
Abstract
The COVID-19 pandemic and associated public health measures have interrupted the daily routines of parents and children. The purpose of this study was to explore parents’ attitudes regarding their children’s play/sport during COVID-19. A secondary objective was to explore the influence of parent demographics and parent-reported physical activity levels and risk tolerance on these attitudes. Ontario parents of children aged 12 and younger completed an online survey (August—December 2020) that assessed their attitudes (grouped by support, safety and socialization-related attitudes; n = 14 items) regarding their child(ren)’s play/sport, their physical activity levels (n = 2 items), and demographic details (n = 16 items). Two open-ended items were used to gather a deeper understanding of attitudes. Parents’ tolerance for risk was measured via the validated Tolerance of Risk in Play Scale. Descriptive statistics were calculated to describe attitudes and risk tolerance. Least Absolute Shrinkage and Selection Operator regressions were conducted to examine factors influencing parents’ attitudes. Multiple linear models were computed using the identified predictors for each attitude category. Deductive content analysis was undertaken on open-ended responses. Participants (n = 819) reported the highest scores for safety-related attitude items (M = 3.54, SD = .63) followed by socialization and support, which all influenced attitudes regarding children’s play/sport (p < .05). Demographics and parents’ physical activity levels were identified as important predictors of parents’ attitudes. Qualitative data revealed that parents had mixed levels of comfort with respect to their children’s return to play/sport. Findings from this study reveal that increased support is needed to guide future play/sport decision-making.
Physical activity during childhood offers many health benefits (Carson et al., 2017; Timmons et al., 2012). Nonetheless, since the announcement of the SARS-CoV-2 Coronavirus Disease (COVID-19) on March 11, 2020 (World Health Organization, 2021), opportunities for children’s physical activity have largely changed (Moore et al., 2020; Nigg et al., 2021; Pelletier et al., 2021). Many countries imposed physical distancing rules and contact restrictions (e.g., maintain a distance of 2 m from others; World Health Organization, 2021), and while important to protect citizens, these public health measures limited children’s opportunities to engage in activity with peers outside of their household, which has been recognized to positively influence physical activity levels (Barkley et al., 2014). Furthermore, in Canadian provinces such as Ontario, these public health measures included restrictions of settings (e.g., schools, outdoor playgrounds, and sports facilities) that previously supported children’s physical activity participation (Government of Canada, 2021). These measures have remained in place for extended periods of time, with staggered phases of re-opening across Ontario depending on contextual factors (e.g., state and risk of transmission, positive cases; Government of Ontario, n.d.). More specifically, during the timeframe of this study, citizens across Ontario were in 1 of 3 of Ontario’s phases of re-opening dependent on their city of residence; these phases directed the types of activities that were permitted (Ontario Newsroom, n.d.). 1
As 2 years have passed since the onset of the pandemic (World Health Organization, 2021), studies exploring the influence of COVID-19 public health restrictions on children’s physical activity have transpired (Bates et al., 2020; Moore et al., 2020; Okely et al., 2021; Tandon et al., 2021; White et al., 2019). Most studies have identified decreases in children’s physical activity (Dunton et al., 2020; Medrano et al., 2021; Moore et al., 2020), including reduced higher intensity activity (e.g., moderate-to-vigorous physical activity [MVPA]; Tulchin-Francis et al., 2021), while some have shown no significant change (Okely et al., 2021). Furthermore, some research has highlighted a shift in children’s engagement in structured activities (e.g., sports participation) toward more unstructured or child-led play (e.g., outdoor free play; Dunton et al., 2020; Pelletier et al., 2021; Szpunar et al., 2021). However, findings are inconsistent and largely dependent on geographical location and community type (Mitra et al., 2020).
To date, factors found to be associated with increases in children’s physical activity during COVID-19 in Canada have included access to outdoor spaces (Szpunar et al., 2021), dog ownership (Moore et al., 2020), living in low-density areas (Mitra et al., 2020), and encouragement from parents/family members to engage in movement (Moore et al., 2020). Nevertheless, COVID-19 has required many to adapt the ways in which they get active (e.g., engaging at home or outdoors vs. at organized sport). This has revealed new barriers for parents such as financing new toys and activities, time constraints due to work from home and homeschooling demands, and lack of motivation (Szpunar et al., 2021).
