
Abstract
Exercise is recommended for people with Parkinson’s (PwP) but clinical exercise-based interventions are generally ineffective. Social, cultural and environmental factors can influence exercise behaviours, but these topics are under-researched. We interviewed 18 PwP using a narrative approach to identify factors influencing their exercise behaviours throughout their lives. Thematic analysis identified three themes: (1) Why I exercise, (2) What helps and (3) Exercise with Parkinson’s. Participants had consistent core motivations to exercise: mood and well-being, body image, competition, and camaraderie. Having active partners, supportive work, and varied exercise options were among the important facilitators of long-term exercise. Participants believed strongly in the benefits of exercise for Parkinson’s, but experienced guilt about not exercising enough and frustration when symptoms made it harder to continue. This study illustrates how narrative interviews can reveal important social, cultural and environmental influences on exercise behaviour, offering potential to develop more individualised and effective exercise interventions.
Introduction
There are over 145,000 people with Parkinson’s (PwP) in the UK, and this will increase by 20% in the next 10 years (Parkinson’s UK, 2022a). Parkinson’s is a neuro-degenerative disease which causes a reduction of dopamine in the brain. This neurotransmitter helps regulate movement, and many symptoms are movement related (Damier et al., 1999). Symptoms usually manifest in people over 50 and progress at a variable rate (Bloem et al., 2021). Many PwP live with a reduced quality of life for years (Schrag et al., 2000). Pharmacological treatments relieve some of the symptoms but do not affect the underlying neuro-degenerative process (Bloem et al., 2021).
Exercise and Parkinson’s
Exercise is an important non-pharmacological treatment (Bogosian et al., 2020), and is recommended for all PwP (Keus et al., 2014; National Institute for Health and Clinical Excellence (NICE), 2017). Systematic reviews have shown that exercise can reduce falls and improve motor symptoms and quality of life (Allen et al., 2022; Ernst et al., 2024). However, there is considerable variation in effect size, and research is ongoing into different exercise types and doses.
The evidence from pragmatic exercise-based studies is less positive, with three large therapist-led UK trials yielding small or non-significant effects (Ashburn et al., 2019; Clarke et al., 2016; Goodwin et al., 2011). PwP face many barriers to exercise, but studies examining these tend to focus on cognitive-behavioural influences such a self-efficacy and knowledge (Ellis et al., 2013; Schootemeijer et al., 2020). A systematic review of qualitative studies on barriers and motivations found that PwP value exercise which is highly individualised (Hunter et al., 2019). One possible reason, therefore, that exercise interventions are ineffective is that they do not align with PwP’s individual backgrounds, goals and attitudes (Amateis et al., 2019). This may affect the person’s engagement and thereby the efficacy of interventions.
Social, cultural and environmental influences on exercise
By contrast with cognitive-behavioural models, ecological approaches emphasise how behaviours are influenced by a system of social, cultural and environmental factors (Burke et al., 2009; Sallis et al., 2008). Qualitative studies in different populations have shown how childhood experiences, education, ethnicity, religion, gender roles, migration, environmental factors and cultural beliefs can interact and influence attitudes to exercise (Caperchione et al., 2009; Jang et al., 2016; Mahmood et al., 2022; Mayes et al., 2022; O’Driscoll et al., 2014) . Recognising these wider influences, some researchers are now using the COM-B model to understand and map determinants of exercise behaviour among people with neurological conditions (Huynh et al., 2023; Nicholson et al., 2014; Pekmezi and Motl, 2022; Riemann-Lorenz et al., 2021; Silveira et al., 2021). COM-B assesses the capabilities, opportunities and motivations associated with a behaviour, integrating external opportunities (i.e. social, cultural and environmental factors) with intrinsic capabilities and motivations, to establish the most appropriate type of behavioural intervention (Michie et al., 2011).
Very few studies have examined the social, cultural and environmental influences on exercise among PwP. One systematic review of experiences of exercise among PwP (Hunter et al., 2019) found only two studies conducted in Jordan (Khalil et al., 2016, 2017). They noted that stigma can hinder a PwP’s disclosure of their diagnosis, limiting exercise options in the early stages, while some PwP may view exercise culturally inappropriate after young adulthood. These studies did not fully explore the variety of influences on attitudes to exercise, nor how they interact and build over time in individuals.
Research aim
Our premise is that deeper understanding of individuals’ relationships with exercise could improve clinical interventions. This study aimed to describe how social, cultural and environmental factors influence the meaning of, and attitudes to, exercise among PwP. We used thematic analysis to examine how exercise behaviours develop over time, before and after a diagnosis of Parkinson’s.
