
Abstract
This mixed-methods study used an online cross-sectional survey to explore perspectives of 533 adult Australian women living with endometriosis pain, and their relationship with biopsychosocial factors. Four themes were constructed: The primary theme, ‘Stigma and change’ reflected women’s experience of dismissal, and the wish to reverse the narrative of pain as normal. Some women emphasised self-education and self-advocacy to affect change, reflecting the theme ‘self-empowerment’. Participants described the ‘debilitating impact’ of endometriosis and the enduring difficulty of ‘inadequate healthcare’, reflecting themes three and four. Analysis indicated type of social support may impact perceived outcomes for endometriosis. Hierarchical regression analyses indicated too few significant relationships between biopsychosocial factors and themes to indicate meaningful patterns without risk of common method variance. Future research should explore the influence of social support and interventions which develop participant autonomy and practitioner competence and knowledge, using disease-specific measures over time.
Keywords
Introduction
Endometriosis is a chronic pelvic condition whereby endometrial tissue forms outside the uterus, causing inflammation (Cox et al., 2003; Nnoaham et al., 2011). Common symptoms include heavy bleeding, fatigue, and painful intercourse (Schoep et al., 2019; Soliman et al., 2017). A key disease feature is debilitating pain, significantly more severe compared to other gynaecologic conditions and linked to reduced quality of life (QOL) (Evans et al., 2021; Gao et al., 2006;). In Australia, it takes 6–8 years from symptom onset to diagnosis (Cox et al., 2003; Moradi et al., 2014). Diagnostic delay can be attributed, partly, to stigma associated with menstrual symptoms, as women avoid help-seeking with critical implications for wellbeing (Grogan et al., 2018; Simonsen et al., 2020). Due to complex symptomatology and unknown aetiology, research is inconclusive regarding the relationship between disease stage and symptom severity; some women with mild endometriosis experience severe symptoms while others classified moderate to severe are asymptomatic (Culley et al., 2013). Fatigue affects over 70% of this population, significantly impacting daily functioning and social lives (Culley et al., 2013; Schoep et al., 2019; Soliman et al., 2017). A meta-synthesis of 18 qualitative studies revealed women with endometriosis tend to reduce social participation to avoid experiencing symptoms in public (Young et al., 2015). Thus, it is unsurprising that psychological symptom prevalence in these women is estimated between 50% and 86%; 60% reporting moderate to severe symptoms (Schoep et al., 2019; Sepulcri and Do Amaral, 2009; Soliman et al., 2017).
Endometriosis treatment typically adopts a biomedical approach, reductionist in emphasis on mind-body duality, and inadequate given the rate of symptom reoccurrence and associated psychosocial factors (Engel, 1977; Joseph and Mills, 2019). Given reported frustration over disease-centric approaches that dismiss the quality of pain, treatment and research should be conducted through the lens of pain rather than disease (i.e. spread of lesions) (Denny, 2009; Van Barneveld et al., 2020; Young et al., 2015). Research has quantified biopsychosocial symptoms of endometriosis, however their impact on psychological health is equivocal as studies are often of poor quality or lack comparator groups. For example, studies have yet to confirm significant differences in psychological distress in endometriosis when compared to healthy women and show no differences when compared to non-endometriosis related chronic pain, highlighting the influence of pain (Coiplet et al., 2022; Evans et al., 2021; Pope et al., 2015). However, studies show women with endometriosis score significantly lower than healthy women in measures of health-related QOL (Friedl et al., 2015; Kalfas et al., 2022). Given the psychological impact and the primacy of women’s concerns, are unconfirmed (Denny, 2009), it is important to explore these within a large-scale study to best understand how to reduce the impact of endometriosis (Joseph and Mills, 2019).
Qualitative studies offer in-depth analysis of the lived experience, but few have been conducted within Australia, though one study found over a third of women were dissatisfied with treatment options and care (Evans et al., 2022). Drawing on a previously studied, large and ongoing cohort of Australian women with dysmenorrhoea and endometriosis (Evans et al., 2021, 2022), this study aims to use the strength of mixed-methods to investigate the relationship between women’s salient perspectives and biopsychosocial factors of fatigue, perceived social support, psychological symptoms, and QOL. Previously, this method has only explored information needs, dyspareunia, and treatment satisfaction in women with endometriosis (Culley et al., 2013; Evans et al., 2022). This is important for a population whose reticence to disclose may reflect stigma which has left them feeling unheard, isolated, and distressed.
