
Abstract
The objective of this study was to explore stigma related to breast cancer among Druze women and men and identify factors associated with low screening rates among Druze women. A sample of 270 Druze women and men completed an online questionnaire adapted to detect breast cancer stigma and internalized breast cancer stigma. Independent samples t-test results showed higher scores for men compared to women, at a significant level, on four of the Breast Cancer Stigma scales: awkwardness, avoidance, policy opposition, and personal responsibility. Independent samples t-test results also showed higher scores for men compared to women, at a significant level, on two of the Internalized Breast Cancer Stigma scales: stereotype endorsement and discrimination experience. These results suggest a need for psychoeducation about breast cancer screening for minority groups such as the Druze, with male partners of women who are diagnosed with breast cancer being the main target recipients.
Introduction
Breast cancer is the most common form of cancer in women around the world. It accounts for 25% of all types of cancer diagnosed per year and is also among the leading causes of death in women (Bray et al., 2018; Fitzmaurice et al., 2015). In Israel, some 4000 new cases of breast cancer are diagnosed annually (Zidan et al., 2017). Despite being relatively lower, compared to the Jewish majority, breast cancer rates among the Arab Israeli minority have also been increasing since the 1980s (Zidan et al., 2017). Early detection of breast cancer through clinical breast examination (CBE) has been shown to decrease mortality (Azaiza and Cohen, 2006). Survival rates among Arab women are significantly lower, which is generally attributed to diagnosis at a later stage, possibly reflecting lower use of early detection screening. Data also indicate lower mammography exam rates among Arab women, compared to Jewish women, even though tests are offered free of charge to all women over 50, by all health insurance programs in Israel (Baron-Epel, 2010; Cohen and Azaiza, 2005).
Lower screening rates have been found in association with sociodemographic and cultural factors, such as lack of resources, unfamiliarity with the spoken language, less exposure to health communications, distrust of Western medicine, and a fatalistic view of health and illness (Azaiza and Cohen, 2006). Research suggests that religiosity may also play a role in illness perception and, by extension, in attitudes toward screening. According to past findings, the more religious women are, the more they believe that getting sick and receiving a diagnosis are matters of fate (“God’s will”), incidents that they have no control over (Azaiza and Cohen, 2006). A belief that one has no control over their health could deter women from engaging in screening and early detection mechanisms, as they may construe their own participation as a futile attempt to intervene in matters of fate.
Research has also indicated that group membership may affect the physical health of individuals. Members of minority ethnic groups may experience worse physical health compared to members from advantaged majority groups (Dovidio et al., 2016). One potential significant social factor may be cultural differences that prevent members of specific ethnic minority groups from undergoing specific medical procedures. Research conducted with Muslim women has found, for example, that stigma related considerations as well as religious factors, played a crucial role in women’s decision to undergo medical tests related to pregnancy (Ben Natan et al., 2016).
With respect to cancer, research has revealed that cancer stigma can present a barrier to treatment and lead to social isolation, as patients are “outed” and avoided by friends and loved ones (Else-Quest and Jackson, 2014; Lebel and Devins, 2008). Accordingly, in the present study, we were interested in exploring stigma related factors that may affect social and self-perceptions of breast cancer, for it may pave the way to understanding barriers to breast cancer screening, as indicated in previous research in other populations and medical conditions.
To our knowledge, this study is among very few to have investigated this minority group. Research on breast cancer incidence in Israel, and indeed on perceptions regarding breast cancer, has mostly focused on Jewish and Arab Israeli communities. The current study adds to the literature by specifically focusing on the Druze community, a unique under-researched, ethnic, religious, and tradition-oriented minority in Israel. Adopting a culture-centered approach (Dutta, 2008), the aim of the present study was to explore stigma related to breast cancer among Druze women and men.
Breast cancer among the Druze
The Druze are an ethnic minority constituting 7.7% of Arab Israelis and 1.6% (140,000) of the general population of Israel (9 million). Druze communities are characterized by a relatively young population (the median age is 27.5). The marital age is also relatively lower than that of the Jewish and Christian populations (men—27.7; women—23) (Central Bureau of Statistics, 2018). Druze communities are generally characterized by low socioeconomic status, ranking third to fourth out of 10, on a scale rating the entire population of Israel (Central Bureau of Statistics, 2018). Nearly 2% of all students attending higher education institutions in Israel are Druze (Central Bureau of Statistics, 2018) in line with the number of Druze in the general population.