Parent’s (including guardians) influence their children’s movement opportunities through role-modeling, providing encouragement, enrolling and paying for their children’s participation inclusive of registration and equipment fees, organizing their scheduling, and providing needed transportation (Gustafson & Rhodes, 2006; Rhodes et al., 2020; Strauss et al., 2018; Van Der Horst et al., 2007). Likewise, researchers have previously identified various demographic factors, including socioeconomic status and geographical location that influence parents’ ability to support children’s activity (Inchley et al., 2005; Smith et al., 2010). For example, Smith et al. (2010) identified cost and transport as notable barriers to supporting children’s movement, prior to a pandemic. Finally, a handful of studies have explored how parents’ risk tolerance impacts their children’s physical activity opportunities (Brussoni et al.,2021, 2018; Hilland, 2019; Jelleyman et al., 2019); for example, research has found that parental fears can diminish children’s opportunities to engage with risk (Jelleyman et al., 2019). This is an especially important consideration in the COVID-19 era.
Given the associated COVID-19 transmission risks that may be associated with allowing children to return to their pre-COVID-19 activities, some parents may be hesitant to do so. The purpose of this article was to explore parents’ attitudes regarding their children’s physical activities inclusive of play and sports during COVID-19 (e.g., as reported by participants during the timeframe of this study—August to December 2020). A secondary objective was to explore if demographic factors (e.g., housing type and the number of children) or parent-reported MVPA levels and risk tolerance influenced these attitudes. It was hypothesized that the re-opening of facilities that support physical activity would leave Ontario parents with a challenging dilemma regarding their child(ren)’s return (or not) to their previous physical activity-related programming and that parents’ attitudes would vary based on demographic and parent-reported MVPA and risk tolerance.
Impact Statement
This article assessed parents’ attitudes toward their children’s play/sport during the COVID-19 pandemic. Parent participants reported higher scores toward safety-related attitudes, when compared with support and socialization attitudes. Parents’ moderate-to-vigorous physical activity showed a positive, albeit nonsignificant association with safety and socialization-related attitudes.
Method
Study Design and Procedures
Return to Play, a repeated measures study that employed multiple online surveys (August—December 2020; survey 1 and August—December 2021; survey 2) using Qualtrics, assessed Ontario parents’ perspectives of their children’s (≤12 years) physical activity-related behaviors over the course of the pandemic as well as their plans for their children’s play/sport during various time points of COVID-19. The surveys asked parents to report on types of activities their child(ren) engaged in prior to COVID-19 (e.g., sports enrolled in, amount of time spent in these activities per week), spaces that children engaged in play/sport prior to and during COVID-19 (e.g., at home, at sports facility, and gyms), amount of time children spent engaged in physical activity prior to the pandemic, and parents’ perceptions of changes in their children’s physical activity levels. This article presents cross-sectional findings from Survey 1 (e.g., baseline; August—December 2020). Ethical approval was provided by the Non-Medical Research Ethics Board at the University of Western Ontario (REB #116331).
Recruitment and Participants
English-proficient parents living in Ontario with children aged 12 years or younger (at the time of the first survey; with custody at least 50% of the time) were invited to participate. Recruitment took place using various social media platforms (e.g., Twitter), where infographics with study details (e.g., eligibility criteria, principal investigators’ contact details) were shared. In addition, various sport and physical activity organizations across Ontario were contacted and invited to circulate study details to their respective communities. Upon confirming their eligibility, participants were directed to the survey, the completion of which indicated their consent to participate.
