
Abstract
Moral distress denotes a negative reaction to a morally challenging situation. It has been associated with adverse outcomes for healthcare professionals, patients and healthcare institutions. We argue that existing definitions, along with measures of moral distress, compromise the validity of empirical research. First, the definition and measurement of moral distress conflate moral events and psychological distress, even though they are distinct phenomena that should be assessed independently. Second, in many studies, there is a lack of clarity in distinguishing between moral and non-moral events. Finally, prior research on moral distress often overlooks the substantial body of evidence demonstrating the impact of diverse work-related factors, beyond moral events, on both distress and job retention. These challenges might undermine the effectiveness of interventions aimed at alleviating moral distress. We outline a comprehensive research agenda that encompasses conceptual clarifications, the refinement of data collection instruments, the design of studies and the application of appropriate statistical methods.
Introduction
The concept of moral distress refers to negative physical and psychological reactions experienced by healthcare professionals. This phenomenon occurs when individuals are hindered from acting in alignment with their moral beliefs, often as a result of constraints or a feeling of powerlessness (Kolbe and de Melo-Martin, 2023; Morley et al., 2019; Ulrich et al., 2010). In essence, the idea of moral distress relies on the basic assumption that there is a causal link between (a) an event that elicits a moral response from an observer – hereafter referred to as a moral event – and (b) short-term psychological reactions, such as feelings of frustration, guilt and distress (Giannetta et al., 2020; Morley et al., 2022). Initial moral distress can then cause a wide range of longer-term psychological consequences, which may include burnout at an individual level, workplace attrition within institutions and a decline in the quality of care (Giannetta et al., 2020; Kolbe and de Melo-Martin, 2023; McCarthy and Monteverde, 2018; Sanderson et al., 2019). Initially described in nursing, moral distress has been shown to affect professionals across all healthcare disciplines (McCarthy, 2013; Riedel et al., 2022; Varcoe et al., 2012), prompting an extensive body of research since the term was coined by the philosopher Andrew Jameton (Jameton, 1984; Kolbe and de Melo-Martin, 2023).
Numerous empirical studies have underscored the burden of moral distress, yet extensive debate persists regarding the types of events classified as moral and leading to such distress. Building on Jameton’s conceptualization, many researchers have regarded illegitimate external constraints as a central feature of moral events leading to moral distress (Kolbe and de Melo-Martin, 2023; McCarthy, 2013). These constraints include regulations or an adverse institutional climate that forces healthcare professionals to act against their own moral beliefs, values or principles. For example, a supervisor may instruct a nurse to administer a medication to a patient at a dosage that raises potential safety concerns for the nurse. However, feeling pressured and unable to voice her concerns effectively due to a strong hierarchical culture, she administers the medication. This action leaves the nurse experiencing distress and guilt, accompanied by fears of having compromised the patient’s safety and her own professional integrity.
Following Andrew Jameton’s original conception, advocates of a narrow definition limit the occurrence of moral distress to scenarios where healthcare professionals know what needs to be done but are unable to act accordingly. This construal emphasizes the aspect of moral evaluation, where the individual’s judgment about what is right or wrong is informed by established ethical principles or standards. Conversely, proponents of a broader definition acknowledge the role of constraints in moral distress, while also encompassing a range of morally undesirable events, such as dilemmas, uncertainties or conflicts (Fourie, 2015; Lützén and Kvist, 2012). Therefore, this description of moral distress includes scenarios where healthcare professionals do not know what needs to be done. For example, a physician is torn between her professional duty to inform a patient about a terminal diagnosis and the family’s request to withhold this information. This situation places the physician in a moral conflict between her obligation to respect the family’s wishes and her obligation to be honest and trustworthy with the patient.
However, this broader definition and the corresponding debate seem to have contributed little to the conceptual clarification. Instead, moral distress is referred to as an ‘umbrella term’ that can represent many different situations and phenomena, complicating further empirical investigation (Hanna, 2004; McCarthy and Gastmans, 2015; Morley et al., 2019). Notably, Fourie (2017) and Morley et al. (2023) have advanced an approach that introduces subcategories of moral distress. According to this approach, there are various distinguishable types of moral distress. For example, moral-tension distress is described as psychological stress that arises when someone is ‘unable to share beliefs with others’ (Morley et al., 2023: 892). Nevertheless, while multiple conceptual frameworks for moral distress have emerged, the quantitative empirical literature predominantly adheres to Jameton’s original, narrow conception (Giannetta et al., 2020).