Limited information is available regarding breast cancer morbidity among the Druze. Data published by the Israeli Cancer Association indicate that relative to Jewish and Arab Israelis, cancer rates among Druze men and women are lower (Atzmon et al., 2017). Specific data for breast cancer show that rates among Jewish women are twice as high as among Druze women. Among Muslim Arab women, breast cancer rates are 33.3% higher than among Druze women (Atzmon et al., 2017).
Past research has suggested the Druze diet, consisting mainly of non-processed foods, as one possible explanation for the difference in breast cancer incidence between Druze women and women from other ethnic groups (Azaiza and Cohen, 2006). It has also been suggested that higher morbidity rates stem from low adherence to routine screening for breast cancer among the Arab population in general, including the Druze (Baron-Epel, 2010; Cohen and Azaiza, 2005). Low participation in screening may hinder early detection, leading to late or no detection, which could lead to higher morbidity in these communities (Baron-Epel, 2010; Cohen and Azaiza, 2005).
Differences in screening rates could be affected by cultural perceptions held by Druze women regarding barriers to conducting early detection tests, such as fear and stigma (Cohen, 2014; Remennick, 2006). Research has shown that a significant barrier to performing a mammography is that the procedure itself may cause embarrassment, especially for Druze and Muslim women; these groups reported high social restrains and highly valued modesty (Azaiza and Cohen, 2006).
In a review conducted several years ago, a total of 20 studies were found to have explored attitudes and behaviors regarding mammography screening, almost all of which focused on Muslim Arab Israelis (Cohen, 2014). Studies that specifically explore attitudes and behaviors toward breast cancer screening among minority women within the Arab Israeli population are even rarer. A small group of Druze women was included in one study, which focused on psychological aspects of coping with breast cancer but did not explore stigma related to breast cancer nor barriers to breast cancer screening participation (Cohen et al., 2011). The present study focuses solely on Druze women and men. The aim was to explore stigma related to breast cancer, which has previously been found in association with relatively low breast cancer screening participation among Druze women.
Methods
Participants and procedure
This study constitutes a preliminary quantitative study preceding a qualitative study for which ethical approval was received from the Ethical Review Board of the academic institution with which it is affiliated in June 2021. The aim of the current study was to discover stigma related to breast cancer among men and women in the general Druze community. It pre-dates a qualitative study that focuses on the population of Druze women who have been diagnosed with breast cancer, exploring their subjective experiences. Since the scopes of these studies were quite different from one another, it was deemed appropriate to conduct them separately.
The eligibility criteria included women and men aged 18 or older who belong to the Druze population. Since the Druze community is traditionally patriarchal (Barakat et al., 2018; Zeedan and Luce, 2021), to explore whether there are differences between Druze women and men, it seemed important to compare the incidence and levels of stigma between the groups. If Druze men were found to hold stigma on breast cancer, in the context of a patriarchal society, this could explain, to some extent, why early detection rates are relatively low for women. The assumption is that in a more tradition-based community such as that of the Druze, women adhere to their partners’ opinions and decisions.
Participants were 270 Druze individuals (188 women and 82 men). An additional 37 respondents were excluded due to missing information, which made it impossible to verify these individuals met the inclusion criteria (age, for example). Research questions were integrated on a survey platform. Advertisements were posted on social media platforms (Facebook and Instagram) with a direct link to the research survey. Participants had given informed consent by signing a form integrated on the platform, prior to survey completion.
Instruments
Both questionnaires used in this study had been translated into Arabic by two native Arabic speaking translators of Druze origin. Demographic details were collected and included age, sex, place of living, level of education, perceived socioeconomic status, social status, and level of religiosity. In addition, participants were asked whether they have ever been diagnosed with breast cancer and whether they knew anyone in their close social circles who has been diagnosed with breast cancer.
To assess stigma related to breast cancer, five scales were adapted and amended from the Cancer Stigma Scale (Marlow and Wardle, 2014), which included awkwardness, severity, avoidance, policy opposition, and personal responsibility (see Appendix A). The new scale was renamed Breast Cancer Stigma Scale. The word “cancer” was replaced with “breast cancer” in all relevant items. Internal reliability (Cronbach’s α) was calculated and was recorded for the adapted scale, as follows: for awkwardness 0.80, for severity 0.85, for avoidance 0.91, for policy opposition 0.71, and for personal responsibility 0.79.
