
Abstract
This study aimed to explore how social distancing and self-isolation measures, aimed at protecting vulnerable groups from COVID-19, affected the wellbeing and physical activity levels among adults diagnosed with asthma. Twenty-seven participants took part across four online focus groups. Transcripts were analysed using thematic analysis. Participants reported becoming more health conscious due to being labelled as vulnerable. Their relationship with the severity of their asthma was altered and they reported making positive changes to increase their physical activity levels. Findings suggest there is a window of opportunity to engage with people diagnosed with asthma to promote beneficial lifestyle changes and self-management.
Introduction
Coronavirus disease (COVID-19), caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SAR-CoV-2), was declared a pandemic by the World Health Organization in March 2020 (World Health Organization, 2020a). The virus primarily targets the respiratory system, resulting in symptoms including fever, coughing and anosmia/hyposmia and is transmitted from person to person, spread mostly via respiratory droplets or contact with contaminated surfaces (Rothan and Byrareddy, 2020). To reduce transmission, governments all over the world have advised the public on both hand hygiene and social distancing as preventative steps (World Health Organization, 2020b).
Evidence regarding the impact of COVID-19 on individuals with underlying health conditions is limited. As a result, the World Health Organization (2020c) devised a list of vulnerable groups who were considered to be more at risk. Additional measures have been taken to protect these vulnerable groups; countries such as Australia, Canada, Norway, Singapore and Switzerland introduced ‘protective self-separation’ to avoid unnecessary face-to-face social interactions and physical contact with others (Health Information and Quality Authority, 2020). However, some countries, including the UK, took highly protective measures to ‘shield’ those who are vulnerable to severe illness. The Chief Medical Officers of the UK developed the Shielded Patient List, which identified individuals who were deemed ‘Clinically Extremely Vulnerable’ from the effects of COVID-19 (NHS Digital, 2020). Those identified received an individualised letter advising them to ‘shield’ and to self-isolate at home, from the 23rd March 2020 until the 16th August 2020 to prevent themselves coming into contact with the virus (Public Health England, 2020).
Understanding individuals’ responses to being identified as vulnerable are important to improve the support given in such circumstances. Leventhal’s Common-Sense Model (2016) proposes that perceptions about illness, such as COVID-19, are important determinants of behaviour and that in the face of a health threat, people may either act to address the health threat or choose to ignore it. Research has shown that vulnerable individuals are anxious about their vulnerability to COVID-19 and what it would be like for them if they were to contract the virus (Malhotra et al., 2020; Philip et al., 2020a).
The importance of staying active during the pandemic has been emphasised due to its multiple benefits on physical and mental wellbeing (Dwyer et al., 2020; Lades et al., 2020; Matias et al., 2020). However, prolonged self-isolation may make maintaining a physically active lifestyle challenging by both increasing sedentary behaviours and reducing physical activity with a resulting decline in health (Chen et al., 2020). Therefore, we must seek to identify how social distancing and self-isolation may have influenced physical activity levels (Arora and Grey, 2020).
Limited data exist on how protective measures have affected the wellbeing and physical activity levels of vulnerable groups. Therefore, this study aimed to explore the effects of social distancing and self-isolation on the wellbeing and physical activity levels of vulnerable individuals. Due to the severe adverse outcomes, respiratory viruses can have on people diagnosed with asthma (Busse et al., 2010) and how prevalent the disease is globally (World Health Organization, 2020d), we chose this population group to be used as an exemplar of a vulnerable group. Findings will inform how we can support this population group and other vulnerable groups during this and future pandemics.
Methods
Design
A cross-sectional qualitative study was carried out, using data collected from focus groups with adults diagnosed with asthma. Focus groups were conducted online using the video-conferencing application ‘Zoom’ (Zoom Video Communications Inc, Version: 5.0.3). The study was conducted according to good clinical practice and approved by the University of East Anglia Faculty of Medicine and Health Sciences Research Ethics Committee (Reference: 2019/20-100).
Participants and recruitment
Participants were recruited through convenience sampling, using advertisements posted on Facebook. The advertisements briefly explained the study to potential participants and requested anyone interested to complete an online eligibility questionnaire. Potential participants were deemed eligible if they were over 18-years old with a diagnosis of asthma (evidenced by potential participants self-reporting that they were currently prescribed asthma medication) and had access to a smartphone, computer, laptop or tablet with an internet connection. Anyone unable to speak English, unable or unwilling to provide informed consent, or with a diagnosis of any other respiratory condition was not eligible to take part.
