
Abstract
Engagement in health-promoting behaviors has been argued to be dependent on psychological factors in addition to simply having knowledge or access to resources. We systematically reviewed the evidence for the association between body (dis)satisfaction and health screening behaviors using six electronic databases and supplementary manual searches in the current study. To be included in the review, studies had to be empirical, in any language, and examined the potential link between body (dis)satisfaction and health screening. Findings from the final 16 quantitative and 12 qualitative studies generally suggest that people who were more satisfied or less dissatisfied with their bodies were more likely to engage in health screening. This review also highlighted key gaps in the literature such as the limited studies that included men as participants and the lack of examination of the underlying mechanisms and contingencies of the relationship between body (dis)satisfaction and health screening behaviors.
Introduction
Health screening, which is a process aimed at identifying individuals who are at a higher risk of contracting or developing a specific disease to benefit from early intervention or treatment (World Health Organization, 2020), has been shown to lower disease mortality and reduce premature deaths (Stang and Jöckel, 2018). Despite national efforts in England and the United States to encourage participation in frequent health screenings, the engagement rate remains low (Harte et al., 2018; Smith et al., 2019). Given that raising awareness of the importance of screening and increasing their accessibility is insufficient to promote engagement, some researchers have turned their attention to the psychological predictors of health screening behaviors such as one’s evaluation of their body image (Ridolfi and Crowther, 2013). One evaluative component of body image is body dissatisfaction, which refers to one’s “negative thoughts and feelings about his or her own body” (Grogan, 2017: 4), and includes evaluations of (dis)satisfaction related to body size, shape, overall appearance, and body parts/areas. Because health screenings require the exposure of the physical body or the exposure of bodily information (McBride et al., 2019), such situations may heighten the salience of bodily-related concerns and fear of negative appearance-based evaluations (Cash et al., 2004) among those with more body dissatisfaction.
Indeed, studies have shown that individuals who are more satisfied with their body shape (Ludman et al., 2010) and appearance (Samah and Ahmadian, 2014) were more likely to engage in health screening. From their review of the literature on body image and cancer screening among women, Ridolfi and Crowther (2013) proposed that the association between body image evaluation and cancer screening behaviors may be explained by feelings of body shame and motivation to avoid the exposure of one’s body to oneself and others. These may represent strategies aimed to protect oneself from possible drops of their already impoverished evaluation of their body. Health screening behaviors require individuals to perform visual or tactile self-examinations of their body or have another person closely examine their body during clinical examinations. Thus, individuals with more body dissatisfaction may engage in fewer self-examinations to minimize confrontation with their source of dissatisfaction or shame, that is, their body, or avoid or delay clinical examinations to prevent negative evaluations from healthcare professionals (Mensinger et al., 2018; Swami and Furnham, 2018).
Nevertheless, findings on the association between body (dis)satisfaction and screening have been mixed. Andrew et al. (2016) found that body areas dissatisfaction predicted skin cancer screening but not breast cancer screening among female university students in Australia. Adams et al. (1993) found that adult women aged 40–65 years who evaluated their body more positively were more likely to have a past pelvic examination. However, this association was not found in a sample of breast cancer survivors (Katz et al., 2009). These findings suggest that the effect of body (dis)satisfaction may vary by the type of screening behaviors, as well as the age or health experiences of the participants. Indeed, Ridolfi and Crowther’s (2013) review of the literature has highlighted the roles of age, self-efficacy, subjective norms, risk perception, and health anxiety as potential attenuators of body dissatisfaction effects.
To the best of our knowledge, the only published review on the association between body image evaluation and screening behaviors (Ridolfi and Crowther, 2013) focused on cancer screening and women samples. A more thorough understanding of this association is essential, given the experience of body dissatisfaction across genders and ages (Frederick et al., 2007; Runfola et al., 2013), the lower uptake of screening among men (Davis et al., 2012), and evidence suggesting the relevance of body dissatisfaction in men’s health screening behaviors that are not cancer-specific (Ramseyer Winter et al., 2020).
Hence, the aim of this systematic review was to summarize the existing evidence on the role of body (dis)satisfaction in health screening behaviors following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Page et al., 2021) guidelines (Table S1). To this end, we searched for relevant studies to address the broad question of whether body (dis)satisfaction is associated with any health screening behaviors among individuals of any gender and age. We included studies that tested interventions as well as quantitative and qualitative observational studies.
Method
The protocol of this systematic review was registered with PROSPERO (CRD42021229840). The original protocol involved the broader construct of body image. However, because body image is multidimensional, the mechanisms that underlie its associations with health behaviors likely vary according to the different dimensions (Ramseyer Winter et al., 2020). Given our aim of searching for studies involving any health screening behavior, we decided to focus on one aspect of body image, that is, body (dis)satisfaction, and amended our original protocol accordingly.