An adaptation of the original Internalized Stigma of Mental Illness Scale (ISMI; Ritsher et al., 2003) was used to assess stigma regarding breast cancer and breast cancer patients. In both its original and adapted versions, participants are asked to denote how much they agree or disagree with each statement assessing potential stigma experienced by people with an illness. Accordingly, our interest was in exploring both male and female participants’ stigma regarding breast cancer patients. Such stigma might affect important domains which are related to coping mechanisms with the disease (in women) and might be related to provision of social and emotional support (by male partners, for example).
The use of scales from different domains to assess cancer stigma is not uncommon (see Daryaafzoon et al., 2020; Taft et al., 2014). The ISMI has also been adapted in past studies where stigma regarding other diseases was assessed. In one study, researchers modified the ISMI specifically for irritable bowel syndrome (IBS). The modified version assessed the degree to which participants believed or internalized stigmatizing attitudes about IBS. The researchers replaced “mental illness” with “IBS” or “irritable bowel syndrome.” They cited several studies where the ISMI was used, all demonstrating good reliability and validity, including when modified for other medical populations (Taft et al., 2014). The ISMI was chosen for the current study as it provides a comprehensive spectrum of stigma perceptions, including self-stigma, public stigma, professional stigma, and institutional stigma (Boyd et al., 2014).
Three scales were adapted and amended from the ISMI scale to form the Internalized Breast Cancer Stigma scales for use in this study: alienation, stereotype endorsement, and discrimination experience (based on Ritsher et al., 2003; see Appendix B). The phrase “mental illness” was replaced with “breast cancer” in all relevant items. Each item on these scales is rated on a four-point Likert-type scale (1—strongly disagree; 4—strongly agree). Internal reliability (Cronbach’s α) for the adapted scales was 0.86 for alienation, 0.83 for stereotype endorsement, and 0.85 for discrimination experience.
