
Abstract
We examined the associations between childhood maltreatment and the risk of impaired glucose metabolism (IGM) or type 2 diabetes (T2D) in young adults aged 18–35. Participants (N = 8506) from the Lifelines Cohort Study without IGM or diabetes at baseline (2007–2013) were included. Childhood maltreatment was assessed by the Childhood Trauma Questionnaire (CTQ) and incident IGM/T2D was assessed by haemoglobin A1c levels (≥5.7%) in 2014–2017. There were 223 (2.6%) cases of IGM/T2D during the follow-up period. After adjusting for sociodemographic and health/lifestyle covariates and follow-up time, only the CTQ Sexual Abuse subscale was significantly associated with IGM/T2D (RR = 1.05 [95% CI = 1.01, 1.10]). The association remained when additionally accounting for depressive and anxiety symptoms (RR = 1.05 [95% CI = 1.00, 1.09]). Childhood sexual abuse was associated with an increased risk of IGM/T2D in young adults, highlighting the long-term metabolic consequences of childhood maltreatment.
Keywords
Introduction
Impaired glucose metabolism (IGM), or ‘pre-diabetes’, is characterized by glucose levels that are above normal levels, but do not reach the threshold for a diagnosis of diabetes (Tabák et al., 2012). Though the rate of progression from IGM to type 2 diabetes varies according to sample demographics and diagnostic methodologies, approximately 4%–7% of those with IGM are estimated to develop diabetes annually (Hagman et al., 2016; Morris et al., 2013). IGM prevalence estimates are increasing globally in the general population (Hostalek, 2019) and also in young people (Andes et al., 2020; Thomas Pustorino et al., 2023). For instance, in a nationally representative cross-sectional study of adolescents aged 12–18 years and young adults aged 19–34 years in the United States, 18% and 24% had prediabetes, respectively (Andes et al., 2020). Young adults with IGM have a heightened risk of adverse cardiovascular and metabolic health (Andes et al., 2020; Suzuki et al., 2022). For instance, young adults with IGM were found to have an increased risk of higher systolic blood pressure (mean of 117 mmHg vs 113 mmHg), non-HDL cholesterol (mean of 133 mg/dL vs 102 mg/dL), and waist-to-height ratio (mean of 0.60 vs 0.53), compared to young adults with normal glucose metabolism (Andes et al., 2020). These findings underscore the importance of understanding and addressing IGM in the younger age groups.
In addition to evidence demonstrating a moderate risk of IGM associated with lifestyle factors such as physical inactivity and smoking (Bennasar-Veny et al., 2020; Graham et al., 2015), traumatic childhood experiences may also increase the risk of IGM. Evidence from several longitudinal studies suggests that chronic stress, including stress experienced in childhood, is associated with an elevated risk of developing IGM and type 2 diabetes (T2D) (Hackett and Steptoe, 2017; Pouwer et al., 2010). According to the biological embedding of adverse childhood experiences model (Berens et al., 2017), stressful and traumatic events experienced during childhood may impair glucose regulation among those exposed via metabolic, inflammatory, and behavioural pathways and may therefore increase the likelihood of IGM in young adulthood. In keeping with this hypothesis, adverse childhood experiences have been shown to increase the risk of metabolic conditions including T2D (Deschênes et al., 2018a; Huang et al., 2015; Lynch et al., 2013; Rich-Edwards et al., 2010; Shields et al., 2016; Zhu et al., 2022) and prediabetes (Li et al., 2017) in adulthood. However, less is known about the role of childhood maltreatment in glucose dysregulation in younger adulthood. IGM is a precursor for the development of T2D (Tabák et al., 2012), and therefore identifying young adults at the highest risk of IGM could be beneficial. Based on the limited body of evidence thus far, childhood maltreatment may be among the factors that increase the risk of IGM in young adults.
Childhood maltreatment refers to acts of commission or omission by a parent/caregiver that harm, have the potential to harm, or pose a threat to a child (Arias et al., 2008). Acts of commission include physical, sexual, and emotional abuse, while acts of omission involve physical and emotional neglect. Physical abuse entails intentional use of physical force against a child that may result in physical injury; emotional abuse includes intentional non-physical actions (e.g. terrorizing, blaming, confining, corrupting, exploiting); sexual abuse entails involvement of a child who has not reached the legal age of consent in any kind of sexual behaviour, completed or attempted, or activity including sexual exploitation of the child (e.g. sexual trafficking) and non-contact sexual interaction (e.g. exposure to pornography); and emotional and physical neglect of a child entail failure of the caregiver to fulfil the child’s basic emotional, physical, and/or educational needs or to protect the child from harm or potential harm.
Childhood maltreatment is a major public health concern, with the WHO reporting a lifetime prevalence ranging from 8% to 36% for different types of maltreatment (World Health Organization, 2022). It constitutes a profound traumatic experience with devastating consequences on children’s development and long-term psychological and physical wellbeing, often persisting into adulthood. Meta-analytic evidence suggests that individuals exposed to any type of childhood maltreatment were 2.5 and 1.6 times more likely to develop depression and anxiety disorders, respectively (Gardner et al., 2019). Childhood maltreatment has also been linked to increased risk of developing chronic physical conditions such as heart disease, chronic pain, and diabetes (Gordon, 2021).