Method
Participants
Between June and August 2020, 533 Australian women with endometriosis, answered questions on pelvic pain. Participants were recruited through social media (health groups on Facebook and Instagram), university forums, and gym membership groups, and directed to an online survey, where they were screened for eligibility, provided informed consent, and completed a 30-minute questionnaire, hosted by Qualtrics version XM. Eligible participants included Australian women aged 18–50 years, menstruating within the last year, and who could respond in English. Exclusion criteria included those who: did not have a period in the last 12 months, resided outside Australia, did not identify as a woman, did not provide consent, did not complete the survey, or reported no menstrual pain on the numeric rating scale (0–10). Surveys were piloted with a group of nine fourth-year psychology students. University Human Ethics Advisory Group (HEAG-H 10_2019) approved this study. Informed consent was derived from participation.
Measures
Quantitative measures
Participants provided sociodemographic information on age, education, employment status, ethnicity, marital status, and parous state. Endometriosis pain was rated on an experience of no pain (0), mild (1), moderate (2), or severe (3) pain, as per the Pain Severity Scale, and usual level of endometriosis pain without pain medication was rated on a scale of zero to ten.
Participants answered questions regarding biopsychosocial factors related to endometriosis. Endometriosis-related fatigue was measured using the 14-item Fatigue Symptom Inventory (FSI; Hann et al., 1998), which has a reported Cronbach’s alpha of 0.94 (Hann et al., 2000). Psychological symptoms were self-reported using the 21-item Depression Anxiety Stress Scales Short Form (DASS-21; Lovibond and Lovibond, 1995), indicating frequency of symptoms of depression (7 items), anxiety (7 items), and stress (7 items), higher scores indicating greater symptom frequency. Mild to moderate scores range between; five and ten for depression, four to seven for anxiety, and eight to twelve for stress. Scores above these indicate severe symptoms. Subscales report Cronbach’s alpha’s ranging from 0.87 to 0.94 (Antony et al., 1998). Perceived social support of family, friends, and significant others was measured using the 12-item Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988), higher scores indicating greater perceived social support. The MSPSS subscales report Cronbach alpha’s ranging from 0.85 to 0.91 (Zimet et al., 1988). Quality of life was measured on a 5-point Likert scale of the 26-item WHOQOL-BREF (WHOQOL; WHOQOL Group (1996) across four domains: Physical (7 items), Psychological (6 items), Social (3 items), and Environmental (8 items), higher scores indicating greater quality of life. Internal consistency coefficients range from 0.68 to 0.82 (Skevington et al., 2004).
Qualitative measures
Qualitative measures included the open-ended health communication question: ‘What would you like to say to other people interested in learning more about what it’s like to live with pelvic pain (including period pain)?’, and questions regarding endometriosis diagnosis; ‘have you ever received a diagnosis of endometriosis?’; ‘how was the diagnosis made?’
Study design
Mixed-methods analysis was conducted on cross-sectional data collected from a large community sample. Data were analysed using a subtle realist lens which assumes existence of an objective truth however acknowledges that observation and inquiry is enmeshed within the perspective of, and contexts and concepts held by the researcher, but allows for meaningful interpretation of phenomena (Brooks et al., 2015; Hesse-Biber, 2016). A rich descriptive approach was adopted to determine important themes and insights on what is considered a poorly understood phenomenon (Kim et al., 2017). Inductive approach guided qualitative analysis of responses from the open-ended health communication question.
Analysis
The mixed-methods approach has been previously published and involves a qualitative analysis of themes followed by a logistic regression to explore theme correlates (Keeton et al., 2015). This method was deemed appropriate as it responds to the need for a large, representative sample from which to better understand the experience of endometriosis to improve education, research, and outcomes for those affected (Keeton et al., 2015; Tariq and Woodman, 2010). The first author is a psychology student with clinical endometriosis diagnosis, and the second and third authors are health psychology researchers with lived experience of endometriosis. Despite access to information, support, and healthcare, the first author acknowledges empathising with the experiences of respondents, particularly the stigma, lack of social understanding, and dismissal of symptoms reported. This position was discussed in initial research meetings, and the decision made to institute reflexive journaling and menstrual symptom tracking. Thus, constant reflection and several iterations of analysis were involved to minimise excessive interpretation of data. When data elicited strong responses, these were discussed with respect to the influence on coding, with additional coding conducted by another team member to maintain template integrity.
Qualitative data analysis
Template analysis was employed to analyse the open-ended health-communication question as a flexible but structured approach focusing on the richest data (Brooks et al., 2015). This experiential approach elucidates common perspectives of women with endometriosis pain and provides a template with which to compare to biopsychosocial factors of endometriosis, to understand whether such quantitative data reflects women’s perspectives on living with endometriosis pain. This study utilised Brooks et al.’s (2015) six step process as follows; (1) Familiarisation through first author reading the full dataset twice before notetaking; (2) Preliminary hand-written coding of 10% of data by first author, though codes and themes were not developed a priori. Words, concepts, and ideas were noted from each response, sometimes producing one code, such as;’ severe pain’, and sometimes several codes such as; ‘self-educate’, ‘persevere’ or ‘doctors don’t listen’. (3) Organising codes (first author) into a hand-written thematic map; (4) Entering codes into a spreadsheet to formalise the initial template (first author); (5) Refining template; re-reading and formulating codes, and organising themes based on full dataset, in discussion with second and third authors; (6) Final template produced with compelling extracts. From the full dataset, approximately 10% of data (56 responses) were separately double coded by another investigator at stage five to confirm and refine themes (Lombard et al., 2004). Themes were coded into SPSS and combined with quantitative data for analysis.