Materials and methods
This was a qualitative study featuring semi-structured interviews with PwP in the UK. This study is reported using the COREQ criteria (Tong et al., 2007) (see Supplemental Materials), and was approved by the City, University of London School of Health and Psychological Sciences Ethics Committee (Ref: ETH2223-1452).
Epistemology
The ontological basis for this study was naïve or direct realism, where the emphasis is on enabling the participants to recall, describe and reflect on experiences in their terms (Willig, 2023). The analytic approach was broadly inductive (Braun and Clarke, 2021). However, interviewees were guided (see below) to focus on the external influences on their behaviour, reflecting the ecological approach to the study.
Reflexivity
Reflexivity recognises that the standpoint and values of the researcher will affect all aspects of the study (Berger, 2015). The lead author is a neurological physiotherapist with experience of working with PwP. Interviewees were aware of his profession, which may have shaped their comments about NHS services and exercise. The author completed field notes and reflections after each interview. Where his experiences of exercise aligned with those of interviewees, there is a risk that their comments may have had undue influence in the analysis.
Participants
Participants were recruited by the lead author from Parkinson’s UK’s support groups and their network of PwP interested in research. Flyers were distributed at a Dance for Parkinson’s group, and the study was promoted via X (formerly Twitter) and a video on YouTube, which was shared with African and Jewish Parkinson’s organisations. To increase the diversity of the data, recruitment materials highlighted the desire to recruit Black, Asian and Minority Ethnic (BAME) PwP.
Participants aged ≥18 years were eligible if they had a self-reported diagnosis of idiopathic Parkinson’s disease, were a UK resident and were able to participate in an interview. Interpreters and translations of study material were available. Participants were excluded if they were unable to consent due to apparent cognitive impairment during initial interaction with the lead author.
A target of 15 participants was established based on resources and the ‘information power’ of the sample (Malterud et al., 2016). This methodology proposes six dimensions which influence how many participants are needed in qualitative research. Most dimensions suggested a higher number for this study, including a broad topic area, absence of theoretical grounding and predominantly convenience sampling.
Forty-two PwP expressed an interest, of whom one was ineligible due to cognitive impairment. No interviewees declined to participate after reading the information sheet. In response, purposive sampling was introduced to maximise the diversity of the data set. Interested PwP completed a survey, giving their age, gender, ethnicity, education level, employment type, time since diagnosis, use of mobility aid and frequency of exercise. The lead author selected participants to maximise variation in each category.
