
Abstract
Food insecurity may predict poorer body image, which is associated with increased risk of mental health problems. However, minimal attention has been given to the food insecurity-body image link and to factors that may influence this link, such as assigned sex; importantly, females are more likely to experience both food insecurity and body dissatisfaction. The present study used data from the 2017 to 2018 Canadian Community Health Survey (N = 32,017) to investigate the effects of food insecurity and sex on body satisfaction via generalized ordered logistic regression. Results indicated: (1) Food insecurity predicted lower odds of body satisfaction, (2) Males were more likely than females to be satisfied with their bodies, and (3) Food insecurity no longer predicted body satisfaction following the inclusion of sex. Findings suggest the association between food insecurity and body satisfaction may largely be driven by the link between food insecurity and sex. Further investigation is warranted.
Food insecurity—defined as inadequate access to food due to financial limitations (Gundersen and Ziliak, 2015; Tarasuk et al., 2018)—was experienced by nearly 7 million Canadians in 2022 (PROOF, 2023). Research has linked food insecurity to poorer physical and mental health (Jessiman-Perreault and McIntyre, 2017; Leung et al., 2020). However, limited research has examined how food insecurity relates to dissatisfaction with one’s body, despite body dissatisfaction being associated with adverse physical and mental health outcomes (Griffiths et al., 2016). The purpose of the present research was to determine how food insecurity predicts body dissatisfaction among a provincially representative sample of Canadians. Moreover, as a novel addition to the literature, the current study examined whether sex-based differences are present in this association, given the presence of sex-based disparities in the rates of food insecurity and body dissatisfaction (Drakoulidou et al., 2020; Griffiths et al., 2016).
Food Insecurity
Food insecurity is a marker of pervasive material deprivation with deleterious consequences (Tarasuk and Mitchell, 2020). Various risk factors for becoming food insecure have been identified. For example, females experience food insecurity at a disproportionate rate to their male counterparts (Drakoulidou et al., 2020; Walker et al., 2021). Additionally, among adults, those who are younger, are single, or identify as Black, Indigenous, or a Person of Color (BIPOC) are more vulnerable to experiencing food insecurity (Drakoulidou et al., 2020; Tarasuk et al., 2019; Walker et al., 2021).
In recent years, it has been recognized that food insecurity has implications extending beyond monetary resources. In particular, food insecurity has been deemed a key social determinant of health (Gottlieb et al., 2019; Hawkins and Panzera, 2021), as being food insecure has been linked to poorer self-rated health and increased risk of developing chronic health conditions such as diabetes (Drakoulidou et al., 2020; Gucciardi et al., 2009; Leung et al., 2020). Experiencing food insecurity has also been linked to poorer mental health outcomes, including: poorer perceived mental health; greater risk for anxiety, depression, and suicidality (Jessiman-Perreault and McIntyre, 2017; Nagata et al., 2019); and greater rates of psychopathologies such as mood, anxiety, and eating disorders (Davison and Kaplan, 2015; Hazzard et al., 2022). Given its associated adverse effects and its widespread prevalence in the general population, food insecurity is considered a public health issue in Canada (Tarasuk and Mitchell, 2020).
Body dissatisfaction and food insecurity
Another factor related to health is body image, which is a multidimensional construct encompassing how a person experiences their physical appearance and related functioning via self-perceptions and self-attitudes (Cash, 2004, 2012). A person will cognitively and affectively evaluate aspects of their appearance, such as size and shape, and these evaluations result in specific attitudes toward, and perceptions of, their body (Cash, 2012; Smolak, 2006). When these self-evaluations are negative, this is referred to as body dissatisfaction (Baker et al., 2019).
As is the case with experiencing food insecurity, experiencing body dissatisfaction has adverse implications for one’s well-being. Namely, body dissatisfaction is associated with poorer physical health-related quality of life (Griffiths et al., 2016; Wilson et al., 2013), as well as greater levels of psychological distress (Griffiths et al., 2016), anxiety, depression (Barnes et al., 2020), disordered eating (Cruz-Sáez et al., 2020), and eating disorders (Polivy and Herman, 2002). Importantly, not only do food insecurity and body dissatisfaction both have implications for health, but these factors may co-occur at a rate greater than chance. Palmer et al. (2011), in a sample of HIV-positive persons in British Columbia, reported that people who reported positive body image were less likely to be food insecure, and Soulliard et al. (2022) found that among a sample of sexual minority men in Los Angeles, food insecurity was correlated with a greater prevalence of body image concerns. Additionally, food insecurity was linked to a greater risk for body dissatisfaction among a sample of children in California (Altman et al., 2018) and a sample of adolescents in Catalonia (Shankar-Krishnan et al., 2021). Notably, one published study did not find a significant association between food insecurity and body dissatisfaction, using a sample of African American families in Baltimore (Vedovato et al., 2016). Importantly however, the study’s sample was comprised solely of individuals living in low-income neighborhoods, and thus the sample may have lacked sufficient variability in levels of food insecurity to detect differences in body image. This single finding also has unclear implications for the general picture that is emerging from the literature, which seems to support the notion that food insecurity is a predictor of negative body image. Moreover, within the small body of literature examining food insecurity and body dissatisfaction, there has yet to be an investigation using a general sample of Canadians. In other words, we lack an examination of this relationship using a representative sample at the population level.