Two large population-based studies to date examined the role of child maltreatment in the risk of developing IGM in young adults (Duncan et al., 2015; Sonu et al., 2019). Duncan et al. (2015) examined associations between child maltreatment during two waves of data collection as well as the risk of developing diabetes and prediabetes during the latter of these two waves in a nationally representative sample of US young adults aged 24–35 years, stratified by sex, of the National Longitudinal Study of Adolescent Health. Physical abuse was found to predict an increased likelihood of developing prediabetes in men in unadjusted models, while neglect was consistently linked to an increased risk of developing prediabetes in women both in unadjusted and adjusted models. In a cross-sectional study, Sonu and colleagues (Sonu et al., 2019) examined the associations between adverse childhood experiences (ACEs), including childhood maltreatment, and several early-onset chronic conditions such as cardiovascular disease, cancer, and pre/diabetes, using data from the US 2011–2012 Behavioural Risk Factor Surveillance System. They found that young adults aged 18–34 years with four or more ACEs, compared to those with no ACEs, had a three-fold higher risk of IGM, adjusted for sex, race, income, education, and State. However, childhood maltreatment was not examined separately as an individual predictor. The prospective associations between childhood maltreatment and the risk of incident IGM, objectively measured using blood samples, in a large and longitudinal cohort of young adults, have to our knowledge not yet been examined.
Therefore, the primary aim of the present study was to examine whether different types of childhood maltreatment were longitudinally associated with an increased risk of developing IGM or T2D in young adults. A longitudinal study design can strengthen the inferences that could be made regarding the potential temporal association between childhood maltreatment and the subsequent onset of IGM or T2D. Furthermore, given that meta-analytic evidence has linked childhood maltreatment to an increased risk of developing depressive and anxiety disorders (Gardner et al., 2019; Li et al., 2016), and has also shown that depression (Graham et al., 2020) and anxiety (Smith et al., 2018) are associated with an increased risk of T2D, a secondary aim of the present study was to examine whether childhood maltreatment was associated with an increased risk of IGM independently of associations with depression and anxiety levels in addition to sociodemographic and lifestyle covariates.
Methods
Study design and participants
Data were from the Lifelines Cohort Study and Biobank (Lifelines) (Scholtens et al., 2015). Lifelines is a multi-disciplinary prospective population-based cohort study examining in a unique three-generation design the health and health-related behaviours of 167,729 persons living in the North of The Netherlands. It employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioural, physical, and psychological factors which contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics. Data are collected across multiple waves involving self-report and survey data as well as laboratory visits where biological samples are collected, and anthropometric assessments are performed. Baseline surveys and laboratory assessments were completed in 2007–2013, and a second laboratory visit was completed in 2014–2017. Details on the Lifelines design and recruitment procedures are described elsewhere (Klijs et al., 2015). The Lifelines study design was approved by the Ethics Committee of the University Medical Centre Groningen and all participants provided informed consent prior to participation.
A total of N = 8506 participants met the inclusion criterion for the present study, which first consisted of being 18–35 years of age at baseline. Because there is a lack of consensus regarding the age ranges that constitute young adulthood, we employed a liberal and more inclusive definition of this life stage by extending the age range of young adulthood up to 35 years of age at the time of the baseline blood test for IGM assessment, and up to 39 years old in the follow-up assessment. Other inclusion criteria were having available data on childhood maltreatment at baseline and having complete data on haemoglobin A1c (HbA1c; a measure of diabetes control over the previous 2–3 months) levels at baseline and in the follow-up laboratory visit, with HbA1c levels within the normal range (20 mmol/mol; 4%–38 mmol/mol; 5.6%) at baseline. Of those meeting the baseline inclusion criteria (N = 9007), 501 did not have HbA1c data available in the follow-up laboratory visit and were therefore lost to follow-up. Table 1 presents the participant characteristics for the total included sample and the sample stratified by IGM/T2D status at follow-up.
Frequencies, means and standard deviations.