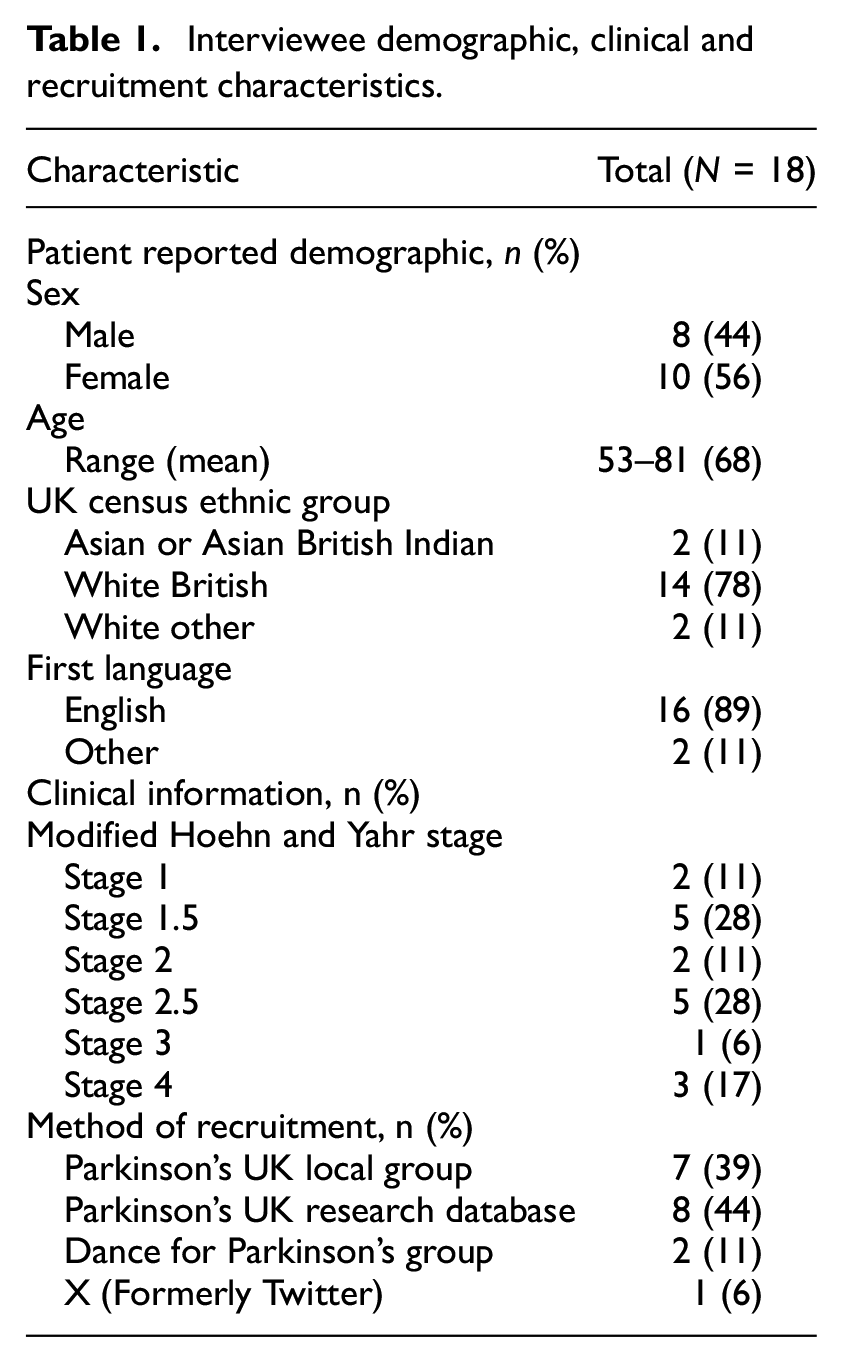
Written informed consent was obtained. Table 1 shows the interviewee characteristics and method of recruitment. Eighteen PwP (44% male, 56% female) were recruited. The mean age was 68 years, and the majority were white British (78%), with two British Indian, one Portuguese and one Jewish American. Most participants (83%) were Hoehn and Yahr stage ≤3, meaning they could walk without a walking aid. Most participants (83%) were recruited through Parkinson’s UK.
Interviewee demographic, clinical and recruitment characteristics.
Data collection
Interviews were conducted between 16 June and 1 August 2023 by the lead author. The semi-structured format allowed participants to describe experiences in detail while focussing on set of topics (Holloway and Wheeler, 2010). Interviews lasted between 23 and 53 minutes. Seven interviews were conducted in participants’ homes, 10 by video, and 1 by phone. No interpreters or repeat interviews were required. The partner of one participant (A) was present during their interview.
Narrative approaches are appropriate to illuminate how individuals’ health behaviours build over time, influenced by social relationships and environments (Greenhalgh et al., 2015; Haydon and van der Riet, 2017). This involves collecting and interpretating data from people’s accounts of their lives (Anderson and Kirkpatrick, 2016). Interviews were structured to identify childhood, adult and later life exercise experiences, using a guide adapted from a methodologically similar study (Mayes et al., 2022) (see Supplemental Material). The interview guide was reviewed after two pilot interviews and after the first six interviews. Initial questions encouraged storytelling about exercise experiences and attitudes. Follow-up prompts were open, ‘You mentioned X, can you please tell me more about this?’. Specific prompts were used, if needed, to ask participants to focus on social, cultural or environmental influences.
Participants were given diagrammatic handouts to explain ‘culture’ and ‘exercise’ (see Supplemental Materials). The term ‘exercise’ was considered simpler for interviewees, though the examples given conform to the broader definition of ‘physical activity’ (World Health Organization (WHO), 2022).
Data processing
Interviews were recorded through Microsoft Teams or Zoom or by encrypted digital audio recorder. Participants were assigned lettered study IDs and pseudonymised recordings were professionally transcribed. Verbatim transcripts were analysed using NVivo 14. It was not possible to seek interviewees’ comments on transcripts.
Data analysis
The data was analysed using thematic analysis (Braun and Clarke, 2021). This methodology is appropriate for a novice researcher and is compatible with realist approaches (Campbell et al., 2021). It involves discovering patterns of meaning across the interview transcripts and field notes through a multi-staged approach (See Supplemental Materials for description of process and coding tree example).
