
Abstract
This mixed-methods study investigated how and why physical activity (PA), anxiety, depression and self-perceived loneliness are related, and the feasibility of social prescribing (SP). Whilst SP may involve PA with broader effects on health and wellbeing, there is little research exploring perceptions of this intervention. Data from the UCL-Penn Global COVID Study wave 1 (17 April–17 July 2020, N = 1037) were analysed. Twenty-one UK adults who self-identified as low (n = 15) and high (n = 6) on PA at wave 1 were interviewed at wave 4 (18 March–1 August 2022). At wave 1, depression was associated with higher odds of low-PA (OR = 1.05; 95% CI 1.01–1.10, p = 0.02). Both high/low-PA groups cited the threat of contracting COVID-19, general impacts of COVID-19 policies and heightened awareness of the mind-body connection. Five recommendations are made to address challenges in engaging with SP.
Introduction
The COVID-19 pandemic made countries globally enforce restrictions and lockdowns to reduce COVID transmission (Hale et al., 2021), which has led to: higher levels of psychological distress, loneliness (Carollo et al., 2022; Groarke et al., 2020; Wong et al., 2021), depressive and anxiety symptoms (Pieh et al., 2020) and reduced physical activity (PA) (Ding et al., 2021; Wilke et al., 2021). Also, 27.5% of the global population pre-pandemic were not meeting the World Health Organization (WHO, 2010) PA guidelines for health benefits (≥150 minutes of moderate-intensity, 75 minutes of vigorous-intensity or any equivalent combination of moderate-to-vigorous PA per week, Guthold et al., 2018). Considering both mental and physical health as interconnected global health priorities, research to understand the impact of COVID-19 is much needed to inform preventative responses to future practices around times of isolation or of limited access to PA facilities and equipment.
Studies to date have varied considerably on how PA is measured quantitatively and qualitatively (Stockwell et al., 2021). Often PA intensity and duration are measured using single items with little consistency across studies unless the standardised International Physical Activity Questionnaire (IPAQ-Short Form) (Craig et al., 2003) is used. Of the COVID-19 qualitative studies of PA to date, the focus has been on regular gym users (Kaur et al., 2020), older adults (Adams et al., 2021) or people with severe mental health difficulties (Newbronner et al., 2022). Only a few qualitative studies focusing on the general population (Hailey et al., 2022; Petersen et al., 2021). Little comparison is made between low and high-PA groups to understand why and how reduced PA is related to poorer mental health outcomes. Thus, this study used the IPAQ-SF to identify low and high-PA groups in the general population for follow-up interviews to understand the impacts of COVID-19.
Interventions improving an individual’s PA may directly improve mental health. PA has been found to reduce stress, anxiety, depression (Molarius et al., 2009; Rebar et al., 2015), protect against psychological distress during COVID-19 (Christoffersen et al., 2023; Wang et al., 2020) and lower risks of severe COVID-19 outcomes (Hamer et al., 2020; Sallis et al., 2021). Compared to physically active individuals, those with low-PA report poorer mental health and greater feelings of loneliness during COVID-19 (Meyer et al., 2020; Wolf et al., 2021; Xiang et al., 2020). Despite the mental health benefits of PA, people might have placed less emphasis on PA as a coping strategy for stress, anxiety and social isolation during COVID-19 (Faulkner et al., 2020). Social determination theory argues that relatedness is a basic psychological need for fostering wellbeing and motivation (Ryan and Deci, 2000). A UK longitudinal study found that 28.6% of adults in the general population reported sustained reduced PA level from the first global lockdown in March 2020 to post-lockdown in August 2020, with an additional 11.6% of adults being persistently inactive (Bu et al., 2021). Thus, limited access to outdoor space, changes in daily routine, concerns around catching the virus from indoor PA and ‘stay-at-home’ governmental advice are likely barriers to PA (Hailey et al., 2022).
Evidence indicates that SP – a targeted intervention that encourages individuals to engage with their social surroundings, communities and activities – can alleviate healthcare usage by increasing social connectedness and reducing anxiety, depression and feelings of loneliness (Costa et al., 2021). For example, research showed significant positive long-term impacts from participation in a 6-month exercise referral scheme on increased PA and improvements in physical and mental health outcomes at a 12-month follow-up (Prior et al., 2019). Like other research on SP (e.g. Pescheny et al., 2019), a significant proportion of participants did not respond to follow-up, highlighting potential issues with dropout. Interviews with lonely or isolated individuals highlighted they might be unwilling to join SP groups due to social fears and other unmet needs (Stuart et al., 2022). While community resources and support were highly valuable during COVID-19 (Hossain et al., 2020; Younan et al., 2020), literature on the potential of SP in addressing public health challenges from a global crisis is limited.