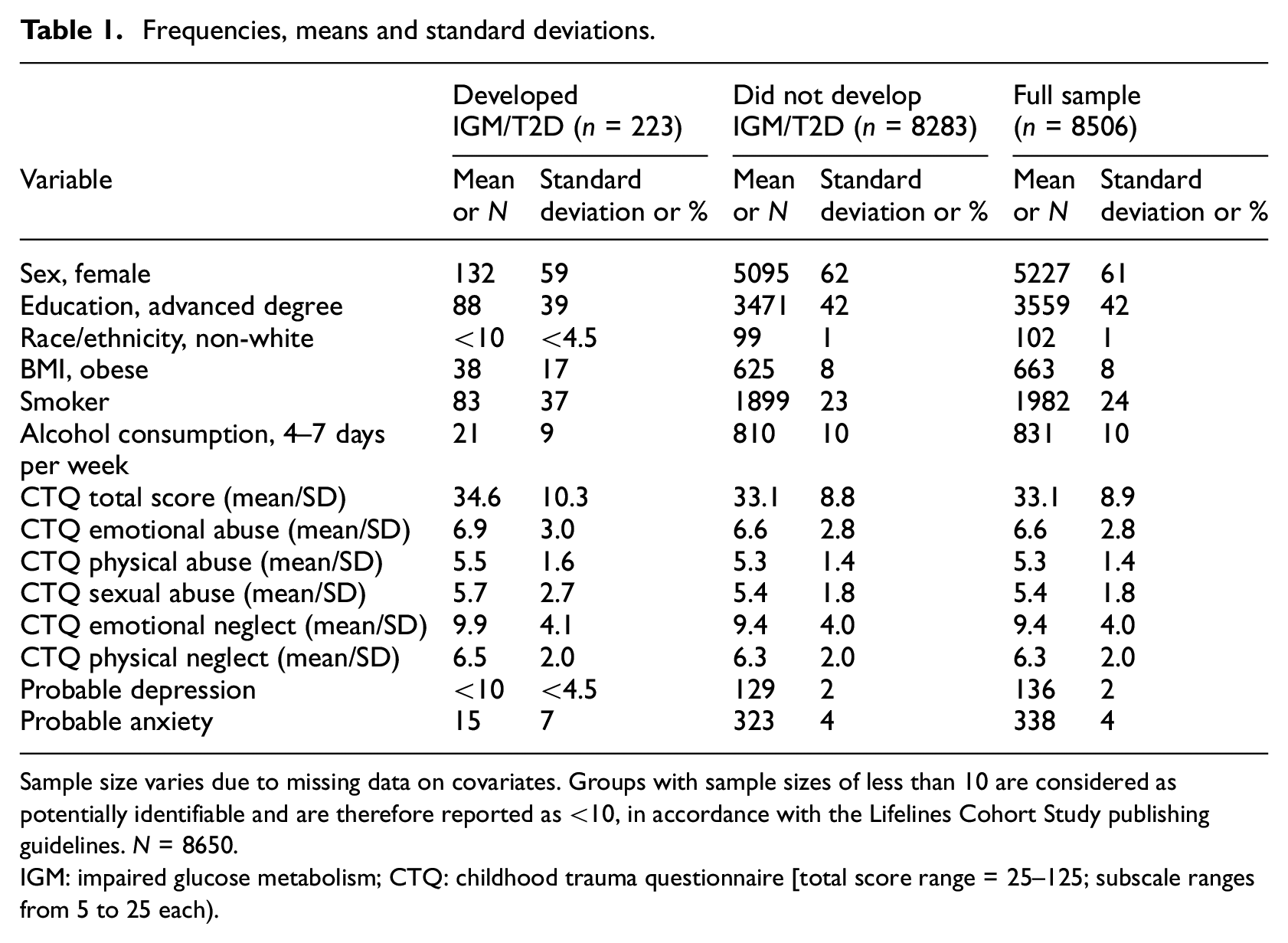
Sample size varies due to missing data on covariates. Groups with sample sizes of less than 10 are considered as potentially identifiable and are therefore reported as <10, in accordance with the Lifelines Cohort Study publishing guidelines. N = 8650.
IGM: impaired glucose metabolism; CTQ: childhood trauma questionnaire [total score range = 25–125; subscale ranges from 5 to 25 each).
Participants who were lost to follow-up were, on average, significantly younger at baseline (mean age = 27.1, SD = 4.9), though with only a small difference (Cohen’s d = 0.16) compared to those included (mean age = 27.9, SD = 4.9), p < 0.001. There were also sex and education level differences, with a higher proportion of women and higher education levels (71.3% and 45.3%, respectively) among those lost to follow-up compared to those included in the present study (61.5% and 41.8%, respectively), p < 0.001 and p = 0.046, respectively. There were no differences between those included and those who met the inclusion criteria at baseline but were lost to follow-up on baseline HbA1c levels, Childhood Trauma Questionnaire scores (described below), probable depression, probable anxiety, ethnicity, BMI, smoking status, or alcohol use frequency (p > 0.26).
Childhood maltreatment
Childhood maltreatment was retrospectively assessed by self-report using the Childhood Trauma Questionnaire-Short Form (CTQ) (Bernstein et al., 1997; Thombs et al., 2009). The CTQ is a widely used screening tool used to assess and quantify a history of childhood maltreatment in adults. The CTQ Short Form comprises 25 items that are divided into five subscales measuring Emotional Abuse, Physical Abuse, Sexual Abuse, Emotional Neglect, and Physical Neglect. Responses are rated on a 5-point Likert scale (1 = never true, 2 = rarely true, 3 = sometimes true, 4 = often true, 5 = very often true). Each subscale is represented by five items, and the total CTQ summary score ranges from 5 to 25. Items are responded to with the context ‘During my childhood’, and example items for each subscale include: ‘I felt that someone in my family hated me (Emotional Abuse)’; ‘I was hit so hard by family members that it left me with bruises or marks’ (Physical Abuse); ‘Someone tried to touch me in a sexual way or tried to make me touch them’ (Sexual Abuse); ‘I felt loved [reverse scored]’ (Emotional Neglect); and ‘I had to wear dirty clothes’ (Physical Neglect). The CTQ was administered later in Lifelines, during the second assessment from 2015 to 2017. Notably, this psychometric tool was designed to retrospectively capture childhood maltreatment up to the age of 18 years.