Patient and physiotherapist advisory groups
Two PwP with research experience were recruited through Parkinson’s UK. They reviewed the information sheet, undertook pilot interviews, commented on interview guides, and reviewed the initial themes. Three physiotherapists were recruited through the Association of Chartered Physiotherapists in Neurology (ACPIN) by invitation to members with an interest in Parkinson’s. They commented on the initial themes, relating them to their patient cohorts. Both groups were remunerated according to NIHR guidance (National Institute for Health and Care Research (NIHR), 2023).
Results
Qualitative themes
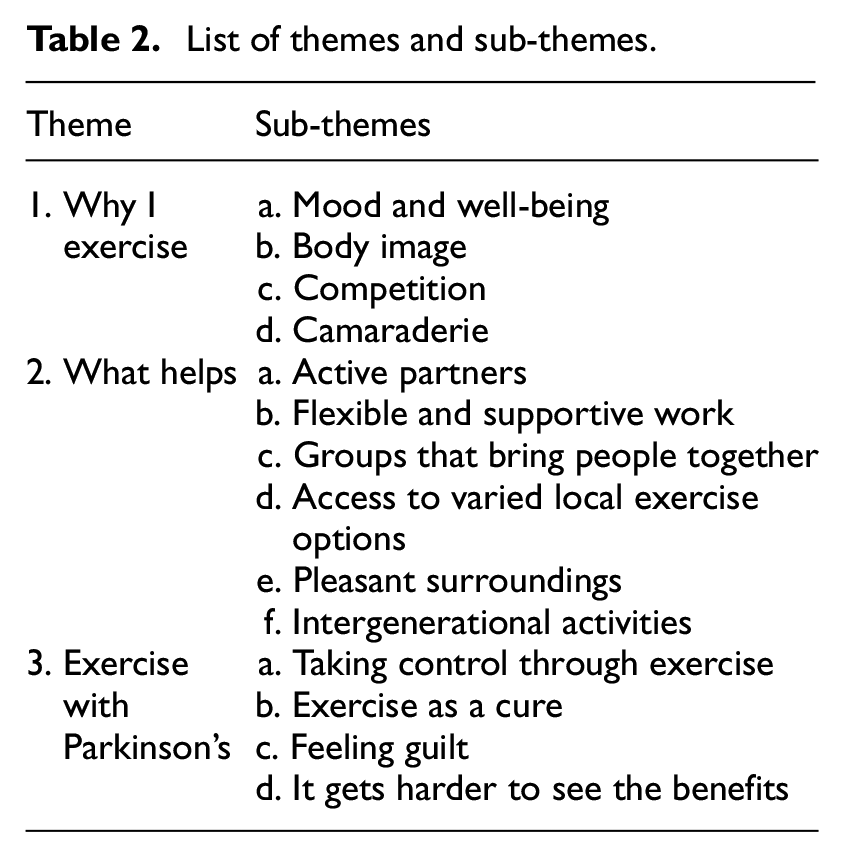
Three themes and 14 sub-themes were identified, shown in Table 2. Theme 1, ‘Why I exercise’, describes the differing motivations participants have to exercise. Theme 2, ‘What helps’, identifies the social, cultural and environmental factors which enabled the participants to exercise throughout their lifetime. Theme 3, ‘Exercise with Parkinson’s’, describes how exercise has a significant role in participants’ responses to Parkinson’s, but brings with it practical, psychological and emotional challenges.
List of themes and sub-themes.
The three themes can be represented temporally in relation to PwP’s lifetimes as shown in Figure 1. In doing so, it is also possible to map the themes against the three dimensions of the COM-B model.