Why may food insecurity and body dissatisfaction be connected?
This association between food insecurity and body dissatisfaction may come about through several different mechanisms. One explanation is via weight status. Being food insecure has been linked to having a higher-weight body 1 (Domingo et al., 2021; Pruitt et al., 2016), which could owe to factors such as people who are food insecure consuming low-cost diets which are more calorie dense and are of lower nutritional value, resulting in higher weight status (Drewnowski and Darmon, 2005). Having a body of a higher weight is predictive of experiencing weight discrimination (Spahlholz et al., 2016) and the internalization of weight stigma (Puhl and Suh, 2015), both of which are associated with greater body dissatisfaction, as well as lower self-esteem and more negative mental health symptoms (Harriger and Thompson, 2012; Puhl and Suh, 2015).
The Tripartite Influence Model posits that one’s perception of body ideals or norms is shaped through distinct sociocultural influences: parents, peers, and media (Thompson et al., 1999; Tiggemann, 2011, 2012). Body dissatisfaction occurs when the internalization and social comparison of societal beauty ideals negatively influence one’s self-perception of their own bodies; in other words, it occurs one does not perceive themselves to meet the standards as set by society (Tiggemann, 2012). If we were to consider food insecurity in the context of the Tripartite Influence Model, it could be argued that sociocultural influences are likely comparable across levels of food security/insecurity; in other words, individuals experiencing food insecurity likely face the same societal standards for body ideals as those who are not food insecure (e.g. the “thin ideal” within Western society; Thompson et al., 1999). However, it is what can be done to achieve these ideals that likely differs between people who are food insecure and those who are food insecure. Specifically, people who are food insecure likely face more barriers to achieving societal body norms/ideals, such as having limited choices in food options due to having limited financial resources and not being able to afford services such as gym membership programs (Winter et al., 2021). Because of these additional barriers, people who are food insecure may be limited in their ability to make desired changes to their bodies to meet societal beauty standards, such as losing weight through following a diet and exercise regimen.
Importantly, food insecurity and body image share several risk factors, making their association challenging to disentangle. For example, both food insecurity and body dissatisfaction have been shown to be linked to sex (Griffiths et al., 2016; Walker et al., 2021), racial/ethnic identity (Frederick et al., 2022; Tarasuk et al., 2019), and socioeconomic status (SES; McLaren and Gauvin, 2002; Palmeira et al., 2019). Importantly, although food insecurity is strongly associated with low SES/poverty (Vozoris and Tarasuk, 2003), not all people experiencing food insecurity also experience poverty (Coleman-Jensen et al., 2017). Findings from the literature also suggest that food insecurity is associated with adverse effects independent of measures of SES (e.g. income, education; Tarasuk et al., 2019); therefore, even in cases where both food insecurity and poverty are present, the effects of food insecurity on body image likely extend beyond the effects of SES alone.
Exploring assigned sex as an effect modifier
As noted above, a point of overlap between food insecurity and body image is sex. Just as females are more likely to experience food insecurity, they are also more likely to experience body dissatisfaction (Fernández-Bustos et al., 2019; Fiske et al., 2014). The Tripartite Influence Model, posits that body dissatisfaction occurs when one does not feel they have met society’s ideals/norms (Tiggemann, 2012), meaning one’s (dis)satisfaction with their body is inextricably linked to the gendered/sexualized body standards that are present in society (Thompson et al., 1999; Tiggemann, 2011, 2012). Therefore, females are faced with an exceptional risk due to significant societal emphasis on female beauty standards, frequent exposure to unrealistic standards through media, and frequent objectification of female bodies in media (Frederick et al., 2015; Thompson et al., 1999). We would be remiss not to mention that although this model represents a psychosocial framework, we are not stating that sex is a psychosocial construct. Rather, to put it plainly, persons of all sexes live in a society that upholds beauty standards or expectations for people who look like them, which impact individuals of different sexes in unique ways.