Potential participants who met the inclusion criteria were emailed an invite to participate in the study with a link to an online participant information sheet. Those who were still interested were asked to complete an online consent form. Consent was verbally reaffirmed at the start of the focus group, which was audio-recorded.
Variation in asthma severity and physical activity levels were selected to obtain diversity within the sample. Participants were allocated to different focus groups based on their asthma severity (i.e. moderate or severe asthma, in terms of their requirement for long-acting bronchodilators or not). Each group included participants reporting different levels of physical activity prior to the social distancing and self-isolation measures. Focus groups were arranged when an adequate number of eligible participants were available. Participants were compensated with £20 worth of shopping vouchers for focus group participation.
Four focus groups were conducted: two focus groups were conducted with participants with moderate asthma, and two focus groups with participants with severe asthma. Although data was collected from participants with moderate asthma separately from those with severe asthma, the same themes were present across both groups. Therefore, all participants and their narratives were analysed together.
Data collection
The semi-structured online focus groups were conducted in May 2020. At the time of data collection, specific lockdown measures had been lifted within the UK, but people identified by the NHS as ‘Clinically Extremely Vulnerable’ were still self-isolating. Participants were asked to complete a brief online questionnaire before the commencement of the focus group. The questionnaire was used to collect demographic information (e.g. age, gender, ethnicity and employment status), physical activity levels (General Practice Physical Activity Questionnaire: Department of Health and Social Care, 2013)), and to determine the level of asthma control (the validated Asthma Control Test (Asthma UK, 2002).
Every effort was made to ensure data security and protection of the focus groups by using the highest levels of security available to ensure that only consenting participants could join. Participants joined the focus groups through the available two-factor authorisation and following admission via the ‘waiting room’, a virtual staging area that stopped participants from joining automatically, participants were admitted. Once all participants had been admitted, the virtual room was ‘locked’ to prevent uninvited entry and creating a secure environment free from interruption. With the participant’s permission, all focus groups were audio-recorded.
A standardised topic guide was used during the focus group, informed by the objectives of the study. Questions included: What effect has social distancing and self-isolation had on your physical activity levels?, How do you feel about current restrictions being lifted? and What do you think of the information and guidance that has been provided during the pandemic? Questioning remained flexible to allow for full probing of any relevant issues raised by the participants. Focus groups lasted between 76 and 96 minutes. All the audio-recordings were transcribed verbatim except all names of participants and places which were anonymised to assure confidentiality.
Data analysis
We used Braun and Clarke’s (2006) Thematic Analysis to analyse the narratives collected in the online focus groups. An inductive, bottom-up approach was used, which involved identifying, analysing, and reporting patterns of meaning across the dataset. The initial stage of the analysis started with the familiarisation process. This process involved reading, and re-reading transcripts, highlighting points of interest and significance (Braun et al., 2016). Focus groups were independently coded. Sections of the transcripts relevant to the research objectives were highlighted and given shorthand labels or ‘codes’ to describe their content (Braun and Clarke, 2006). Initial themes and sub-themes were then generated by reviewing codes and identifying the similarities and overlap between them (Braun et al., 2016). Thematic mapping was used to explore the relationships between codes and themes, and themes and sub-themes. The research team revised and refined the initial themes and sub-themes by assessing the data associated with each theme. Theme names were devised to capture the sense of each theme, and then the final themes were evidenced by data extracted directly from the transcripts (Braun and Clarke, 2006).
Data sharing statement
The current article includes the anonymised transcripts of the focus groups conducted in this study. Pending acceptance for publication, all of the data files will be automatically uploaded to the Figshare repository.