Reliability of the total scale and each subscale was calculated, with Cronbach’s alpha coefficients indicating good to excellent reliability for the total scale (α = 0.88), the CTQ-Emotional Abuse (α = 0.80), CTQ-Physical Abuse (α = 0.78), CTQ-Sexual Abuse (α = 0.87), and CTQ-Emotional Neglect (α = 0.87). However, the CTQ-Physical Neglect subscale demonstrated low reliability (α = 0.38), and therefore we did not include this subscale in analyses examining the unique contribution of each type of childhood maltreatment.
IGM
IGM status at baseline (2007–2013) and follow-up (2014–2017) was determined by haemoglobin A1c (HbA1c) levels ranging from 39 mmol/mol (5.7%) to 46 mmol/mol (6.4%), according to the American Diabetes Association (ADA) diagnostic criteria for prediabetes (American Diabetes Association, 2010). The ADA HbA1c threshold for prediabetes is lower than other diagnostic guidelines such as those published by the World Health Organization (42 mmol/mol or 6.0%) and was therefore selected to identify a greater number of participants at high risk and maximize the statistical power of the study. T2D was considered as an HbA1c level of 6.5% or above.
Covariates
The Mini-International Neuropsychiatric Interview (MINI) (Sheehan et al., 1998) was used to screen for a current, probable episode of major depressive disorder and generalized anxiety disorder symptoms at baseline. The MINI is a structured diagnostic interview designed to assess psychiatric disorders adhering to the Diagnostic Statistical Manual IV or International Classification of Diseases-10 diagnostic criteria. Participants were asked whether they experienced depressive symptoms, such as changes in appetite, sleep, or anhedonia in the past 2 weeks, and anxiety symptoms such as excessive worry and anxiety about several aspects in the past 6 months. Research has established the psychometric quality of the MINI (Sheehan et al., 1997, 1998). More information about the use of MINI as a diagnostic tool for depressive and anxiety symptoms in the Lifelines study is available elsewhere (Deschênes et al., 2018b; Meurs et al., 2016). In the present study, the probable depression group and the probable anxiety group refer to participants with a positive screen for major depressive disorder and generalized anxiety disorder, respectively, on the MINI.
Other covariates included sociodemographic characteristics (sex, ethnicity, educational attainment) and lifestyle/health characteristics at baseline and were examined in adjusted analyses. These are presented with their respective categories in Table 1. Data for covariates except from body mass index (BMI) were collected through self-report. BMI was measured by trained research staff during the laboratory visit and was calculated as kg in weight/meters2 in height and categorized according to World Health Organization BMI classification. Alcohol consumption frequency was assessed by asking participants on how many days in the past 4 weeks they drank one or more alcoholic drinks. Smoking status was coded as current smoker or current non-smoker.
Statistical analysis
Descriptive and frequency analyses were calculated for the CTQ total score and each of the subscales, probable depression and anxiety groups, incident IGM and T2D, and covariates. Given the low expected frequency of T2D, IGM and T2D outcomes were combined. Associations between the CTQ and the risk of IGM/T2D were examined using modified Poisson regression analyses with robust standard errors (Zou, 2004). Risk ratios, p-values, and 95% confidence intervals (CI) are reported. Unadjusted and adjusted analyses are reported. A first set of adjusted analyses controlled for potential confounders of age, sex, and follow-up time. A second set of adjusted analyses additionally controlled for other sociodemographic and lifestyle factors including education level, smoking, alcohol use, and BMI. A final set of adjusted analyses additionally controlled for probable depression and anxiety. Covariates were selected to examine whether any associations between childhood maltreatment would remain after accounting for traditional risk factors for IGM/T2D. However, given that some covariates could have temporally followed childhood maltreatment, these traditional risk factors could also be potential mediators. Therefore, we employed a stepwise approach to examining potential covariates. This approach allowed us to control for traditional risk factors while also providing a better understanding of the potential processes linking childhood maltreatment with IGM.
The CTQ was first examined as a continuous total score, followed by comparable analyses using each subscale separately. Associations between each CTQ subscale with incident IGM were also examined using an established categorical cut-off score (Walker et al., 1999) to compare moderate to severe childhood maltreatment with no or low childhood maltreatment. Of those meeting inclusion criteria for the present study, missing data on covariates was low, with 7.0% missing data in sociodemographic and lifestyle/health covariates and 9.2% missing data on all covariates. Therefore, missing data were not imputed.
Results
There were 8506 participants (61% female) aged 18–35 years (mean age = 28 years, SD = 5 years) included in unadjusted analyses, with 223 (2.6%) incident cases of IGM/T2D over an average follow-up duration of 4 (SD = 1.2; range = 2–10) years (see Table 1). The mean CTQ total score was 33.1 (SD = 8.9, range = 25–104). Two percent of participants met the criteria for probable depression, and 4% of participants met the criteria for probable anxiety.
Univariate analyses demonstrating the unadjusted associations between childhood maltreatment, probable depression, and probable anxiety, with the risk of IGM/T2D are presented in Table 2. The CTQ total score and the CTQ-Sexual Abuse subscale were independently associated with an increased risk of IGM/T2D. Probable anxiety was also independently associated with an increased risk of IGM/T2D.
Univariate (unadjusted) associations between childhood maltreatment, probable depression and anxiety, and the risk of IGM/T2D.