Notably, rates of both food insecurity and body dissatisfaction vary by sex, such that females are at greater risk of experiencing both than their male counterparts. Given this, it is plausible that the association between food insecurity and body dissatisfaction may also vary by sex. In other words, the food insecurity-body image association may differ in terms of magnitude and/or directionality when comparing individuals of different sexes. This has yet to be examined in the current literature, and thus the exact nature of this supposed moderated effect (e.g. whether the association between food insecurity and body dissatisfaction is larger among females than males, whether the association differs in direction between males and females, etc.) is unclear.
The current study
We seek to address the research gaps in the current literature. Although some researchers have linked food insecurity to body dissatisfaction, this association has yet to be studied in a provincially representative sample of Canadians. Previous studies have generally relied on small, non-random samples, which affects the extent to which the results can be generalized to the broader population. Examining a random sample of Canadians allows for results that can be applied to a larger population. Further, while sex has been identified as a common correlate between food insecurity and body image, no study to date has examined whether sex-based differences exist in the association between food insecurity and body dissatisfaction.
The first research objective is to examine the association between food insecurity and body dissatisfaction in Canadian adults. We use representative data from four Canadian regions (i.e. Nova Scotia, Quebec, Alberta, and Yukon). We hypothesize that individuals who are food insecure will be less satisfied with their bodies (i.e. will experience greater body dissatisfaction) relative to individuals who are not food insecure. The second research objective is to examine whether sex assigned at birth will modify the association between food insecurity and body dissatisfaction. As this is a novel area of exploration, our hypotheses are exploratory in nature. Our study did not require ethics clearance, as per Section 2.2 of the Tri-Council Policy Statement, we accessed pre-existing, publicly available data.