Eligibility criteria
All quantitative and qualitative studies that were published up to 31 December 2021 and explored the possible association between body (dis)satisfaction and health screening were included. No language restriction was imposed. These steps were taken to ensure the records obtained were up to date at the time of search and to minimize selection bias due to the language of the journals. We excluded gray literature, conference proceedings, theses, non-peer-reviewed monographs, books and book chapters, study protocols, and studies that reported on body image or health screening tool development or validation. We focused the literature search on high-quality, peer-reviewed studies to reduce the risk of bias and ensure the reliability and rigor of studies included in our review.
Information sources and search strategy
We searched for peer-reviewed articles on the following databases: Ovid MEDLINE, PubMed, PsycINFO, EMBASE, and CINAHL+. The following combination of Medical Subject Heading (MeSH) terms and keywords was used: (“body image” OR “body dissatisfaction” OR “body satisfaction”) AND (“screening” OR “medical screening” OR “health screening” OR “medical examination” OR “physical examination” OR “screening test” OR “health check” OR “check up” OR” health examination” OR “health assessment” OR “clinical examination”). We then hand-searched the reference lists of the included articles for potentially relevant studies (see Table S2 for the complete search strategy).
Study selection
We imported the articles from the literature search to Covidence (Veritas Health Innovation, n.d.). After deleting duplicated records, we began a two-stage screening process. First, two reviewers (Authors 2 and 3) independently screened the titles and abstracts of all potential articles according to the eligibility criteria. Full texts were then retrieved for the articles that could not be excluded based on title or abstract, and further screened following the same criteria. A third reviewer (Author 4) resolved any conflict in the agreement between the two reviewers.
Data extraction and synthesis
The following data were extracted from each finalized article: citation, study design, country, target population, gender of study participants, age, sample size, body (dis)satisfaction measures, health screening behavior assessed, and main findings.
Quality assessment