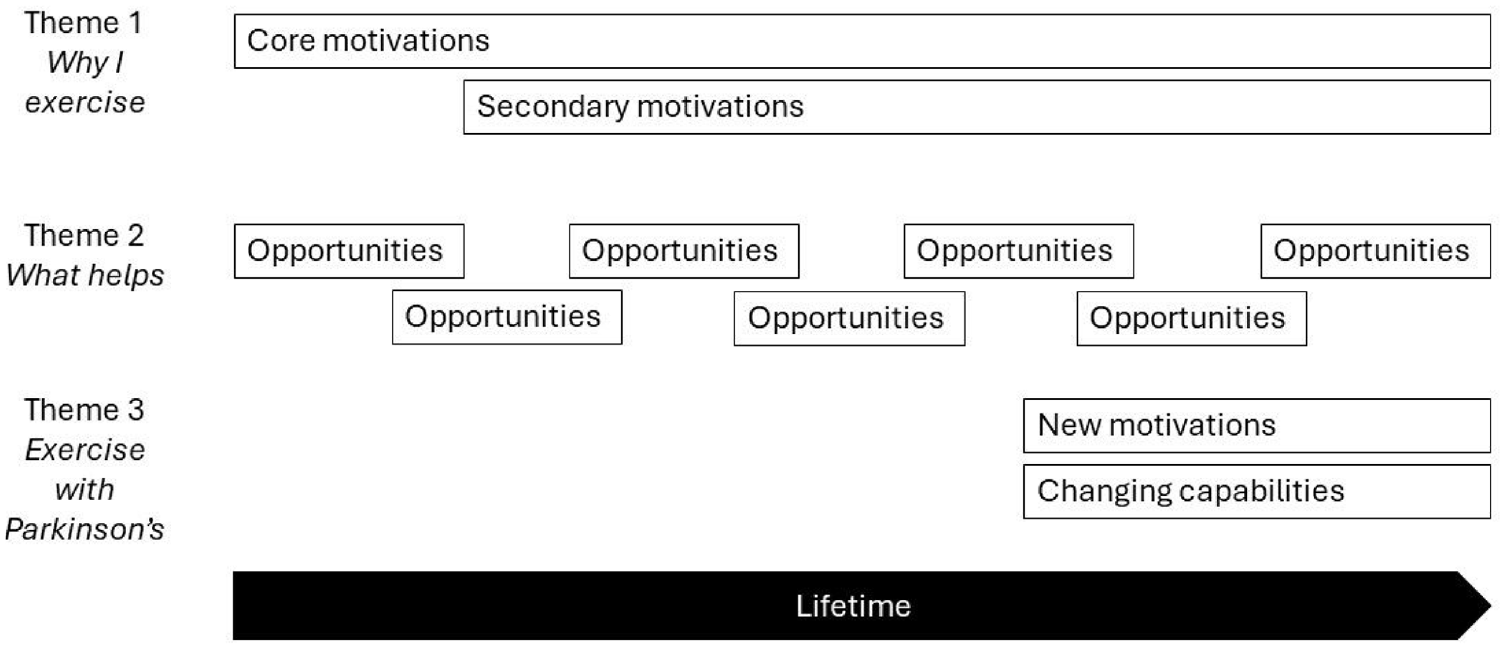
Qualitative themes mapped against COM-B dimensions.
Theme 1: Why I exercise
Interviewees had rich experiences of exercise. They were all active as children, but often in adolescence developed an identity as ‘sporty’ or not, based on aptitude, opportunities or interests. While this identity persisted into adulthood, being ‘non-sporty’ did not preclude later life enjoyment of exercise. By early-to-mid adulthood most interviewees had developed a core reason to exercise, which consistently motivated them from then on. Four types were identified, which were individualistic or more collective in nature.
Mood and well-being
Immediate feelings of wellness were the key motivator for some, while others found that regular exercise stabilised their mood in the long term, counteracting the effects of stressful work or relationships.
It makes you feel good, when you walk and you think about stuff and you go through things in your head and sort them out. And it just makes you feel really good. (Participant J)
For some interviewees, the well-being from exercise came from having time alone. Sometimes this took on a spiritual quality, exercising in a way or place which was important for them.
Body image
For some female interviewees, exercise was a means to avoid gaining weight, and to look good. They articulated the societal pressures for this, which developed during adulthood.
I started doing the gym. I felt I needed to do it, to improve my looks. I think that’s probably why I am doing it now, trying to. In my mind it’s important to look nice. (Participant E)
No male interviewees expressed an aesthetic motivation to exercise, perhaps reflecting the cultural norms of males in this age group.
Competition
For some interviewees, competition provided an enjoyable sense of achievement, either within team sports, or in beating personal bests.
Well, I used to like being competitive, so if I did well in a competition, that gave me a boost. (Participant K)
Camaraderie
Team or group exercise was often a source of belonging and togetherness, and of long-term friendships.
I had a tennis four. We still call ourselves “the tennis four” …. We played, we drank coffee, we sorted the world out, helped each other out, forty something years, fantastic. (Participant R)
Some participants held negative views about their non-preferred exercise types, for example competitive sports or gym-based activities.
I can’t get up in the morning or go to a gym and do half an hour exercise. That is just not in my psyche. I wish I could, but I can’t. But I did play a lot of squash, I did play bowls, so I got plenty of exercise. (Participant M)
Many participants reported knowledge of the health benefits of exercise, but this tended to develop later in adulthood.