Method
Data
The current study used secondary data from the 2017 to 2018 cycle of the Canadian Community Health Survey (CCHS)—Annual Component. The CCHS is a cross-sectional survey that collects information on the health status, health determinants, and healthcare utilization of Canadians by surveying a large sample of respondents from the general population (Statistics Canada, 2019). The survey is representative of almost 98.0% of Canadians aged 12 years or older; its coverage excludes peoples living on reserves and other Indigenous settlements, full-time members of the Canadian Forces, youth living in foster homes, individuals who are institutionalized, and persons living in Nunavik and Terres-Cries-de-la-Baie-James in Quebec (Statistics Canada, 2019). Data for the 2017–2018 cycle were collected using both telephone and personal interviews (Statistics Canada, 2019). A total of 105,049 adults responded to the survey (adult response rate = 61.5%); however, not all CCHS respondents were asked or answered all questions relevant to the present study. The descriptive statistics for the current study’s sample (N = 33,515) are presented in Table 1, by the absence or presence of food insecurity (i.e. food secure or food insecure). Of the total sample, 6.6% of respondents (N = 2215) were classified as being food insecure. Moreover, a correlation matrix was used to assess the associations between all variables examined in the current study (see Table 2).
Weighted means/SDs or percentages for all variables, for the full sample and by food security status, and weighted group comparisons.
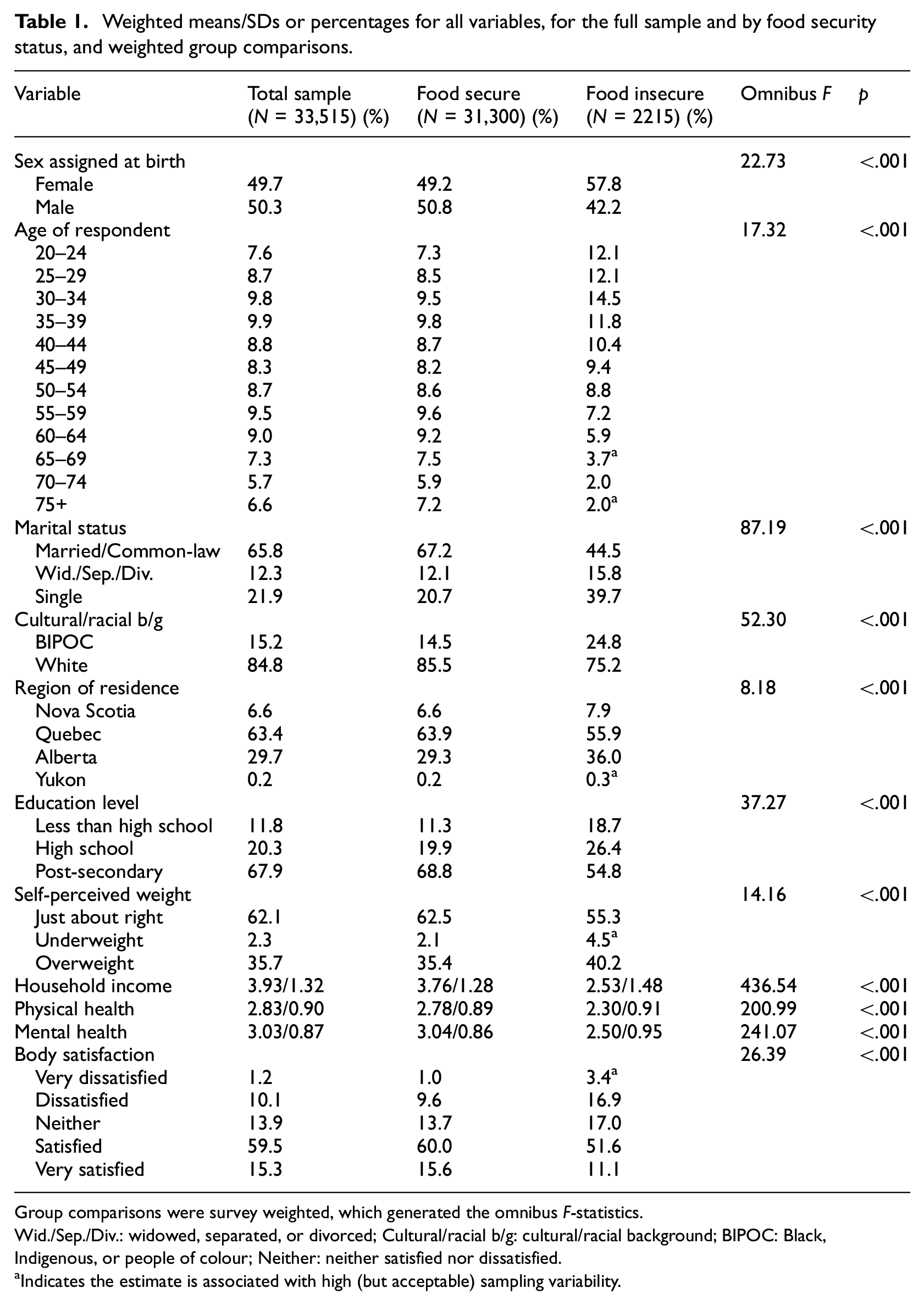
Group comparisons were survey weighted, which generated the omnibus F-statistics.
Wid./Sep./Div.: widowed, separated, or divorced; Cultural/racial b/g: cultural/racial background; BIPOC: Black, Indigenous, or people of colour; Neither: neither satisfied nor dissatisfied.
Indicates the estimate is associated with high (but acceptable) sampling variability.
Zero-order correlations for select variables.
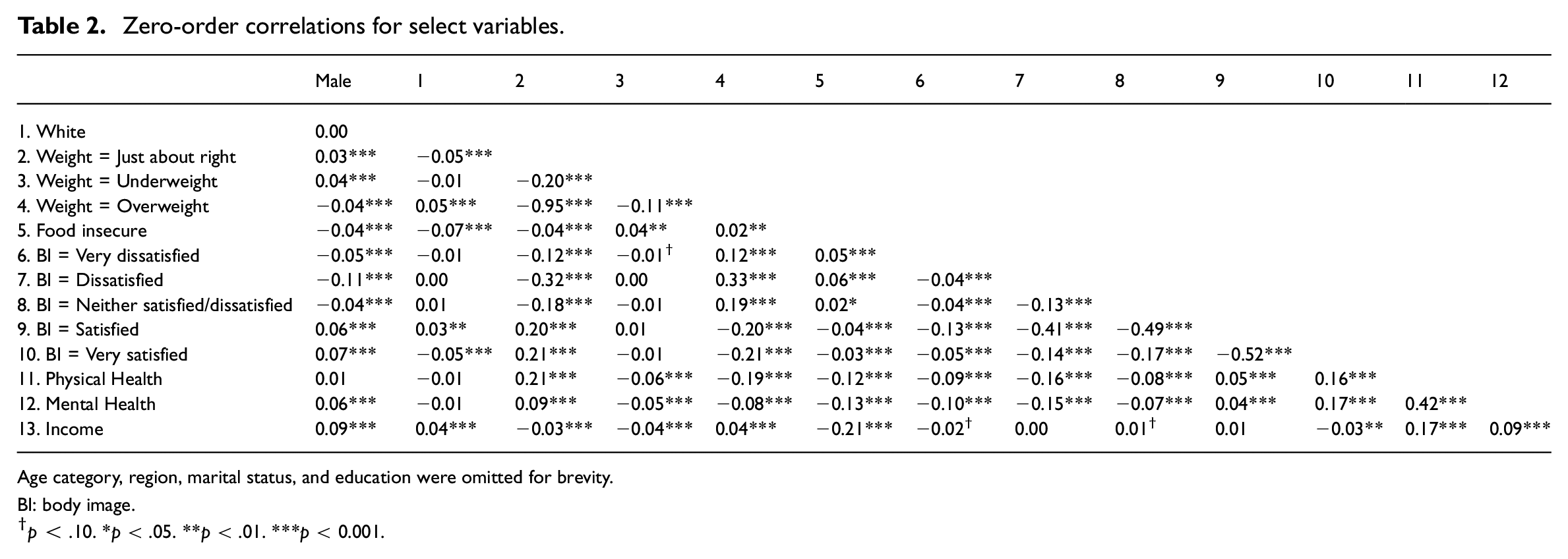
Age category, region, marital status, and education were omitted for brevity.