The current mixed-methods study leveraging the UCL-Penn Global COVID Study dataset (Wong and Raine, 2020) first establishes the impacts of the COVID-19 pandemic on PA and mental health outcomes (i.e. self-perceived loneliness, depression and anxiety) in the UK adult general population during wave 1 (17 April–17 July 2020). Participants who self-reported high or low-PA during wave 1 were followed up with a one-on-one semi-structured interview to examine how they have fared 18 months later (18 March–1 August 2022). The aims to understand: (1) the challenges of being physically active during COVID-19 and (2) their views toward ‘socially prescribing’ community-based activities as a pandemic recovery solution.
Methods
Participants and procedure
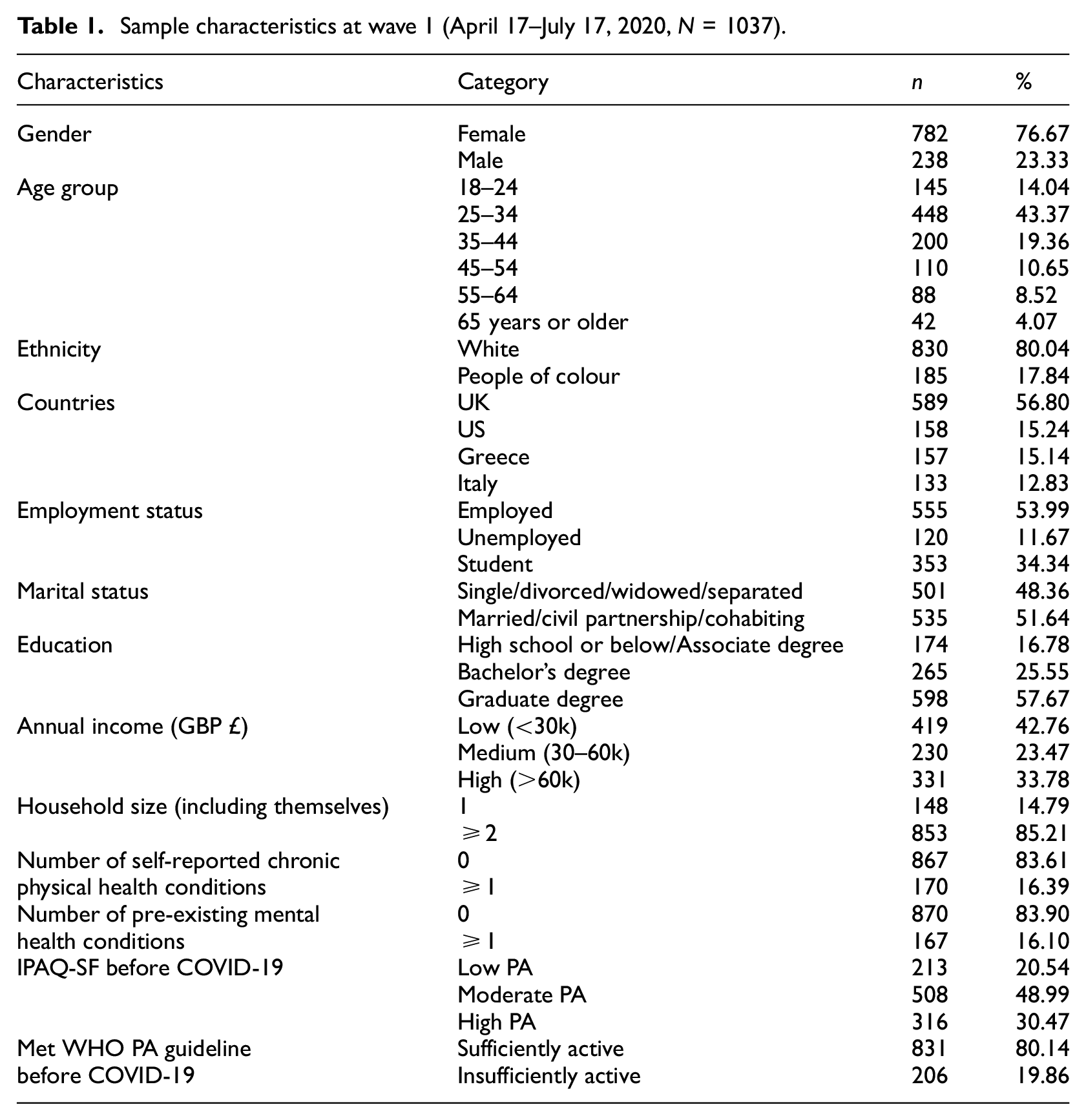
This mixed-methods study involved initial analyses of the UCL-Penn Global COVID Study (Wong and Raine, 2020; see https://osf.io/fe8q7/), a three-time-point longitudinal study (17 April 2020–21 July 2021) aimed to examine the short- and longer-term effects of COVID-19 on people’s mental and physical health and social trust in others. Altogether, 2288 participants (≥18 years old) with access to the Qualtrics study link on social media platforms and personal contacts were recruited using convenient sampling in wave 1. To contextualise the data, wave 1 data collection (17 April–17 July 2020) began 4 weeks after the first UK national lockdown was introduced in 2020 and ended in July 2020. The self-reported survey available in seven languages (English, Greek, Spanish, German, French, Italian and Chinese – traditional or simplified) measured physical and mental wellbeing, social trust towards others, common stressors, lifestyle, worries related to COVID-19 and sociodemographic factors. These were presented randomly to account for order effects. Data were analysed on a subsample of 1037 participants aged 18 and 89 years old (mean = 36.54, SD = 13.03) (see Table 1) with data on PA, anxiety and depression, and loneliness. Most participants resided in the UK (56.8%), 80.0% self-identified as White and 82.3% were living with one or more persons. Participants’ country of residence at the time of survey completion (a potential confounder due to country lockdown differences) was used rather than permanent residence. Only countries with the largest sample size were included (e.g. UK, US, Greece and Italy). This study was approved by the University College London Institute of Education Ethics Committee (REC 1331).