Given the reported widespread occurrence of moral distress and its associated adverse effects, it has been argued that researchers should look ‘beyond’ conceptual definitions (Amos and Epstein, 2022), focusing instead on interventions to prevent the incidence of moral distress or to limit its impact on healthcare workers and patients. However, the effectiveness of these interventions might be reduced because of several issues. These include conceptual ambiguities, variability in measurement methodologies and underlying assumptions that may not hold true. As a result, the findings of prior research might not give an accurate picture of what causes distress in clinical practice. On the one hand, if the narrow definition depicts the clinical reality – that moral distress is mainly caused by illegitimate constraints that hinder moral agency – then it seems necessary to first identify, name and analyse those constraints (cf. Monteverde, 2016). In institutions where healthcare professionals are limited by a rigid hierarchical structure that restricts their decision-making autonomy, ethics education may not suffice to mitigate their distress. On the other hand, if the broader definition of moral distress more accurately reflects the complexities of clinical settings, and more precisely identifies the sources of distress among healthcare professionals, then interventions ought to incorporate ethics education and readily accessible clinical ethics support services to enhance moral agency. In other words, if moral uncertainties, conflicts or dilemmas are relevant causes of distress, – for example, if professionals frequently encounter ethical dilemmas where they are unsure of the correct decision –, ethics education or support services may help healthcare professionals by providing guidance on ethical decision-making.
Accordingly, it seems that moral distress can be effectively mitigated and specifically addressed only by identifying the particular moral events that cause such distress. However, the question remains whether all occurrences of moral distress can and should be prevented. While the term distress denotes a negative stress response, moral distress can also be understood as an expression of the moral sensitivity of healthcare professionals, a trait that is considered indispensable in their field. Certain moral events are expected to elicit moral distress, signalling the need for attention to a specific aspect of the situation. Similarly, Lützén et al. (2003) differentiate ‘moral stress’, which they identify as an essential condition for ethical practice, from ‘moral distress’, which they view as a potential threat to the delivery of effective and compassionate care (cf., McCarthy and Monteverde, 2018). Thus, moral distress cannot or should not be prevented in every clinical situation (cf. Kolbe and de Melo-Martin, 2023), and professionals must learn to cope with it. Finally, some interventions, such as mindfulness training, might reduce stress even without a thorough understanding of the real causes of moral distress (Morley et al., 2021b).
Given the existing empirical research on moral distress, an additional challenge in identifying the causes of moral distress lies in the wide range of contextual factors, ‘triggers’ (Giannetta et al., 2020) or ‘compounding factors’ (Kolbe and de Melo-Martin, 2023; cf. Morley et al., 2022) that are thought to intensify or attenuate moral distress. For instance, as previously mentioned, healthcare professionals need moral sensitivity to recognize moral issues (Lützén and Kvist, 2012), which may lead to the experience of moral distress. Other individual factors include vulnerability to moral distress (Monteverde, 2019), moral motivation and commitment, conflicting responsibilities (Morley et al., 2022) and empathy or feeling close to the patient (McCarthy and Gastmans, 2015). Conversely, assertiveness (Oelhafen and Cignacco, 2020), moral courage or resilience may inhibit or mitigate the experience of moral distress, although Viens et al. (2020) suggested that moral distress may also impair resilience. At the institutional level, contextual factors such as poor team communication, hierarchical cultures and structural issues like low staffing levels are associated with moral distress (Giannetta et al., 2020; McCarthy, 2013). In summary, a wide range of factors labelled as ‘contextual’ at both the individual and institutional levels significantly complicate the understanding of the causes of moral distress.
Finally, there are smooth or fluid transitions between moral distress and distinct but related concepts. For instance, compassion fatigue or post-traumatic stress may be triggered by secondary trauma when healthcare professionals witness suffering (Varcoe et al., 2012). Moral distress has also been distinguished from stress of conscience, which can occur when people are prevented from doing the knowingly good or right action (Lützén and Kvist, 2012). Other reported consequences of prolonged exposure to moral distress include burnout, moral injury (Dean et al., 2019), moral residue (Lützén and Kvist, 2012) and moral failure (Morley et al., 2022), suggesting that these are related but conceptually distinct concepts. This overlap presents an issue because the ongoing debate regarding the ‘boundaries’ of moral distress and the lack of consensus hinder efforts to clearly differentiate moral distress from these related concepts, complicating both the understanding and the management of these phenomena within healthcare settings.
In summary, the extensive and heterogeneous body of existing empirical research, diverse definitions, methodologies and the variability of factors identified as ‘contextual’ complicate the conceptualization of moral distress. This complexity makes it challenging to define moral distress with empirical validity and to distinguish it clearly from related phenomena. While not suggesting that the concept should be abandoned (cf. Johnstone and Hutchinson, 2015), we argue that current conceptualizations of moral distress hinder valid empirical testing of the premise that the observed distress genuinely stems from moral events (of any nature) rather than other sources of distress. This difficulty arises because
(a) cause and effect are intertwined in the definition and measurement of moral distress (cf., Fourie, 2015),
(b) many studies do not address the fundamental question of how they differentiate between moral and non-moral events and subsequently fail to differentiate between moral and other causes of distress and
(c) studies on the long-term impacts of moral distress do not adequately consider non-moral distress as a possible confounder.
Consequently, these circumstances may result in an overestimation of the prevalence of moral distress and an underestimation of non-moral distress, both of which warrant equal attention. Finally, existing empirical evidence from the fields of industrial and organizational psychology and economics suggests that restrictions on work-related autonomy and social support can adversely impact job satisfaction, with long-term consequences similar to those attributed to moral distress.