The quality of the quantitative studies was assessed independently by two reviewers (Authors 2 and 4) using the National Institutes of Health Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies checklist (National Institutes of Health Quality, 2014). The overall quality was rated as poor (0–4), fair (5–7), or good (8–14). The qualitative studies were classified as “high,” “medium,” or “low” quality based on Critical Appraisal Skills Programme (2021; CASP) quality-assessment tool for qualitative studies. As the CASP checklist does not provide scores, we followed Bohren et al.’s (2014) approach to categorize the qualitative studies into “high,” “medium,” or “low” quality based on the evaluation of the two reviewers. A third reviewer (Author 1) acted as a conflict resolver.
Results
Study selection
We identified 2799 records through electronic database searches. After removing 1153 duplicates and screening by title and abstract, the full texts of 38 articles, which were all in English, were assessed for eligibility. Twenty-three full texts were excluded. Of these, 19 did not examine the association between body image and health screening and four were conference abstracts (Table S3). We found 15 articles via manual search and excluded two for duplicated reporting (Ahmadian et al., 2016; Wang et al., 2017). Hence, a final total of 28 unique studies was included in this review (see Figure 1).
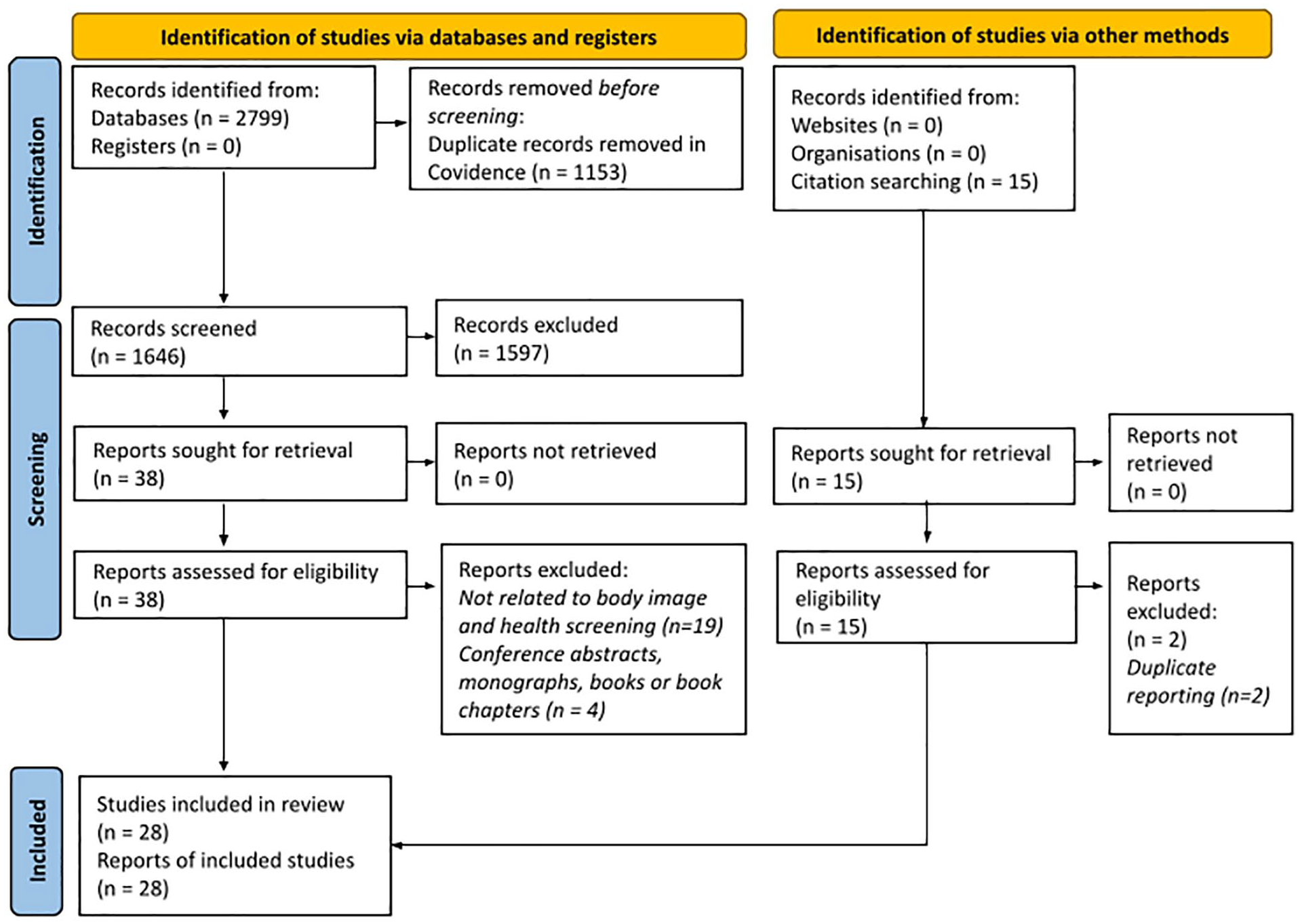
PRISMA 2020 flow chart showing the study selection process.
Study characteristics
Design of the studies
Of the 28 studies (See Table 1), 16 used quantitative methodologies, all of which relied on cross-sectional designs. The remaining 12 studies used qualitative methodologies, which mostly relied on loosely-structured or semi-structured interviews (Ellingson, 2003; Lende and Lachiondo, 2009; McBride et al., 2019; Russell and Carryer, 2013; Wang et al., 2018).
Studies included in the review (n = 28).
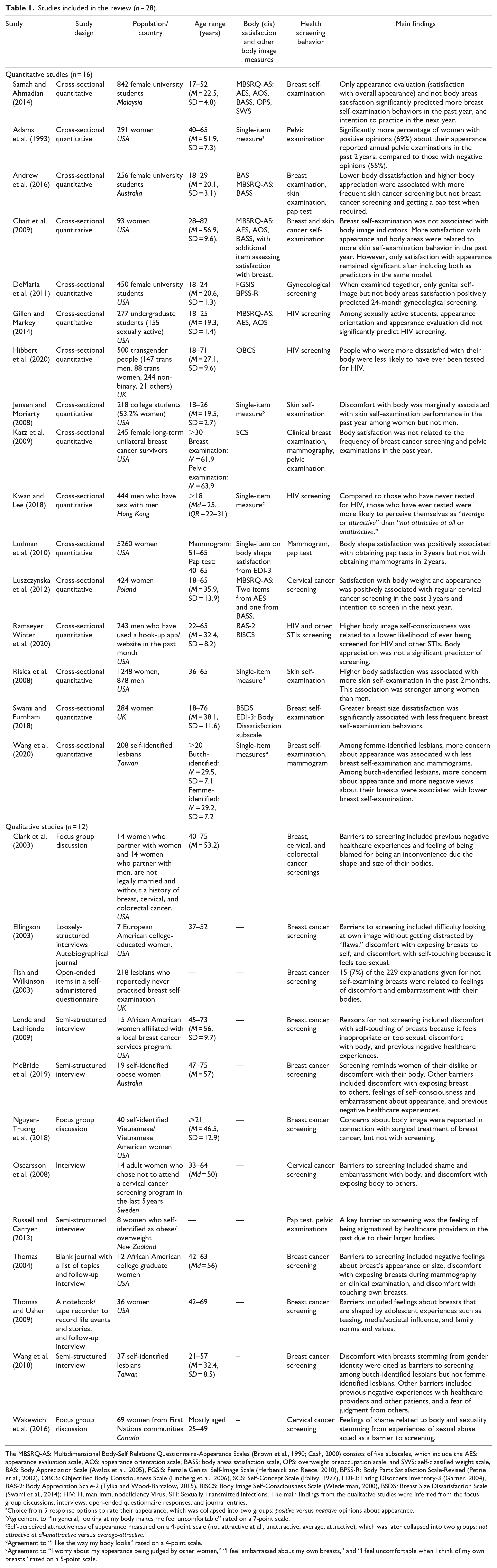
The MBSRQ-AS: Multidimensional Body-Self Relations Questionnaire-Appearance Scales (Brown et al., 1990; Cash, 2000) consists of five subscales, which include the AES: appearance evaluation scale, AOS: appearance orientation scale, BASS: body areas satisfaction scale, OPS: overweight preoccupation scale, and SWS: self-classified weight scale, BAS: Body Appreciation Scale (Avalos et al., 2005), FGSIS: Female Genital Self-Image Scale (Herbenick and Reece, 2010), BPSS-R: Body Parts Satisfaction Scale-Revised (Petrie et al., 2002), OBCS: Objectified Body Consciousness Scale (Lindberg et al., 2006), SCS: Self-Concept Scale (Polivy, 1977), EDI-3: Eating Disorders Inventory-3 (Garner, 2004), BAS-2: Body Appreciation Scale-2 (Tylka and Wood-Barcalow, 2015), BISCS: Body Image Self-Consciousness Scale (Wiederman, 2000), BSDS: Breast Size Dissatisfaction Scale (Swami et al., 2014); HIV: Human Immunodeficiency Virus; STI: Sexually Transmitted Infections. The main findings from the qualitative studies were inferred from the focus group discussions, interviews, open-ended questionnaire responses, and journal entries.