BI: body image.
p < .10. *p < .05. **p < .01. ***p < 0.001.
Measures
Demographic and control variables
To minimize confounding influences on the associations of interest, the present analysis controlled for the effects of several variables. This included participant demographic information, including age (measured in 5-year blocks; 20–24, 25–29, 30–34… 75+), marital status (married/common-law, widowed/separated/divorced, single), cultural/racial background (BIPOC, White), region of residence (Nova Scotia, Quebec, Alberta, Yukon), and education level (less than high school, high school, post-secondary). We also controlled for factors that have previously been identified as being related to food insecurity and/or body satisfaction, including self-perceived weight status (just about right, underweight, overweight), household income (units of $20,000), physical health as rated on a 5-point scale and recoded from 1 (Poor) to 5 (Excellent), and mental health as rated on a 5-point scale and recoded from 1 (Poor) to 5 (Excellent; Drakoulidou et al., 2020; Griffiths et al., 2016; Jessiman-Perreault and McIntyre, 2017).
Food Insecurity
To address the research objectives of interest, food insecurity was employed as the predictor variable. In the 2017–2018 CCHS, food insecurity was measured using Health Canada’s model, which used 10 questions to capture the relative food insecurity of the adult members of the respondent’s household. For example, respondents were asked “[You / You and other household members] worried that food would run out before you got money to buy more. Was that often true, sometimes true, or never true in the past 12 months?” and could respond with 1 (Often True), 2 (Sometimes True), or 3 (Never True). As another example, respondents were asked “In the past 12 months, since last [current month], did [you / you or other adults in your household] ever cut the size of your meals or skip meals because there wasn’t enough money for food?” and could respond with 1 (Yes) or 2 (No). Responses to all 10 items were then recoded as 0 (respondent did not provide a food insecurity-affirming response) and 1 (respondent did provide an affirming response) and were then summed. Based on their responses to the 10 questions, CCHS participants were coded into three levels: food secure (0 or 1 food insecurity-affirming response), moderately food insecure (2–5 food insecurity-affirming responses), and severely food insecure (6 or more food insecurity-affirming responses). However, to create consistency with operationalizations of food insecurity as presented in the current literature (e.g. Altman et al., 2018; Shankar-Krishnan et al., 2021) this variable was recoded as a binary in the current study, such that both levels of food insecurity (i.e. moderate and severe) were combined. In other words, participants in the current study were categorized as being either food secure (0 or 1 food insecurity-affirming response) or food insecure (2 or more food insecurity-affirming responses). This measure of food security was found to be reliable in the current study (Cronbach’s α = 0.99).
Sex assigned at birth
To investigate potential sex-based differences in the food insecurity-body image association, a binary measure of sex from the 2017 to 2018 CCHS was used as a moderator in the present analysis (female = reference, male). This variable was based on sex designation at birth, as reported by the CCHS participants. We acknowledge that this is an imperfect measure of sex, as it does not allow for continuity along the spectrum of possible categorizations (e.g. intersex). However, this was the only measure of sex provided by Statistics Canada for 2017–2018 CCHS and thus was the only variable available to examine sex differences in the present study.
Body satisfaction
A question about body satisfaction served as the outcome variable in the current study. Participants in the 2017-2018 CCHS were asked: “How satisfied are you with the way your body looks?” and provided their response on a 5-point rating scale. Valid responses were reverse coded in the current study such that lower ratings corresponded to lower satisfaction with one’s body (i.e. 1 = Very dissatisfied, 2 = Dissatisfied, 3 = Neither satisfied nor dissatisfied, 4 = Satisfied, and 5 = Very satisfied).
