
Abstract
The purpose of this study was to explore the experiences of Druze women who were diagnosed with breast cancer. Semi-structured interviews were conducted with nine Druze women. Inductive thematic analysis was used to analyze the data and three themes were generated. The first was “cancer discourse”: participants utilized codeswitching and medical jargon in their rhetoric, in a manner that seemed to imply difficulty to speak directly about their experiences. The second was “self-image”: the cancer and its treatments seem to have had an impact on participants’ body image and overall sense of femininity. The third was “coping”: sense and meaning-making as well as faith and family were identified as major coping mechanisms. Findings suggest a need for cultural competence in psychological interventions for breast cancer survivors.
Background
Every year nearly 4000 women are diagnosed with breast cancer in Israel, making it the most common malignancy among women (Zidan et al., 2017). Research indicates that cancer rates among the Druze, a relatively understudied ethnic minority making up 7.7% of the Arab Israeli population and 1.6% of the general population in Israel, are lower compared to those among Jewish and Arab Israelis (Atzmon et al., 2017; Central Bureau of Statistics, 2019). Despite these findings, the reasons for these lower cancer rates remain unclear. To date, most studies in the field have focused on screening rates as a major determining factor in cancer rate trends in the general Arab population in Israel, including the Druze. Research in the field, focusing on Arab Israeli women in general, indicated lower screening rates compared to Jewish Israeli women, although tests are offered free to all women over 50 by all health insurance programs (Baron-Epel, 2010). These studies found that lower screening rates are significantly associated with higher sociocultural barriers (Cohen, 2014). Lower screening rates among Arab Israeli women have been found to be linked to social and accessibility barriers, such as a lack of resources, unfamiliarity with the spoken language, low exposure to health communications, distrust of Western biomedicine, and a fatalistic view of illness (Azaiza and Cohen, 2006; Freund et al., 2019). These findings indicate that sociocultural factors and perceptions of breast cancer could act as barriers to early detection and health promotion.
In Israel, most research exploring perceptions of breast cancer has focused primarily on Jewish and Muslim-Arab women. Only a handful of studies examined the perceptions, and indeed the experiences, of Druze women with breast cancer, and generally did not distinguish between Arab and Druze women (Cohen, 2014; Goldblatt et al., 2013). While Druze scripture emphasizes an egalitarian view of women and men, patriarchy persists in most Druze communities in Israel (Barakat et al., 2018; Zeedan and Luce, 2021). A limited mix of older and recent research indicates that adherence to traditional gender roles could inform the way Druze women and men perceive health and illness and even affect cultural perceptions of breast cancer (Cohen, 2014; Gershfeld-Litvin et al., 2023). One study found that differences in stigma related to breast cancer held by Druze women and men may stem from their relatively moderate religiosity. Women who described themselves as moderately religious were more open to biomedicine than deeply religious women were (Gershfeld-Litvin et al., 2023).
Sociocultural factors have long been of interest to researchers in the fields of medicine and psychology (Lehman et al., 2017). In Arab countries, cancer is viewed as a stigma that affects one’s life, and women with breast cancer resort to concealment of their disfigured body to avoid being treated negatively by society (Assaf et al., 2017). In recent years, several studies have examined the role of social stigma in influencing early detection of and coping with breast cancer across the Middle East (Assaf et al., 2017; Gershfeld-Litvin et al., 2023; Melhem et al., 2023). Arab women were found to express fear that their husbands would leave them if they were no longer fertile or sexually attractive, posing a perceived threat to family integrity (Melhem et al., 2023). It is common for Arab women, who are aware of a family history of breast cancer, to assume this will hinder their likelihood to marry or have children, and thus to engage in self-blame, indicating internalized stigma (Melhem et al., 2023).
This study employs a qualitative approach to explore the perceptions and experiences of Druze women, with the aim of bridging this gap and offering new insights that might inform better standards of care and interventions tailored to their needs. The present study consisted of semi-structured interviews with Druze women who had been diagnosed with breast cancer to develop an understanding of their perceptions and the meanings they ascribe to their experiences.