Results
Participant characteristics
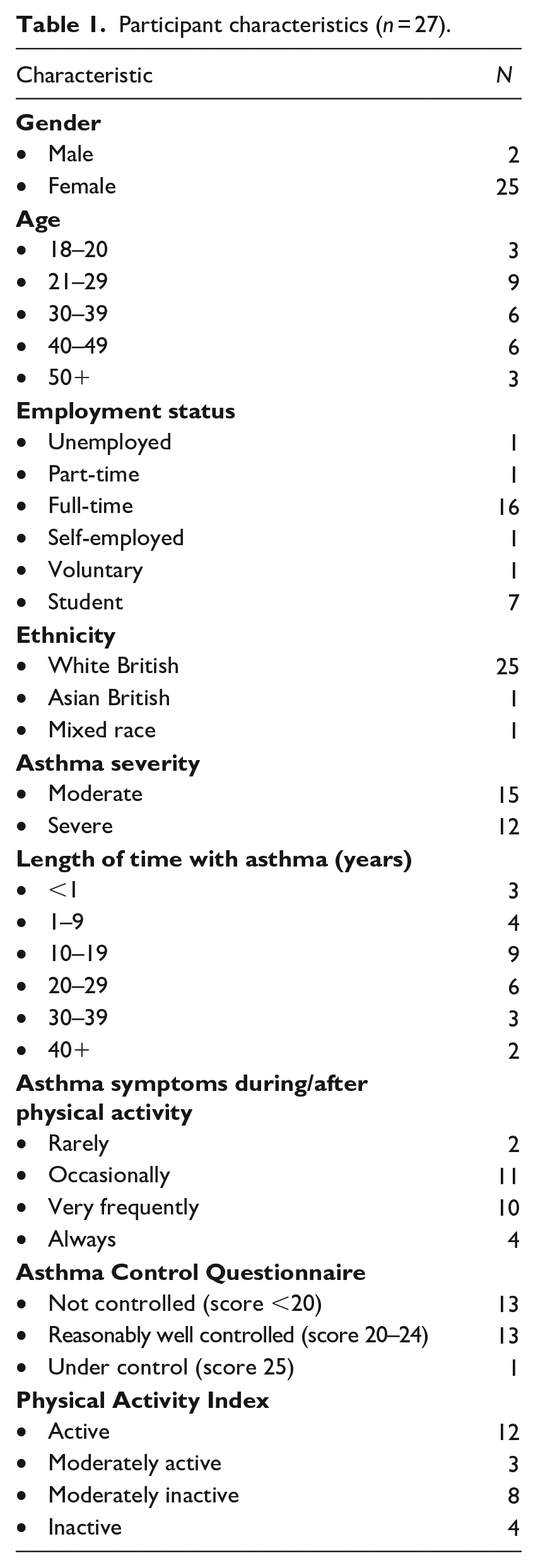
Participants characteristics are depicted in Table 1. Overall, a total of 27 participants (2 men and 25 women) took part across four focus groups. The majority of participants were between the ages of 21–29 (33%), white British (93%) and in full-time employment (59%). Fifteen participants (56%) had moderate asthma, and the remaining 12 (44%) had severe asthma, with most participants symptoms being reasonably well controlled (48%) or uncontrolled (48%). Length of time with asthma varied, but the majority of participants had had asthma for 10–29 years (56%). Twelve participants (44%) were considered active, with most participants occasionally (41%) or very frequently (37%) experiencing asthma symptoms during or after physical activity.
Participant characteristics (n = 27).
Themes identified
We identified four key themes from the data:
Becoming Identified as Vulnerable;
New Ways of Being Physically Active While Social Distancing and Self-Isolating;
The Availability of Information and Guidance on Social Distancing and Self-Isolation with Asthma; and
Looking Ahead and Returning to ‘Normal’.
The four key themes identified from the data are described below. These, along with sub-themes, are presented in Figure 1.
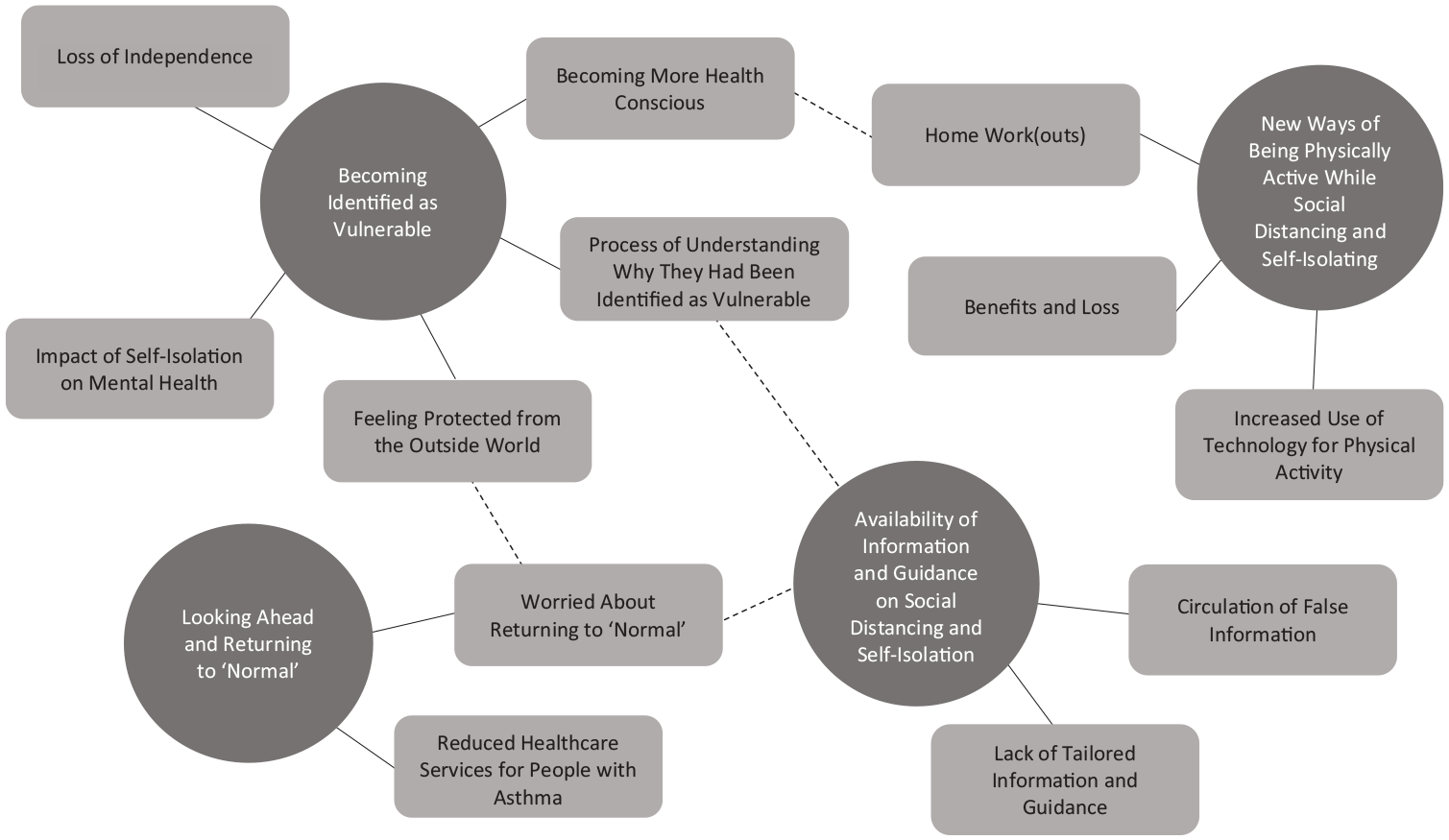
Thematic map, with the four main themes (a solid line demonstrates a relationship between a theme and subtheme and a dotted line indicates a relationship between a theme/subtheme and a subtheme from a different theme).
Theme one: Becoming identified as vulnerable
The continuously changing criteria made it difficult for participants to make sense of why they had or had not been identified as vulnerable and received a letter to shield. Being identified as vulnerable, increased participants worry about contracting the virus, and as a result, their homes became their safe place during the pandemic. However, they were concerned about the effects of self-isolation on their mental wellbeing. Their increased vulnerability also made participants more conscious of improving their health and giving themselves a greater chance of recovering if they were to contract the virus.