Instruments and Tools
The online survey (Survey #1) was created by the research team to address the overarching objectives of the Return to Play study. Survey items were informed by the COVID-19 situation in Ontario, Canada, at the time of survey creation and were tailored to encompass guidance from Ontario’s specific re-opening framework (as outlined in the summer of 2020). The baseline survey in its entirety contained 162 items; however, for the purpose of this article, a subset of 64 items across four sections (i.e., parents’ demographic characteristics [n = 16], parents’ MVPA levels prior to and during COVID-19 [n = 2], parents’ self-reported risk tolerance [n = 30], and their attitudes [n = 14] regarding their children’s play/sport programming) were examined. The validity and reliability of this study’s questionnaire have not been tested, apart from the Tolerance for Risk in Play Scale.
Demographic Questions
Demographic questions included parent age, number of children, the highest level of education, family situation (e.g., single parent, double parent), approximate yearly household income, and employment status.
Parent-Reported Physical Activity
Parent’s MVPA levels prior to and during COVID-19 were assessed via multiple-choice format (e.g., how many minutes per week did you spend engaged in moderate-to-vigorous, heart-pumping activity prior to COVID-19?). Parents were given 5 response options ranging from less than 30 minutes per week to more than 150 minutes per week.
Attitude Questions
Reported on a 5-point Likert-type scale (i.e., 1—strongly disagree to 5—strongly agree), parents were asked 14 questions about their comfort and beliefs (i.e., attitudes) regarding their child(ren)’s eventual return to various forms of play and sport during COVID-19 (e.g., I feel willing to return my child to active play opportunities where they can follow physical distancing guidelines). For analysis, attitude items were grouped into three thematic categories: support-related attitudes (items regarding parents’ skills and access to resources that support children’s play while at home during COVID-19; n = 6 items); safety-related attitudes (items pertaining to physical distancing and overall perceived safety either at home or at play/sport environments; n = 5 items); and socialization-related attitudes, items concerning their child(ren)’s socialization as a result of COVID-19; n = 3 items. Means and standard deviations were computed for each individual attitude, and a total mean score for each of the three attitude groups was computed.
Two-open ended questions were included to allow participants to share more in-depth responses, that is, “Please describe the reasons you do or do not feel comfortable with the idea of your child(ren) returning to their active play/sports activities that they engaged in prior to COVID-19”; “To help increase our understanding, please explain your plan to return your child(ren) to their active play/sport programming (e.g., how you are [or not] planning to return your child(ren) to activities they engaged in prior to COVID-19).”
Tolerance of Risk in Play Scale
A modified version (i.e., 30 of 32 items) of the Tolerance of Risk in Play Scale (TRiPS; Hill & Bundy, 2014) was included at the end of the survey to assess parents’ self-reported risk tolerance for engaging children in various types of play (e.g., playing outdoors while unsupervised). Two items from the scale were removed as they were not appropriate for the age group (i.e., some parents responding for children under 3 years of age). This valid and reliable survey (i.e., Pearson reliability index of 0.87) was originally developed to assess adults’ tolerance for outdoor risky play among children aged 3 to 13 years (Hill & Bundy, 2014), and its psychometric properties have been previously demonstrated with parents and elementary school teachers as respondents (Brussoni et al., 2018). The first item of the tool asks participants, “How often do you encourage everyday risks?” with four response options, ranging from “never” to “often,” while all remaining items provide a “yes” or “no” response. Raw scores were collected (i.e., yes = 1; no = 0), and per the tool creator’s recommendation, a higher total score indicating greater tolerance for risk during children’s play.
Data Preparation and Analysis
Descriptive statistics were used to report parent demographics and risk tolerance and were computed in SPSS (version 27). All other data preparation (i.e., data cleaning) and analyses were computed using R statistical software, version 3.6.1 (R Core Team, 2019). Survey responses with more than 15% missingness (i.e., incomplete data) were removed (Li et al., 2020). A self-defined function was employed to insert median values in instances where a small number of participants did not complete a demographic question (e.g., provided parent age but not ethnicity), and imputation methods were applied to address variables with high levels of missing data using the K Nearest Neighbor (KNN) algorithm (Zhang, 2016). Because some parents provided responses for multiple children, children’s biological sex and age were concluded across families to provide family indices.