Sample characteristics at wave 1 (April 17–July 17, 2020, N = 1037).
Of the subsample with complete data on key study variables, all 320 UK respondents who self-reported as high or low PA levels as measured by the IPAQ-SF (Craig et al., 2003) in the wave 1 were invited take part in an online follow-up survey (Supplemental Appendix Figure 1). PA levels were categorised using frequency, duration and total energy expenditure measured as metabolic equivalent (METs) minutes spent on walking, moderate and vigorous-intensity PA over the last 7 days. Twenty-eight participants completed the online survey, of whom 21 (81.0% women) had one-on-one video call interviews between 18 March and 1 August 2022 (low-PA, n = 15; high-PA, n = 6). One participant had incomplete data on loneliness at wave 1 when inspected retrospectively, but data on all 21 participants were included in the qualitative analysis.
Participants received a study information sheet and completed an online consent form before seeing a 15-minute online survey. The first author (WH) then contacted participants via email to schedule a video call semi-structured interview (range = 24–64 minutes). Prior to the interviews, all participants were advised about confidentiality, data protection and reminded that their participations are voluntary. Informed consents and permission for video call recording were obtained verbally. All participants were debriefed (Supplemental Appendix 2), received information about local services and helplines, and a £10 shopping voucher for their time.
Measures
Data were collected at wave 1 (17 April–17 July 2020) and at wave 4 follow-up interview (18 March–1 August 2022; 18 months later).
The International Physical Activity Questionnaire – Short Form (IPAQ-SF) measures the frequency (in days) and time (in minutes per day) spent over the last 7 days participating in vigorous, moderate-intensity activity and walking (Craig et al., 2003). Aggregated times of walking, moderate and vigorous activities exceeding 960 minutes (equivalent to 16 hours) were excluded as outliers and any values below 10 minutes were re-coded to ‘zero’ based on the argument that a minimum of 10 minutes is needed to obtain health benefits. Participants were asked to reflect on their PA levels they regularly engaged in before and during the pandemic. Data were available at waves 1 and 4. Total PA was calculated by summing vigorous- and moderate-intensity and walking in MET-minutes/week (i.e. activities’ metabolic equivalent x the time spent in minutes × the number of days engaged in those activities). Higher MET-minutes/week indicates greater PA. IPAQ-SF responses were classified into high, moderate or low PA levels (IPAQ Research Committee, 2005): ‘High’: any combination of walking, moderate- or vigorous-intensity PA across seven or more days achieving ≥3000 MET-minutes/week; ‘Moderate’: any combination of walking, moderate- or vigorous-intensity PA across five or more days achieving ≥600 MET-minutes/week; ‘Low’: not meeting the criteria for the ‘High’ or ‘Moderate’ group. Furthermore, PA was dichotomised (insufficiently active = 0, sufficiently active = 1) based on WHO’s PA guidelines of recommended levels of activity (Bull et al., 2020) of ≥150 minutes of moderate-to-vigorous PA (equivalent to ≥600 MET-minutes/week).
The UCLA-Loneliness Scale (LS; Russell, 1996) is a 20-item measure on self-perceived levels of loneliness. Each item is rated on a 1 (never) to 4 (often) scale with higher scores reflecting more lonely feelings (range = 20–80). Whilst the LS has no standard threshold to indicate severe levels of loneliness, individuals in the top 15% or 1 standard-deviation from the mean (i.e. LS score ≥56) were classified as ‘highest level of loneliness’. Research has showed that LS is a reliable and valid for use in adults and epidemics/pandemics (Alsubheen et al., 2021; Das et al., 2021). One participant was not presented with questions on loneliness at follow-up due to technical issues and had to complete the survey post-interview.
The General Anxiety Disorder Scale (GAD-7; Spitzer et al., 2006) is a seven-item self-report measure of anxiety rated on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day). Higher scores reflect more anxiety symptoms (range = 0–21) with scores of ≥10 representing the clinical cut-offs of anxiety (Kroenke et al., 2007). The GAD-7 scale has high internal reliability (α = .89–.92) and is validated to use in the general population (Löwe et al., 2008; Shevlin et al., 2022).