Process of understanding why they had been identified as vulnerable
Many participants had gone through a process of trying to make sense of why they had or had not been identified as vulnerable. They were unsure if it was the number of hospital admissions they had had, the medication they had been prescribed or simply having been diagnosed with asthma that defined them as vulnerable. This process was made difficult by the continuously changing criteria: “I think with asthmatics the way they’ve changed their minds on the list, with what drugs you’re on and then that’s kind of been - you have to keep looking at it to see where you sit on the list. . .” [Participant Twenty-Five - Female, 30-39, Moderately Active, Moderate Reasonably Well Controlled Asthma].
Some participants were confused as to why they had received a letter to shield, as they would not have defined themselves as a vulnerable person, nor did they match the perceptions of someone vulnerable. This put them in a difficult position when having to rely on friends and family for help and support whilst self-isolating, as they did not want to feel like a burden: “. . . it definitely feels a bit of a tricky category because everyone’s seen - thinks of the vulnerable as like the old people or people who are really poorly or whatever” [Participant Six – Female, 40-49, Active, Moderate Uncontrolled Asthma].
Whereas several participants did consider themselves vulnerable but had not received a letter to shield, which left them feeling unprotected from the virus: “I have terrible chest infections every year. Not as bad as you guys-some of you guys, but it still - I’m still feeling quite vulnerable” [Participant Five – Female, 40-49, Active, Moderate Reasonably Well Controlled Asthma].
Feeling protected from the outside world
For participants who were self-isolating, their homes had become their safe place. The possibility of being exposed to COVID-19 whilst outdoors was daunting for participants and being at home gave them a sense of protection from the outside world: “. . . I think I’ll be a bit more apprehensive about leaving the house as well because the house is your safe place at the minute. . .” [Participant Fifteen – Female, 30-39, Inactive, Severe Uncontrolled Asthma].