Methods
Study design
This is a qualitative phenomenological research study with semi-structured interviews. Qualitative phenomenological research seeks to describe the meanings several individuals ascribe to their lived experiences of a concept or a phenomenon (Creswell and Poth, 2016). In collective Arab communities across countries, women may especially have difficulties openly sharing experiences and verbally expressing distress (Hebi et al., 2022). Qualitative methodology and semi-structured interviews were specifically chosen to explore the experiences and perceptions of Druze women with breast cancer, as they are well-established in research and commonly used for the purpose of understanding lived experiences and the meanings they evoke (Walliman, 2021). The Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong et al., 2007) was used to ensure the study was comprehensively reported.
Participants and recruitment
Participants were recruited through purposive sampling. Advertisements were posted on internet forums and Facebook groups, whose members were breast cancer patients, with administrator approval. Women were invited to directly reach out to the research team. Candidates were provided with information regarding the study when they first made contact via email or phone, as soon as their compatibility with the inclusion criteria was ascertained. The criteria were: (1) Druze Israeli women; (2) who were 18 years of age or older; and (3) had been diagnosed with breast cancer.
Nine women, ranging in age from 35 to 70 and meeting the inclusion criteria, were recruited (see Table 1 for details). The interviews, conducted in Arabic, spanned from 30 to 90 minutes, with an average duration of 60 minutes. To ensure anonymity, identifying details were redacted from the transcripts, and all study materials were securely saved with password protection to maintain confidentiality. Quotes were translated into English by the third author, a native speaker of Arabic who is proficient in English, and approved by the first author, who is proficient in English, and the second author, a native speaker of English.
Participant characteristics (n = 9).
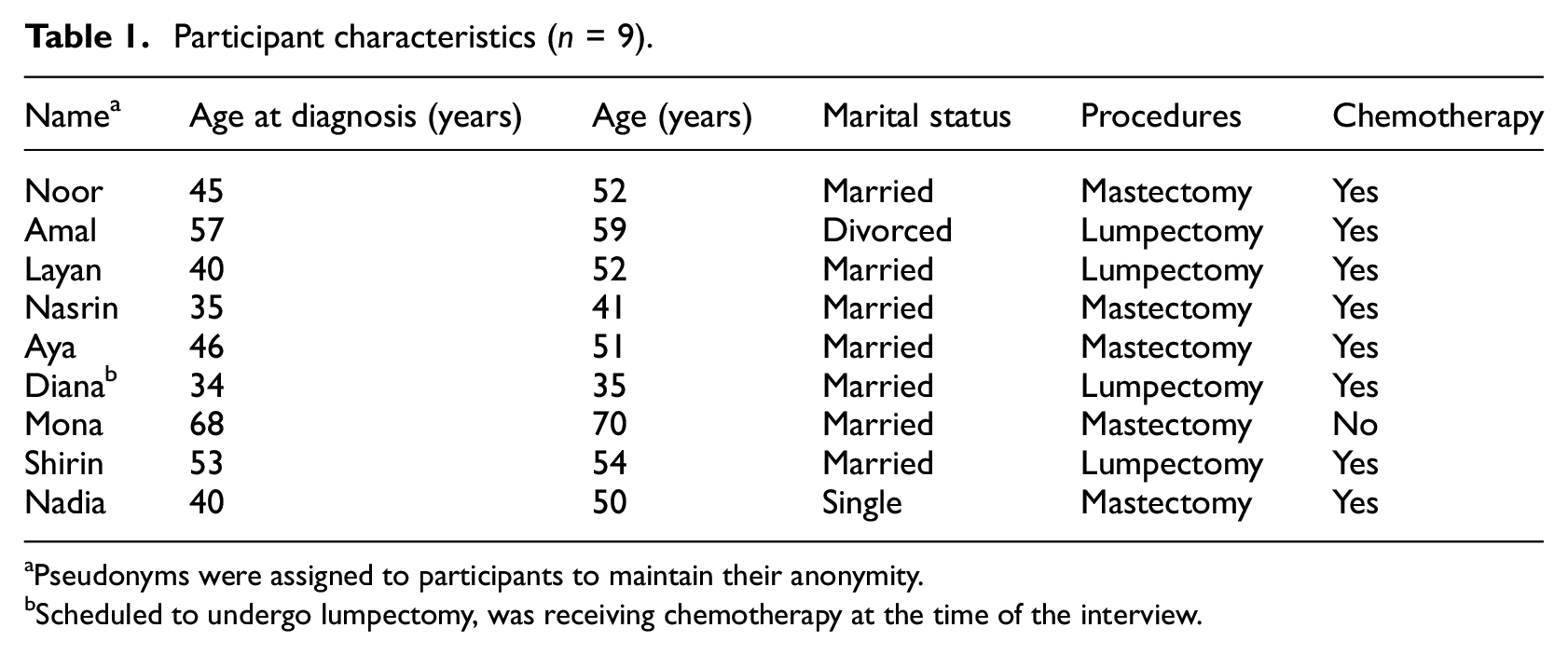
Pseudonyms were assigned to participants to maintain their anonymity.