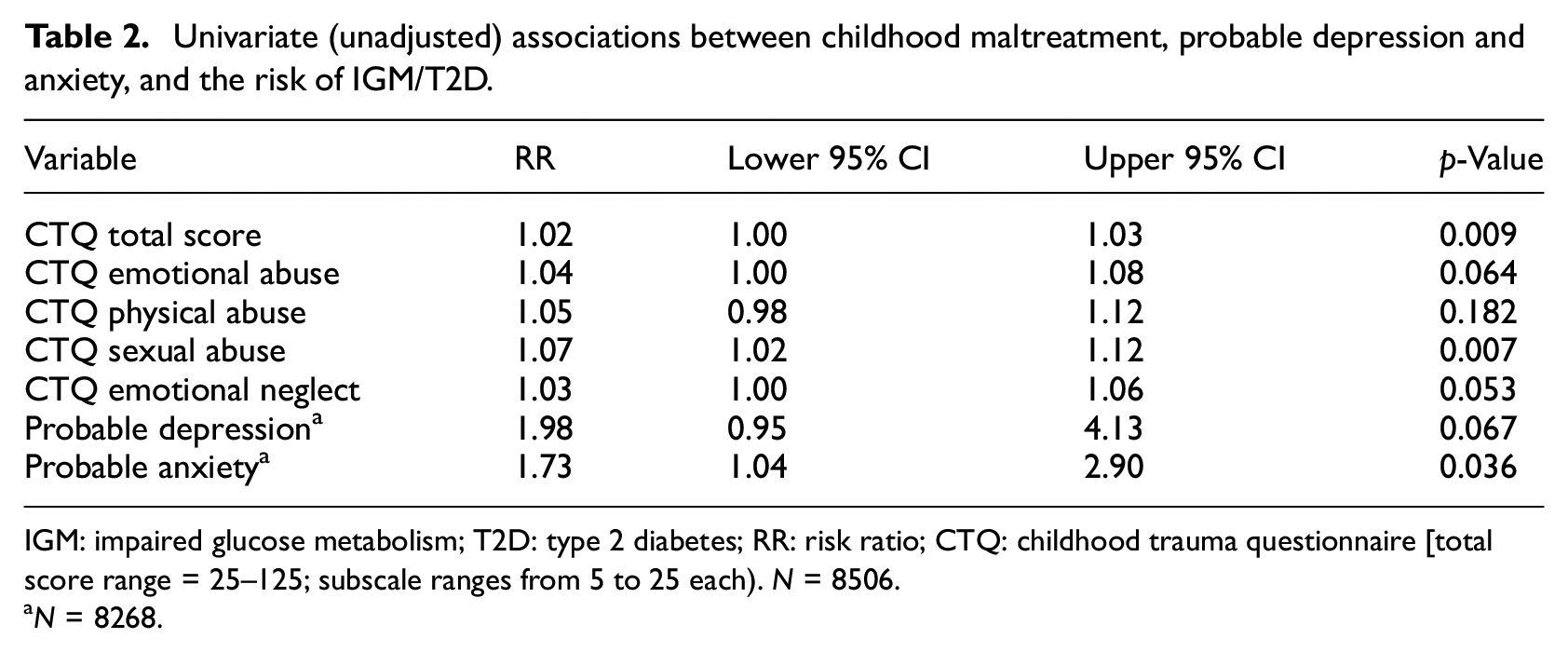
IGM: impaired glucose metabolism; T2D: type 2 diabetes; RR: risk ratio; CTQ: childhood trauma questionnaire [total score range = 25–125; subscale ranges from 5 to 25 each). N = 8506.
N = 8268.
Table 3 describes the adjusted associations between childhood maltreatment and respective subscale scores with the risk of IGM/T2D. In analyses adjusted for age, sex, and follow-up time, a similar pattern of results emerged as in the unadjusted associations, though probable depression was also associated with IGM/T2D. When additionally adjusting for sociodemographic and lifestyle/health variables, only the CTQ-Sexual Abuse subscale remained significantly associated with the risk of IGM/T2D, with every 1-unit increase in the subscale score associated with a 5% increase in IGM/T2D risk. This subscale remained the only statistically significant association in the fully adjusted analyses that additionally controlled for probable depression and anxiety, and with a similar effect size.
Results of adjusted modified Poison regression analyses for the associations between childhood maltreatment types and the risk of IGM/T2D.