With the criteria for being identified as vulnerable continuously changing, participants who were self-isolating feared they would no longer meet the criteria and would be de-shielded (no longer being shielded). Knowing someone who had been de-shielded only increased participants worry: “I know some people who have been de-shielded when they shouldn’t have been, like asthmatics. And there’s always that fear of what if they do it to me next” [Participant Seventeen – Female, 21-29, Active, Severe Uncontrolled Asthma].
Impact of self-isolation on mental wellbeing
The protective measures that were introduced dramatically changed participants lives and the long period of self-isolation had a negative impact on the mental wellbeing of some participants, particularly those who had been isolating alone: “As depression sets in-so, it’s you know-it’s really miserable being in on your own all the time” [Participant Three - Female 21-29, Active, Severe Reasonably Well Controlled Asthma].
To avoid the negative impact, several participants spoke of changing their mindset and accepting the situation they have found themselves in. Reminding themselves that they were not the only ones having to self-isolate and that they were not only keeping themselves safe but others too, made the situation easier: “Yeah, I think for me, I had to have a real mind shift on the whole - on the whole staying in and I just kind of put a positive spin on it” [Participant Three – Female 21-29, Active, Severe Reasonably Well Controlled Asthma].
Becoming more health conscious
Being identified as vulnerable, increased participants worry about contracting COVID-19. As a result, participants had become more conscious of their health. As such, they talked about reprioritising their health as central, made possible by increased time and focus: “. . .I found actually the lockdown, the COVID scenario of having to be home all the time and self-isolate, I’ve actually had more time to focus on my health, and it’s become the number one priority” [Participant Eight – Male, 21-29, Inactive, Moderate Uncontrolled Asthma].
Several participants acknowledged that they had not taken their asthma seriously before the pandemic, but after being made aware of their vulnerability to the virus, they started to take their asthma more seriously: “I sort of think of myself as fairly fit and I yeah, I’m very much a minimalist with my asthma, but actually, I need to take it a lot more seriously” [Participant Six – Female, 40-49, Active, Moderate Uncontrolled Asthma].
For some participants, there was an intent behind the shift in focus. Some believed that by improving their health, they would have a greater chance of recovering if they were to contract the virus: “. . .I feel like I need to be more physically active because it doesn’t really affect my asthma, but it will protect me more in case I do get infected” [Participant Twenty-Six – Female, 30-39, Moderately Inactive, Moderate Uncontrolled Asthma].
Theme two: New ways of being physically active while social distancing and self-isolating
Self-isolation meant that participants usual physical activity routines had changed. Their reluctance to be outdoors meant that they opted to be more active at home. Participants who were more conscious of improving their health made an effort to increase their physical activity levels, but they were concerned about pushing themselves too much in fear of triggering their asthma symptom. Increasing their activity levels benefited them both mentally and physically, but the lack of social support and opportunity affected their motivation to be active.
Home work(outs)
Whilst self-isolating, participants usual physical activity routines had changed completely. They no longer had access to their usual forms of physical activity and had become reluctant to be active outdoors. Instead, participants reported having been more active at home: “So, then that [the pandemic] kind of pushed me into doing it at home. I never did it at home before” [Participant Nineteen – Female, 21-29, Inactive, Moderately Active, Moderate Reasonably Well Controlled Asthma].
Self-isolation meant that participants had lost the activity that was built into their daily routine. Having to work from home, meant participants were more sedentary than they usually would have been, and this had an impact on their daily step count: “I’m usually working in an office, but at school, I usually walk around the school but obviously at home I’m just sat in front of the computer” [Participant Thirteen – Female, 21-29, Moderately Inactive, Severe Uncontrolled Asthma].
Participants who considered themselves active before the pandemic had found it harder to adjust. They had new priorities, such as home-schooling, so had to find the time and make more of a conscious effort to be active: “But actually, being cooped up inside has meant that it’s harder to be active because you aren’t walking around, you aren’t doing things” [Participant Seventeen - Female, 21-29, Active, Severe Uncontrolled Asthma].
Previously inactive participants who were more conscious of improving their health used the pandemic as an opportunity to increase their physical activity levels gradually: “I personally have probably been more active during COVID-19” [Participant One – Male, 30-39, Moderately Inactive, Severe Uncontrolled Asthma].
Several participants were concerned about pushing themselves too much during the pandemic and were holding back. They feared that physical activity would trigger asthma symptoms and were worried about having to go to hospital and thus the possibility of being exposed to COVID-19: “. . .I think during COVID, I’ve been more scared you know to push the limits of my fitness for fear of having an asthma attack or being exposed to COVID” [Participant Seventeen – Female, 21-29, Active, Severe Uncontrolled Asthma].