Statistical Methods
Demographic data were analyzed using descriptive statistics as well as a one-way ANOVA to test for differences between men and women. 1 For stigma related to breast cancer, an independent t-test was used, testing for differences between men and women. For internalized stigma related to breast cancer, an independent t-test was used as well. In addition, a one-way ANOVA was performed to examine the relationship between level of education and internalized stigma about breast cancer. A probability level of 0.05 was accepted as significant. Levels of significance are presented in the results section where applicable.
Results
Demographics
Participants were women and men of Druze origin, ranging in age from 18 to 54 years. A one-way ANOVA was performed on the demographic data and revealed no significant differences between women and men in the following characteristics: age, socioeconomic status, social status, and religiosity (see Table 1). A separate breakdown of differences between men and women in breakdown is also provided (see Table 2). Two of the participants had a diagnosis of breast cancer.
Demographic characteristics of Druze women and men. a .
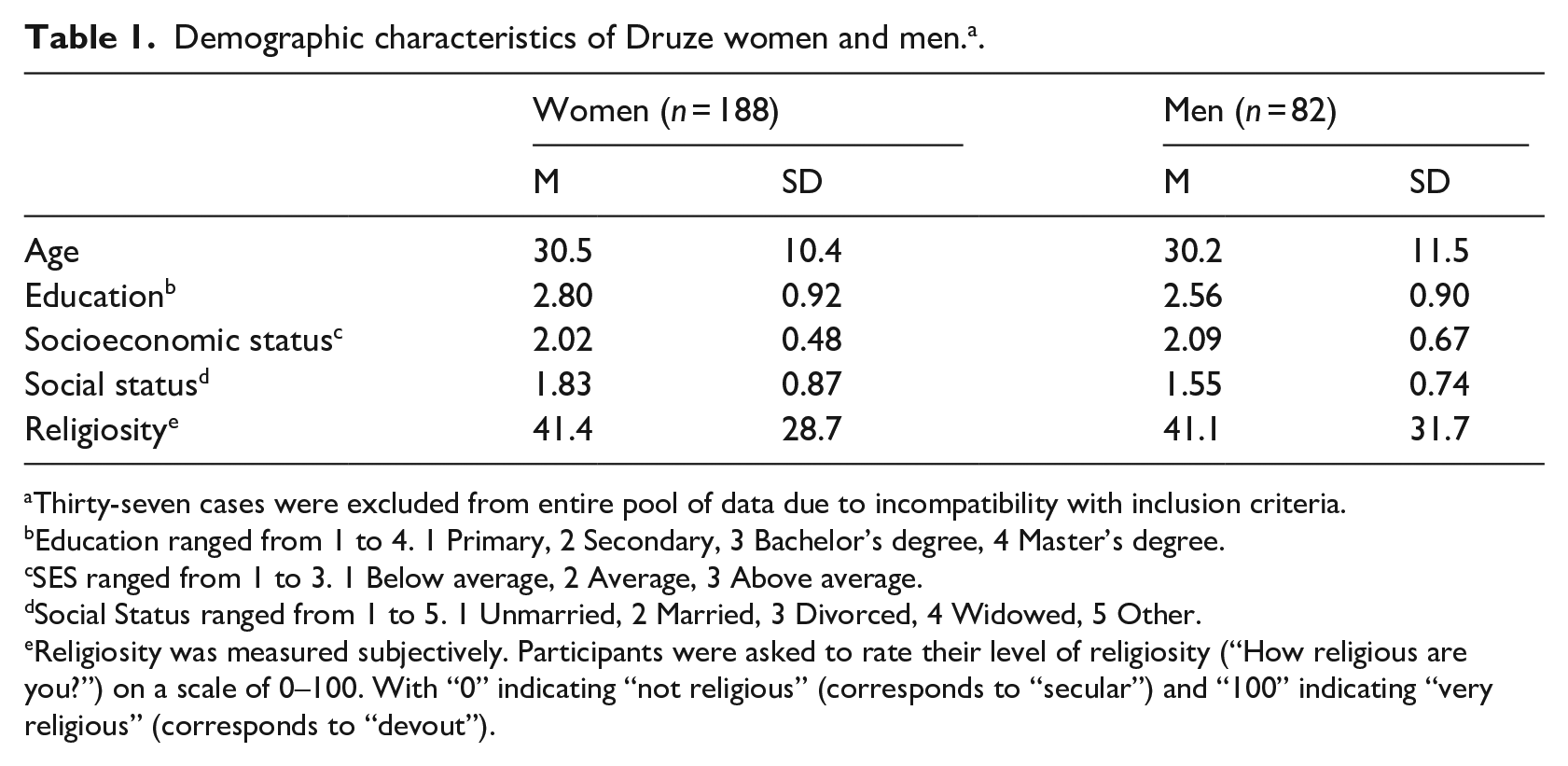
Thirty-seven cases were excluded from entire pool of data due to incompatibility with inclusion criteria.
Education ranged from 1 to 4. 1 Primary, 2 Secondary, 3 Bachelor’s degree, 4 Master’s degree.
SES ranged from 1 to 3. 1 Below average, 2 Average, 3 Above average.
Social Status ranged from 1 to 5. 1 Unmarried, 2 Married, 3 Divorced, 4 Widowed, 5 Other.
Religiosity was measured subjectively. Participants were asked to rate their level of religiosity (“How religious are you?”) on a scale of 0–100. With “0” indicating “not religious” (corresponds to “secular”) and “100” indicating “very religious” (corresponds to “devout”).
Comparing women and men by level of education.
