findings have implications for public health in illustrating wider representations of disability to counter implicit bias.
Conclusion
The study gives insights into how individuals can use cognitive and behavioural strategies to experience positive psychological changes following SCI, and how relationships can support these processes by providing safety, acceptance and enablement. People with visible impairment can encounter negative attitudes and confront their own beliefs about disability. Social inclusion and acceptance from others are important in reconstructing beliefs and developing a positive self-image. Better understanding of relational processes is important clinically for facilitating positive adjustment.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251315891 – Supplemental material for Safety, acceptance and enablement in a shaken world: The role of relationships in post traumatic growth development following spinal cord injury
Supplemental material, sj-docx-1-hpq-10.1177_13591053251315891 for Safety, acceptance and enablement in a shaken world: The role of relationships in post traumatic growth development following spinal cord injury by Gemma Smith, Andrew R Thompson, Anna McCulloch and Jennifer Moses in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053251315891 – Supplemental material for Safety, acceptance and enablement in a shaken world: The role of relationships in post traumatic growth development following spinal cord injury
Supplemental material, sj-docx-2-hpq-10.1177_13591053251315891 for Safety, acceptance and enablement in a shaken world: The role of relationships in post traumatic growth development following spinal cord injury by Gemma Smith, Andrew R Thompson, Anna McCulloch and Jennifer Moses in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053251315891 – Supplemental material for Safety, acceptance and enablement in a shaken world: The role of relationships in post traumatic growth development following spinal cord injury
Supplemental material, sj-docx-3-hpq-10.1177_13591053251315891 for Safety, acceptance and enablement in a shaken world: The role of relationships in post traumatic growth development following spinal cord injury by Gemma Smith, Andrew R Thompson, Anna McCulloch and Jennifer Moses in Journal of Health Psychology
Footnotes
Acknowledgements
With thanks to the individuals living with SCI who generously offered their time and experiences to contribute towards the research. Acknowledgement also goes to the spinal cord injury charity and lived experience group who supported recruitment through advertising the study online.
Author contributions
Gemma Smith: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, visualisation, writing – original draft preparation. Andrew Thompson: conceptualisation, methodology, supervision, validation, writing – review and editing. Anna McCulloch: Supervision, validation, writing – review and editing. Jennifer Moses: conceptualisation, methodology, supervision, validation, writing – review and editing.
Data availability statement
Data supporting the findings of this study cannot be made available as the confidentiality and informed consent of participants would be compromised.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was completed as partial fulfilment of the requirements of the Doctorate of Clinical Psychology for the lead author and as such was partially funded by Health Education and Improvement Wales.
Ethics approval
This study was approved by the Ethics Committee of Cardiff University (Ethics Code: EC.21.01.12.6220R) on February 7th 2021 and was conducted ethically in accordance with the British Psychological Society Code of Ethics and Conduct.
Informed consent
Informed consent was obtained verbally before participation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.