The Patient Health Questionnaire (PHQ-9) is a nine-item self-report measure of depression (Kroenke et al., 2001) rated on a scale from 0 (not at all) to 3 (nearly every day). Higher scores reflect more depressive symptoms (range = 0–27), with scores of ≥10 indicating clinical cut-offs for depression (Kroenke and Spitzer, 2002). The PHQ-9 scale has high internal reliability (α = .89–.92) and is validated measure in the general population (Martin et al., 2006; Shevlin et al., 2022).
Participants self-reported on their sociodemographic information at wave 1: gender (male = 0, female = 1), age (18–24 = 0, 25–34 = 1, 35–44 = 2, 45–54 = 3, 55–65 = 4, or ≥65 = 5), ethnicity (White = 0, person of colour = 1), country (UK = 0, US = 1, Greece = 2, Italy = 3), employment (student (full/part time) = 0, working (full/part time) = 1, or not working = 2), marital status (single/separated/divorced/widowed = 0 vs. married/civil partnership/cohabiting = 1), education (high school degree or below/associate degree = 0, Bachelor’s degree = 1, or Graduate degree = 2), annual income (low < £30k = 0, medium £30–60k = 1, or high > £60k = 2), household size (total number of people in household including self: 1 = 1 vs. ≥2 = 2), chronic physical health conditions (none = 0 vs. one or more = 1, including: respiratory conditions, heart conditions, circulatory problems, diabetes, other medical conditions (e.g. cancer, epilepsy, lupus, sleep apnoea, obesity)), pre-existing mental health conditions (none = 0 vs. one or more = 1, including: alcohol or substance use disorder, anxiety disorder, bipolar disorder, depression, disruptive/impulse-control/conduct disorders, feeding/eating disorder, obsessive-compulsive disorder, schizophrenia and psychotic disorders, trauma and stress-related disorder and personality disorder). Data on gender, ethnicity, age, physical and mental health conditions were available at waves 1 and 4.
One-on-one interview: The semi-structured 8-item interview guide (Supplemental Appendix 2) was piloted and developed to understand: (1) the challenges of PA participation during COVID-19 and (2) participants’ views toward ‘socially prescribing’ community-based activities as a pandemic recovery solution. All interviews were conducted by the first author (WH).
Analysis
Quantitative data
Data were analysed using SPSS v.27. To test for normality, variables were assessed using histograms, Q-Q plots and the skewness and kurtosis values (>2 or kurtosis >7 = non-normal distribution). PHQ-9, GAD-7 and LS were normally distributed. The histogram of PA in MET-minutes/week measured by the IPAQ-SF suggests that the data were positively skewed and platykurtic, but the skewness and kurtosis values were under 2 and 7, respectively. Outliers were identified using boxplots and z-scores. Multivariate outliers were identified using the Mahalanobis distance method, and four cases warranted removal. Multicollinearity was assessed using tolerance value (<0.1) and the variance inflation factor (VIF > 10) (Field, 2018). All data met the assumption of collinearity for analyses. With moderate-PA during COVID-19 as the reference category, two logistic regressions with PA groups (low/moderate-PA or high/moderate-PA) and mental health outcomes (PHQ-9, GAD-7 and LS) were entered to predict the likelihood of low-PA group memberships during COVID-19, after adjusting for correlated sociodemographic variables (i.e. ethnicity, countries, employment, education, annual income, self-reported chronic physical health conditions and pre-existing mental health conditions) and pre-COVID-19 IPAQ-SF PA levels.
Qualitative data
All interviews were transcribed verbatim using GDPR-compliant paid transcription service Scrintal and carefully checked by WH to ensure accuracy. Data were anonymised. An inductive six-step reflexive thematic analysis (Braun and Clarke, 2006) was conducted, which involved: familiarising with the interview data, line-by-line coding using NVivo software, generating initial themes through mind maps, developing and reviewing themes and writing up. We adopted the critical-realist position, considering broader social context and systemic factors when explaining people’s behaviours and experiences. The first author worked as an NHS clinician throughout COVID-19 and was particularly aware of the potential risk factors to poor mental health because of the pandemic. She kept reflexive journal following the interviews, reflecting on her own positioning and biases. A second coder (JL) independently coded two transcripts and any discrepancies were discussed and resolved. Candidate themes were labelled, revised and discussed with the research team (KW and JL) to increase reflexivity.
Results
Quantitative results
Descriptive results. Table 1 presented the characteristics of 1037 participants at wave 1. The majority of the sample (39.6%) reported a moderate level of PA on the IPAQ-SF, followed by 35.7% of low-PA and 19.9% high-PA. 32.2% did not meet WHO’s PA guidelines for minimum PA (equivalent to ≥600 MET-minutes/week on the IPAQ-SF), and the median PA levels reduced by 28.5% from before COVID-19 to wave 1. The mean scores for depression and anxiety at wave 1 were 7.6 (SD = 5.7) and 5.8 (SD = 5.0), respectively, indicating mild depressive and anxiety symptoms. A significant number of participants reported clinical levels of depression (30.6%) and anxiety (21.6%) (Supplemental Table 1). The mean loneliness levels were 42.6 (SD = 11.4), with 15.1% (n = 157) self-reporting highest level of loneliness.