Three Least Absolute Shrinkage and Selection Operator (LASSO) regressions (one for each attitude category) were conducted to identify whether demographic and/or parent-reported physical activity and risk tolerance influenced parents’ attitudes regarding their children’s play/sport during and following COVID-19. LASSO regressions reduce unstable estimates to zero to exclude variables without the need for formal statistical testing and are frequently used when a large number of covariates need to be considered (Steyerberg et al., 2001). Once predictors were identified from the LASSO regression, multiple linear models (R package “lmtest”) were computed for each attitude category; however, upon visual inspection of the QQ plots for safety and socialization-related models, nonappropriate shapes were observed and the Shapiro tests reported very small p values (p = 1.80 and 1.90, respectively). Consequently, Box-Cox transformations (R package “EnvStats”; Millard & Kowarik, 2022) were undertaken to improve the linear models and normalize the residuals to increase the applicability and usefulness of the data for the safety and socialization models (Teugels & Vanroelen, 2004). Parameter lambdas (λ) were set to 2 based on minimizing the log-likelihood of potential models for the safety and socialization-related attitude models. F-tests were used to identify if categorical variables were significant. The two open-ended questions were analyzed via deductive content analysis (Kyngäs & Kaakinen, 2020) by two independent researchers using QSR NVivo (Version 12), and common responses were identified based on the questions asked (e.g., assessing plan to return and comfort to return; Anderson, 2010).
Results
A total of 819 parents, mean age of 38.1 (SD = 6.1) years, participated; the majority identified as female (93%), Caucasian (84%), lived in a detached house (77%), and had full-time employment (65%). Most parents (59%) had 2 or more children, and children were, on average, 6.5 (SD = 3.2) years of age, and most were reported to be female (69%). Participants most frequently (27.4%) reported spending less than 30 min/week in MVPA during the pandemic. The average risk tolerance score was 17.1 (SD = 5.1) out of 29, and most participants (56%) reported sometimes encouraging children’s everyday risks. See Table 1 for complete parent demographics, physical activity, and risk tolerance.
Parent (n = 819) Demographics, Self-Reported Physical Activity, and Risk Tolerance.
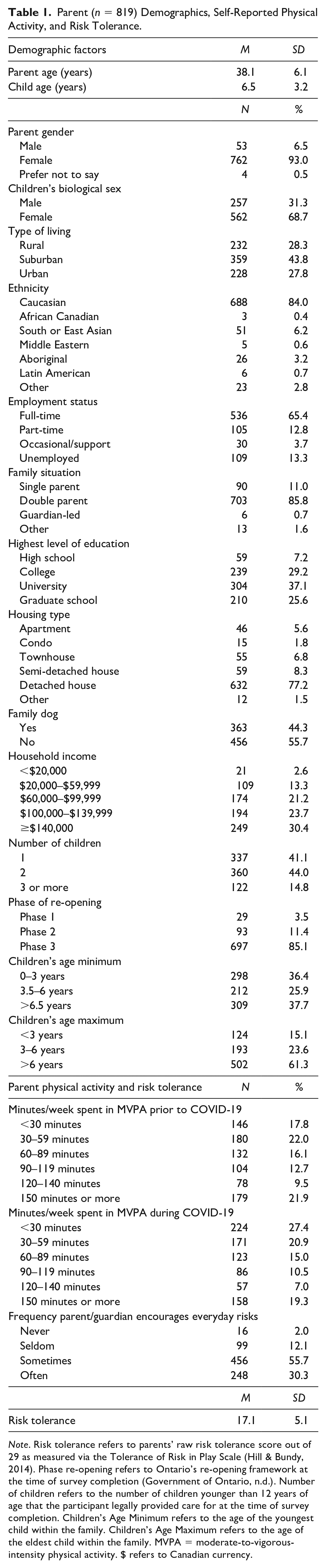
Note. Risk tolerance refers to parents’ raw risk tolerance score out of 29 as measured via the Tolerance of Risk in Play Scale (Hill & Bundy, 2014). Phase re-opening refers to Ontario’s re-opening framework at the time of survey completion (Government of Ontario, n.d.). Number of children refers to the number of children younger than 12 years of age that the participant legally provided care for at the time of survey completion. Children’s Age Minimum refers to the age of the youngest child within the family. Children’s Age Maximum refers to the age of the eldest child within the family. MVPA = moderate-to-vigorous-intensity physical activity. $ refers to Canadian currency.