The problem of intertwining cause and effect
Both broad and narrow definitions of moral distress conflate cause and effect (or aetiology and symptoms), hindering an empirically informed conceptualization of moral distress. While distinctly different from moral distress, definitions of mental disorders – for example, in the Diagnostic and Statistical Manual of Mental Disorders (DSM) – typically accommodate a wide range of possible biopsychosocial factors and causes, and the ongoing debate on which groups of symptoms should be considered a syndrome or a mental illness is informed by current evidence. By adopting an inductive approach, empirical researchers can investigate possible causal chains that lead to mental disorders. For instance, while individual symptoms of post-traumatic stress disorder (PTSD) may not be unique, it is the combination of its causes, such as direct exposure to life-threatening events, and its broad spectrum of symptoms – including intrusion, avoidance behaviours, altered mood, cognition and arousal – that distinguishes PTSD from other distress-related disorders. To this extent, the definitions of mental disorders are empirically informed, and specific causes should be identified only if they are recognized as triggers for symptoms or diseases.
While moral distress is not considered a mental disorder, the preceding explanations demonstrate how empirically informed definitions can include cause and effect. Instead, the debate around moral distress appears to reiterate untested assumptions. By way of illustration, consider two simplified models of factors causing moral distress (Figure 1). Both models encompass objective work conditions (such as the number of employees, structural circumstances, etc.) and more subjective psychosocial work environment factors (ethical climate, perceived work autonomy, etc.). In Panel A, moral distress is defined and operationalized as a singular concept, implying that the objective and subjective working conditions can only serve as ‘compounding factors’, as ‘triggers’ of moral distress. Importantly, given the model in Panel A, there is no possibility of assessing the impact of non-moral events on psychological distress. Conversely, in Panel B, moral events and the possibly resulting distress are operationalized independently. This approach allows for empirical examination of whether working conditions lead to more frequent moral events that subsequently result in moral distress, and/or whether the working conditions or work environment factors directly cause this distress independently of any moral events. As we will demonstrate later, current instruments assessing moral distress do not permit such differentiation. Consequently, since most empirical studies adopt the approach outlined in Panel A (cf., Giannetta et al., 2020; McCarthy, 2013), potential alternative causes – such as team communication problems and low levels of staffing – are labelled as contextual factors, triggers or compounding factors of moral distress a priori. However, empirical studies are needed to determine whether these contextual or compounding factors are direct causes of the observed distress.
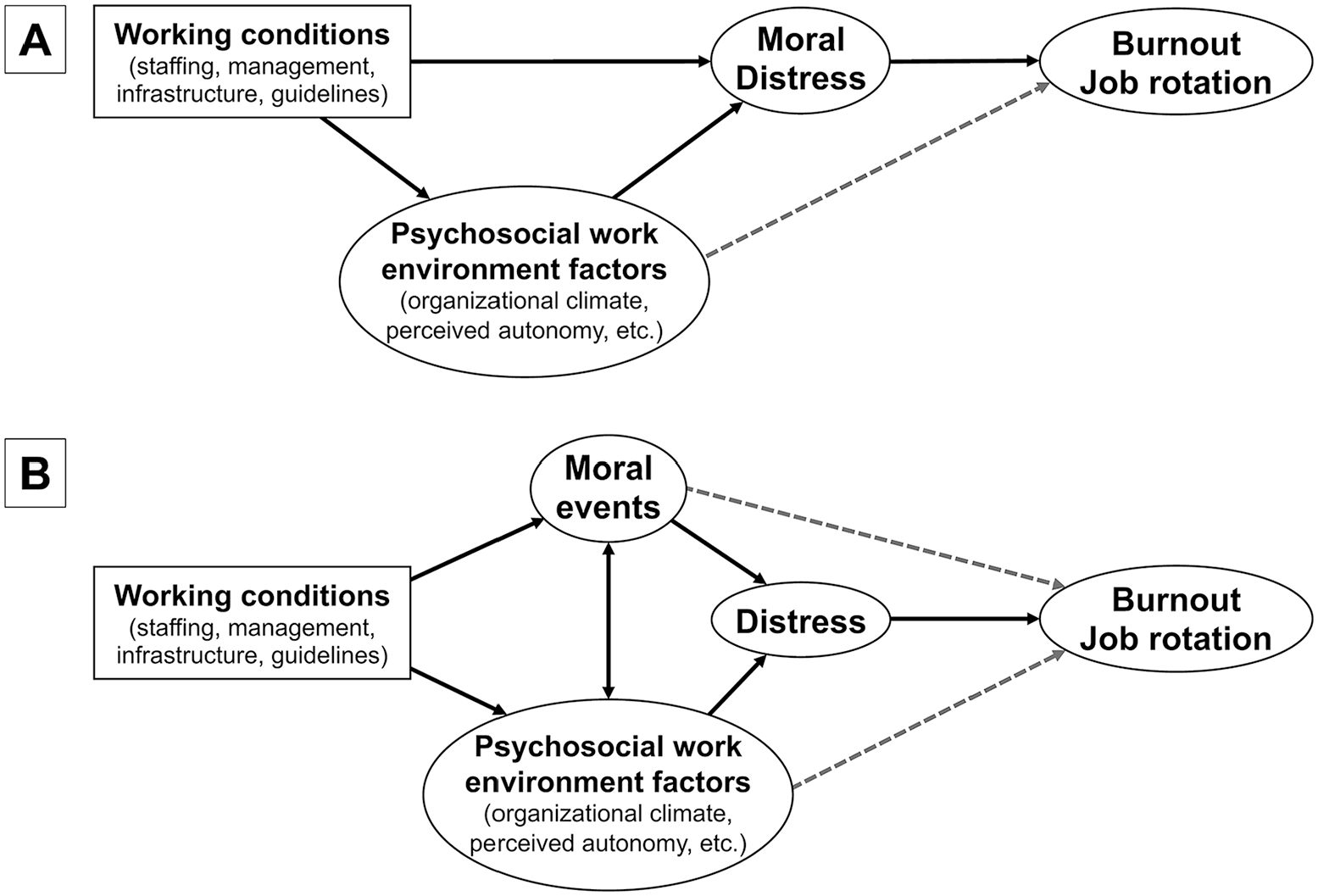
Two causal models illustrating the relationship between working conditions, (moral) distress and long-term negative consequences. These models either integrate moral events and distress into a single concept (A) or distinguish between them (B), enabling the examination of the extent to which working conditions and psychosocial factors cause distress. Both models are simplified for illustrative purposes, given that the influence of other individual and institutional factors is highly probable.
The problem of confounding moral and non-moral distress