Quantitative data analysis
Quantitative analysis was conducted using IBM SPSS Grad Pack standard V28. Bivariate correlations using Spearman’s rho were conducted between themes (coded as a binary variable – reporting vs not reporting a particular theme) and factors of interest (e.g. symptoms of anxiety and depression). Not all factors were correlated to all themes at the univariate level; fatigue was not correlated to any. However, as this investigation was exploratory, all correlates were included in regression models. Hierarchical logistic regressions were run to investigate relationships, using themes as dependent binary variables. Independent variables in all regressions, were included in steps; with demographic variables at step one, and psychological domains, perceived social support, fatigue, and quality of life at step two. Education was recoded to 0 = ‘non university’, 1 = ’university’ and Employment was recoded to 0 = not employed, 1 = employed. All regression assumptions were met. Mean score imputations were conducted on missing data (<5% of responses). The p value of less than 0.05 was considered significant.
Results
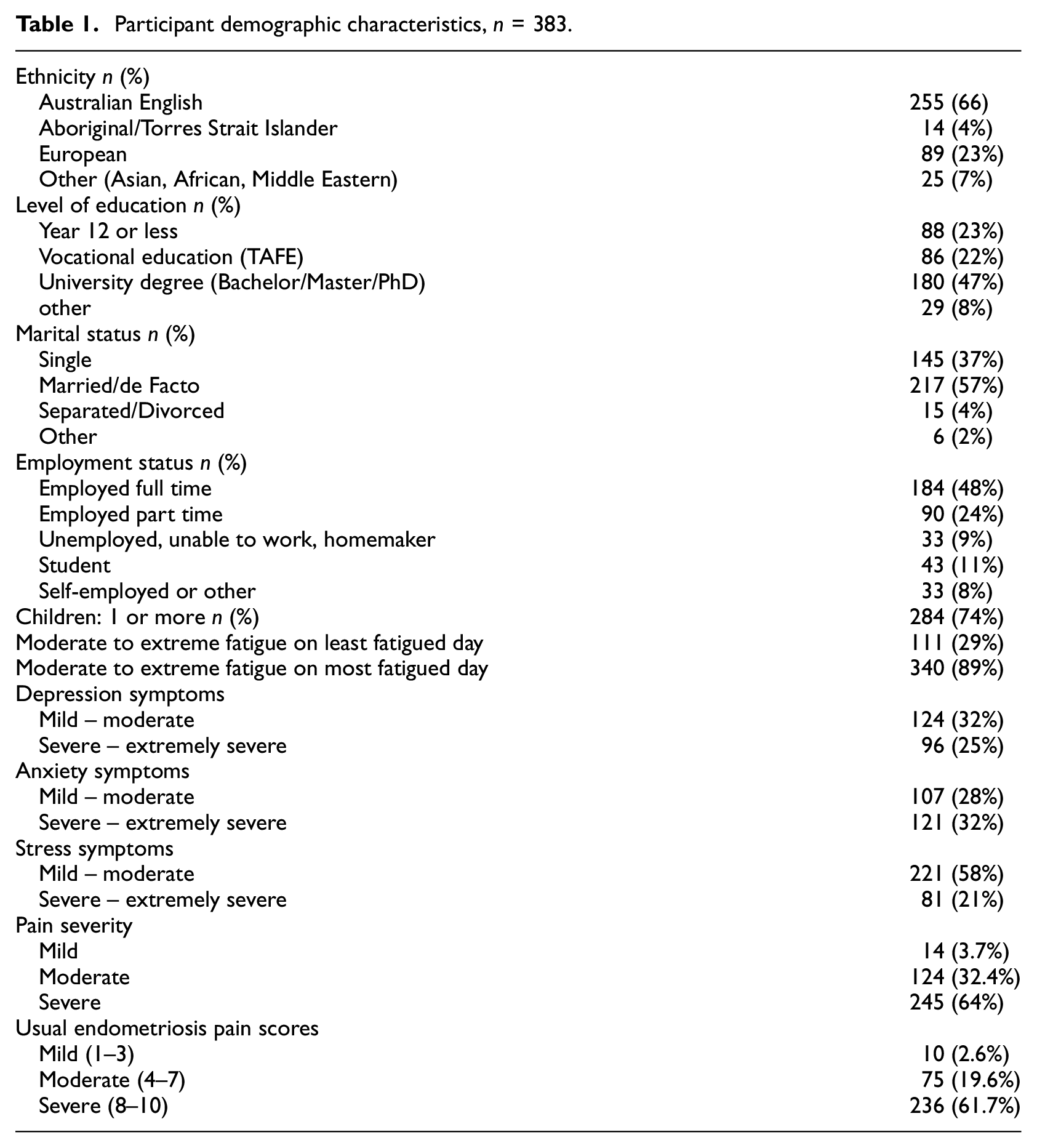
Of 533 participants, 150 did not answer the open-ended question or answered tentatively (e.g. ‘unsure’, ‘don’t know’) and were excluded from analysis. Final participants were 383 Australian women with endometriosis aged 18–49 years old (M = 30.9 years, SD = 7.1), predominantly Australian English (66%), who were or had been married (63%), and had conceived at least one child (74%). Almost half were university educated (47%) and employed full-time (48%). Women reported on average, 15 years of period pain (SD = 6.7) with 62% indicating usual pain scores above 8 (out of 10). Laparoscopy was the main form of diagnosis (85%). All women reported experiencing fatigue in the prior week, and over half reported experiencing psychological symptoms. Participant demographics and symptom prevalence are presented in Table 1. Means and Standard deviations of questionnaires included are presented in Appendix A.
Participant demographic characteristics, n = 383.
Themes of living with endometriosis pain
Responses were coded then clustered using arrows, colours, or lines to represent associations, forming a thematic map, and finalised into a template. The first author reflected on feeling empathy with participant frustration during data familiarisation, and so, conducted several iterations and refinement of coding to ensure veracity of coded responses. This acknowledges the interpretive nature of thematic analysis, and the fact that such work can produce multiple perspectives dependent on researcher context (Brooks et al., 2015). Qualitative analysis produced four main themes: Debilitating Impact, Stigma and Change, Inadequate Healthcare, and Self-Empowerment, presented with subthemes and illustrative verbatim quotes.