Predictors of low-PA or high-PA levels during COVID-19
Binary logistic regression with levels of depression, anxiety and loneliness as IVs predicting low-PA (moderate-PA = reference category) at wave 1 controlling for sociodemographic variables and pre-COVID-19 PA levels was statistically significant, X2(17) = 211.25, p < 0.001 (Supplemental Table 2). Individuals with higher levels of depression were more likely to be in the low-PA group at wave 1 (OR = 1.05; 95% CI = 1.01–1.10, p = 0.020). However, anxiety (p = 0.532) and loneliness (p = 0.504) were not significantly associated with higher likelihood of low-PA.
Binary logistic regression with levels of depression, anxiety and loneliness as IVs predicting high-PA (moderate-PA group = reference category) at wave 1 controlling for sociodemographic variables and pre-COVID-19 PA levels was statistically significant, X2(17) = 152.91, p < 0.001. Anxiety (p = 0.596), depression (p = 0.066) and loneliness (p = 0.603) were not significant predictors of high-PA, but ethnicity (p = 0.017), chronic physical health conditions (p = 0.029) and pre-COVID-19 PA levels (IPAQ-SF; moderate-PA = reference category) (high-PA, p < 0.001; low-PA, p = 0.008) were significant predictors of high-PA at wave 1.
Qualitative results
At wave 4, 21 UK participants were followed-up and interviewed one-on-one between 18 March and 1 August 2022 (Supplemental Table 3). Of whom, 15 participants were in the low-PA group (women = 86.7%, M = 45.8, SD = 15.7 years, range = 23–65) and six participants were in the high-PA group (women = 66.7%, M = 51.0, SD = 14.2 years, range = 33–72).
Low-PA group
Over half of the low-PA sample met clinical cut-off for depression (PHQ-9 ≥ 10; 53.5%) at wave 1, and this proportion halved (26.7%) at wave 4 follow-up. PA levels from wave 1 increased by wave 4 follow-up in two-thirds of the low-PA sample, while five participants (33.3%) reported no change.
High-PA group
One participant met the clinical cut-offs for depression and anxiety at wave 1 and wave 4 follow-up, respectively. Whilst five participants maintained their high-PA levels at follow-up, one participant reported low-PA level at wave 4.
Using thematic analysis, the researchers generated eight subthemes within two themes 18 months from the first global lockdown (Supplemental Table 4). These have provided further explanation to the quantitative findings of this study.
Theme 1. Challenges for PA Participation
Some participants described consistent levels of physical activity/inactivity, while the majority cited reasons for fluctuations in their PA levels as the pandemic unfolded.
Subtheme 1
The Threat of Contracting COVID-19. The majority of high/low-PA participants described an association between increased awareness of the COVID-19 virus and being ‘terrified’ for themselves and/or their social network: I was quite scared about it, and I was sent messages because I’m an insulin-dependent diabetic, telling me that I had to be very careful even to isolate at some point […] But people were very fearful […] it was very, very scary, not just physically, but therefore emotionally. (P04, 56 years)
Particularly, low-PA participants tended to avoid leaving their homes: […] I felt that if I stepped out of the house like I’d get COVID instantly, and I would feel unwell and stuff. So that worry of getting COVID and getting ill […] I value that more compared to my motivation to go outside and do my walks. (P18, 23 years)
As the pandemic unfolded, some low-PA participants described reduced PA when the ‘excitement’ and ‘novelty wore off’. Some high/low-PA participants expressed gratitude for the unanticipated benefits of the pandemic, namely re-evaluation of lifestyle and more time for PA. Yet, most recognised that the ‘sense of fear hasn’t dissipated’ (P21, 65 years) and ‘still have to be cautious’ (P02, 72 years). This has contributed to how people engaged with PA. Some high/low-PA participants have continued with online classes or outdoor PA instead of returning to indoor settings (e.g. gym, indoor classes) because these did not ‘feel safe’.
Subtheme 2. COVID-19 policies – ‘Groundhog Day’
Many participants spoke about the implications of COVID-19 policies on mental health and behaviours. Participants acknowledged that adhering to legalised COVID-19 policies resulted in loss of normal daily activities – including socialising, out-of-home movements, work, and hobbies. Both high/low-PA accounts described wanting and lacking physical contact with people, with some low-PA participants expressing feelings of loneliness caused by the absence of in-person contact. Many people recognised that the pandemic was more challenging for people living alone: […] I had gotten sixty days without a hug, without touching anyone […] my physical health risk from COVID is much, much less than the mental health risk of not being able to socialise or like have any social touch at all. (P13, 38 years, living alone)
While some – mostly older participants (≥55 years) – felt gratitude in technology enabling alternative ways to stay connected and widen their social network, several younger low-PA participants stated that virtual interactions were ‘not the same’ (P10, 24 years) and inadequate to meeting their social needs.