Scheduled to undergo lumpectomy, was receiving chemotherapy at the time of the interview.
Data collection
Participants were interviewed in Arabic by the third author, a psychologist of Druze origin and a native speaker of Arabic who has extensive experience with interviewing (gained through academic and professional training). The interviews were semi-structured, held face-to-face, and took place between June and September of 2021 (see Table 2 for interview guide). Interviews were digitally recorded and later transcribed verbatim by the third author. Transcripts were translated into English by the third author (a native speaker of Arabic who is proficient in English and Hebrew) and approved by the first author (a native speaker of Hebrew who is proficient in English) and by the second author (a native speaker of English and Hebrew). The translation of all transcripts was conducted under the supervision of the fourth author (a native speaker of Arabic who is proficient in English and Hebrew).
The interview guide.
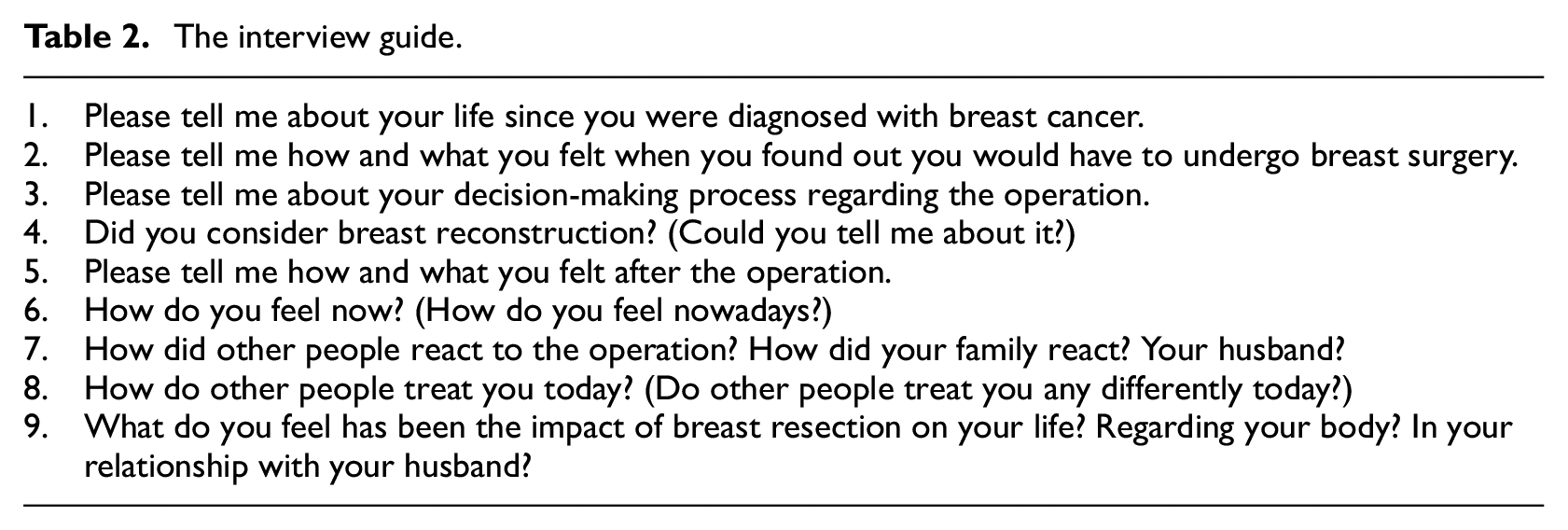
A general opening question was used in the beginning of each interview: “Please tell me about your life since you were diagnosed with breast cancer.” Subsequent questions consisted of follow-up, exploratory, and open-ended questions, including: “Please tell me how and what you felt when you found out you would have to undergo breast surgery.”; “Please tell me how and what you felt after the operation.”; “How did other people react to the operation?”; and “What do you feel has been the impact of breast surgery on your life?”