Data Analysis
All analyses were performed using Stata version 17 (StataCorp, 2021). A hierarchical generalized ordered logistic regression was performed to obtain all statistical values using the Stata user-written gologit2 program (Williams, 2016). Ordered logistic regression is an analytical regression method used to examine the association between predictors and an ordinal dependent variable (i.e. an outcome with ordered categories); however, given that the assumptions of such models are frequently violated, generalized ordered logistic regression presents as a less restrictive alternative (Williams, 2016). With generalized ordered logistic regression, the assumptions of the model are relaxed only as needed (Williams, 2016). The results of a generalized ordered logistic regression are similar to what would be produced by a series of binary logistic regressions (Williams, 2016). A pre-analysis check of the assumption of parallel lines was carried out, and this assumption was found to be violated for the following categories/variables: age 60–64 years, age 70–74 years, age 75+ years, widowed/separated/divorced, White cultural/racial background, household income, post-secondary education, underweight status, overweight status, physical health, mental health, and male sex designation. Conceptually, this means that the relationship that those variables had with body satisfaction were non-linear. Our models accounted for these changes by allowing those variables to have unique coefficients per level of the outcome variable, at the cost of degrees of freedom.
Person-level weights provided by Statistics Canada were applied to the model. The model progressed as follows:
In interpreting effect sizes, we follow the conventions described by Cohen (2013), where OR = 1.44 (OR = 0.70 for a negative association) is the cut-off for a small effect size, OR = 2.48 (OR = 0.40 for a negative association) is the cut-off for a medium effect, and OR = 4.27 (OR = 0.23 for a negative association) is the cut-off for a large effect.
Results
In Block 1, body satisfaction was regressed onto the demographic and control variables. Block 1 emerged as significant, indicating that the overall model was predictive of the outcome, ΔF(60,33,514) = 70.47, p < 0.001. Please note we have omitted the results of Block 1 from the regression table for the purposes of conciseness and clarity in our portrayal of the main analyses of interest.
In Block 2, food insecurity was entered, with the food secure group as the reference category, and the model again improved, ΔF(4, 34,825) = 5.59, p = 0.018. Being food insecure was associated with a lower likelihood of reporting a higher level of body satisfaction across all levels of the outcome variable, although this effect was of a trivial size, OR = 0.83, 95% CI [0.71, 0.97], t = −2.36, p = 0.018. Overall, the results of Block 2 generally suggested that relative to not being food insecure, being food insecure was associated with reduced odds of reporting greater body satisfaction.
In Block 3, assigned sex was added with female as the reference category, and the model again improved, ΔF(4,33,514) = 65.82, p < 0.001. Males were more likely to report a higher level of body satisfaction than: “Very dissatisfied,” OR = 2.28, 95% CI [2.02, 2.57], t = 13.46, p < 0.001; “Dissatisfied,” OR = 2.28, 95% CI [2.02, 2.57], t = 13.46, p < 0.001; “Neither satisfied nor dissatisfied,” OR = 1.83, 95% CI [1.68, 2.00], t = 13.26, p < 0.001; and “Satisfied,” OR = 1.43, 95% CI [1.30, 1.58], t = 7.04, p < 0.001. These were generally small-sized effects. Taken together, the results of Block 3 indicated that compared to females, males had greater odds of reporting greater body satisfaction, although this relationship appears more pronounced when comparing the lowest levels of body satisfaction to higher levels of body satisfaction. Notably, following the inclusion of sex in the model, food insecurity was no longer a significant predictor of body satisfaction.
In Block 4, the interaction between food insecurity and sex (i.e. food insecurity × male) was entered and did not improve the model, ΔF(1,33,514) = 0.07, p = 0.795. The interaction term was not statistically significant across all cut-points, OR = 0.96, 95% CI [0.70, 1.31], t = −0.26, p = 0.795. The results of Block 4 suggested that sex did not act as an effect modifier in the association between food insecurity and body satisfaction. To put it more plainly, the effects of sex and food insecurity were independent of one another (see Table 3 for details).
Prediction of body satisfaction by covariates (block 1, results omitted), food insecurity (block 2), sex (block 3), and the interaction of food insecurity and sex (block 4), using generalized hierarchical logistic regression.