In addition to the (physical) social disconnection, a sense of listlessness coupled with boredom when ‘stuck’ at home were frequently acknowledged. Accounts did not differ between high/low-PA participants who asserted a need to keep busy or establish structure to their day, including through PA. However, this appeared insufficient considering the circumstances, as one high-PA participant reported: ‘[…] there were some times when it was just like no walking is going to fix this. I’m just too sad to know that the world is going to hell’ (P5, 46 years). Some low-PA participants mentioned their usual coping strategies were ‘taken away’, suggesting this need for maintaining their mental wellbeing were ‘denied’ forcibly.
In some cases of the low-PA group, the constraints of COVID-19 policies have resulted in sedentary behaviour and under- or over-eating: Initially when the first lockdown came, I must admit I hit the sugar quite badly […] what we really did with being at home all the time and not able to go out, we just basically gorged on everything. We didn’t stop eating at all. (P14, 56 years).
Subtheme 3. Heightened awareness of the mind-body connection
Many participants described having more time compelled them to focus on their physical and psychological health during lockdown, especially participants in the high-PA group. However, almost all acknowledged the challenges of maintaining PA due to competing demands post-lockdown. Specifically, one high-PA individual described feeling ‘panic’ and a sense of ‘guilt’ with less time to exercise when transitioning out of lockdown (P3, 33 years). Conversely, others from the low-PA group acknowledged an awareness of the ‘proven’ health benefits of PA, but this idea that ‘motivating yourself is the most difficult’ (P7, 27 years) was frequently described: […] from March 2020 till last September, it didn’t change because I was always at home sitting at my desk with my PC, eating ((laughs)) and I never thought to do better. I thought I have to start to do exercising, but I never started because I didn’t have the motivation, so it was very difficult. (P19, 45 years)
Motivation for PA was influenced by internal and external barriers. Low-PA participants frequently described the influence of external barriers, including limited space for exercising, unmotivating surroundings, missing usual exercise partner or groups, and seasonality. Consequently, some felt that PA was less rewarding and ‘pointless’. Others low-PA participants also acknowledged the contributions of psychological distress and symptoms of existing health conditions: Fatigue is a part of my condition anyway […] when I wasn’t doing anything, things like stamina definitely dropped off…my energy levels were really low. And because I was really stressed, I wasn’t sleeping well, so I was even more tired, and that additional stress was making me feel so much more exhausted and there just wasn’t really any way to kind of get any of that out. (P10, 24 years)
Several participants, particularly those with disability or mobility issues, emphasised feeling ‘different’ and frustrated that their fitness has been negatively impacted. People with existing or recently diagnosed health conditions may have fared worse – loss independence and suffered health consequences – as the pandemic unfolded. A low-PA participant described their experience with Long COVID: ‘I didn’t feel able to try or at times I was even afraid to try in case I brought on a symptom flare-up or went backward, took a step backwards in my recovery’ (P8, 29 years).
Theme 2. COVID-19 recovery solution: Barriers and recommendations for social prescribing
Almost all participants endorsed ‘social prescribing’, but many acknowledged barriers to access, engagement and maintaining involvement. The feasibility of SP may involve changes on multiple levels: interpersonal (e.g. the role of healthcare professionals), policy (e.g. resources and accessibility issues) and population (e.g. repositioning health systems – medical/social model). Thus, recommendations are suggested to overcome the identified barriers – in order of feasibility.
Subtheme 1. Listen to individuals’ concerns, collaborate and provide interventions to address doubts and needs
Some participants have experienced or predicted SP as an insufficient standalone intervention. Support needed to be ‘more regular and in-depth’ (P8, 29 years) and SP as ‘part of a package of care’: the thing that I worry about with social prescribing is thinking that is going to fix the system […] And it can’t. ((laughs)) So I would be really insulted if I came to my GP and described the traumatic ordeal I’ve been through and that I really need some professional mental health support. And they said, ‘Mmm. Well, we can’t do that, but have you tried gardening?’ …would be really upsetting for me because I am working so hard on trying to do everything I can to make links in the community. But I also need this professional support as well. (P13, 38 years)
Many participants highlighted the idea of ‘doing things with you’ (P4, 56 years). Some indicated that people are sceptical of being ‘told’ and prescribed with suggestions, implying a sense of mistrust exacerbated by COVID-19. This highlighted the role of clinicians, including GPs and link workers, to work collaboratively – to co-create – with people who are seeking help ‘to break it down for them’ (P11, 64 years). Active listening, empathy, curiosity, modelling and problem-solving are important for improving and maintaining engagement, increasing motivation and enhancing self-efficacy.