I think by that age I was probably beginning to understand that it wasn’t just about enjoyability. It was probably still about not putting weight and looking like somebody who worked near Bond Street and liked to kind of present herself in a certain way. But I think I was beginning to understand that this is also something that’s good for you. (Participant N)
In this case, the participant had a core, affective motivation to exercise, which was reinforced later by a secondary, reflective reason.
Theme 2: What helps?
Participants were mostly frequent exercisers, before and after their diagnosis of Parkinson’s. However, there were periods when they had exercised less, when focussing on careers, during child-rearing, or when recovering from illness. By exploring these times, participants were able to identify people, places and structures around them which provided opportunities or encouragement to exercise.
Active partners
Interviewees’ partners were often significant influences. Some joined in their partners’ exercise activities; others were brought into new social environments where exercise was integral.
After college, I met my husband who was a very keen rugby player… His life was always at the rugby club. So then, bringing up my children in that rugby club scenario, I started playing netball for Leamington ladies as well. And so that was really important to me, so yeah, I discovered sport again. (Participant Q)
However, where individuals’ exercise needs did not align with their partners’ interests, there were relationship tensions.
They [exercise classes] are in places which are very, very difficult and [my wife] has got her own life. It may be when she has a doctor’s appointment or something, or she’s got one of her hobby groups. How to get there…? (Participant A)
Flexible and supportive work
Work could have positive impacts on exercise behaviour, sometimes instrumentally by providing cycle parking, or by organising sports days which reinforced the social acceptability of exercise. In other cases, work introduced enjoyable physical demands on individuals.
I went to work with horses… I was doing a lot of physical activity, there was mucking out and going out to the fields to fetch them in and that kind of thing… I loved it, really loved it. (Participant J)
Participants highlighted the importance of autonomy and flexibility in their job roles to undertake exercise. Following their diagnosis, this further enabled them to alter or reduce their hours to focus on their health.
Work is very flexible… Today I went in, in the morning, to the office. Came home, brought some work home, and exercised in the back [garden] and then did some more work. So yeah, a lot of flexibility. (Participant O)
By contrast, some interviewees who were self-employed or were paid by the unit reported working very long hours, which left little time for exercise.
I used to work in the textile industry. I used to work basically, morning, afternoon and night…. It was hard, there wasn’t always time to get it. (Participant G)
Groups that bring people together
Many interviewees participated in group exercise classes. Their comments revealed complexity in group relationships, and the need to find groups which matched their needs. Some participants described a threshold of being ready, or not, to join groups with fellow PwP.
I feel I would like to be part of a group now, people with Parkinson’s… I feel like I’d like a more intimate discussion group with people I think about things that are important, like how people feel about the future… (Participant E)
The contrast between bonding relationships which form between people of similar backgrounds, and the bridging needed to involve people from more diverse backgrounds was also evident.
The ones at the dance class are all thinnish, mostly very thin and very high achieving and kind of pushing, self-pushing… I really enjoy it, I mean I find them very nice interesting people… I feel that I get on with them because I feel I am like that. (Participant F)
One of the things that we try and do in our group is have a coffee, either before or after… We’ve got people that we can talk to and say ‘Hello’ to when we turn up, rather than just do the exercises. And then if they want to take it further, we then have a ‘walk and talk’ … (Participant D)
Access to varied local exercise options
Individuals who were able to continue exercising after breaks, or adapt their exercise to their changing symptoms, highlighted how personal resources and a variety of options in their area significantly helped them.
Through the kids I just stopped. Wanted to go back to it [netball]… my back just couldn’t take it. So, I really needed to find something else that I really enjoyed, and some of my friends were joining this local tennis club, and I thought, do you know what, I’ll give it a go. I’m not brilliant, but I just absolutely loved it. (Participant Q)
The need for stable, regular and long-term options was highlighted by one participant who is involved in coaching other PwP.
I’d rather you slow it down and come more regular than get injured and then I don’t see you for a month or six weeks. The older we get, the more recovery time is, like we’re not young anymore and so we recover within a couple of days. (Participant O)
Interviewees with more severe physical impairments expressed the need to take advantage of any appropriate exercise option available, even if doing so had negative effects.
I do that [dance group], then horse-riding straight after on the same day. Unfortunately, after that I am that wiped out, totally wiped out, so that’s probably why I fell over. (Participant E)
Pleasant surroundings
Access to places where people felt comfortable was important, whether it was the natural world, or a friendly gym.