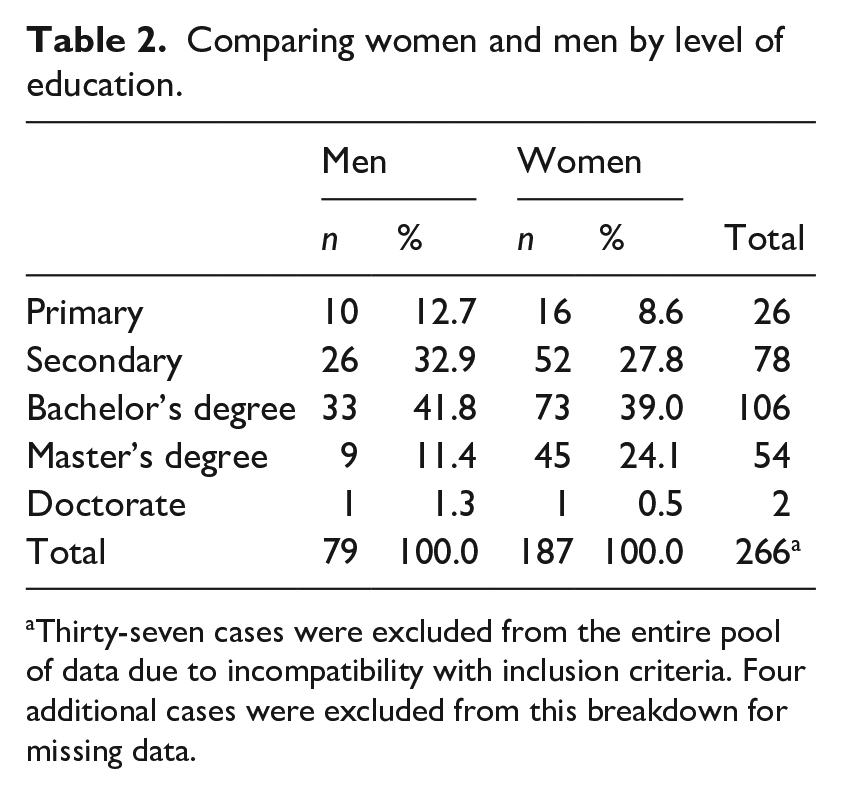
Thirty-seven cases were excluded from the entire pool of data due to incompatibility with inclusion criteria. Four additional cases were excluded from this breakdown for missing data.
Breast cancer stigma
An independent samples t-test was performed for the Breast Cancer Stigma scales, comparing between women and men. Levene’s test results for this analysis were significant for awkwardness, avoidance, policy opposition, and personal responsibility, p < 0.05. Since the homoscedasticity assumption was violated, we report results where equality of variances is not assumed. The analysis revealed significant differences between women and men on the following scales: awkwardness, t(95.0) = 3.08, p < 0.01; avoidance, t(83.5) = 2.98, p < 0.01; policy opposition, t(81.6) = 3.11, p < 0.01; and personal responsibility, t(87.2) = 3.02, p < 0.01. Men scored significantly higher than women on all the reported scales. Table 3 presents means and standard deviations for each of the scales.
Comparing women and men on breast cancer stigma scales. a .
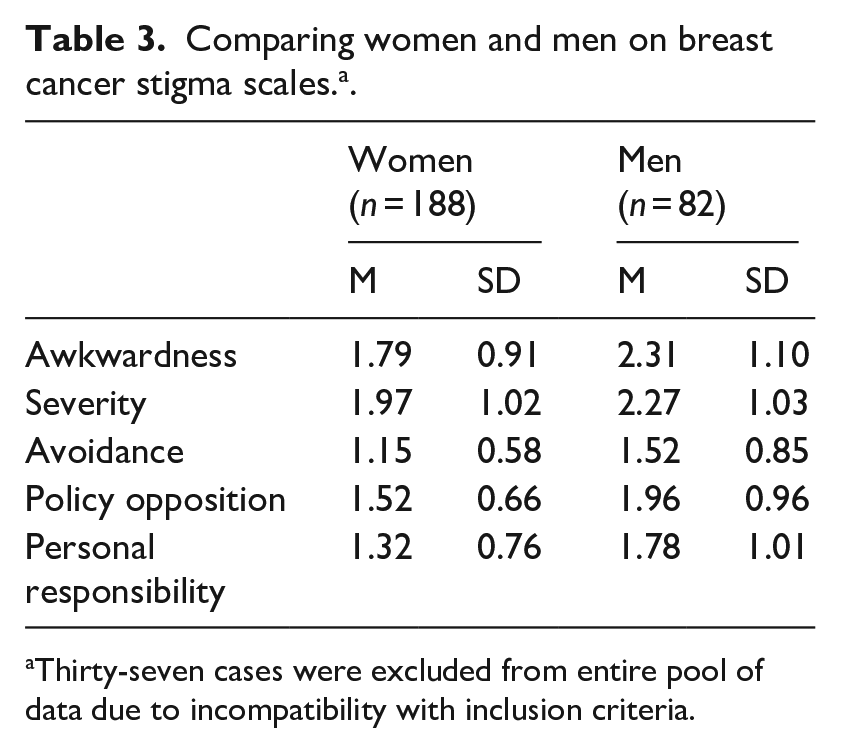
Thirty-seven cases were excluded from entire pool of data due to incompatibility with inclusion criteria.