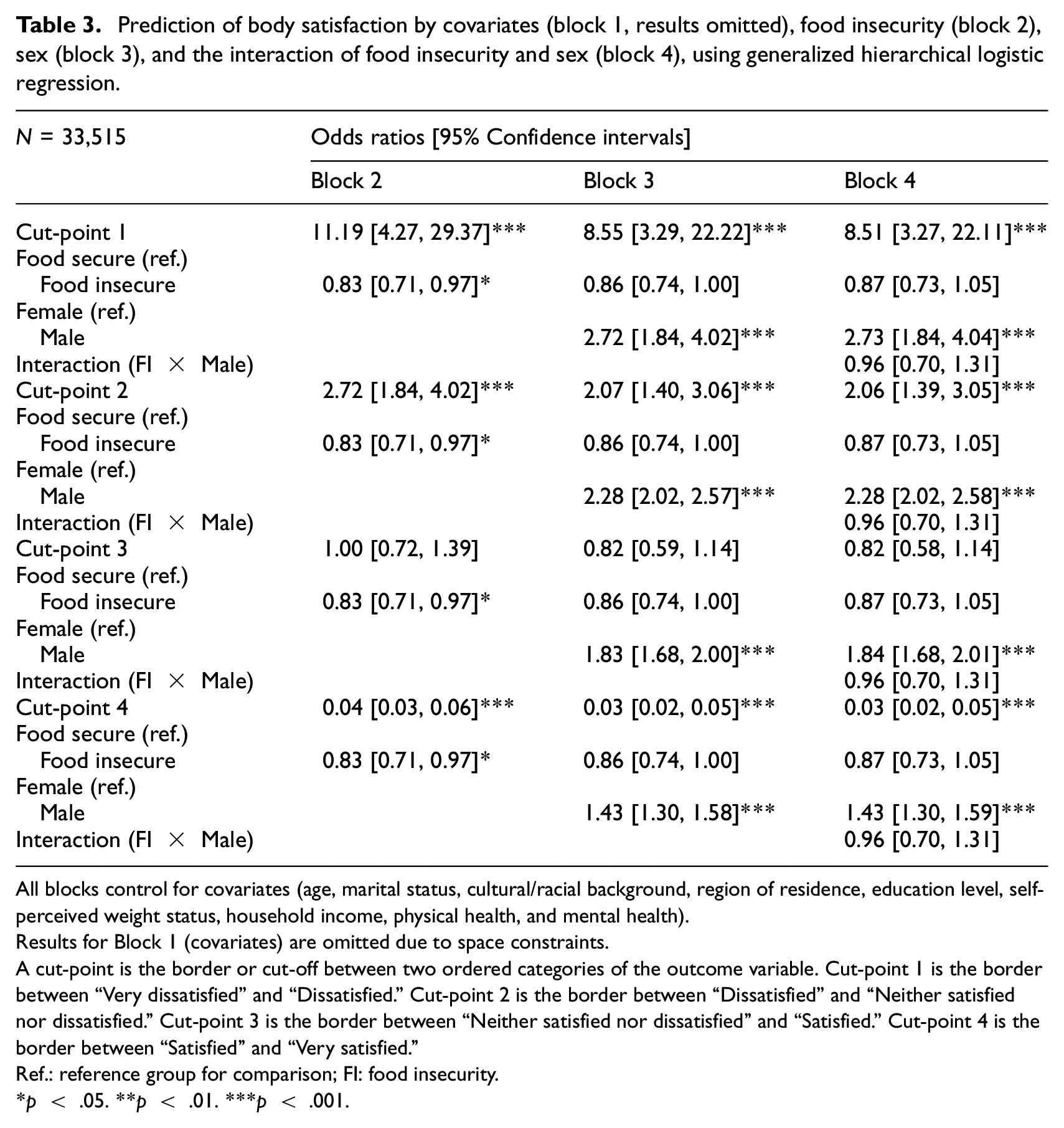
All blocks control for covariates (age, marital status, cultural/racial background, region of residence, education level, self-perceived weight status, household income, physical health, and mental health).
Results for Block 1 (covariates) are omitted due to space constraints.
A cut-point is the border or cut-off between two ordered categories of the outcome variable. Cut-point 1 is the border between “Very dissatisfied” and “Dissatisfied.” Cut-point 2 is the border between “Dissatisfied” and “Neither satisfied nor dissatisfied.” Cut-point 3 is the border between “Neither satisfied nor dissatisfied” and “Satisfied.” Cut-point 4 is the border between “Satisfied” and “Very satisfied.”
Ref.: reference group for comparison; FI: food insecurity.
p < .05. **p < .01. ***p < .001.
Discussion
The present study provides support to the growing body of literature on the association between food insecurity and body dissatisfaction. The current findings extend previous research to a large sample of Canadians, as being food insecure was predictive of lower body satisfaction. Interestingly however, the results indicate that after adjusting for sex assigned at birth, the effect of food insecurity on body dissatisfaction is no longer significant. Further, in a novel addition to the literature, the results of the present study indicate that sex did not modify the effect of food insecurity on body satisfaction. The implications of these various findings are discussed in detail below.