Choice from 5 response options to rate their appearance, which was collapsed into two groups: positive versus negative opinions about appearance.
Agreement to “In general, looking at my body makes me feel uncomfortable” rated on a 7-point scale.
Self-perceived attractiveness of appearance measured on a 4-point scale (not attractive at all, unattractive, average, attractive), which was later collapsed into two groups: not attractive at all-unattractive versus average-attractive.
Agreement to “I like the way my body looks” rated on a 4-point scale.
Agreement to “I worry about my appearance being judged by other women,” “I feel embarrassed about my own breasts,” and “I feel uncomfortable when I think of my own breasts” rated on a 5-point scale.
Samples
Most studies were conducted in the United States (n = 15; Adams et al., 1993; Chait et al., 2009; Clark et al., 2003; DeMaria et al., 2011; Ellingson, 2003; Gillen and Markey, 2014; Jensen and Moriarty, 2008; Katz et al., 2009; Lende and Lachiondo, 2009; Ludman et al., 2010; Nguyen-Truong et al., 2018; Ramseyer Winter et al., 2020; Risica et al., 2008; Thomas, 2004; Thomas and Usher, 2009), followed by the United Kingdom (n = 3; Fish and Wilkinson, 2003; Hibbert et al., 2020; Swami and Furnham, 2018). Only six studies did not examine women exclusively (Gillen and Markey, 2014; Hibbert et al., 2020; Jensen and Moriarty, 2008; Kwan and Lee, 2018; Ramseyer Winter et al., 2020; Risica et al., 2008). The sample size of the studies ranged from 93 to 5260 for quantitative studies and 7 to 218 for qualitative studies.
Quality assessment of studies
Of the quantitative studies, four (Hibbert et al., 2020; Katz et al., 2009; Luszczynska et al., 2012; Ramseyer Winter et al., 2020) were rated to be of good quality, 11 of fair quality (Andrew et al., 2016; Clark et al., 2009; DeMaria et al., 2011; Gillen and Markey, 2014; Jensen and Moriarty, 2008; Kwan and Lee, 2018; Ludman et al., 2010; Risica et al. 2008; Samah and Ahmadian, 2014; Swami and Furnham 2018; Wang et al., 2018), and one (Adams et al., 1993) of poor quality (see Table S4a). There was a 75% agreement rate in quality assessment between the reviewers.
Five qualitative (Clark et al., 2003; Lende and Lachiondo, 2009; Thomas, 2004; Wakewich et al., 2016; Wang et al., 2018) were rated to be of high quality, and only two (Ellingson, 2003; Russell and Carryer, 2013) were rated to be of poor quality. The remaining studies were of medium quality (Fish and Wilkinson, 2003; McBride et al, 2019; Nguyen-Truong et al, 2018; Oscarsson et al, 2008; Thomas and Usher, 2009; see Table S4b).