Given that the concept of moral distress encompasses both cause and effect in its conceptualization and measurement, empirical research often insufficiently distinguishes between moral and non-moral distress. Thus, the prevalence of moral distress and its long-term consequences are likely to be overestimated, albeit to an unknown extent. As outlined above, moral distress is usually understood as a psychological reaction caused by a moral event. The emphasis on the term ‘distress’ draws attention to emotions and negative psychological consequences, thereby overlooking the critical question of which events or problems should be meaningfully labelled as ‘moral’. Indeed, the conceptual debate regarding ‘narrow’ or ‘broader’ definitions of moral distress should not revolve around the events that cause distress. Instead, it should focus on identifying what qualifies as moral events, irrespective of whether these events lead to distress. The question of the distress that these events may subsequently cause is an empirical matter. Therefore, establishing a conceptual distinction between moral and non-moral events is foundational for the empirical differentiation between moral distress and other forms of distress.
While one could argue that many situations have a moral component, especially in clinical settings, categorizing all types of events or issues as ‘moral’ blurs our conception of moral distress and hampers effective interventions for preventing both moral and non-moral distress (Lützén and Kvist, 2012). However, a potential objection to the context-independent classification of events as moral or non-moral might be that a situation becomes morally relevant only when perceived as morally relevant by an individual. However, this subjective evaluation alone cannot be deemed a sufficient condition. For instance, if a professional claims to experience moral distress due to an overwhelming workload, we would need to better understand whether this distress is genuinely rooted in moral concerns (e.g. compromised patient safety or quality of care), or if the distress is simply a consequence of the heavy workload itself. Therefore, some consensus on what constitutes a moral event is required.
Another related objection could be that no situation or action possesses inherent moral relevance. Drawing an abstract line between moral and non-moral events overlooks the individual’s judgment of what is deemed to be a morally relevant feature of the situation. For example, in a study by Oelhafen et al. (2019), some midwives reported finding late-term abortions distressing. Their distress was heightened when they were required to administer medication without being involved or informed about the decision-making process or without understanding the reasons behind the couple’s decision. Conversely, experienced midwives did not generally regard abortions as a moral issue. Therefore, we cannot assert that abortions have inherent moral features for all midwives under all circumstances.
Nonetheless, the abstraction and categorization of events is necessary to foster discussions regarding categories of moral issues and to facilitate empirical research. Reflecting on the previous example, we would certainly consider abortions if the aim were to understand which events midwives perceive as moral issues. This is particularly true for quantitative research that aims to measure the frequency and intensity of distress linked to categories of moral events and to establish causal inferences, although such inferences are limited in cross-sectional studies. As a result, in discussing certain categories of moral issues, we inevitably bypass the nuanced, individual context of a situation – a context which largely influences a professional’s evaluation of the moral relevance of a situation.
According to many scholars, any definition of ‘moral problems’ is based on a moral judgment or normative assumptions, thereby presenting a risk of circularity (Morris, 2004; Storchevoy, 2018). For instance, Morley et al. (2022) assert that moral events encompass phenomena such as ‘moral tension, moral conflict, moral dilemma, moral uncertainty or moral constraint’ (p. 1314). This reliance on the term ‘moral’ to define ‘moral events’ highlights the difficulty in demarcating moral from non-moral events. Zichy (2012) posits that moral problems are a distinct category that cannot be fully explained by referencing non-moral or extra-moral criteria. For example, while strong emotions, such as frustration or helplessness, may accompany moral problems, they cannot serve as definitive criteria to distinguish moral from non-moral issues. Consequently, clearly differentiating between moral and non-moral issues becomes challenging. Nevertheless, some important considerations can be made regarding this matter.