The effect of food insecurity
In support of our hypothesis, individuals who were food insecure were less likely to report greater body satisfaction compared to individuals who were not food insecure. As discussed previously, this association between food insecurity and body dissatisfaction may exist due to a shared connection via weight status, weight discrimination, and internalized weight stigma (Domingo et al., 2021; Puhl and Suh, 2015; Spahlholz et al., 2016), or due to the overlap in risk factors for food insecurity and body dissatisfaction such as SES and sex (Griffiths et al., 2016; McLaren and Gauvin, 2002; Palmeira et al., 2019; Walker et al., 2021). Alternatively, another explanation is one that proposed by Altman et al. (2018): experiencing food insecurity may make an individual more conscious of their body, and consequently, such an individual would be more prone to experiencing body dissatisfaction. In other words, being food insecure may affect how often a person thinks about or evaluates their own physical appearance, and a greater frequency of self-evaluations may put them at risk for experiencing negative attitudes/perceptions of their body. Although Altman et al. offered this explanation in regard to the food insecurity-body image link in children, it could be extended to examining food insecurity and body image in adults, as greater body surveillance has also been linked to body dissatisfaction in adult samples (Fitzsimmons-Craft et al., 2012, 2015; Mercurio and Rima, 2011).
Sex-based differences in body satisfaction
Under the Tripartite Influence Model, females are at a greater risk for body dissatisfaction (Frederick et al., 2015; Thompson et al., 1999). The findings of the current study offer support to the Tripartite Influence Model as serving to address sex-based differences in body satisfaction, as female respondents were found to be less likely to report higher levels of body satisfaction than their male counterparts (i.e. they were more likely to report being dissatisfied with their bodies).
No sex-based differences were found in the relationship between food insecurity and body dissatisfaction relationship. This lack of a moderated effect could owe to the effect of food insecurity on body satisfaction essentially being “lost” following the inclusion of assigned sex in the regression model (i.e. when added to the model, the effect of sex on body satisfaction suppressed the predictive power of food insecurity). Essentially, there was little effect left to be modified.
Limitations and strengths
The present study is not without limitations. Drawbacks relate to the use of cross-sectional secondary data: the sample is now several years old, and this limited the pool of useable variables and resulted in our inability to assess causality. In this vein, the data only described respondents from select provinces (i.e. Nova Scotia, Quebec, Alberta, and Yukon), and thus the results have unclear generalizability to the other regions of Canada. In addition, as discussed previously, the 2017–2018 CCHS included only a single-item measure of body satisfaction and only a binary measure of assigned sex. The survey also did not include a measure of gender identity/expression: as gender is a social construct, body satisfaction may be influenced more consistently within gender identities than within sex categorizations. However, our study had several strengths that ameliorate these deficits. In using secondary data, the researchers were able to carry out an investigation of the association between food insecurity and body image using a sample that was representative on a provincial level. Further, using survey data allowed for a large sample size with ample statistical power to examine between-groups differences across multiple levels of body satisfaction.
Future directions
Several avenues exist for further investigation within this area of research. For example, future work could examine gender as an effect modifier of the food insecurity-body dissatisfaction association, given that gender identity/expression can influence food insecurity (Hallward et al., 2023; Haskett et al., 2020) and body image (Goldhammer et al., 2019; Mofradidoost and Abolghasemi, 2020), and given that as a sociological variable, it may more readily lend itself to the framework of the Tripartite Influence Model. Moreover, food insecurity has been observed to demonstrate a gradient or dose-dependent effect on other mental health outcomes (Jones, 2017; Temple, 2008), such that greater levels of food insecurity are associated with a greater effect. Therefore, future studies could investigate the influence of food insecurity on body dissatisfaction while comparing different levels of food insecurity (e.g. moderate, severe) to establish whether the previously observed gradient effect extends to the exploration of body dissatisfaction.
Conclusion
The present findings add support to the growing body of literature asserting that experiencing food insecurity is predictive of experiencing body dissatisfaction, but only prior to controlling for sex-based differences in body dissatisfaction. Therefore, these findings highlight how the link between sex and food insecurity may serve a larger role in explaining body dissatisfaction than food insecurity alone. Further investigation is warranted to understand if, and how, food insecurity serves as a risk factor for body dissatisfaction. As experiencing either food insecurity or body dissatisfaction poses threat to physical and mental wellness (Barnes et al., 2020; Griffiths et al., 2016; Palmer et al., 2011; Vozoris and Tarasuk, 2003), it is crucial to not only address each of these issues in isolation, but also to understand their complex relation to one another and the implications for when these factors co-occur.
Footnotes
Authors’ note
Although the research and analysis are based on data from Statistics Canada, the opinions expressed do not represent the views of Statistics Canada. Any errors in recoding, analysis, or interpretation are the responsibility of the authors.
CRediT statement
Data sharing statement
The data that support the findings of this study are available from Statistics Canada. Interested researchers can access the public use microdata file from Statistics Canada.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethic approval
This study did not require ethics clearance, as per Section 2.2 of the Tri-Council Policy Statement, the authors accessed pre-existing, publicly available data.
Informed consent
Informed consent is not required.