In the data collected and the quotes presented henceforth, remarks made in Hebrew were italicized to differentiate between Arabic and Hebrew. Additional information regarding interviewee intent is presented in brackets. Denotations for overlaps and pauses are presented in block letters in parentheses.
Data analysis
Data analysis was performed by the first three authors under the supervision of the fourth author, using Braun and Clarke’s (2019) method for reflexive thematic analysis. It is a well-documented method for analysis of qualitative data. This method lends structure to the analysis, as it consists of six duplicable steps: (1) becoming familiar with the data; (2) generating codes; (3) generating themes; (4) reviewing themes; (5) defining and naming themes; and (6) locating exemplars. However, its depth is not solely derived from the framework it provides, but rather emanates from the notion that a theme captures an important facet of the data in a manner that primarily focuses on generating meaning, irrespective of whether the theme represents a common element or the prevailing experience (Braun and Clarke, 2019).
The interviews were conducted and transcribed by the third author, a native speaker of Arabic with full proficiency in English. Following this stage, all authors thoroughly reviewed the transcripts and familiarized themselves with their contents. Initial codes were generated from each transcript. These codes were then grouped into higher categories based on shared conceptual domains. These were then synthesized into themes. Throughout this process, the team engaged in reflection on their research experience, carefully reviewing the outcomes generated. The aim of this was to foster a nuanced interpretation of the data. The outcome is a report of themes and sub-themes, theme descriptions, and extracts representing each of the sub-themes.
Researcher reflexivity
To increase the rigor of the outcomes, the principles of trustworthiness such as credibility, conformability, transferability, and dependability were considered (Lincoln and Guba, 1985). The most critical consideration was that of the researchers’ preconceptions, backgrounds, beliefs, and experiences. The research team has experience in the field of medical psychology, including with the subject of breast cancer. The first, second, and third authors have worked directly with patients coping with breast cancer in hospital settings in their capacity as psychologists. The researchers also have extensive experience in collecting and interpreting qualitative data; experience gained through conducting multiple qualitative studies in their field. The third author openly shared these facts with the participants at the start of each interview. Throughout this process, the team reflected on their research experience, engaging in discussions geared toward refining the outcomes, where the authors provided feedback and reviewed the outcomes.
Ethical considerations
Ethical approval was granted by the Institutional Review Board of The Academic College of Tel Aviv-Yaffo, reference number: 2021110. Written informed consent was obtained from all participants.
Results
Three themes were generated: “cancer discourse,” “self-image,” and “coping.”
First theme: “Cancer discourse”
The sub-themes of “cancer discourse” were “codeswitching” and “medical jargon.” Throughout their interviews, participants were asked to share details pertaining to both their physical and emotional experiences of coping with cancer. Their rhetoric suggested that their ability to speak directly about their experiences and disease was inhibited. Two phenomena were observed.