Subtheme 2. Provide options to increase personal capital through purposeful activities
Participants spoke about the importance of engaging in purposeful work or activity, especially during COVID-19 when opportunities and information were limited but may have helped nonvulnerable individuals to feel ‘useful’, to have ‘purposes’ and to feel ‘grounded’: […] everybody needs to work out and identify what feeds them in life. What gives them strength? What makes them feel good? What gives them energy? […] for some people, it will be connecting to nature or gardening […] that was something which I learned about myself. Thanks to this pandemic. (P5, 46 years)
Subtheme 3. Support individuals to (re)kindle relationships in the community to enhance wellbeing
Most participants endorsed SP to reduce loneliness and cultivate social connection, particularly the need to connect because of greater significance during COVID-19. Participants suggested that groups could link people to peer support in recognition that individuals can feel as though they are ‘the only one’ struggling, but also creating a sense of belonging: I’ve always been interested in what’s going on in the community […] it’s a great sense of belonging. So even if people don’t have family around them, they can feel that they do belong somewhere […] they’ve got a sort of a social group […] not just friends. There’s something a lot deeper than that. (P17, 54 years)
Subtheme 4. Offer diverse SP to meet various needs
Much of the feasibility of SP expressed in the data were related to practical challenge (e.g. cost, transport, disability, vaccination status, working hours), which seemed to derive from the idea of inequality and ‘what you can or can’t get now’ (P4, 56 years). Despite known benefits of SP groups, some participants stated that they would avoid or refuse SP due to a fear of social interaction or rejection, perhaps resonating with others who are socially anxious: […] you feel that you wouldn’t fit in with other people or like other people know each other and you don’t, or you don’t know what you’re doing or like you won’t meet anyone who’s like you, and then that will just make you feel more alone because you’ve tried, and you’ve still not found anything. (P16, 32 years)
Subtheme 5. Destigmatise mental health and its treatment
Many participants acknowledged the tensions between medical and social models that influence individuals’ attitudes towards mental health and its treatment. A few participants spoke about how the ‘negative connotation’ creates shame, preventing people from ‘admitting’ feelings of loneliness and/or isolation, and therefore seeking help. Others have acknowledged that participating in activities and the name itself – social prescribing – is more approachable. Most felt that SP could be effective as a preventative measure or in conjunction with medication. However, further changes in attitudes towards mental health, and a change to the idea of medication as ‘a quick fix’ are needed to improve its acceptability: […] I think we as a population have to understand what is best for us and work hard to do those things before immediately going to the doctor and saying ‘I feel anxious. Can I have some medication?’ And I think also the doctors as well probably have got to say do the social prescribing first before offering the medication as well, so it’s a bit of both. (P1, 58 years)
Discussion
This mixed-method study documented how and why physical activity (PA) and mental health were related during the COVID-19 pandemic and whether social prescribing could be a potential COVID-19 recovery solution. The quantitative (survey) and qualitative (interview) findings will be discussed in turn.
Our wave 1 quantitative findings showed that individuals with more depressive symptoms were more likely to be in the low-PA group, while anxiety and self-perceived loneliness were not significant predictors of low-PA group membership relative to moderate-PA. Furthermore, anxiety, depression and self-perceived loneliness were not associated with a higher likelihood of being highly active (high-PA) compared to moderate-PA. It is possible that the specific features of depression, such as anhedonia, lower energy levels and reduced motivation, play a significant role in low-PA (Leventhal, 2012). Whilst anxiety did not predict low/high-PA in our study, a Chinese cross-sectional study of college students conducted from February to March 2020 showed that PA had a stronger relationship with depressive symptoms than with anxiety symptoms (Xiang et al., 2020). These findings suggest that the relationship between PA and mental health are likely to be bi-directional. These are also in line with the mixed evidence around PA for reducing anxiety and consistent findings of the antidepressive effects of PA in both clinical and non-clinical populations (Rebar et al., 2015).
Interestingly, our wave 1 logistic regressions indicated that self-perceived loneliness did not predict an individuals’ group membership of low or high-PA. This indicates that loneliness levels were not different across the groups, and other factors might have influenced PA during the pandemic. Indeed, our qualitative analyses supported this as participants in the low-PA group described a lack of intrinsic motivation and enjoyment without the social aspects of PA participation. Therefore, encouraging PA co-participation within the family or household during lockdowns might be beneficial (Faulkner et al., 2020). Given that individuals in solitary living and with long-term physical and mental health problems tended to be inactive relative to the fairly/highly active groups (Bu et al., 2021), the role of health status and social support in PA is highlighted. Greater adherence to COVID-19 policies (i.e. avoiding crowded places/ public transport, staying at home and reducing travels) and solitary living were also associated with high levels of loneliness (Christoffersen et al., 2023). Altogether, policy makers should consider the impact of isolation and limited access to PA facilities/equipment on people’s physical and psychosocial wellbeing, while creative ways to reduce persistent feelings of loneliness and/or physical inactivity are necessary.