Assessment of body (dis)satisfaction
As shown in Table 1, ten measures were used to assess different aspects of body (dis)satisfaction in 11 studies while five studies (Adams et al., 1993; Jensen and Moriarty, 2008; Kwan and Lee, 2018; Risica et al., 2008; Wang et al., 2020) used self-developed single-item measures. The most used measure was the Multidimensional Body–Self Relations Questionnaire–Appearance Scales (MBSRQ-AS; Brown et al., 1990; Cash, 2000). One study used the complete MBSRQ-AS, which includes subscales that examine other dimensions of body image (Samah and Ahmadian, 2014), three used selected subscales (Andrew et al., 2016; Chait et al., 2009; Gillen and Markey, 2014), while one used only three items from MBSRQ-AS (Luszczynska et al., 2012). The body dissatisfaction subscale of the Eating Disorders Inventory-3 (Garner, 2004) was used in two studies. One used the entire subscale (Swami and Furnham, 2018) while another utilized an item from this subscale to capture body shape dissatisfaction (Ludman et al., 2010).
The most commonly assessed aspects of body (dis)satisfaction were satisfaction with overall physical appearance (n = 7; Adams et al., 1993; Chait et al., 2009; Gillen and Markey, 2014; Kwan and Lee, 2018; Luszczynska et al., 2012; Risica et al., 2008; Samah and Ahmadian, 2014) and overall body areas (n = 6; Andrew et al., 2016; Chait et al., 2009; DeMaria et al., 2011; Katz et al., 2009; Samah and Ahmadian, 2014; Swami and Furnham, 2018). Few studies examined (dis)satisfaction with specific body areas such as breasts (Chait et al., 2009; Swami and Furnham, 2018; Wang et al., 2020) and genitals (DeMaria et al., 2011). Other dimensions of body image that are not specific to body (dis)satisfaction, such as body appreciation (Andrew et al., 2016; Ramseyer Winter et al., 2020), appearance orientation (the extent to which one invests in their appearance; Chait et al., 2009; Gillen and Markey, 2014; Samah and Ahmadian, 2014), evaluation concerning body weight, size, or shape (Ludman et al., 2010; Samah and Ahmadian, 2014), feelings about how one’s body appears to others (Ramseyer Winter et al., 2020; Wang et al., 2020), and negative feelings when looking at one’s body (Jensen and Moriarty, 2008), were also examined. Hibbert et al. (2020) examined objectified body consciousness (McKinley and Hyde, 1996), which encapsulates elements of appearance evaluation, concerns about how one appears to others, and internalization of cultural standards of bodies.
Health screening behaviors assessed
The 28 studies included in this review assessed health screening behaviors that concern breast, cervical, skin, and colorectal cancers; Human Immunodeficiency Virus (HIV); other sexually transmitted infections (STIs); and gynecological examinations not specific to cervical cancer screening such as pelvic examinations. We combined cervical cancer screening and pelvic examinations in our reporting as some studies did not specify whether these gynecological examinations performed were specific to cervical cancer screening.
Breast cancer screening was the most assessed behavior (n = 16). Five studies captured breast self-examinations only (Chait et al., 2009; Ellingson, 2003; Fish and Wilkinson, 2003; Samah and Ahmadian, 2014; Swami and Furnham, 2018), five captured clinical examinations only (Clark et al., 2003; Katz et al., 2009; Ludman et al., 2010; McBride et al., 2019; Thomas and Usher, 2009), while six captured both (Andrew et al., 2016; Lende and Lachiondo, 2009; Nguyen-Truong et al., 2018; Thomas, 2004; Wang et al., 2018, 2020).
The second most assessed behavior was cervical cancer screening and other gynecological exams (n = 10; Adams et al., 1993; Andrew et al., 2016; Clark et al., 2003; DeMaria et al., 2011; Katz et al., 2009; Ludman et al., 2010; Luszczynska et al., 2012; Oscarsson et al., 2008; Russell and Carryer, 2013; Wakewich et al., 2020), which were solely clinical examinations. Four studies examined skin cancer screening, whereby three captured self-examinations only (Chait et al., 2009; Jensen and Moriarty, 2008; Risica et al., 2008) while the other combined self- and clinical examinations into one measure (Andrew et al., 2016). Four studies reported on HIV screening (Gillen and Markey, 2014; Hibbert et al., 2020; Kwan and Lee, 2018; Ramseyer Winter et al., 2020). Colorectal cancer (Clark et al., 2003) and other STIs screening (Ramseyer Winter et al., 2020) were the least assessed. The measures for HIV and other STIs screening did not differentiate between self and clinical examinations.