[My physiotherapist] got me on that [exercise on referral]. I went to the gym and it’s fine! It wasn’t intimidating at all…. It’s very welcoming and the people are very helpful. (Participant J)
Intergenerational activities
Many participants recalled childhood activities that sowed the seeds for exercise in adulthood, such as countryside walking. In turn, as participants became parents, the need to occupy and stimulate their own children reinforced their exercise behaviours.
We played it [tennis] as a family, when we went on holidays. If there was tennis or table tennis or anything with a ball, we’d probably favour a place like that. That’s how you sort of spend two or three hours to keep the younger people occupied. (Participant C)
Theme 3: Exercise with Parkinson’s
All participants believed that exercise is beneficial for PwP, though interviewees who had been diagnosed for longer reported that exercise was not promoted to them initially. Many were diagnosed as they were considering retirement or reducing work to make time for themselves, including doing more exercise.
Taking control through exercise
All participants viewed exercise as a means of exerting some control over Parkinson’s and ageing, and of retaining independence. Some articulated the tension between this and accepting the progressive nature of the condition.
I don’t want to be a vegetable. I want to work within the strictures of knowing I’ve got Parkinson’s. I know I can’t beat Parkinson’s but I don’t want Parkinson’s to overtake me massively. If I can contain it I will. (Participant A)
Exercise as a cure
Many participants believed that exercise could delay their disease progression, citing information from healthcare professionals and their own experience.
People that work in health that have dealt with me, like chiropractors, physios, GP, consultants. They all say that they consider that my Parkinson’s has not… has been slower shall we say in its onset or in its development, because I exercise. (Participant K)
Feeling guilt
The belief that exercise could slow their progression brought a source of hope for some, but it also brought feelings of guilt about how much exercise they should be doing.
One of the things that I’m constantly being told is that exercise is very good for Parkinson’s, so you’re always in the back of your mind, right I’ve got to go and do this exercise. (Participant C)
In some cases, the fear of being a burden to family was a strong motivator, while others felt tension about choosing between family and exercise.
I don’t want to be a burden on my wonderful partner and my kids when, the older I get and become a jabbering shaking idiot. I mean, which I will probably be, but if I can delay that for as long as possible… (Participant L).
My 21 year old, his girlfriend’s pregnant. So that would be amazing, and that will take up a lot of my time. So that’s the worry actually, a little bit about the exercise, I’m going to have to fit it in between baby duties as well. (Participant Q)
It gets harder to see the benefits
As peoples’ symptoms progressed it was harder for them to exercise, and harder to see the positive effect on their physical appearance or performance, which had motivated them previously.
It’s not really much motivation, because in the past when I did [exercise] I was seeing the benefits, especially with my marathon running… When I initially did Tai Chi and Pilates, I felt that [it] was helping really well and might stop me falling over. But it hasn’t really stopped me from doing that, so, yeah, that’s bad really. (Participant B)
This final quotation articulates the frustration felt by the more impaired participants of losing physical ability and having fewer exercise options, while hearing from more and more sources how important exercise is for Parkinson’s. It speaks to the importance of exercise-based interventions which facilitate a closer matching of individuals capabilities, opportunities and motivations.
Discussion
This study aimed to examine the social, cultural and environmental factors that influence the meaning of, and attitudes to, exercise. Through interviews with 18 PwP, insights were gained in three areas: their motivations to exercise, their external facilitators of exercise through their lifetimes, and the practical, psychological and emotional challenges of exercising with Parkinson’s.
Exercise as part of individuals’ identities
The results highlight how exercise motivations, whether aesthetic, psychological or social, often remain relatively constant. Research among stroke survivors has suggested that exercise experiences and behaviours are parts of individuals’ identities, and they shape their approach to exercise after stroke (Espernberger et al., 2023). Research into exercise and identity is limited among PwP. Qualitative studies investigating the meaning of exercise for PwP have found that preserving one’s identity as an active person was important (Eriksson et al., 2013; O’Brien et al., 2016), but differences between individuals’ exercise identities were not explored. Other studies have highlighted the importance of individualised exercise, but these have focussed on individualisation in exercise prescription rather than meaning or motivation (Amateis et al., 2019; Hunter et al., 2019; Rowsell et al., 2022).