Summary of Parents’ Support, Safety, and Socialization-Related Attitude Scores
Parents, on average, reported slightly higher attitudes to safety-related items (M = 3.54, SD = 0.63) compared to socialization- and support-related attitude items (M = 3.50, SD = 0.54; M = 3.30; SD = 0.82, respectively). With regard to individual attitude items, “I reserve time out of my day to support my child’s active play” was ranked highest (M = 3.89, SD = 1.09) in the support category; “I feel that having my child at home with me during the pandemic makes me feel safe” (M = 3.86, SD = 1.11) in the safety category; and “I am looking forward to allowing my child to interact with others” (M = 4.36, SD = 0.93) in the socialization category. Finally, a high score was noted for the socialization item, “I feel that my child has missed out on health benefits of extracurricular activities due to the COVID-19 pandemic” (M = 4.19; SD = 1.06). See Table 2 for support-, safety-, and socialization-related attitudes and total scores for each category.
Means and Standard Deviations for Parents’ Attitude Scores.
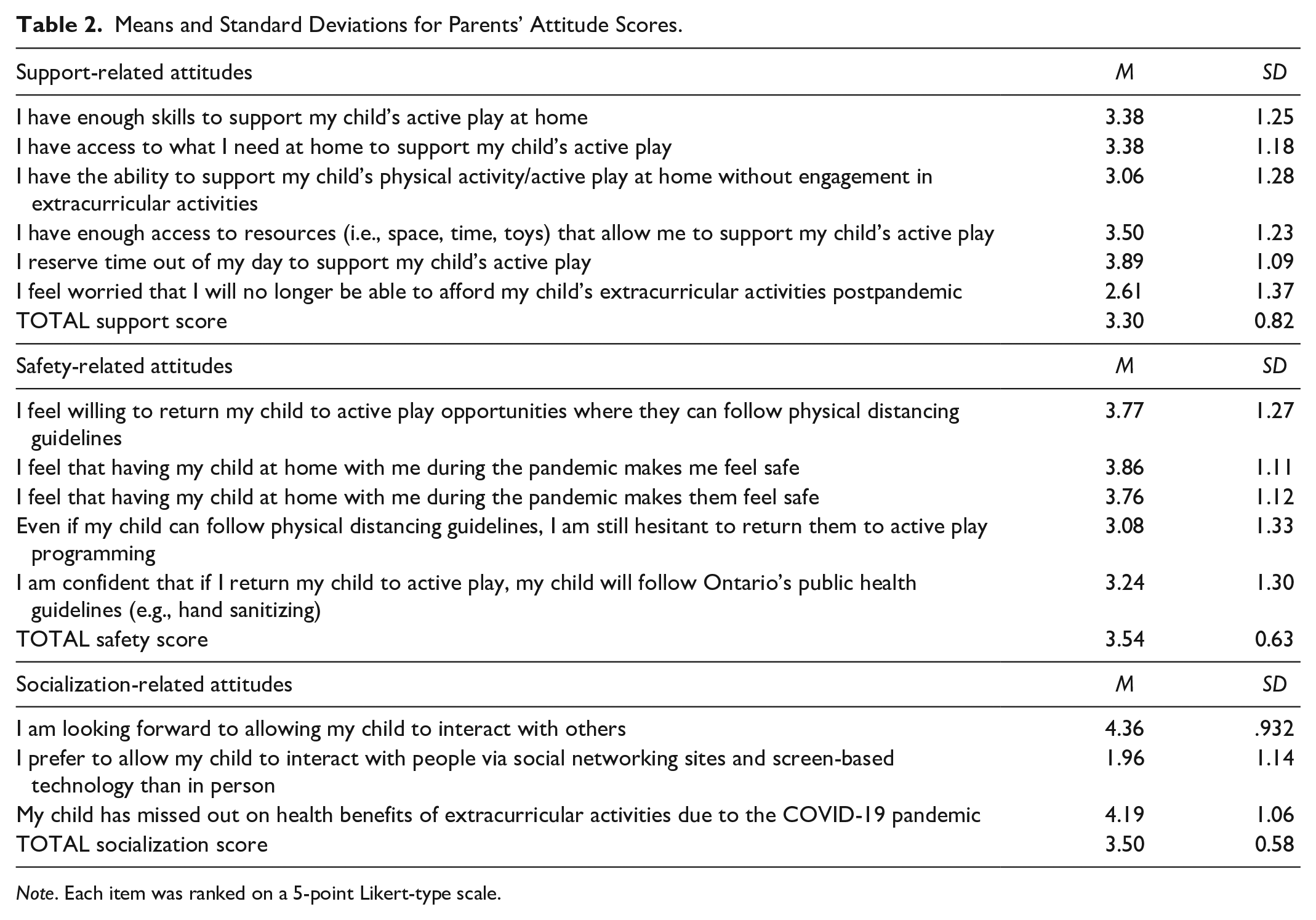
Note. Each item was ranked on a 5-point Likert-type scale.