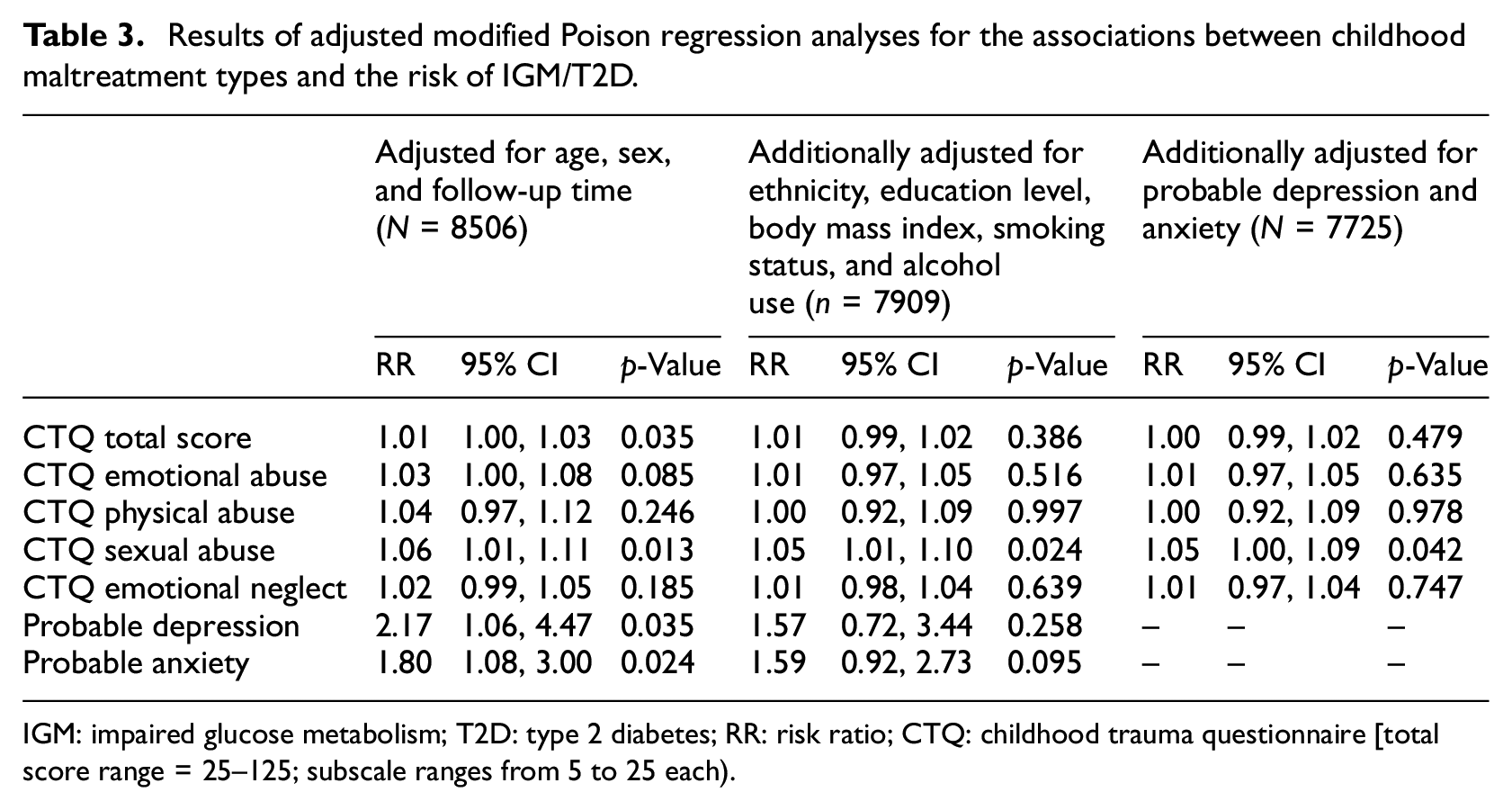
IGM: impaired glucose metabolism; T2D: type 2 diabetes; RR: risk ratio; CTQ: childhood trauma questionnaire [total score range = 25–125; subscale ranges from 5 to 25 each).
There was no significant interaction between CTQ-Sexual Abuse and probable depression (OR = 1.00, 95% CI = 0.85, 1.18) or probable anxiety (OR = 1.05, 95% CI = 0.93, 1.18) on the risk of IGM/T2D.
A post-hoc analysis was conducted using a categorical cut-off score (Walker et al., 1999) applied to the CTQ subscales to compare those with moderate to severe levels versus no or low reports of childhood maltreatment. In unadjusted analyses and analyses adjusted for age, sex, and follow-up time, sexual abuse (n = 376, 4.4%) was associated with an increased risk of incident IGM/T2D (unadjusted RR = 1.78, 95% CI = 1.10, 2.89, p = 0.019; adjusted RR = 1.74, 95% CI = 1.08, 2.82, p = 0.025). A total of 17 participants (4.5%) in the sexual abuse category developed IGM/T2D, compared to 206 (2.5%) in the no/low sexual abuse category. However, this association was no longer statistically significant in analyses that were adjusted for sociodemographic and lifestyle characteristics (RR = 1.53, 95% CI = 0.95, 2.48, p = 0.081) or in analyses that were additionally adjusted for probable depression and probable anxiety (RR = 1.48, 95% CI = 0.90, 2.41, p = 0.120). No significant associations were found for emotional abuse (n = 928, 10.9%), physical abuse (n = 371, 4.4%), or emotional neglect (n = 942, 11.1%). All unadjusted and adjusted risk ratios and confidence intervals for each maltreatment subtype are presented in Supplemental Table 1.
The covariates that were most consistently associated with IGM/T2D risk in the fully adjusted analyses were consistently age (continuous), follow-up time in years (continuous), obesity (categorical), and smoking status (binary). In the fully-adjusted analysis examining the CTQ-Sexual Abuse subscale presented in Table 3, the RR associated with continuous age was 1.07 (95% CI = 1.04, 1.11, p < 0.001), the RR associated with follow-up time in years was 1.24 (95% CI = 1.13, 1.38, p < 0.001), the RR associated with smoking category was 1.87 (95% CI = 1.41, 2.48, p < 0.001), and the RR associated with obesity relative to normal BMI was 2.25 (95% CI = 1.54, 3.28, p < 0.001).