Social support and groups
Social support is an important enabler of exercise (Schootemeijer et al., 2020), and exercise groups are common within NHS services (Parkinson’s Excellence Network, 2023). However, our study shows how varied PwP’s needs are. For some, exercise is an asocial activity. There may also be periods when individuals are unable to engage with other PwP. Interviewees spoke about why some groups worked for them and others didn’t, and about the skills of group leaders in bringing people together. This resonates with other studies. Researchers have found that PwP need different types of social support (informational, emotional and instrumental) at different times (Ravenek and Schneider, 2009). PwP have been found to experience anxiety when joining a group, driven by comparing themselves to other PwP, and to their imagined future selves (Sheehy et al., 2017). Participants in boxing classes cited the importance of love and care from inspirational instructors (Borrero et al., 2022), while a nurturing, cohesive and supportive environment was instrumental in long-term participation in another exercise class (Rossi et al., 2018).
The successful groups cited by interviewees were run by private or charitable organisations. Many participants had the resources to trial different options, which would not be the case for all PwP. Several participants had started exercise groups for PwP (D, O and P), perceiving the need for peer-led initiatives. There has been limited research into these (Soundy et al., 2019). Further studies into PwP exercise leaders could illuminate their experiences and support needs.
Cultural factors
Cultural influences were evident throughout the interviews. Walking in the countryside was a common activity, while being thin was a motivation among female interviewees, several of whom cited the influence of fitness videos such as Jane Fonda’s Original Workout. Research has shown how women with Parkinson’s from different ethnic backgrounds have variations in perceived ideal body shape and how this influences exercise goals and identity (Pentecost and Taket, 2011). The belief that Parkinson’s can be ‘fought’ was almost universally expressed. This homogeneity is unusual, as ‘fighting spirit’ is only one of several coping strategies among PwP (Charlton and Barrow, 2002; Haahr et al., 2021). It may reflect the predominant cultural background of the participants or their motivations to participate in research.
Strengths and limitations
The study had several strengths. The sample was well balanced by age, gender, geographical location and symptom severity. Interviewees had interests in exercise and its role in Parkinson’s, which enabled deep reflection. The narrative interview structure helped develop rapport to allow participants to speak about difficult topics, including adjustment, guilt and relationship tensions. The stimulus material reduced the chance of important influences on exercise behaviour being missed. A degree of validation of the themes was achieved through discussing them with PwP and physiotherapists.
However, we only recruited a small number of PwP from BAME backgrounds, due in part to the lack of diversity in Parkinson’s UK’s membership (Parkinson’s UK’s, 2022b). Efforts were made to reach groups for PwP from different ethnic backgrounds, but there was not time to develop these relationships. Nevertheless, some influences on exercise were found which have been previously documented among migrant or minority groups. Sporting prowess helped participant C assimilate as a child migrant, and climate unfamiliarity was a barrier to exercise for participant G. Participant O discussed how racist abuse led him towards karate as a means of self-defence.
A further limitation is that nearly all interviewees were regular exercisers, and few negative beliefs about exercise were expressed. Additionally, barriers such as pain, apathy and depression, which are common in PwP (Schootemeijer et al., 2020), were not substantially reported.
Implications for research
This research suggests that narrative interviews can successfully identify important influences on PwP’s exercise behaviours. They should be repeated among other groups, particularly among BAME PwP and those who have not regularly exercised. The findings highlight significant variation in PwPs’ exercise identities and needs. This supports our premise that deeper, more holistic understanding of individuals could improve exercise interventions. The alignment between the themes identified and the COM-B dimensions suggest that this model could underpin a future theory-based approach to designing individualised exercise interventions among PwP.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241296647 – Supplemental material for Exploring social, cultural and environmental factors that influence attitudes to exercise among people with Parkinson’s disease: A qualitative study
Supplemental material, sj-docx-1-hpq-10.1177_13591053241296647 for Exploring social, cultural and environmental factors that influence attitudes to exercise among people with Parkinson’s disease: A qualitative study by Fred Baron and Angeliki Bogosian in Journal of Health Psychology
Footnotes
Acknowledgements
The authors wish to thank the 18 people with Parkinson’s who participated in the study. The authors are grateful for the support from Parkinson’s UK in the recruitment of participants and patient advisory groups, and the help from the Association of Physiotherapists in Neurology in recruiting the peer advisory group members. Thanks to the group members themselves: Valsala Benn and Beverley Price; Jennie Meadway, Deborah Whitfield and Victoria Wright. Thanks also to the two anonymous peer reviewers for their positive and helpful comments.
Data sharing statement
The data generated during the current study are not publicly available due to resource constraints, but are available from the corresponding author on reasonable request. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Barts Charity (grant number G-002234).
Ethics approval
This study was approved by the City, University of London School of Health and Psychological Sciences Ethics Committee (Ref: ETH2223-1452, date: 15 May 2023).
Informed consent
All participants provided written informed consent prior to enrolment in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.