Identified Predictors and the Influence of Demographic and Parental Factors on Parents’ Support, Safety, and Socialization Attitudes
The variable selection from the LASSO regression revealed 20 main predictors for parents’ attitudes regarding their children’s play/sport during COVID-19. See Table 3 for all identified predictors as identified by the LASSO regression for each attitude group.
Main Predictors for Parents’ Safety, Socialization, and Support-Related Attitudes.
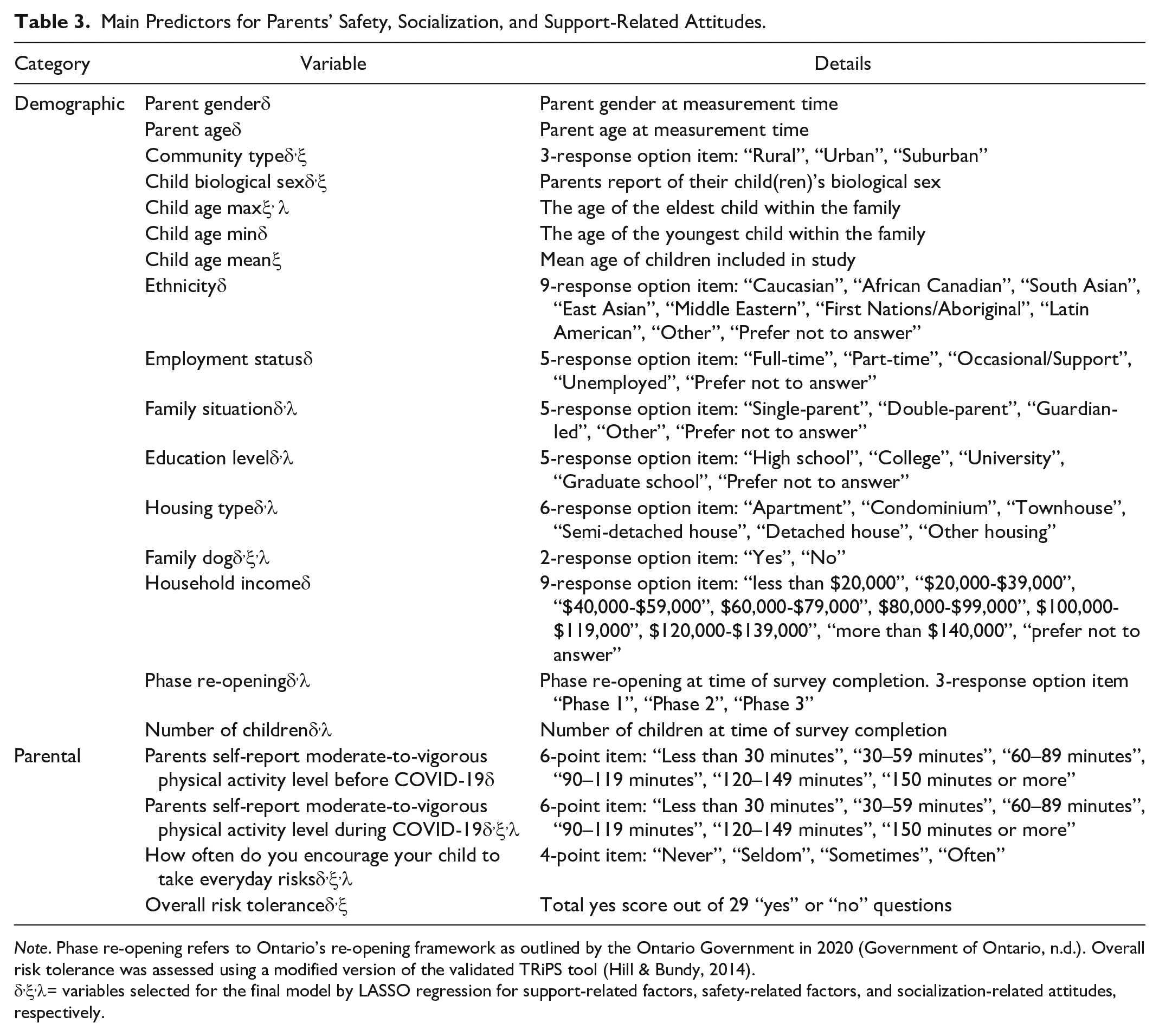
Note. Phase re-opening refers to Ontario’s re-opening framework as outlined by the Ontario Government in 2020 (Government of Ontario, n.d.). Overall risk tolerance was assessed using a modified version of the validated TRiPS tool (Hill & Bundy, 2014).
= variables selected for the final model by LASSO regression for support-related factors, safety-related factors, and socialization-related attitudes, respectively.
Support-Related Attitudes
For support-related attitudes, significant predictor variables were parent age, living in an urban community, family situation (i.e., in the “other” category), and not having a family dog. This model accounted for 