Qualitative interviews explained key reasons behind the quantitative findings. UK participants who self-identified as low or high-PA at wave 1 spoke of three themes that promoted and hindered their PA during the pandemic: the (1) threats of contacting COVID-19, (2) impacts of pandemic-related policies and (3) heightened awareness of the mind-body connection. Whilst some participants reported positive changes and adjustment during and post-lockdowns, others have fluctuated in their PA and mental health. To improve people’s psychosocial wellbeing, the majority of interviewees have endorsed SP to address loneliness and social isolation. All participants acknowledged practical and emotional barriers to accessing support and engaging with this intervention. Therefore, five recommendations for clinicians were identified to increase the viability of SP: (1) working collaboratively with clients to address doubts and needs, (2) providing options in purposeful activities, (3) (re)kindling relationships for wellbeing, (4) offering diverse SP to meet various needs and (5) destigmatising mental health and its treatment.
A key finding from the qualitative analyses suggests that high/low-PA participants expressed limited opportunities for usual out-of-home PA (e.g. walking, cycling or commuting to work or other activities) when adhering to COVID-19 policies. Similar to regular gym users (Kaur et al., 2020), the high-PA participants in our sample adapted their usual PA routines while some of the low-PA participants spoke about a lack of motivation to be physically active during the pandemic.
Our interview responses show that participants recognised the benefits of SP for maintaining psychosocial wellbeing because of learnings from COVID-19, yet there are also known barriers to entry for individuals with different needs. These findings are consistent with previous research on the fundamental human need to feel socially connected with others and the values in belongingness were acknowledged (Hossain et al., 2020; Younan et al., 2020). Several theories, including theory of planned behaviours (McEachan et al., 2011), social determination theory Ntoumanis et al., 2021) and social cognitive theory (Young et al., 2014), have stressed the significance of social support and social connectedness in PA behavioural change. Activity coach characteristics, shared learning opportunities/experiences and increased meaningful interaction were valued by older adults who participated in PA intervention to reduce loneliness (Franke et al., 2021).
Despite this, social fears of being in groups, feelings of loneliness, stigma and social isolation were barriers that may prevent people from accessing support in the first place or engaging with SP, even though SP can address the same issues (Stuart et al., 2022). Clinicians therefore could implement coproduction with and for individuals. Finding ways to (re)build trust and engage people with SP is important given that participants predicted people may resist a social cure model and being prescribed with activities compared with a predominant medicalised healthcare model. Thus, organisational and policy levels to address practical challenges, inequality and population beliefs about mental health and its treatment are needed.
Limitations
This study has several limitations. Firstly, 80.0% of the sample at wave 1 was White, which limits the generalisability of findings to non-White communities. Second, the current findings are potentially susceptible to recall biases with primacy and recency effects, as UK participants may have different reference points during the interview. Future research should examine changes in PA and mental health using waves 2 and 3 of the Global COVID study datasets (Wong et al., 2021). Although many people feel that the pandemic has ended, continued research examining the longer-term impact of COVID-19 on people’s PA and mental health are necessary and valuable.
Conclusion
The health benefits of regular PA are widely recognised. Our findings show that depression is associated with low-PA level during COVID-19. The threat of contracting COVID and impacts of COVID-19 lockdown policies may have resulted in reduced PA levels. While some participants spoke about improvements to PA levels and mental health post-easing of lockdowns, others described ongoing psychological distress and/or reduced PA that should not be ignored. These are informative for future practices around times of isolation or situations where people may have limited access to PA/outdoor space. Our findings also suggest that social prescribing, generally supported by the participants, can be effective when practical and emotional barriers are also addressed. Multilevel changes, including interpersonal, policy and population, are important to increase the viability of SP.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241275599 – Supplemental material for The impact of COVID-19 on physical activity and mental health: A mixed-methods approach
Supplemental material, sj-docx-1-hpq-10.1177_13591053241275599 for The impact of COVID-19 on physical activity and mental health: A mixed-methods approach by Wai Tung Hung, Vaughan Bell and Keri Ka-Yee Wong in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to thank the 21 UK participants with whom we interviewed. They have dedicated their time to speaking to us and sharing their stories, reflections and insights, contributing to the research on the impacts of COVID-19 pandemic. Thank you to Jaimie Ka Yu Leung for her contributions in coding and for sharing her insights.
Author contributions
WTH and KW were involved in designing and conceptualising the study. KW was involved in providing secondary data for the quantitative phase of this project. WTH and KW were involved in coordinating the data collection for the qualitative phase. WTH was involved in qualitative data collection. WTH was involved in analysis and interpretation of both quantitative and qualitative data. KW and VB were involved with the supervision of the work. WTH was responsible for manuscript writing with contributions from KW and VB. All authors reviewed the final manuscript.
Data sharing statement
Data are available from the corresponding author, upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the UCL Doctorate in Clinical Psychology, funded by Camden & Islington NHS Foundation Trust and the UCL Global Engagement Fund. K.W. is currently funded by the ESRC Policy Fellowship (ES/Y004906/1).
Ethics approval
This study was approved by the University College London (UCL) Institute of Education Research Ethics Committee (REC 1331) with an amendment made to collect wave 4 data. This was approved on 9th February 2022.
Pre-registration OSF links
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.