Debilitating impact
Overall, 163 participants reported endometriosis disrupting all aspects of their lives including physical, psychological, and social wellbeing. Coding examined symptoms of fatigue, migraines, and nausea, with most experiencing severe and chronic pain, comprising the subtheme ‘physical impact’. ‘ … typically for me it’s extreme fatigue, nausea, intense abdominal stabbing pain & running to the bathroom… ’ (aged 31, moderate pain).
Many reported heavy bleeding or embarrassing symptoms that interfered with social or work commitments resulting in disruptions with plans. Here, codes indicated ‘physical impact’ and ‘social-relational impact’, reflecting impact to work, employability, intimate relationships, and social lives. For example, presenteeism was common as women evaluated the level of debilitation and saved leave for ‘unbearable days’ when functioning would be impossible. ‘I’d say that it effects every facet of your social/sexual/personal wellbeing. It effects my husband just as much’ (aged 24, severe pain).
You have to be cautious taking time off work or school because you dont know how bad it is going to get. There is always a worse day so if your pain is at a level you can function, you really need to try and push through so that you can take time off when you have days that are unbearable (aged 25, severe pain).
For some, psychological effects were most impactful with reports of depression, anxiety, loneliness, and hopelessness. Naming of diagnoses, feelings, or impact to mood or functioning, such as ‘ … takes the joy out of life’ (aged 30, moderate pain), were coded individually but formed the subtheme ‘psychological and emotional impact’. ‘ … they should be aware that the pain is intense, often radiates, and is (in my experience), connected with fatigue and mood issues like anxiety and depression’ (aged 37, severe pain). Many reported that endometriosis impacted their whole life but only few conveyed uncertainty or resignation toward their situation. ‘ … The person has to reconcile trying to manage the pain, potentially indefinitely’ (aged 37, severe pain). ‘Resignation’, although originally conceptualised as a contrasting but related cluster to ‘see the positive side’, was designated to the ‘debilitating impact’ theme because women reported ‘putting up with’ or being uncertain of its end often referencing the pervasive burden of endometriosis, that ‘ …affects every aspect of your life’ (aged 34, moderate pain). Overall, women reported endometriosis as relentless and isolating, particularly due to lack of empathy, support and stigma they endured.