Codeswitching
Most participants were fluent in both Arabic and Hebrew and felt comfortable speaking in either language. In fact, it was quite common for participants to transition from Arabic to Hebrew during the interview. The switching occurred mostly for single words and two or three-word phrases, and seldom for complete sentences. While the practice of switching between Arabic and Hebrew is a common and natural occurrence for bilingual Druze Israelis, it was intriguing to observe the precise moments when these switches took place.
One participant described the aftermath of her resection surgery: “I found things were very difficult, I took a nifrad (separate) room from my husband … I just felt I needed to be alone.” ]Noor]. This participant consistently used the Hebrew word for “separate” to articulate her memory of the emotional experience of the period following her breast surgery. Making the decision to sleep apart from her husband marked a significant departure from her usual routine, yet it was congruent with the notion that she herself had undergone a profound change.
Another example can be seen in the following account, by another participant: “Giliti et zeh (I discovered it) alone, at home. My daughter had just given birth to her baby, it must have been a month or so in between, and then giliti et zeh (I discovered it) in my breast.” [Aya]. The juxtaposition of the recollection of her initial suspicions with her memory of her daughter’s childbirth potentially symbolizes the intense emotional significance attached to both memories. It appears that conveying emotional aspects symbolic of their experiences, in Arabic, posed a greater challenge for participants, prompting them to switch to Hebrew.
Medical jargon
Participants also displayed a distinct codeswitching pattern whenever they employed medical terminology directly associated with their personal experiences. For example: “I was unable to walk. I couldn’t do anything on my own. The rof’ah (doctor) sent me to the hospital, where they said I had grurot (metastases) in my atzamot (bones).” [Layan]. Another participant shared: “I didn’t want a kritah mele’ah (mastectomy) because they were going to do a shikhzur (reconstruction), and then an operation where they take from your belly area. But I didn’t like it. Praise Allah, it passed with just a kritah khelkit (lumpectomy).” (Shirin). This was also evident in the following account: “My oncolog (oncologist) said only kritah (mastectomy). My goosh (mass) is ah’lim (aggressive).” [Amal]. While one might have assumed that this codeswitching pattern could be attributed to a dearth of equivalent terms in Arabic, it is worth noting that all these medical terms are present in both Hebrew and Arabic.
Second theme: “Self-image”
The sub-themes of “self-image” were “body image” and “femininity.” Most participants underwent surgical treatment for cancer, which involved either a partial or complete mastectomy. Furthermore, as a preventive measure, most participants received chemotherapy, radiation therapy, or both. These treatments seem to have had a profound impact on their body image, thereby significantly reshaping their overall sense of femininity and self.
Body image
The perceived psychological and physical effects of cancer treatments varied among participants. In response to a question about how she felt regarding hair loss, a participant replied: “My hair was long, and I told myself it would just be better to cut it off than to have it fall out in front of my children … I gave it away because there were people who could use it for wigs. It would help them. So why not?” [Noor]. She realized that while hair loss could not be prevented, it was not lost in vain and could serve a purpose. She discussed her experience of hair loss in terms of the function it could still serve, rather than describing the emotional impact it had on her.
Another participant shared the following account: “I think that throughout this experience of cancer, the hardest part wasn’t losing my head hair, but rather losing the eyelashes and eyebrows. You start to look very ill.” [Amal]. Once her eyelashes and eyebrows were gone, she believed she would be seen and identified as a cancer patient by other people, which filled her with both anxiety and grief.
Another effect on body image can be observed in the following account: “It’s true that it isn’t very comfortable, everyone wants to be perfect. But I keep saying that the change hasn’t affected me that much. It doesn’t bother me at all. At first it did. I think I took it in a normal way.” [Layan]. While she presently does not feel bothered by it, she conveyed that her body was perfect before the surgery but no longer is.
Femininity
The physical experience of cancer as well as changes in body image have had an impact on the participants’ sense of femininity. One of the participants described her experience after breast surgery: “For what is a woman without the most beautiful part of her body? Without her breast?. … Even now, whenever I shower, I look at myself and I am not like other women.” [Noor]. The hardest part of the experience was losing a part of herself that she identified with femininity.