Benefits and loss
Increasing physical activity during the pandemic benefited participants both mentally and physically. Specifically, several participants reported a reduction in the use of reliever medication and improved asthma symptoms. Experiencing these benefits was motivational for participants and encouraged them to continue making improvements in physical activity efforts: “I actually felt better for some reason and feel better then the hours after that. So, that encouraged me to go for longer. . .” [Participant One – Male, 21-29, Moderately Inactive, Severe Uncontrolled Asthma].
However, for some participants, it was challenging to stay active whilst self-isolating as they had lost their social support networks and, in some cases, this included a person they were usually active with: “I think a lot of us when we’re exercising, especially within COVID and stuff at the moment, where we’re doing [exercise] individually, you’re losing that [social support]. . .” [Participant Fourteen - Female, 21-29, Active, Severe Reasonably Well Controlled Asthma].
As self-isolation had gone on, participants had found it difficult to self-motivate themselves because of the lack of opportunities, and had lost motivation to be active: “I found my motivation is just the one that kills me; I have no motivation to do anything because I can’t go anywhere, I don’t see a reason to do it [exercise] almost” [Participant Twenty – Female, 40-49, Moderately Inactive, Moderate Uncontrolled Asthma].
Theme three: The availability of information and guidance on social distancing and self-isolation with asthma
All groups felt that during the pandemic, they had not been given enough information and guidance on managing their asthma in the new climate. This was particularly problematic in the early stages of the pandemic when participants did not know what to do. Later on, the biggest problem for participants was the lack of consistency with the information and guidance that had been provided and the contentiously changing messages: “But I think as an asthmatic, although Asthma UK are trying, they change their messages on their website every five seconds and unless you keep an eye on it, you don’t know what’s going on. It’s quite hard to get it [information] though” [Participant Seventeen – Female, 21-29, Active, Severe Uncontrolled Asthma].
Information and guidance that had been given by the UK Government were not tailored, and participants felt that there was not enough available specifically for people with asthma. When participants had questions, healthcare professionals did not seem to have any answers, but they did acknowledge that they were trying their best: “. . .because I’m asking them [healthcare professionals] questions, and they don’t have sometimes enough information to give to myself because they just, they just don’t know enough about it” [Participant Twenty – Female, 40-49, Moderately Inactive, Moderate Uncontrolled Asthma].
Therefore, several participants reported trying to self-educate themselves about the situation, but with false information circulating (e.g. the misinformation on social media that inhaler corticosteroid therapy increased the risk of COVID-19), it was difficult for participants to know what information could be trusted: “I think especially in the beginning because a lot of people were scared to almost take their preventers” [Participant Fourteen – Female, 21-29, Active, Severe Reasonably Well Controlled Asthma].
Theme four: Looking ahead and returning to ‘normal’
Returning to ‘normal’ once restrictions had been lifted was a worry for some participants. They doubted that social distancing could be implemented properly and if they could trust other people to follow the guidelines. Participants were also apprehensive about the likelihood of having to wear a facemask, and the adverse effects it could have on their breathing. They were concerned about the long-term effects on the healthcare system and the possibility of reduced access to healthcare services for people diagnosed with asthma.
Worried about returning to ‘normal’
In all groups, participants expressed concerns about returning to ‘normal’ and if the pandemic would ever be completely over. Participants were worried about restrictions being lifted, particularly those who had been self-isolating. They did not think that the public would follow guidelines and doubted that social distancing could properly be implemented: “. . .I mean, where I am people are not being safe, and it has kind of stopped me this last week wanting to go out again” [Participant Twenty-Two – Female, 21-29, Active, Moderate Uncontrolled Asthma].
Participants were also apprehensive about the possibility of having to wear a face mask once their self-isolation had ended and the adverse effects it could have on their breathing. Because of the possible adverse effects, they believed that more guidance needed to be made available about wearing face masks as there was confusion over whether people with asthma should be wearing them or not: “Because I tried one, but I could hardly breathe with it” [Participant Ten – Female, 50+, Inactive, Moderate Reasonably Well Controlled Asthma].
Reduced healthcare service for people with asthma
By prioritising COVID-19 over non-COVID-19 conditions such as asthma, participants thought there would be a long-term effect on the healthcare system. Several participants reported having their usual asthma medications changed or delayed during the pandemic, and they worried that it would be a long process to reintroducing them: “. . .but they stopped all biological injections just like that” [Participant Thirteen– Female, 21-29, Moderately Inactive, Severe Uncontrolled Asthma].