Association between body (dis)satisfaction and health screening
Breast cancer screening
Three out of the seven quantitative studies reviewed found significant associations between body (dis)satisfaction and breast screening behaviors. Of the three, two featured body dissatisfaction effects that were breast-specific: Women who were more dissatisfied (Swami and Furnham, 2018) or more embarrassed and uncomfortable with their breasts (Wang et al., 2020) were less likely to engage in self-examinations. The role of breast dissatisfaction as a barrier to screening was also highlighted in qualitative studies. Women tend to report discomfort in exposing and touching their breasts during examinations due to the high sexual or negative feelings that they attach to their breasts (Ellingson, 2003; Lende and Lachiondo, 2009; Thomas and Usher, 2009; Wang et al., 2018). Many of these feelings may have been shaped by socioculturally-cultivated norms and values (Lende and Lachiondo, 2009; Oscarsson et al., 2008; Thomas, 2004; Thomas and Usher, 2009; Wang et al., 2018), and adolescent experiences (Lende and Lachiondo, 2009; Thomas and Usher, 2009). Butch-identified lesbians, who prefer appearing more masculine, also report feelings of discomfort stemming from their gender identity and the disconnect that they feel between their body and breasts as reasons for avoiding clinical examinations (Fish and Wilkinson, 2003; Wang et al., 2018). The third quantitative study that found body (dis)satisfaction effects revealed that women who were less satisfied with their appearance reported fewer past behaviors and future intentions of breast self-examination (Samah and Ahmadian, 2014). Indeed, qualitative findings suggest that women with more body dissatisfaction may find it difficult to examine their body closely as it reminds them of their discomfort with and disliking of their body (Ellingson, 2003; McBride et al., 2019). Additionally, their fear of their appearance being judged by others may also exacerbate their avoidance of clinical examinations (Clark et al., 2003; Wang et al., 2018, 2020).
(Dis)satisfaction with other bodily attributes, such as overall body areas (Andrew et al., 2016; Chait et al., 2009; Katz et al., 2009; Samah and Ahmadian, 2014) and body shape (Ludman et al., 2010); and other body image indicators, such as the degree of investment in one’s appearance (Chait et al., 2009; Samah and Ahmadian, 2014) and weight-related concerns or perceptions (Samah and Ahmadian, 2014), did not predict breast cancer screening. Of the four quantitative studies that did not find any significant associations, most involved older participants (at least or on average 50 years old) and were not specific to self-examinations.
Cervical cancer screening and other gynecological examinations
Four out of the six quantitative studies that examined cervical cancer screening behaviors or other gynecological examinations found significant associations. More satisfaction with body shape (Ludman et al., 2010), body weight and appearance (Luszczynska et al., 2012), and genitals (DeMaria et al., 2011); and having a more positive opinion about one’s own appearance (Adams et al., 1993) were linked to more screening behaviors among American and Polish women. Among young Australian women, however, the frequency of pap tests did not vary by body areas satisfaction or appreciation (Andrew et al., 2016). Body areas satisfaction also did not predict past screening behaviors among breast cancer survivors (Katz et al., 2009).
Findings from qualitative studies suggest that some women avoid cervical cancer screening due to their reluctance to expose their body to another person. This reluctance is driven by negative feelings toward their body, which may stem from childhood physical abuse, a history of eating disorders, or aging (Oscarsson et al., 2008; Wakewich et al., 2016). Women, especially those who are obese, also avoid gynecological examinations because of their past negative experiences with healthcare providers that concern their physical appearance. These include comments or nonverbal behaviors that make patients feel like they are an inconvenience (Clark et al., 2003; Russell and Carryer, 2013), which eventually gets internalized as guilt and shame by some women (Clark et al., 2003).
Skin cancer screening
All four studies that examined skin cancer screening relied on quantitative methods. Higher satisfaction with overall body areas (Andrew et al., 2016; Chait et al., 2009), satisfaction with physical appearance (Chait et al., 2009; Risica et al., 2008), and body appreciation (Andrew et al., 2016) were linked to more frequent skin cancer screening in the past. Less discomfort with one’s body marginally predicted engagement in skin self-examination within the past year among women (Jensen and Moriarty, 2008). Both studies that included men and women in their sample found stronger correlations among women (Jensen and Moriarty, 2008; Risica et al., 2008).
HIV and STI screening
Three of four quantitative studies showed that body (dis)satisfaction was associated with ever having HIV and STI tests. Screening behaviors were more prevalent among transgender men and women with lower body dissatisfaction (Hibbert et al., 2020), men who have sex with men who perceived themselves to have an attractive appearance or a fit body (Kwan and Lee, 2018), and less bodily self-conscious men who “hook up” (Ramseyer Winter et al., 2020). Screening behavior did not vary by the degree to which men appreciated their body (Ramseyer Winter et al., 2020) and the degree to which undergraduate men and women were satisfied with or invested in their appearance (Gillen and Markey, 2014).
Colorectal cancer screening
Only one qualitative study reported body dissatisfaction concerns related to colorectal screening. Clark et al. (2003) found that women avoided screening because they felt blamed for their body shape or size and felt embarrassed about the preparation for the procedure.
Discussion
The current review collated existing findings from 16 quantitative and 12 qualitative studies on the association between body (dis)satisfaction and health screening behaviors. While the abovementioned association does not appear consistent across studies—likely because of the variability in the body (dis)satisfaction measures used, screening behaviors captured, and population characteristics—some key patterns were evident from the current review.