Discussion
In this prospective study of 8506 young adults without IGM or diabetes at baseline from the Lifelines Cohort Study, we found significant positive associations between childhood sexual abuse and the risk of developing IGM/type 2 diabetes during the follow-up period. Notably, however, the effect size was small. To our knowledge, this is the first longitudinal study to investigate the prospective associations between distinct types of childhood maltreatment and the risk of incident IGM/T2D, objectively measured using blood samples, in a large prospective cohort of young adults aged 18–35 years old at baseline. Our findings demonstrate that childhood sexual abuse is a predictor of IGM/T2D in young adults, even after adjusting for age, sex, and study follow-up time. We further adjusted for other sociodemographic factors and variables such as lifestyle, obesity, and mental health covariates, which could serve as potential pathways between childhood sexual abuse and IGM/T2D. The association between childhood sexual abuse and IGM/T2D were attenuated but remained with these adjustments, which may suggest that these pathways, in addition to others, are involved.
In fully adjusted analyses, every unit increase in the CTQ-Sexual Abuse subscale score was associated with a 5% increase in the likelihood of developing IGM/T2D in young adulthood. When examining the associations between a binary childhood sexual abuse variable and IGM/T2D using an established cut-off for the CTQ-Sexual Abuse subscale, we found that young adults reporting having experienced moderate to extreme sexual abuse during childhood had a 78% increased likelihood of developing IGM/T2D compared to those with low or no childhood sexual abuse in unadjusted analyses. However, this association dissipated when accounting for covariates, which may suggest that lifestyle factors, body mass index, and depressive and anxiety symptoms are potential mechanisms underlying the associations between childhood sexual abuse and IGM/T2D. The use of categorical cut-offs applied to the continuous measures may have also reduced statistical power, which may explain the non-significant results after adjusting for the covariates. Overall, these findings highlight the role of childhood maltreatment, especially sexual abuse, in the risk of developing IGM/T2D in young adulthood. Further research is needed to investigate the mechanisms linking childhood sexual abuse to IGM/T2D in young adults.
In our study, we found that childhood sexual abuse was the only type of childhood maltreatment that was associated with IGM/T2D in young adults after accounting for covariates. In contrast to the study by Duncan et al. (Duncan et al., 2015), we did not find a significant association between physical abuse or emotional neglect and the risk of IGM/T2D. This discrepancy in findings between our study and the study by Duncan et al. (2015) may be due to different measures used to capture childhood maltreatment. For instance, in our study, the validated psychometric tool CTQ was used, while Duncan et al. (2015) used single items employed by the National Longitudinal Study of Adolescent Health survey. We therefore may have had a more nuanced approach, capturing to a greater extent the complexity of childhood maltreatment experiences. Previous studies have reported that the association between childhood maltreatment and the risk of diabetes in adulthood, including middle age and older adulthood, depended on the type of abuse experienced, though the nature of the associations with maltreatment type has been inconsistently reported (Pouwer et al., 2010). For instance, in a German study of 2510 participants aged 14 years and above, physical neglect had the strongest association with diabetes while sexual abuse had the weakest association, although all types of abuse were significantly associated with diabetes (Clemens et al., 2018). Conversely, a study of 21,878 adults (Shields et al., 2016) found sexual abuse to be a stronger predictor of diabetes than physical abuse, though both were significant predictors. Consistent findings emerged in another large study (Campbell et al., 2018a), where sexual abuse demonstrated a stronger association with diabetes compared to verbal abuse, physical abuse, or having a parent with mental illness, though all subtypes were significantly associated with increased diabetes risk. Discrepant findings across individual studies may reflect underlying differences in measurement, sample age and composition, or cultural norms in reporting maltreatment.
Moreover, a 2015 meta-analysis (Huang et al., 2015) incorporating seven cross-sectional and prospective cohort studies explored the relationship between adverse childhood experiences and diabetes in adulthood. In this analysis, sexual abuse was associated with a 39% increased likelihood of type 2 diabetes – a smaller effect size compared to neglect (odds ratio of 1.92) but larger than for physical abuse (odds ratio of 1.30) (Huang et al., 2015). However, in our sample, the physical neglect subscale had low internal consistency, rendering direct comparisons unreliable. Finally, a more recent systematic review and meta-analysis found statistically significant pooled associations for specific types of adverse childhood experiences and diabetes in adulthood, including sexual abuse, but not for childhood maltreatment subtypes of emotional abuse or neglect (Zhu et al., 2022).