Another participant shared the following account: “Before I started chemotherapy, I bought a wig, though I was hopeful that my hair would not fall out. … Whenever I told my husband that my hair was falling out, he would just treat me as usual, like I was normal. But it constantly bothered me.” [Nasrin]. The participant in question purchased a wig in anticipation of potential hair loss. This action, along with her frustration with her husband’s insistence on treating her “as usual,” seems to imply that she perceived hair loss as a symbol of abnormality, thereby representing a deviation from societal expectations of femininity.
Third theme: “Coping”
The sub-themes of “coping” were “causality,” “faith, spirituality, and existentialism,” and “family.” Participants actively sought to make sense of their illness. While some found solace in faith as the sole explanation, perceiving their illness as a predetermined fate, others shouldered the burden of personal responsibility, believing they were somehow accountable for their illness. Meanwhile, there were also those who focused on the broader implications, particularly the potential effects on their children and the possibility of death.
Causality
Participants frequently pondered the question “Why did I get sick?” They shared their assumptions regarding the underlying causes. One explanation was that the cancer was a test from Allah (God), divine intervention. This mostly resonated with deeply religious participants. One participant provided insight on the meaning of cancer as she sees it: “As a woman, it’s normal to feel certain changes throughout life. It seems to me that you are insinuating that the breast is a particularly sensitive topic, because it’s what defines a woman. But breast cancer is what Allah had planned for me, so I accept it. The Druze, we have our faith, and that’s it.” [Mona]. An antithetical view was given predominately by secular participants; they held themselves personally responsible for their getting sick. For example: “I felt as if my body had given me this warning sign, a bright red light. ‘Be careful! You are hurting yourself! You are putting too much pressure on yourself!’.” [Diana]. Another account was that cancer provided an opportunity for discovery or rediscovery. As one participant shared: “Let me tell you something that I have also told my family. This is probably the best thing to have come out of this illness. I found that I have people who have my back … and now I don’t take that for granted.” [Aya].
Faith, spirituality, and existentialism
It became apparent that the diagnosis sparked reflections on life and death, demonstrating the significant role of faith and spirituality in sense-making and meaning-making processes. One participant shared her experience of receiving the diagnosis from her doctor: “You know, my cousin also had cancer, in the blood, and he died very young. We were quite close. Now, the doctor is talking to me about the process, but my thoughts are racing. I’m sitting here and all I can think about is my cousin.” [Nasrin]. Another participant recounted: “All sorts of ideas came to mind. I looked at my children … I thought to myself, I might not even live long enough to see the coming summer. Just imagined the worst of thoughts.” [Diana].
While the faith-based notion of life and death being predestined provided an explanatory framework for the presence of cancer among participants, faith also emerged as a prominent coping mechanism. A question regarding breast cancer elicited connotations of fear, which Mona was adamant were unsubstantiated for she trusted in Allah to shepherd her through this experience. “I am telling you that I have faith. I am not scared of anything. Neither this nor other diseases. Other diseases don’t scare me any more than this one does. Allah drew our path, and we must accept it.”
Another participant talked about her feelings post-surgery: “My morale is high, praise be to Allah …. Of course, it’s not easy. I expected I would only need surgery and be able to rest. But they came back with chemotherapy. I was a little annoyed, but look where faith gets you, it makes you stronger.” [Shirin]. Drawing strength from faith, participants found they were able to conquer fears associated with cancer and thereby alleviate the potential toll the treatments might have had on their self-image. When Nadia was asked about her current physical condition, she responded: “I rely on Allah, I am still strong, I didn’t change, praise be to Allah ….”
Family
The extent to which participants felt supported by their family had a profound impact on how they dealt with their illness. Relatives often served as a valuable source of emotional support. As one participant described: “You know how people around you are nice when times are hard? Well, I didn’t expect the support I got. I felt such support that I even found myself enjoying these hardships. I was able to see and look at the bright side of it all.” [Aya]. Family was also depended upon for practical support: “Praise Allah for my mother-in-law, my sisters-in-law, and my cousins. They were all there, they didn’t leave us. My mother-in-law would come and help me bathe. Some days I couldn’t even shower on my own” [Noor].