First, not all aspects of body (dis)satisfaction were related to health screening. Screening behaviors were most consistently shown to be associated with one’s satisfaction with physical appearance (Adams et al., 1993; Chait et al., 2009; Kwan and Lee, 2018; Luszczynska et al., 2012; Risica et al., 2008; Samah and Ahmadian, 2014) and not their overall satisfaction with body areas (Andrew et al., 2016; Chait et al., 2009; DeMaria et al., 2011; Katz et al., 2009; Samah and Ahmadian, 2014; Swami and Furnham, 2018). Skin cancer screening, which was mostly measured as self-examination, is the only screening behavior that was consistently associated with various measures of body (dis)satisfaction (Andrew et al., 2016; Chait et al., 2009; Jensen and Moriarty, 2008; Risica et al., 2008). As suggested by Andrew et al. and Chait et al., overall body dissatisfaction and skin cancer self-examination may be more closely linked because it relies on one’s visual inspection of all body parts rather than a confined area. In support, our review suggests that screenings that require the inspection of a specific body area may be better predicted by one’s dissatisfaction with that body area rather than overall body dissatisfaction: Women who were more satisfied with their genitals attended more gynecological examinations (DeMaria et al., 2011) and women who were more satisfied with their breast size self-examined their breasts more frequently (Swami and Furnham, 2018).
Second, current findings highlight the role of potential moderating variables in the association between body (dis)satisfaction and screening behaviors. The quantitative studies that found significant associations between body dissatisfaction and breast examinations were generally conducted with younger participants. Older women may be more likely to include clinical breast cancer screening as part of their routine medical check-ups than younger women, given the higher risk of breast cancer with age (Siegel et al., 2022). The opposite pattern was found in cervical cancer and gynecological screening. Following the same argument, younger women may be more motivated to seek routine pap tests regardless of their feelings about their body because of the higher prevalence of human papillomavirus infections among young adults (Sargent et al., 2008). Taken together, these findings suggest that increases in screening behavior due to age-related needs, risks, or norms could weaken the effects of body dissatisfaction (Ridolfi and Crowther, 2013).
Only two of the four studies conducted with more than one gender examined how the correlation between body dissatisfaction and screening behavior varied by gender (Jensen and Moriarty, 2008; Risica et al., 2008). Both found a stronger correlation for women than men, which may be driven by women’s stronger prioritization of appearance (Quittkat et al., 2019) or higher uptake of screening (Davis et al., 2012). Our finding that body (dis)satisfaction was shown to be a more consistent predictor of breast self-examinations than clinical examinations suggests the role of examination type as a potential moderator. The effect of body (dis)satisfaction effect may be weaker in clinical examinations as they tend to be performed as routine checks and do not require one to confront their own body. However, we refrain from forming conclusions based on these limited studies and urge future researchers to further test the potential role of age, gender, and examination type as moderators of the association between body (dis)satisfaction and health screening behaviors.
None of the quantitative studies directly tested the possible mechanisms or mediating pathways underlying the body dissatisfaction and screening association. Nevertheless, qualitative findings suggest a few possible pathways. People who view their body more negatively may be more likely to encounter or recall negative interpersonal experiences such as stigmatization from service providers (Russell and Carryer, 2013) or other patients (Wang et al., 2018) when seeking healthcare. Over time, these feelings may develop into a generalized fear of negative evaluation from others (Cash et al., 2004) or feelings of stress related to healthcare encounters, which in turn predicts higher healthcare avoidance (Mensinger et al., 2018). Moreover, people who are less satisfied with their appearance may not want to confront their source of dissatisfaction, which may develop into a motivation to avoid their body. This motivation may manifest behaviorally as avoidance of body exposure (Ridolfi and Crowther, 2013), which could explain the link between body dissatisfaction and screening behaviors that require close examination of their body. Additionally, the avoidance motivation may manifest cognitively as reduced attention to bodily health and functioning (Fish and Wilkinson, 2003), which could explain the link between body dissatisfaction and screening behaviors that do not require bodily exposure such as HIV screening. Future work should empirically examine these potential mechanisms using longitudinal observational designs or experimental methods.
Among the quantitative studies included in this review, only five tested other dimensions of body image in addition to body (dis)satisfaction. Weight-related concerns and investment in appearance did not emerge as significant predictors of health screening (Chait et al., 2009; Gillen and Markey, 2014; Samah and Ahmadian, 2014). Two studies (Andrew et al., 2016; Ramseyer Winter et al., 2020) examined the role of body appreciation, which captures the degree to which one loves, accepts, appreciates, and respects their body’s unique beauty and functionality (Tylka and Wood-Barcalow, 2015), and findings were mixed. However, it is important to note that conclusions on the role of these other dimensions of body image cannot be made given that this was not the purpose of this review and we have not fully captured the studies that have examined body image constructs other than body dissatisfaction.