Stigma and change
Overall, 235 women reported being stigmatised and having their pain and symptoms dismissed, forming the subtheme ‘dismissed and chastised’; ‘It’s like being a second-class citizen, no one takes you seriously… ’ (aged 30, moderate pain). Some associated this dismissal with a general lack of understanding about endometriosis and menstrual pain, coded as the subtheme; ‘lack of understanding’. ‘Develop understanding…I’m so sick of having to justify my pain to others. Just a lack of general understanding’ (aged 28, moderate pain). Some mentioned the ‘invisibility’ of endometriosis, living through pain or hiding symptoms for fear of judgement, representing ‘suffering in silence’, ‘ …I think women often underplay their pain because they are told for so long that period pain is normal and don’t want to be perceived as dramatic… ’ (aged 22, moderate pain). Some women expressed lack of care from family and friends, implying an ongoing disregard of their pain, some since adolescence, and a feeling of desperately wanting more support.
‘Women have tried to speak and been shut down so they stop trying to express themselves. Please ask questions and listen. We need to rethink and shed light on what is “normal” and what needs support and treatment. It should not be considered normal for women to suffer from pain all their lives’ (aged 36, moderate pain).
Others discussed symptom concealment in specific relation to work; needing relief but feeling forced to downplay symptoms or pretend to be okay for fear of losing their job. These were coded as both ‘social-relational impact’ and ‘suffering in silence’. ‘ …mention the pain or complain so much less than they experience pain…for fear of being thought of as incapable of the job, or that we are making excuses’ (aged 22, mild pain).
Women also reported the need for increased empathy, and greater awareness and research into endometriosis. ‘Do your research! Listen with empathy to people that actually have this kind of pain and don’t brush it off as part of “being a woman”!’ (aged 21, severe pain). In addition to stigma, women expressed the need for others to help change the narrative of women’s pain; no longer wanting it normalised. ‘Pain is a sign something is wrong and women are constantly told this pain is normal and to deal with it. So I’d want them to know that in addition to pain we have to deal with bullshit attitudes’ (aged 31, moderate pain).
Template refinement produced two opposing themes; ‘stigma’ (what participants discouraged) and the ‘need for change’ (what participants encouraged), and author discussions centred on whether to consider these separately. Many responses coded across both subthemes; women needed both greater support and change regarding stigma. Thus, authors agreed they be considered together under the theme ‘stigma and the need for change’ (labelled as ‘stigma and change’), thereby achieving greater parsimony.
Listen to women as if they were your most cherished person. The level of debilitation related to pain cannot be quantified. We are all suffering in our own ways, and it’s so disheartening when you or others compare ‘how bad it is’ related to someone else. Believe women when they say they have pain!… to have your integrity questioned every time you raise the issue just makes you hide it more (aged 31, mild pain).
Inadequate healthcare
Overall, 86 women reported healthcare as inadequate, suggesting doctors have limited endometriosis knowledge leading to diagnostic delay or misdiagnosis. Women felt they needed to ‘push for care’ and get a second opinion; ‘It took me 12 years to find gynochologist who took the time to listen to me… ’ (aged 27, severe pain), and participants reasoned this was because doctors did not take them seriously or blamed them. Women described doctors’ knowledge of endometriosis as inadequate, lacking understanding, and resulting in mismanagement or misdiagnosis.
It is deeply depressing to be dismissed and sent home by specialists who either dismiss your pain or refuse to offer surgical cure, or be pushed to try hormonal contraceptives that worsen the problem. Rather than admitting there is no solutions, some doctors try to ‘victim blame’ … (aged 41, severe pain).
Here, the lack of understanding and stigma about women’s health was specifically regarding experiences with doctors, often expressed in terms of the disparaging and misinformed opinions of clinicians; ‘treatment and public health care is largely inadequate. AND no drinking some herbal tea or probiotics wont fix it’ (aged 33, severe pain). Stigma created a financial burden because of increased costs associated with doctor shopping and trying multiple treatments ‘its very expensive and i cannot afford to treat myself properly’ (aged 36, severe pain). This consequently impacted women’s capacity to earn money, impacting their career and financial stability.
Self-empowerment
Overall, 115 participants expressed the need to be self-empowered, including the need for self-advocacy and education, and being positive. Initially, responses were coded as separate subthemes of self-advocacy and self-education, but participants often discussed these concurrently, thus they were combined to achieve parsimony. ‘ … research / absorb as much info and educate/ spread awareness yourselves for you own sake if suffering personally or know of those around you suffering… ’ (aged 23, severe pain).
Women felt empowered through self-education and emphasised the importance of taking charge, considering alternative therapies, and finding treatment that worked. ‘See as many people as possible and get as many options as possible. Be your own advocate and if you know something is not right within yourself you are right and know better.’ (aged 28, severe pain). Although conveyed by only a few participants, positive perspective-taking was a salient aspect of self-empowerment, showing these women still appreciated life and were finding ways to cope by acknowledging their strengths; ‘ …sometimes there’s pain, but it doesn’t mean there’s damage being done. This helps me cope with the pain’ (aged 44, severe pain).