Internalized breast cancer stigma
An independent samples t-test was performed for the Internalized Breast Cancer Stigma scales, comparing between women and men. Levene’s test result was significant for stereotype endorsement, p < 0.05. Since the homoscedasticity assumption was violated, we report the corrected result where equality of variances is not assumed. The analysis revealed significant differences between women and men in stereotype endorsement, t(90.1) = 2.93, p < 0.01. Levene’s test result for discrimination experience was not significant, p > 0.05. The analysis revealed a significant difference between women and men in discrimination experience, t(95.5) = 2.034, p < 0.05. Men scored significantly higher on both scales. Table 4 presents means and standard deviations for each of the scales.
Comparing women and men on internalized stigma scales. a .
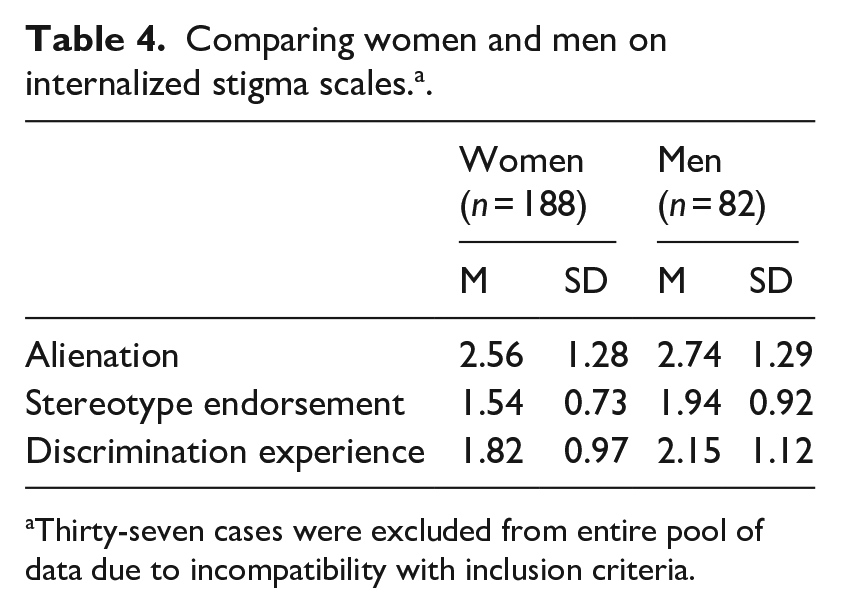
Thirty-seven cases were excluded from entire pool of data due to incompatibility with inclusion criteria.
A one-way ANOVA was also performed to examine associations between level of education and the stereotype endorsement and discrimination experience scales of the Internalized Breast Cancer Stigma scale. Levene’s test result was significant for stereotype endorsement, p < 0.05. Since the homoscedasticity assumption was violated, we conducted an additional Welch’s t-test. The result of Welch’s t-test was not significant for stereotype endorsement, p > 0.05. Levene’s test result was not significant for discrimination experience, p > 0.05. The analysis revealed a significant effect for level of education on the discrimination experience scale, F(3, 186) = 4.46, p < 0.01. Table 5 presents means and standard deviations for discrimination experience according to level of education.
Level of education on discrimination experience. a .
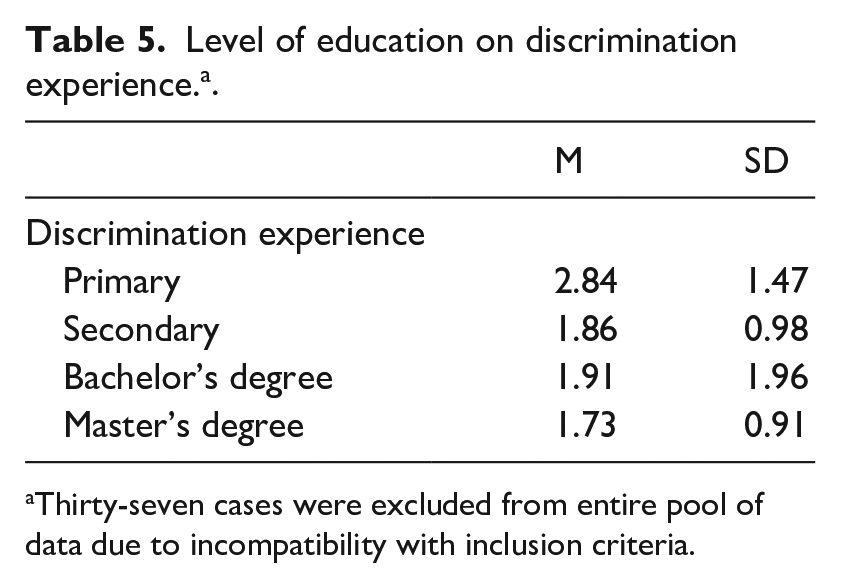
Thirty-seven cases were excluded from entire pool of data due to incompatibility with inclusion criteria.