A previous cross-sectional study (Campbell et al., 2018b) found that the association between childhood sexual abuse and diabetes was accounted for by obesity and depression. In our prospective study, we found that the association between sexual abuse and incident IGM/T2D remained after accounting for a host of covariates including obesity and depression, suggesting that other mechanisms may also be involved. Overall, there are several potential behavioural, psychological, and physiological mechanisms through which childhood maltreatment may increase the risk of IGM in young adults. Childhood adversity is associated with many behavioural, social, and emotional factors associated with the development of diabetes, including unhealthy eating, heavy drinking, smoking, poor educational and employment outcomes (Bellis et al., 2014), anxiety, and depression. However, the present study found that adjustment for these factors only moderately reduced the association between childhood sexual abuse and IGM/T2D. While some residual confounding may remain, these findings suggest that there may be additional pathways of insulin dysregulation associated with sexual abuse. Childhood sexual abuse may activate proinflammatory processes (Bertone-Johnson et al., 2012), which have been consistently associated with insulin resistance (Luc et al., 2019) and increased risk of diabetes (Wang et al., 2013). Similarly, sexual abuse in early childhood may lead to disruption of the hypothalamic–pituitary–adrenal (HPA) axis (Hulme, 2011), which, in turn, can lead to insulin resistance and visceral adiposity (Björntorp, 2001; Champaneri et al., 2010), precursors to IGM and T2D. Future research is needed, particularly exploring potential sex and gender differences, and examining biological systems suggested to be activated by early life sexual abuse that are also implicated in affecting glycaemic outcomes, to clarify the mechanisms linking childhood maltreatment to IGM/T2D in young adulthood. Finally, contradicting previous findings, in our study, neither discrete types of maltreatment, other than sexual abuse, nor cumulative exposure to abuse predicted risk of IGM/T2DM in young adults in adjusted models. Although speculative, one possible interpretation of this finding is that the long-term impact of sexual abuse may have significantly more detrimental outcomes when compared to other types of childhood maltreatment (Lewis et al., 2016).
Strengths and limitations
This population-based cohort study examining the prospective associations between childhood maltreatment and IGM in young adults without IGM or diabetes at baseline had considerable strengths. The longitudinal design employed by the present research allows to determine the temporal sequence of childhood maltreatment and onset of IGM/T2D, while it minimizes the risk of confounding factors such as potential differences in disease management or treatments. Furthermore, IGM was determined through objective measurements of HbA1c levels.
Despite its strengths, the present study had important limitations. First, there was no information available about characteristics of childhood sexual abuse cases such as age of onset, chronicity, frequency, or severity of exposure, and these dimensions may have a differential impact on physical health outcomes (Winter et al., 2022). Second, despite using a well-established tool to retrospectively measure childhood maltreatment, the physical neglect subscale demonstrated a low Cronbach’s alpha coefficient in our sample and was subsequently excluded from some analyses. Thus, we were not able to explore the unique link between this type of childhood treatment and IGM (Georgieva et al., 2021). Third, as an observational study, there is a risk for unmeasured confounding. In particular, other potential risk factors for IGM could be examined alongside childhood maltreatment in future research, such as a family history of type 2 diabetes, to account for potential genetic risk factors. Finally, the sample of the present study, drawn from the Lifelines dataset, has high demographic homogeneity predominantly comprising of White participants. While this could be addressed by future research, caution is required in generalizing the present study findings in cohorts from diverse demographic backgrounds.
Conclusions
Overall, our findings add to the pool of evidence highlighting the adverse long-term health outcomes of childhood maltreatment, and particularly sexual abuse, that often persist into adulthood (Gordon, 2021), and suggest that the chronic metabolic impact of childhood trauma can be evident in young adulthood. Childhood sexual abuse is one of the most profound adverse childhood experiences linked to long-term outcomes including mental disorders and physical health conditions (Hailes et al., 2019). In the present study, we found that childhood sexual abuse was associated with an increased risk of IGM/T2D in young adults. Increasing awareness of the possibility of childhood trauma among clinicians working with young adults could be helpful, so that trauma-informed care strategies could be adopted as needed (Oral et al., 2016). Awareness of a potential history of trauma can help inform treatment or health prevention strategies.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241243285 – Supplemental material for Childhood maltreatment and the risk of impaired glucose metabolism or type 2 diabetes in young adults: Findings from the Lifelines Cohort Study
Supplemental material, sj-docx-1-hpq-10.1177_13591053241243285 for Childhood maltreatment and the risk of impaired glucose metabolism or type 2 diabetes in young adults: Findings from the Lifelines Cohort Study by Sonya S. Deschênes, Finiki Nearchou, Amy McInerney, Norbert Schmitz, Frans Pouwer and Arie Nouwen in Journal of Health Psychology
Footnotes
Acknowledgements
The authors wish to acknowledge the services of the Lifelines Cohort Study, the contributing research centres delivering data to Lifelines, and all the study participants.
Data sharing statement
The data that support the findings of the present study are available by Lifelines (https://www.lifelines.nl/); however, data access is restricted. Requests for data access can be sent to the Lifelines Cohort Study and Biobank (![]() ).
).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Lifelines initiative received support from the Dutch Ministry of Health, Welfare and Sport, the Dutch Ministry of Economic Affairs, the University Medical Center Groningen (UMCG), Groningen University and the Provinces in the North of the Netherlands (Drenthe, Friesland, Groningen). The present study additionally received funding from the University College Dublin Ad Astra Start-Up grant and Enterprise Ireland support grant.
Ethics approval
The Lifelines study design was approved by the Ethics Committee of the University Medical Centre Groningen.
Informed consent
All participants provided informed consent prior to participation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.