Participants also reported having appointments cancelled and were now facing long wait times to see specialists and reschedule appointments when protective measures had eased: “But he said, “Look I’ll put you erm I’ll refer you to a respiratory consultant, but it’s not happening until lockdown has been lifted”. So, a long time down the line. You are not seeing a respiratory consultant for probably he estimated probably about three to four months maybe before I’d get the opportunity to see one” [Participant One – Male, 31-39, Moderately Inactive, Severe Uncontrolled Asthma].
Discussion
The purpose of this study was to explore the effects of the social distancing and self-isolation measures taken in the UK on the wellbeing and physical activity levels of adults diagnosed with asthma. Using focus groups, we identified four key themes: ‘The Impact of Being Identified as Vulnerable or Not Vulnerable’; ‘Effects of Social Distancing and Self-Isolation on Physical Activity Levels’; ‘The Availability of Information and Guidance on Social Distancing and Self-Isolation with Asthma’; and ‘Looking Ahead and Returning to ‘Normal’.
Our findings suggest that being identified as vulnerable influences the illness perceptions of adults diagnosed with asthma, particularly if they did not identify themselves as vulnerable pre-pandemic. The Common-Sense Model proposes that illness perceptions can directly influence a person’s behaviours and coping strategies (Leventhal et al., 2016). In this instance, changes to their illness perceptions resulted in participants taking their asthma more seriously and becoming more health conscious. These results go beyond previous findings that personal vulnerability increased anxiety and concern about the potential impacts of COVID-19 to themselves and their families (Philip et al., 2020a, 2020b) and provided insight into how this patient group has acted in response to their increased vulnerability. These self-reported changes have created a unique opportunity for healthcare professionals to discuss self-management strategies with people living with asthma. Patients are maybe more open to self-managing their disease better compared to before the pandemic.
Social distancing and self-isolation had varying effects on physical activity. Evidence suggests that life-changing events can result in behaviour change and influence physical activity levels (Allender et al., 2008). It could be argued that the pandemic and the restrictions that have been put in place to reduce the transmission of the virus has been a life-changing event. It is likely that the additional discrepancy time and with physical activity being one of the exceptions for leaving the house, that people have used this time to be active (Smith et al., 2020). In our study, participants had more time to focus on their health, and some made an effort to become more active if a conscious effort had been made to improve their health, contradicting what was initially thought at the start of the pandemic about self-isolation increasing sedentary behaviours (Chen et al., 2020). Moving forward, it will be important to provide support and encouragement to the adults diagnosed with asthma who have made positive changes towards improving their physical activity to ensure progress is not lost over the course of the COVID-19 pandemic.
On the other hand, our study found that concerns regarding the adverse effects of physical activity on asthma symptoms increased reluctancy to be active. Concurrent with previous thoughts (Charlesworth et al., 2020), participants feared being exposed to COVID-19 while accessing health care and treatment and were therefore apprehensive about anything that could have adverse effects on their asthma symptoms. Changing their fear of infection would likely be a difficult task, but healthcare professionals could carefully monitor those who have not had contact with healthcare as expected to ensure that they are receiving the health care and treatment that they need.
Lack of opportunity was another factor that negatively affected physical activity levels during the pandemic. The COM-B (Capability, Opportunity, Motivation and Behaviour) Model argues that for someone to engage in a particular behaviour, they need to have the opportunity to do so (Michie et al., 2011). Congruent with previous findings (West and Michie, 2020), this lack of opportunity negatively influenced participants’ motivation to be active, but our study participants perceived a lack of motivation rather than lack of opportunity. It is important that healthcare professionals emphasise that behaviour change is not just about motivation, but also lack of opportunity and capability, and there is a need to be kind to oneself during challenging times.
In agreement with previous research (Finset et al., 2020), our findings suggest that improvements could have been made to the information and guidance provided about COVID-19 during the initial stages of the pandemic. Everyone identified as vulnerable, including people diagnosed with asthma, had been grouped as one, and no tailored advice had been given in regard to specific conditions, which led to confusion and concern. It is important that as scientists and healthcare professionals learn more about COVID-19, that up-to-date, accurate, consistent, and tailored information and guidance is being published. Tailoring needs to be clear so that people can see what easily applies to them, and so they are not distracted by content that is not relevant to them (Michie et al., 2020). Although there was a lack of information and guidance during the initial stages of the pandemic, improving healthcare communication can help to reduce people’s uncertainty and fear about returning to ‘normal’ life and adapt to changes in restrictions over time. It is important to note that younger adults prefer information through social media, whereas older adults are generally informed by television news reports and newspapers (Finset et al., 2020). Moving forward, this should be taken into consideration to ensure the reach and accessibility of information and guidance.