Analysis produced multiple codes for most responses, then refined into a template through several iterations. The included quotes convey multiple subthemes chosen due to their sentiment or depth of detail, and the authors acknowledge this choice, reflecting author context and the subtle realist lens. At template completion, responses were mapped against the themes, indicating endorsement (marked 1) or non-endorsement (marked 0) of a theme. Authors decided on theme endorsement based on specific words or phrases that reflected codes within each theme.
Mixed-method analysis
Bivariate correlations, presented in Appendix C, showed all four themes statistically significantly correlated with one or more factors. ‘Self-empowerment’ positively associated with ‘inadequate healthcare’ and negatively associated with ‘debilitating impact’ and ’stigma and change.’ Age positively associated with ‘Inadequate healthcare’ and negatively associated with ’stigma and change,’ and employment associated positively with ‘debilitating impact’ and negatively with ’stigma and change.’ PSS Family associated positively with ‘inadequate healthcare’ and negatively with ’stigma and change.’ Depression and anxiety negatively associated with ’debilitating impact,’ while WHOQOL Psychological, Social and Physical domains positively associated with ’Self-empowerment.’
Hierarchical logistic regressions are presented in Table 2. The regression model for ‘inadequate healthcare’ was not statistically significant (χ2(14) = 22.96, p = 0.061). PSS SO was excluded as the highest p value and regression re-run producing a statistically significant model; χ2(13) = 22.87, p = 0.043 (Bursac et al., 2008). Table 2 shows only 8 of 67 odds ratios reached significance at p < 0.05, with no meaningful pattern in these results. Thus, it was parsimonious to conclude that derived themes were not reliably related to quantitative variables.
Hierarchical binary logistic regression models for factors of themes related to Australian women’s perspectives on endometriosis.
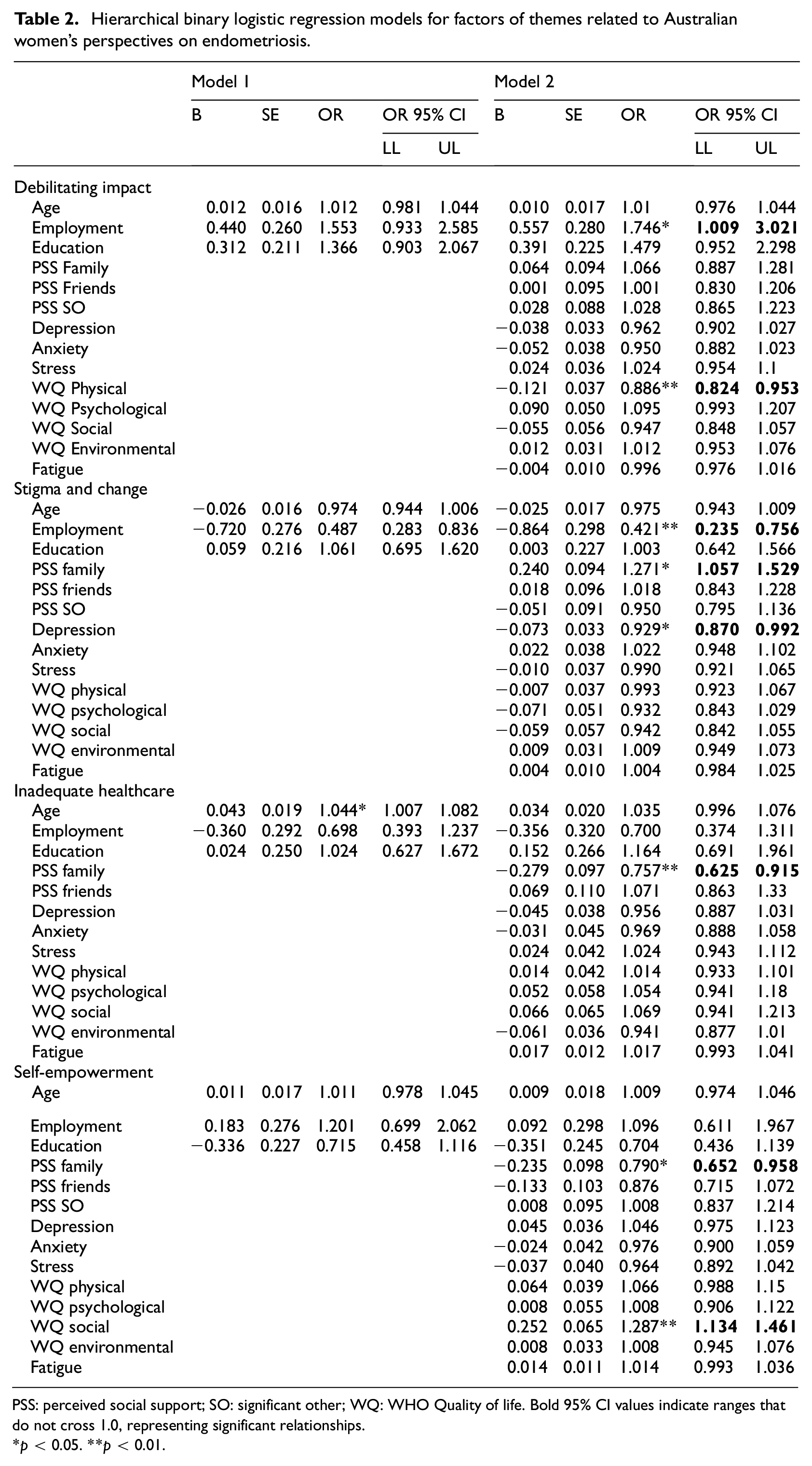
PSS: perceived social support; SO: significant other; WQ: WHO Quality of life. Bold 95% CI values indicate ranges that do not cross 1.0, representing significant relationships.