However, there were instances where participants felt they could not rely on their relatives for either type of support. As one participant shared: “One must be strong to get through it. The people around me are weak. In my family, they are all very sensitive. I needed to show them I was strong, so they wouldn’t have to suffer.” [Amal]. The perceived availability of support appears to have played a pivotal role in determining whether participants sought it out. Furthermore, the extent of support received by participants seemed to be contingent upon their willingness and ability to embrace it when available or offered.
Discussion
This study explored the psychological experiences of Druze women in Israel with breast cancer. Thematic analysis generated themes that closely coincide with the existing literature on self-image and coping, underscoring their integral role in the experiences of women with breast cancer. The current findings also provide novel insights into the ways in which Druze women communicate about their illness.
Participants experienced disturbances in self-image that appear to be rooted in fractures in body image and femininity. They expressed a deep sense of loss due to the impact of the cancer treatments and felt that it was primarily because they appeared ill and were easily recognizable as “cancer patients.” These findings align with existing literature on women’s experiences of coping with breast cancer. Across cultures, femininity is closely associated with the concept of an idealized body, encompassing symbolic representations like the nurturing breast, flowing hair, and a harmonious amalgam of physical attributes that epitomize femininity (Alhusban, 2019). Women undergoing cancer treatments that involve breast surgery experience a profound sense of loss over their once healthy, feminized, and socially sexualized breast (Hungr et al., 2017; Martins Faria et al., 2021; Przezdziecki et al., 2013). Attempts to cope with this sense of loss often involved greater observation of and reliance on faith.
Faith was observed as being both a resource for sense and meaning-making and as a means to cope with the challenges of breast cancer. Several studies, conducted in Arab countries, also highlight the role of religion and faith in defining the experiences of women with breast cancer. Adherents to Islam are encouraged to interpret breast cancer as a divine test of faith, a view that is not unique to Arab societies and can also be found in other non-Arab religious groups (Alhusban, 2019; Fearon et al., 2020). Cancer patients often grapple with religious and spiritual concerns that emerge with existential uncertainty about their future. Many survivors have found that their faith helped them accept the diagnosis and provided comfort, with religion serving as a source of strength throughout their experience (Aamir et al., 2022). Studies conducted in Saudi Arabia and the United Arab Emirates show that Islamic beliefs play a significant role in how Arab women make sense of their diagnosis of breast cancer. Arab women often accept their diagnosis as part of fulfilling their deep commitment to obey the will of Allah (Aamir et al., 2022; Almegewly et al., 2019).
We believe that the present findings indicate that faith holds similar roles for Druze women. Participants heavily relied on their faith both as a coping mechanism and as the basis for sense and meaning-making processes. As they confronted the challenges posed by their illness, participants actively engaged in sense-making, seeking to understand its underlying causes. For most, the illness was perceived as an act of divine intervention, either as a consequence of their own perceived lack of faith or as a divine test of their spiritual resolve. Thus, faith also played a significant role in shaping the process of meaning-making. A predominant belief in the notion of predestined life and death cultivated the understanding that cancer, its treatments, and cure, all rested solely in the hands of the divine, consequently emboldening women’s faith in the divine and offering them solace.
The use of codeswitching and medical jargon was prevalent among participants. In general, Arabic-Hebrew codeswitching is not an uncommon phenomenon among the Druze in Israel (Isleem, 2016; Rosenhouse and Brand, 2015), but its occurrence within the context of illness narratives seems to have not been observed nor interpreted. In fact, very few qualitative studies have been done in Arabic, particularly in medical contexts (Almegewly and Alsoraihi, 2022). The use of codeswitching can reflect several meanings. First, limited vocabulary in the primary language. This is unlikely since many of the medical terms the participants used in Hebrew also exist in Arabic; for example, the Hebrew word for cancer, sartan ( ), has an equivalent in Arabic, saratan (
), has an equivalent in Arabic, saratan ( ) (Ismail, 2017). The second, adhering to linguistic and cultural conventions, could be explained by findings from past research on the association between language and cultural identification within Druze society in Israel. The majority of Druze in Israel consider themselves to be culturally Arab and regard the Arabic language as their primary medium of expression (Isleem, 2016). However, the incorporation of Hebrew signifies a strong identification with Hebrew-Israeli culture. In fact, a considerable proportion of Druze demonstrate excellent proficiency and fluency in Hebrew (Isleem, 2016). Thus, the use of Hebrew words in regular speech could be construed as representing a cultural convention.