Discussion
This research was designed to characterize stigma on breast cancer among Druze women and men, a relatively understudied minority group in Israel. There were no significant differences between women and men in factors such as age, level of education, socioeconomic status, social status, or religiosity. This indicates that any significant differences between women and men, found in other variables, most likely did not stem from sociodemographic factors. Druze men scored higher, to a significant level, on both breast cancer stigma and internalized breast cancer stigma scales. Internalized stigma ratings were found in association with level of education; higher ratings, indicating higher levels of stigma, correlated with lower levels of education.
Analyses revealed that Druze men had significantly higher ratings on several scales of the Breast Cancer Stigma questionnaire, when compared to women. A significant difference in the awkwardness scale indicates that Druze men would feel more uncomfortable being around or speaking about breast cancer with someone who has had breast cancer, compared to women. A significant difference in the avoidance scale indicates that Druze men would also more rather actively avoid interactions with people with breast cancer, compared to women. These findings combined suggest that feeling uncomfortable around people with breast cancer may beget avoidance of cancer altogether. Another significant difference was found in the policy opposition scale, implying that they believe that breast cancer should be a top priority for government policies or spending, but to a lesser extent than women do. It should be noted that while men may feel uncomfortable being around and talking about breast cancer, these results suggest that Druze men still believe that breast cancer should be given appropriate attention by officials. Ratings on the personal responsibility scale suggest that neither men nor women strongly believe that it is a person’s own fault if they have breast cancer, however, men significantly lean more toward that position than women do.
Previous research on the perceptions of Arab Israeli women on breast cancer revealed that Arab women tend to hide their disease, and indeed their coping experience, from others in their close social circles. This concealment has been attributed to a traditional view of gender roles in Arab society, as well as related feelings of shame and discomfort (Goldblatt et al., 2013, 2016). Little is known about these aspects when it comes to the Druze society. Past research did emphasize privacy from the outer world as an important pillar in the lives of the religious Druze (Yehya and Dutta, 2010).
It may be the case that subscription to more traditional gender roles in Druze society informs the way Druze men and women view health and illness. Recent research conducted in Saudi Arabia, a relatively traditional society, illustrated that husbands’ knowledge can have an impact on their wives’ attitudes and practices related to breast cancer screening methods (Sabgul et al., 2021). In communities characterized by traditional patriarchal gender roles, similarities in views held by women and men may originate from shared religious values or even arise from a woman’s deference to her husband.
Previous research has shown that the more religious women are, in Arab society, the more likely they are to avoid modern biomedicine and hold a belief that their condition is a matter of fate; this includes Druze women (Azaiza and Cohen, 2006; Yehya and Dutta, 2010). In the present study, differences in stigma related to breast cancer held by Druze women and men may stem from their relatively moderate religiosity all around. That is, women who described themselves as secular or moderately religious held a more progressive view of gender roles and may thus embrace biomedicine more willingly than deeply religious women would. More research is needed to explore the relationship between religiosity, gender roles, and stigma related to breast cancer screening.
Analyses revealed that level of education is associated with internalized breast cancer stigma. The sample consisted of women and men of mixed levels of education, though represented a relatively more educated group on average. Our findings suggest that Druze women and men do not generally internalize breast cancer stigma, such as: the view that people with breast cancer lack the ability to live a good life, make decisions independently, or contribute to society. However, less educated women and men are more likely to hold such stigma compared to the more educated. These findings imply that one’s level of education may indirectly present a barrier to early detection of breast cancer. This is in line with previous research on Arab women in Israel. Arab women, who are characterized by having acquired higher education, attended mammography and CBE screenings more, compared to less educated women (Azaiza et al., 2011). If a person has internalized stigma regarding breast cancer, they may be disinclined to participate in early screening or support others who wish to participate. These findings are novel, as previous research focused mainly on Muslim and Christian Arabs, not on the Druze.