p < 0.05. **p < 0.01.
Discussion
This study revealed that women perceive healthcare to be inadequate, primarily attributed to menstrual stigma which they want changed. However, many women felt self-empowered, allowing them to remain positive in the face of the debilitating impact of endometriosis. Women commonly reported severe and chronic pain, fatigue, psychological distress, and disruption to social and work life. Although significant relationships were found between women’s salient endometriosis experiences (themes) and biopsychosocial factors of employment, social support, and depression, we could not conclude causal relationships due to the study design and potential risk of common method variance. Thus, we focus on qualitative analysis findings.
Participants discussed the debilitating impact of endometriosis on every aspect of their lives, reiterating prior findings (Grogan et al., 2018; Le Roux et al., 2022; Rea et al., 2020). Pain, which is chronic and severe, is depicted through compelling and vivid descriptions of its impact on women’s bodies and daily functioning. By inquiring about the most salient aspects of their endometriosis experience, women detailed ways in which physical symptoms directly impact them, corresponding to prior research (Culley et al., 2013; Grogan et al., 2018; Nnoaham et al., 2011). Participants described how pain and embarrassing symptoms impacted productivity, caused absenteeism, and increased their financial burden due to loss of salary, opportunities, and expensive treatment. This was shown in the correlation analysis in which employment was positively associated to ‘debilitating impact’ theme. Qualitative research has shown women with endometriosis often need to reduce or change their work situation to accommodate disease symptoms (Grogan et al., 2018; Márki et al., 2022; Missmer et al., 2021). In this study some women took extra time-off, while others suffered through symptoms to save leave for extreme pain, avoiding taking leave for fear of losing their job. This fear of judgement reflects the prevailing stigma (the predominant theme) reiterating previously identified themes such as ‘nobody believed me’, and ‘concealment of symptoms for fear of negative judgement’ (Grogan et al., 2018; Rea et al., 2020).
Felt Stigma, related to menstrual symptoms may cause shame and can impair women’s psychological fortitude, impacting their pain experience (Seear, 2009; Sims et al., 2021). Participants explained how menstrual stigma, denigration, and lack of empathy initiated self-silencing and self-doubt, especially in respect of the enduring narrative of pain many had heard since adolescence. Notably, participants attributed symptoms of depression, loneliness, and isolation, to this burden of suffering in silence. Systematic review has previously associated stigma with psychological distress including hopelessness, depression, suicidal ideation, and low self-efficacy (Livingston and Boyd, 2010). Cole et al. (2021) suggest self-silencing by women with endometriosis, not only leads to isolation and distress but also to a loss of self with broad implications for wellbeing.
In endometriosis, dismissal of menstrual pain and symptoms occurs in both healthcare and social and familial contexts (Culley et al., 2013; Markovic et al., 2008; Peterson et al., 2023). In this study, women reported a lack of support and an expectation to pretend to be well which discouraged socialisation. Social support buffers against stress by attenuating negative appraisal of stressful experiences (i.e. stigma), however this is dependent upon type and source of support (Bolger and Amarel, 2007; Shrout et al., 2006). Additionally, stress in endometriosis has been found to exacerbate pain and mental illness for those affected (Demetriou et al., 2022). This study analysis found social quality of life positively associated with self-empowerment, whereas social support from family was positively associated with stigma and change. Although we cannot conclude causal relationships, it is interesting to note this finding reiterates the theoretical position that type of support may impact experience appraisal. Manderson et al. (2008) introduced the concept of circuit-breaking, whereby women’s perspectives change from perceiving menstrual pain as normal to abnormal, most influenced by support from close relations, and only occurring when it respects the recipient’s autonomy. The MSPSS queries the extent to which family ‘tried to help’ including with decision-making, thus, greater support implies greater family influence in decision-making, shown to cause distress when challenging competence or autonomy (Ryan and Solky, 1996; Shrout et al., 2006; Zimet et al., 1988).