First, when a person perceives a situation as deficient in certain respects, and this deficiency is not easily remedied, this person perceives a problem.
Second, although moral problems are closely connected with empirical facts (Reiter-Theil and Mertz, 2012), they do not coincide with ‘purely’ empirical questions. In cases of uncertainty, we evaluate courses of action based on values, the potential and anticipated good or bad consequences for the patient. This involves normative or ethical evaluations that – in the clinical setting – require pausing, hesitating or deviating from routine. Consider, for instance, a scenario in which a team of healthcare professionals is faced with a terminally ill patient who is unable to communicate his or her preferences. While there are empirical facts that offer some clarity and guidance (such as the likelihood of recovery and the potential impact on the patient’s quality of life related to aggressive treatment), uncertainties persist. These uncertainties encompass aspects such as the patient’s unknown preferences and their current level of pain. This necessitates a careful balancing of various values and deviating from established routines, making the decision-making process far from straightforward.
Additionally, the social context reinforces or attenuates the experience of the individual. For instance, a moral problem is considerably more pronounced if a professional unilaterally assumes responsibility for the decision and potentially modifies ‘the life plan of another individual or group of individuals’ (Morris, 2004: 353). Conversely, when there is clear agreement between the healthcare professional and the patient, the moral problem tends to be less significant.
Third, the person experiencing a moral problem may be different from the person affected by that problem. Susewind and Hoelzl (2014), in agreement with Jones (1991), define actions that serve personal interests or are self-serving as non-moral (as opposed to morally relevant actions). Similarly, according to Storchevoy (2018), issues should only be considered moral in the narrow sense, that is, when they involve social interactions and the interdependence of individuals. For instance, a healthcare professional is involved in a decision that might affect a patient’s health or well-being. Given that the patient is primarily affected by the decision, it is unlikely that we would categorize this as the patient’s moral issue. Therefore, although both the professional and the patient are involved in the same situation and participate in the decision-making, the professional may perceive the situation as a moral problem, while the patient, being directly affected, is less likely to view the situation through a moral lens.
In conclusion, in analysing clinical situations, it might be useful to distinguish whether an individual is primarily affected by the moral dimension of a situation or whether it is their well-being, physical or mental health that is primarily affected. In one scenario, a healthcare professional may feel belittled by a supervisor’s comments. The professional does not need to make normative considerations or weigh different values to evaluate the situation. Primarily, this situation affects his well-being or mental health. In another scenario, if the supervisor instructs the healthcare professional not to treat a patient in the manner he believes is right, a moral dimension arises. In this case, even though the right course of action is known, the professional is unable to proceed according to his convictions and to proceed routinely, constituting a moral event for him. Both scenarios could be indicative of a hierarchically structured institutional culture. However, it cannot be determined a priori whether the well-being or mental health of a professional is primarily affected (as in Scenario 1), or whether they experience moral integrity violations (as in Scenario 2). These dimensions may independently dominate in a clinical setting or in a specific scenario, or they may co-occur.
To further illustrate the multifaceted sources of distress that may appear simultaneously in a clinical situation, consider again a scenario in which hierarchical decisions hinder healthcare professionals from providing treatment in alignment with their clinical judgment. First, the professionals may anticipate unnecessary suffering and, as caregivers, may feel (co-)responsible and guilty for causing avoidable suffering. Second, they might regard this decision degrading and a sign of a lack of recognition of their professional competences, regardless of the impact on the patient. In this case, it is the well-being of healthcare professionals that is primarily affected by the decisions of others (e.g. hospital administrators). Third, they may find themselves in a moral conflict, unsure of whether they should advocate more strongly for the patient and themselves. They face a choice between risking consequences in their professional relationships or complying, which could compromise their own integrity and potentially lead to patient suffering.
In summary, ‘moral-constraint distress’ (Fourie, 2015; Morley et al., 2021a) can be considered ‘narrow’ in comparison to other definitions. However, a clinical scenario that aligns with Jameton’s ‘narrow’ conceptualization of moral distress may involve both moral and non-moral sources of distress. We cannot understand which sources of distress are predominant unless we measure them separately. This does not suggest a clear demarcation between moral and non-moral stressors. However, it is important to recognize that these processes can occur independently. For example, healthcare professionals can empathize with a patient, even if, from their perspective, the patient is being treated correctly. Additionally, a professional might feel devalued, even if the decision made within the hierarchy does not pertain to a patient’s treatment but rather to the professional’s request for an unpaid leave. This co-occurrence of psychological processes and moral problems can also occur due to high workloads or inadequate staffing. The high workload can force professionals to prioritize treatments or care more than their standards would indicate. At the same time, they suffer from a high workload irrespective of whether patients are affected. If we adopt the conception that moral problems primarily modify ‘the life-plan’ of other individuals (Morris, 2004), then neither the personal devaluation resulting from hierarchical decisions nor the high workload faced by healthcare professionals should be considered prima facie moral issues.