) (Ismail, 2017). The second, adhering to linguistic and cultural conventions, could be explained by findings from past research on the association between language and cultural identification within Druze society in Israel. The majority of Druze in Israel consider themselves to be culturally Arab and regard the Arabic language as their primary medium of expression (Isleem, 2016). However, the incorporation of Hebrew signifies a strong identification with Hebrew-Israeli culture. In fact, a considerable proportion of Druze demonstrate excellent proficiency and fluency in Hebrew (Isleem, 2016). Thus, the use of Hebrew words in regular speech could be construed as representing a cultural convention.
The third type of usage, emotional distancing, appears to have been prevalent among participants, as they switched to Hebrew to describe memories of medical treatments or other significant experiences, such as the moment of diagnosis. A careful analysis of the transcripts uncovered consistent language switches among participants, though not uniformly across all transcripts. For instance, while one participant might opt for Hebrew to describe a breast lumpectomy, another would maintain Arabic for the same procedure, but then switch to Hebrew when recounting the moment of her diagnosis. Previous research has found that bilingual speakers differentially code-switch between languages during emotional episodes (Williams et al., 2020). This could imply an emotional and linguistic association, possibly as a means of creating emotional distance from the intensity of the events. In the psychotherapeutic setting, women may find considerable benefits through a narrative approach. An effort to engage in the process of naming and framing their experiences, in their own language and words, could foster an environment where a deeper emotional connection and a more personal narrative may develop. These observations warrant further exploration in research.
Study limitations
The sample comprised a total of only nine participants. Although qualitative research does not aim for generalizability, it is important to acknowledge the limited scope of this study. Another aspect to consider is the variation in the time that elapsed between participants’ diagnosis and their involvement in the study. While the diversity in timelines allows for a broader range of perspectives, it also calls for caution when interpreting the narratives. In addition, the time-limited nature of this study may restrict one’s ability to fully capture the changeability of the experiences. Future research could address these aspects by expanding sample size and considering a longitudinal design, to allow for an even more in-depth exploration of the experiences.
Clinical implications
The present study suggests that the experiences of Druze women with breast cancer share similarities with the experiences of Arab women and women in general with breast cancer, particularly in terms of the potential impact of breast cancer, and its treatments, on self-image. The current findings highlight the dominant roles of faith and specific mediums of expression in the experiences of Druze women with breast cancer. These aspects suggest that therapeutic settings may benefit from culturally-competent therapists (Williams et al., 2020; Wood, 2019). More research is needed to explore ways to culturally inform psychotherapeutic training and practice for the benefit of therapists and patients.
Footnotes
Author contributions
All authors participated in planning and designing the study. KD conducted the interviews. AGL, IR, and KD conducted the main analysis of the data, supervised by SH. AGL and IR drafted the first draft of the manuscript. All authors revised the manuscript critically and approved the final version of the manuscript.
Data sharing statement
The current article has relevant raw data generated during the study, including the complete database or other relevant raw data. These files are available and accessible as Supplemental Material via the Sage Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing. The data files from the current study are also available in the Figshare repository at ![]() .
.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Authority of The Academic College of Tel Aviv-Yaffo under a research grant.
Ethics approval
Ethical approval was granted by the Institutional Review Board of The Academic College of Tel Aviv-Yaffo (reference no. 2021110).
Informed consent
Informed consent was obtained in both written and oral forms from all participants in the study.