Research shows that inhibited autonomy and agency, and enmeshment and solicitousness may impede improvements in psychological symptoms and potentially reinforce pain behaviours and menstrual etiquette (Miró et al., 2019; Pettit et al., 2011). Stigma from healthcare professionals also had ongoing implications for social, psychological, and financial wellbeing. Many reported healthcare as inadequate, resulting in the need to push for care or conversely a resignation and retreat from help. These findings may also explain diagnostic delays, as self-silencing attributed to menstrual stigma inhibits help-seeking behaviours (Evans et al., 2021; Kocas et al., 2023; Seear, 2009; Sims et al., 2021). A collaborative therapeutic relationship can positively affect health outcomes for chronic pain patients, as clinicians have reported that women with endometriosis who feel acknowledged often feel satisfied with treatment despite pain (Grundström et al., 2016; Mikocka-Walus et al., 2012; Zoffmann et al., 2008).
Future research
The current study indicates a need for further research and education on ways in which women feel most impacted by endometriosis to reduce the associated lack of knowledge and stigma and improve health outcomes. Disease uncertainty and emotional distress in endometriosis is ascribed by those affected to attitudes of clinicians, and thus specialised care preferencing education and empowerment can improve patient health outcomes (Mikocka-Walus et al., 2012; Pettersson and Berterö, 2020; Sack et al., 2012). Interventions which focus on developing knowledge and competence in clinicians could be useful for women with endometriosis, especially if they serve to increase patient autonomy and self-empowerment. A pilot study using guided self-determination in endometriosis patients found improvement in QOL maintained after 12-months, with participants reporting increased feelings of hope and positivity (Simonsen et al., 2020). Increased pain behaviours associated with greater caregiver solicitousness has been associated with pain catastrophising in endometriosis, thus future research should investigate the role of family support in pain catastrophising in endometriosis (Cano et al., 2005; Mohammadi et al., 2017).
These findings add to an emerging body of research which indicates the way in which women receive support, may impact its efficacy. This reveals a misconception in traditional approaches to care which ordinarily assume social support, including healthcare, cannot have negative psychological impact (Shrout et al., 2006). These findings help explain endometriosis’ psychological impact and support further investigation into the relationship between pain behaviours in people with endometriosis.
Limitations
Using a validated disease-specific measure for QOL, such as the Endometriosis Health Profile (EHP-30), which captures relevant domains of pain, control and powerlessness, social support, work, relationships, and feelings about the medical profession (Jia et al., 2012; Jones et al., 2024), may have provided deeper insight into the importance of autonomy, self-empowerment, and the influence of healthcare and should be considered in future research. This study did not investigate sexual function or fertility typically regarded as important in endometriosis, although only few of the open-ended health communication responses (2.6%) reported these issues, suggesting they were of little concern among these women. However, it is difficult to predict or derive conclusions about the association between women’s perceived experience and endometriosis outcomes given the cross-sectional study design, its one-time measurement, and the mixed method analysis which did not allow for causal predictions given the risk of bias inherent in the method. Future studies could use this method using procedural and statistical controls to lower the risk of bias (Kock et al., 2021). Future research should focus on longitudinal analysis to explore impact over time and include women of diverse backgrounds to better understand their experience of endometriosis. Survey design may have resulted in response fatigue given relegation of the open-ended question to the survey’s end; indicated by short or one-word responses from approximately 20% of participants. However, providing opportunity to respond anonymously may have made honest disclosure more appealing among a population reticent to discuss menstrual symptoms.
Conclusion
Using a novel mixed-methods approach this study revealed that stigma, and inadequate healthcare and social support are related to women’s experience of endometriosis. Social support and healthcare considerate of women’s competence and autonomy may improve health outcomes for affected women.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241250101 – Supplemental material for ‘Listen to women as if they were your most cherished person’: Australian women’s perspectives on living with the pain of endometriosis: A mixed-methods study
Supplemental material, sj-docx-1-hpq-10.1177_13591053241250101 for ‘Listen to women as if they were your most cherished person’: Australian women’s perspectives on living with the pain of endometriosis: A mixed-methods study by Carmen Katz, Subhadra Evans and Antonina Mikocka-Walus in Journal of Health Psychology
Footnotes
Acknowledgements
Charlotte Dowding is thanked for her role in data curation. Yasmine Lai is thanked for her role in Investigation. We would like to thank the women who participated in this study.
Data sharing statement
The data that support the findings of this study are available from the senior second author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
University Ethics Advisory provided approval for this study.
Informed consent
Informed consent was derived from participation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.