Given these clinical examples and the complexity of the manifestation of emotions and distress, it might be too difficult for healthcare professionals to reliably differentiate moral as opposed to non-moral causes of their distress. For example, in the case of institutional constraints, it may be easier for healthcare professionals to attribute their frustration to compromised patient well-being rather than recognizing it as a response to their integrity being violated or as a result of feeling offended or degraded. Consequently, qualitative empirical approaches that capture the experience of moral problems from the perspective of healthcare professionals (e.g. Oelhafen et al., 2019) and thus the ‘subjective interpretation of real-life situations’ (Van Der Arend and Remmers-van Den Hurk, 1999: 471) cannot pretend to offer a clear conceptual distinction between moral and non-moral events and, correspondingly, between moral and non-moral forms of distress. It is important to note, however, that a conceptual distinction between moral and non-moral problems is not intended to discount or exclude any class of problems as irrelevant. There certainly are ‘ethical reasons … to value these experiences’ (Morley et al., 2021a), but it is not helpful to classify all negative experiences as moral issues.
The problem of failing to adequately assess the impact of non-moral distress
A third issue is that common instruments assessing moral distress often include ambiguous or double-barrelled questions that conflate moral issues related to patients with contextual factors, such as understaffing (e.g. ‘number of staff is so low’, ‘unsafe levels of nurse staffing’) and hierarchical pressures (e.g. ‘physician’s orders’, ‘pressures from administrators’, ‘feel pressured’) (Table 1). For example, working with other healthcare professionals ‘who are not as competent’ might be a consequence of understaffing or a general shortage of skilled professionals, leading to non-moral distress and long-term consequences. Importantly, this does not imply that these items fail to capture moral problems entirely; rather, they do not capture them in isolation. In conclusion, the limitations of these questionnaires make it difficult for researchers to ascertain if the assessed distress is solely attributable to moral events and to accurately evaluate the extent to which long-term consequences stem from non-moral versus moral distress.
Sample items from three scales assessing moral distress (cf. Kolbe and de Melo-Martin, 2023).
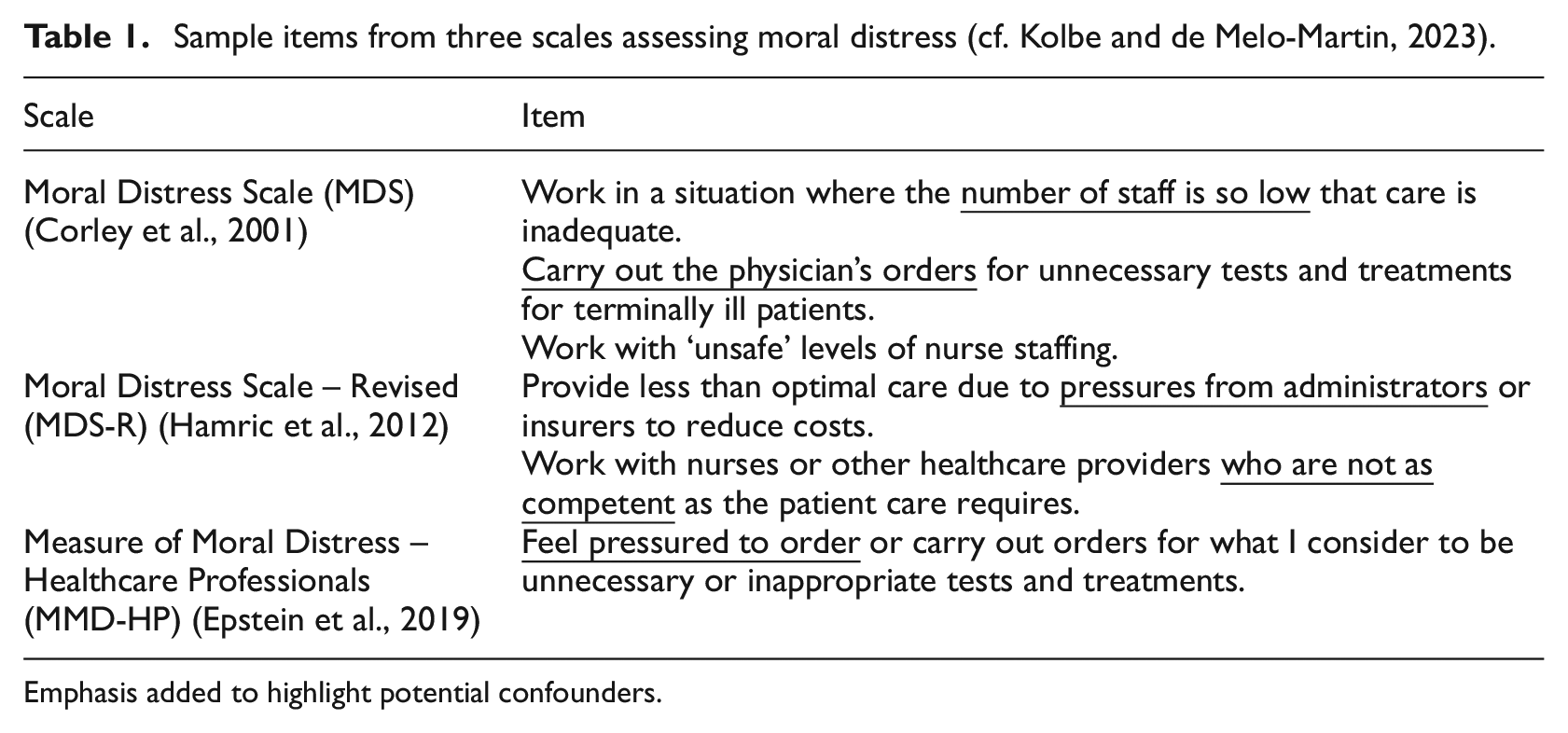
Emphasis added to highlight potential confounders.