The analysis also revealed that while Druze men and women do not generally internalize stigma regarding breast cancer, Druze men are more likely to internalize stigma related to breast cancer as well as a fear of being discriminated against, when compared to Druze women, to a significant level. In a relatively more traditional society such as that of the Druze (Azaiza and Cohen, 2006), where the views of the patriarch are often a deciding factor in health-related issues, this may be crucial for early detection of breast cancer. More research is needed to delineate the relationship between social norms and health beliefs in the Druze community, as it could shed more light on the specific influence of societal roles on health beliefs and behaviors.
This research found evidence of differences in stigma and internalized stigma between women and men, regarding breast cancer. These findings highlight the need for more education to raise awareness to breast cancer and breast cancer screening. They also emphasize the importance of targeted psychoeducation for male partners of women with breast cancer, focused on outlining the emotional and physical challenges involved in coping with cancer as well as on the importance of the support system. Interventions targeting Druze women directly to increase participation in breast cancer screening should focus on sociocultural factors (language-appropriateness and cultural sensitivity in communication) as well as on psychosocial factors (legitimacy and normalization) (see Donnelly and Hwang, 2015; Duffy et al., 2017; Meacham et al., 2016).
This study should be considered within the context of its limitations. The Druze are an under-researched, religious, and traditional minority in several countries in the region (mainly in Israel, Syria, and Lebanon) (Azaiza and Cohen, 2006; Yehya and Dutta, 2010). Living alongside one majority, being exposed to their stigma, may in turn influence minority stigma. Our research focused on the Druze minority in Israel, however, stigma among the Druze may differ in each of the countries mentioned above, as social norms may differ across countries. Future research should explore stigma held by Druze women and men in other countries where they are a minority.
Another limitation to the current study is its reliance on participant self-reports. It is unclear whether the responses of Druze women, who live in a relatively conservative society, reflected their actual perceptions and attitudes, or were shaped by self-presentational motivations to portray themselves and their group in a way that is more consistent with liberal trends regarding breast cancer. Future research should explore attitudes of Druze women more carefully using interviews, for example. It could provide important insight on the way Druze women cope with breast cancer.
The use of the Internalized Stigma of Mental Illness adapted to breast cancer may also be considered as a limitation of the study. Participants had to respond to statements that were adapted for breast cancer stigma but were not originally designed to detect it. While responses may shed light on stigma among participants, it cannot be considered a full replacement for scales primarily designed to detect internalized stigma related to breast cancer and responded to by people with breast cancer. However, it should be noted that the aim of the current study was to explore stigma in the general Druze community, not specifically among people with breast cancer. It may be beneficial to explore cancer stigma among people with breast cancer, for incidence and levels of stigma may differ between the groups.
Despite its limitations, this study demonstrates differences between Druze men and women in stigma and internalized stigma on breast cancer. When compared to women, Druze men were found more likely to hold and internalize stigma on breast cancer. Current findings imply that Druze men may feel awkward and engage in avoidant behavior toward people with breast cancer, more so than Druze women would. Although neither Druze men nor women seem to oppose policies that may contribute to developments in breast cancer research and treatment, this study found that Druze men are less adamant in their policy endorsement than Druze women. Druze men were demonstrated to internalize fear of discrimination and stereotype endorsement, in the context of breast cancer, to a greater extent than women. Overall, these findings suggest a need for future research to provide more information on Druze men, their health beliefs, and on the application of interventions targeting Druze men.
Research Data
sj-sav-1-hpq-10.1177_13591053221115619 – for Stigma related to breast cancer among women and men: The case of the Druze minority in Israel
sj-sav-1-hpq-10.1177_13591053221115619 for Stigma related to breast cancer among women and men: The case of the Druze minority in Israel by Avital Gershfeld-Litvin, Samer Halabi and Keith M Bellizzi in Journal of Health Psychology
Research Data
sj-spv-2-hpq-10.1177_13591053221115619 – for Stigma related to breast cancer among women and men: The case of the Druze minority in Israel
sj-spv-2-hpq-10.1177_13591053221115619 for Stigma related to breast cancer among women and men: The case of the Druze minority in Israel by Avital Gershfeld-Litvin, Samer Halabi and Keith M Bellizzi in Journal of Health Psychology
Footnotes
Appendix A
Appendix B
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Research Authority of The Academic College of Tel Aviv-Yaffo under a research grant awarded to the authors.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.