Strengths and limitations
This study has a number of strengths. To our knowledge, this is the first in-depth qualitative study to gain a unique understanding of the views and experiences of adults diagnosed with asthma during the COVID-19. This study provided valuable information on how this population group can be supported during this and future pandemics. In addition, using online video-conferencing, participants could be recruited from all over the UK, while national lockdown measures were in place.
This study has several limitations that should be noted. The high proportion of females within the sample suggests that this group is overrepresented. However, asthma is more prevalent and severe in female adults (Zein and Erzurum, 2015) which could help to explain why the sample was made up mostly of females. In addition, due to participants registering their own interest in taking part in the study, participants may have been more engaged with their asthma than the average person. Also, participants were required to have access to the internet so the findings may not be generalisable to the whole population.
Conclusion and further research
This study explored the effects of the social distancing and self-isolation measures taken in the UK on the wellbeing and physical activity levels of adults diagnosed with asthma. Our findings showed that participants became more health conscious as a result of being identified as vulnerable. They started to take their asthma more seriously and made positive changes to increase their physical activity levels. Physical activity levels were negatively affected if participants were concerned about the adverse effects on their asthma symptoms or if they had a lack of opportunity to be active. Although not all countries used the highly protective measures seen in the UK, the findings are transferable to vulnerable groups following any form of social distancing or self-isolation measures, including those who advised ‘protective self-separation’.
Identifying and exploring the impact of social distancing and self-isolation on adults with asthma is critical to gaining an understanding of how best to support this patient group during this pandemic and future pandemics. Our findings showed the unique opportunity that healthcare professionals now have to discuss self-management strategies with patients who perceive their asthma as a more serious condition compared to pre-pandemic times. They also highlighted the need for up-to-date, accurate, consistent and tailored information and guidance about COVID-19 to reduce uncertainty and fear about the disease.
When conducting this current study, we aimed to explore the effects of social distancing and self-isolation on adults diagnosed with asthma, specifically looking at how the pandemic had influenced their physical activity levels. Future research should aim to explore further some of the key themes identified in our study. We found that adults diagnosed with asthma had started to take their asthma more seriously and become more health conscious, but besides increasing activity, we do not know the specific changes that have been made as a result of this. For example, has adherence to asthma medication improved. It is important that we continue to examine the views of this patient group in uncertain and challenging times.
Research Data
sj-pdf-1-hpq-10.1177_13591053211012766 – The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study
sj-pdf-1-hpq-10.1177_13591053211012766 for The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study by Leanne Tyson, Wendy Hardeman, Gareth Stratton, Andrew M Wilson and Joanna Semlyen in Journal of Health Psychology
Research Data
sj-docx-2-hpq-10.1177_13591053211012766 – The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study
sj-docx-2-hpq-10.1177_13591053211012766 for The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study by Leanne Tyson, Wendy Hardeman, Gareth Stratton, Andrew M Wilson and Joanna Semlyen in Journal of Health Psychology
Research Data
sj-docx-3-hpq-10.1177_13591053211012766 – The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study
sj-docx-3-hpq-10.1177_13591053211012766 for The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study by Leanne Tyson, Wendy Hardeman, Gareth Stratton, Andrew M Wilson and Joanna Semlyen in Journal of Health Psychology
Research Data
sj-docx-4-hpq-10.1177_13591053211012766 – The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study
sj-docx-4-hpq-10.1177_13591053211012766 for The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study by Leanne Tyson, Wendy Hardeman, Gareth Stratton, Andrew M Wilson and Joanna Semlyen in Journal of Health Psychology
Research Data
sj-docx-5-hpq-10.1177_13591053211012766 – The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study
sj-docx-5-hpq-10.1177_13591053211012766 for The effects of social distancing and self-isolation during the COVID-19 pandemic on adults diagnosed with asthma: A qualitative study by Leanne Tyson, Wendy Hardeman, Gareth Stratton, Andrew M Wilson and Joanna Semlyen in Journal of Health Psychology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was conducted as part of the author Leanne Tyson’s PhD project, which has been funded by Asthma UK Centre for Applied Research and the University of East Anglia Faculty of Medicine and Health Sciences [Reference Number: 10025744].
Data sharing statement
The current article includes the anonymised transcripts of the focus groups conducted in this study. Pending acceptance for publication, all of the data files will be automatically uploaded to the Figshare repository.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.