In many studies, the disentanglement of the possible causes of distress and long-term negative consequences is further complicated by the measurement of total moral distress as the product of the frequency of distressing situations and the intensity of the associated distress (see Giannetta et al., 2020). This means that infrequent situations that cause high levels of distress are scored the same as more frequent situations that cause little distress. As the frequency of certain situations may be strongly correlated with setting and general workload, these factors could again be confounded by non-moral events. Alternately, the intensity of distress experienced may be related to individual factors (e.g. coping strategies). As shown in Figure 1, causal relationships can be better examined by dissecting the individual components of moral distress: the frequency of moral events experienced and their evaluation. Therefore, the conflation of frequency and intensity into total moral distress is questionable and further complicates our understanding of causal mechanisms.
Finally, a substantial body of research in industrial and organizational psychology, as well as in economics, offers an explanation for the observed association between ‘moral’ events and long-term negative consequences. For example, job demands–resources theory contends that the interactions between various job demands and resources predict employee well-being and burnout. Relevant demands include workload, emotional demands and work–life balance, any of which can trigger burnout or other negative outcomes. Relevant resources include autonomy or control, supervisor-related resources, feedback and recognition, all of which can increase motivation, job engagement and productivity (Rattrie et al., 2020; Schaufeli and Taris, 2014).
In a meta-analysis of 259 studies, work-related autonomy and social support were identified as the best predictors of job satisfaction, while low work-related autonomy predicted absenteeism, stress and burnout or exhaustion (Humphrey et al., 2007). In their systematic review, Suleiman-Martos et al. (2020) reported that low work-related autonomy was associated with understaffing and limited resources. Work-related autonomy, which allows workers to pursue specific goals or outcomes based on specific knowledge and convictions about how best to achieve those goals, is an important prerequisite for experiencing work as meaningful. In the case of healthcare professionals, institutional constraints may prevent them from pursuing certain goals or outcomes in a certain way, which limits their autonomy and undermines the perceived usefulness of their work. However, autonomy and meaningfulness may not be relevant issues for all healthcare professionals, as some may regard their work as ‘just a job’ (Both-Nwabuwe et al., 2020).
Importantly, empirical findings linking limited work autonomy and social support to negative psychological consequences extend beyond the healthcare sector (Bakker and Demerouti, 2017). The evidence suggests that workers who, for instance, feel pressured by administrators to follow inappropriate orders (cf. Table 1) may suffer long-term negative consequences, even if they do not work with patients. Equally, the causal relationship between working conditions (e.g. institutional constraints, understaffing, restricted work-related autonomy, compromised agency), distress and long-term consequences does not necessarily presuppose moral events, moral judgments, moral convictions or moral agency. Even among healthcare professionals, experiences of distress and its long-term consequences may simply arise from working conditions that are misaligned with an individual’s attitudes and convictions, and which compromise their agency. These factors can contribute to distress irrespective of the involvement of patients. This means that in many empirical studies, certain manifestations of (moral) distress might stem from a general impact on well-being rather than from the moral facets of healthcare. It is important to note that distinguishing between moral issues that affect other individuals (i.e. patients) and non-moral issues that primarily affect healthcare professionals is relevant for obtaining valid empirical results and designing interventions to alleviate distress. This holds true regardless of whether we accept the distinction between moral and non-moral events as described above.
Although further research is needed, this view has been confirmed by a few small-scale studies based on factor analysis or simultaneously assessing the impacts of multiple stressors. For example, in one Australian study involving 136 nurses in a neonatal intensive care unit, the intensity of moral distress was a significant predictor of the intention to leave. However, after controlling for burnout and ethical climate (e.g. support from peers or managers) as predictors of intention, moral distress ceased to be a relevant factor (Barr, 2020). Similarly, in a Japanese survey of 391 psychiatric nurses, low staffing was the only reliable predictor of burnout, while factors related to unethical behaviour or violations of patient rights did not predict burnout (Ohnishi et al., 2010). Finally, in a survey of 280 Swiss midwives, perceived power asymmetry was the strongest predictor of long-term negative outcomes (e.g. sleep problems or the inability to recover from work), while moral conflict was not a relevant factor (Oelhafen and Cignacco, 2020). Importantly, these studies are also subject to the criticisms noted above and therefore cannot conclusively assess the respective influences of moral and non-moral stressors.