Implications
Overall, the current review extends on Ridolfi and Crowther’s (2013) findings by demonstrating the relevance of body (dis)satisfaction on screening behaviors beyond cancer screenings and among men. Our findings suggest the possible superior roles of the dissatisfaction with one’s overall appearance and body areas that are specific to the health screening as predictors, elaborated on the potential mechanisms underlying the body dissatisfaction and health screening association, and highlight the lack of experimental studies.
Our review also provides further evidence to support the incorporation of body image promotion goals in health interventions such as public health campaigns. Rather than highlighting the deadliness of diseases, which may increase avoidance of screening behaviors due to fear of illness detection (Ellingson, 2003; McBride et al., 2019), it may be more beneficial to incorporate messages or tasks that promote satisfaction with one’s appearance or a healthy relationship with one’s body, while promoting health literacy (Baccolini et al., 2022). More importantly, healthcare providers need to create a safe, stigma-free, and accepting environment for patients. Good provider-patient relationships need to be cultivated as healthcare provider recommendation is a key predictor of preventive health behaviors such as cancer screening (Rollet et al., 2021) and vaccine uptake (Oh et al., 2021). Healthcare-related policymakers and stakeholders could provide sensitivity and communication training to practitioners, which could be reinforced through service evaluations and improvements.
Limitations
Some limitations in the published literature are evident. First, the studies were predominantly done with women and people of Western cultures, which may challenge the generalizability of the findings. For instance, body dissatisfaction may not be a meaningful predictor of screening behaviors among populations with lower health literacy or poorer healthcare access. All studies relied on cross-sectional designs and examined physical health screening behaviors that were mostly related to cancer. There was a lack of standardization in body dissatisfaction and health screening measures. Future studies should account for the multiple aspects of body (dis)satisfaction (i.e. overall appearance and body areas to be screened) as well as the multidimensional nature of body image (i.e. capturing both negative and positive body image) using validated measures, utilize more comprehensive measures of health screening behaviors, and examine other screening behaviors such as psychological or mental health screening.
Moreover, our search was restricted to peer-reviewed journals, and grey literature was excluded from the search. Although efforts were made to search for related articles manually, it is possible that some publications were missed. Our choice of keywords may have also limited our search results. For instance, we did not include more specific terms such as pap smear or prostate exam for medical screening and terms such as body shame and ideal body for body dissatisfaction. Nevertheless, our search strategy was based on similar keywords used in other reviews that concerned health screening (Hoffmann and Del Mar, 2017) and body dissatisfaction (McComb and Mills, 2020), and a preliminary search to verify our keywords.
Conclusion
In conclusion, the current review showed a relatively consistent relationship between several aspects of body (dis)satisfaction and physical health self- and clinical screening behaviors. People who were more dissatisfied with their physical appearance or specific body parts were less likely to engage in self- and clinical-examinations for screening purposes. Findings suggest that more research is required to understand which aspects of body (dis)satisfaction better predict the different forms of health screening, in which context, and through which underlying mechanisms.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053231189413 – Supplemental material for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies
Supplemental material, sj-docx-1-hpq-10.1177_13591053231189413 for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies by Pei Hwa Goh, Hoi Yan Loh, Ker Rou Chung and Amutha Ramadas in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053231189413 – Supplemental material for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies
Supplemental material, sj-docx-2-hpq-10.1177_13591053231189413 for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies by Pei Hwa Goh, Hoi Yan Loh, Ker Rou Chung and Amutha Ramadas in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053231189413 – Supplemental material for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies
Supplemental material, sj-docx-3-hpq-10.1177_13591053231189413 for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies by Pei Hwa Goh, Hoi Yan Loh, Ker Rou Chung and Amutha Ramadas in Journal of Health Psychology
Supplemental Material
sj-docx-4-hpq-10.1177_13591053231189413 – Supplemental material for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies
Supplemental material, sj-docx-4-hpq-10.1177_13591053231189413 for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies by Pei Hwa Goh, Hoi Yan Loh, Ker Rou Chung and Amutha Ramadas in Journal of Health Psychology
Supplemental Material
sj-docx-5-hpq-10.1177_13591053231189413 – Supplemental material for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies
Supplemental material, sj-docx-5-hpq-10.1177_13591053231189413 for Body (dis)satisfaction and health screening behaviors: A systematic review of observational studies by Pei Hwa Goh, Hoi Yan Loh, Ker Rou Chung and Amutha Ramadas in Journal of Health Psychology
Footnotes
Data sharing statement
All data generated or analysed during this systematic review are included in their entirety in this published article itself. Supplemental Material describing the analyses are available via the Sage Journals platform.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study did not involve primary data collection and was thus exempt from ethical review.
Pre-registration
The protocol of this systematic review was registered with PROSPERO (CRD42021229840). We amended the original protocol to focus on body (dis)satisfaction instead of the broader construct of body image.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.