Discussion
Skilled healthcare professionals have been in short supply for many years, and the situation continues to worsen. The World Health Organization (WHO) estimates that, worldwide, an additional nine million nurses and midwives will be needed by 2030 (Pursio et al., 2021). Of the multiple causes of this shortage, the most frequently mentioned are working conditions, workload, emotional demands and wages. In addition to being a public health issue that affects employee retention and quality of care, distress (of any kind) must be taken seriously because it affects individuals’ mental health and violates their personal or moral integrity.
Despite decades of research on moral distress, consensus on the subject is limited, and effective interventions to mitigate moral distress are notably lacking. In fact, the Covid-19 pandemic has exacerbated the problem in many countries, and more people are leaving the healthcare professions because of ingrained systemic issues, including increasing workloads, insufficient resources, dysfunctional collaboration and frequent team changes (Riedel et al., 2022). Accordingly, there is an urgent need for intervention studies to explore how (moral) distress among healthcare professionals can be addressed more effectively (Tigard, 2018). However, as noted in the Introduction, such studies are unlikely to bear fruit if the underlying theory remains incomplete and fails to clarify ambiguities and causal relationships. In their integrative review, Amos and Epstein (2022) found that only approximately half of intervention studies are informed by a theory or model. A theoretical framework grounded more solidly in valid empirical data would help to strengthen ethics education (cf. Viens et al., 2020) and clinical ethics support services.
As argued above, the present state of knowledge reflects the limitations of both narrow and wide definitions of moral distress, contributing to the risk of bias and overestimation of prevalence when collecting and interpreting empirical data. This particularly applies to the observed association between (moral) events, distress and negative long-term consequences, such as poor quality of care or job attrition. Our central contention is that investigations of the ‘causes of moral distress’ (Lützén and Kvist, 2012: 16) are compromised, as most of the empirical approaches attribute some potential causes a priori while excluding others (cf. Figure 1). Taking the classification of mental disorders as a point of reference, it seems useful to combine the causes and symptoms of moral distress only if specific moral events and symptoms can be linked empirically to distress in studies that also assess various non-moral causes known to be relevant for outcomes such as job satisfaction, job attrition and burnout. It should be emphasized that a scientifically accurate distinction between genuine moral distress and other forms of distress does not at all negate the adverse effects of moral distress. For example, it is conceivable that a smaller proportion of healthcare professionals are affected by moral distress – suggesting that the prevalence of moral distress might be overestimated – yet those affected may suffer considerably from it. Such mechanisms can only be revealed through carefully designed studies. Addressing the possible overestimation in the prevalence of moral distress should therefore not be misconstrued as downplaying distress originating from genuine moral events; such distress is burdensome for affected individuals and poses significant challenges for healthcare professionals and their patients.
Future research on moral distress must seek to ground any definitions in empirical evidence from studies that are methodologically sound, considering both moral and non-moral distress as challenges to the effective delivery of healthcare, the well-being of healthcare workers and the functioning of healthcare systems. As this critical examination of previous research suggests, the success of this endeavour will depend on the following methodological requirements. First, as mentioned earlier, a conceptual distinction between moral and non-moral events is foundational for the empirical differentiation between moral distress and other forms of distress. Therefore, conceptual debates and developments should focus on defining which events should be labelled as moral. Qualitative research can aid in this endeavour by facilitating discussions on profession-specific moral issues. Second, once questions regarding these definitional boundaries are addressed, new questionnaire instruments should be developed or existing ones revised to avoid the conflation of multiple events within single questionnaire items, thereby eliminating double-barrelled items. Third, it is imperative to measure the frequency of moral events and psychological distress separately. Combined measures – such as ‘total moral distress’ – do not offer a valid approach for gaining a better understanding of the relationships. Fourth, studies should simultaneously assess the impact of moral events, working conditions and individual factors on distress and other long-term negative consequences. This goal necessitates multivariate statistical methods, such as multivariable regression (potentially combined with factor analysis) or structural equation modelling. Lastly, longitudinal studies, in contrast to cross-sectional studies, allow for valid conclusions regarding causal relationships by establishing links between emerging factors and long-term outcomes. Although related concepts, such as moral injury (Dean et al., 2019), moral residue (Lützén and Kvist, 2012) and moral failure (Morley et al., 2022) were beyond the scope of the present review, a similar conceptual clarification and research agenda would help to distinguish these concepts more clearly from moral distress.
Footnotes
Data sharing statement
Data availability is not applicable to this review article as no datasets were generated or analysed in conducting the review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study is non-empirical and does not involve human or animal subjects; consequently, ethical considerations regarding informed consent and treatment of subjects are not applicable.
Informed consent
Informed consent does not apply to this review article.