17% of the variability observed, F(58, 713) = 3.76, p < .001. See Table 4 for complete results from the mixed linear models exploring various predictors’ influences on support-related attitudes.
Influence of Demographic and Parental Factors on Support-, Safety-, and Socialization-Related Attitudes—Mixed Linear Model Results.
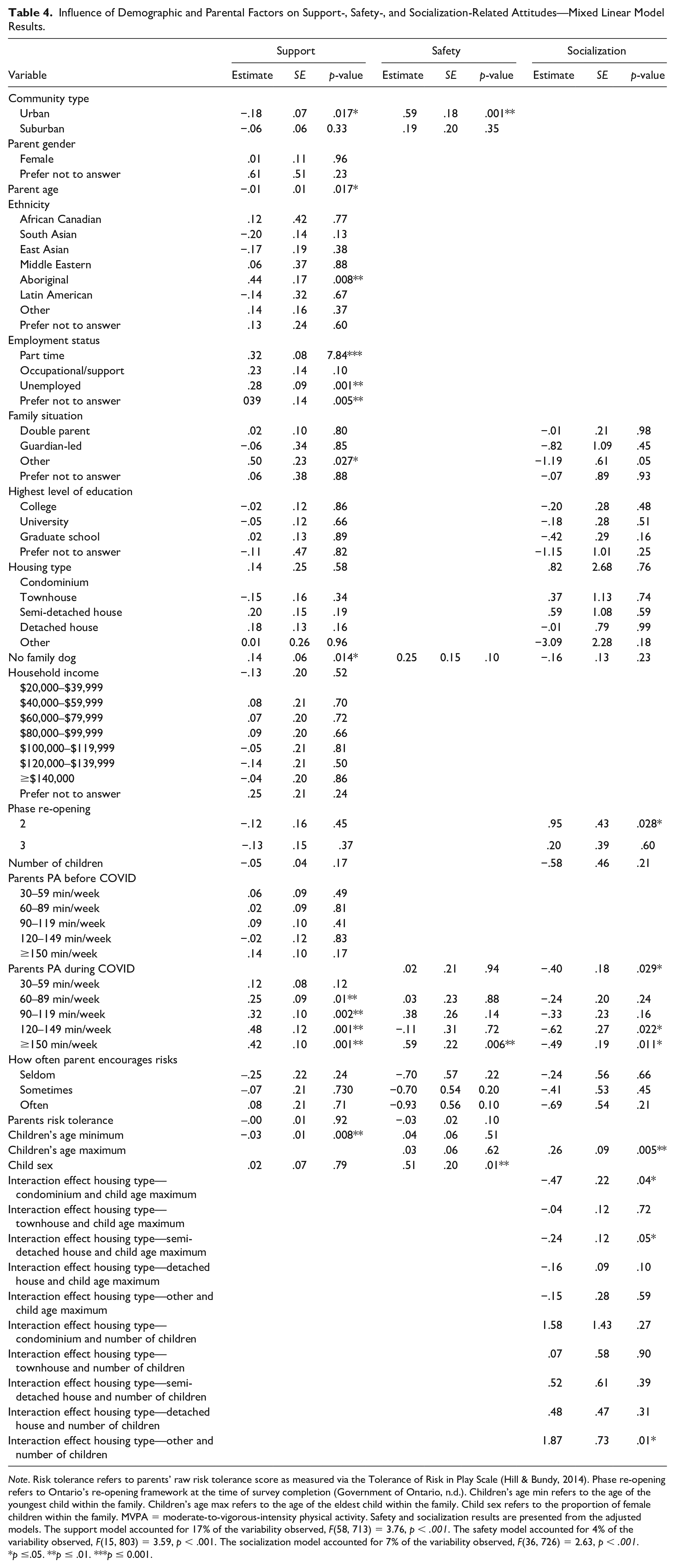
Note. Risk tolerance refers to parents’ raw risk tolerance score as measured via the Tolerance of Risk in Play Scale (Hill & Bundy, 2014). Phase re-opening refers to Ontario’s re-opening framework at the time of survey completion (Government of Ontario, n.d.). Children’s age min refers to the age of the youngest child within the family. Children’s age max refers to the age of the eldest child within the family. Child sex refers to the proportion of female children within the family. MVPA = moderate-to-vigorous-intensity physical activity. Safety and socialization results are presented from the adjusted models. The support model accounted for 17% of the variability observed, F(58, 713) = 3.76, p < .001. The safety model accounted for 4% of the variability observed, F(15, 803) = 3.59, p < .001. The socialization model accounted for 7% of the variability observed, F(36, 726) = 2.63, p < .001.
p ≤.05. **p ≤ .01. ***p ≤ 0.001.
Safety-Related Attitudes
No variables showed a significant association with safety-related attitudes. Living in a suburban environment, risk tolerance, children’s biological sex, and parents who engaged in more than 150 min/week of physical activity prior to COVID-19 all approached significance with safety-related attitudes (p < .10). This model accounted for 4% of the variability observed, F(5, 803) = 3.59, p < .001 (see Table 4).
Socialization-Related Attitudes
Being in Phase 2 of Ontario’s re-opening plan at the time of survey completion, children’s age maximum (i.e., having older children), physical activity levels of parents during COVID-19 (i.e., specifically those with higher levels of weekly MVPA), and the interaction between housing type and age of children, and housing type and the number of children had a significant effect on socialization-related attitudes (p < .05). The model accounted for 7% of the variability observed, F(36, 726) = 2.63, p < .001 (see Table 4).
Parents’ Level of Comfort and Plans to Return Their Child(ren) to Play/Sport
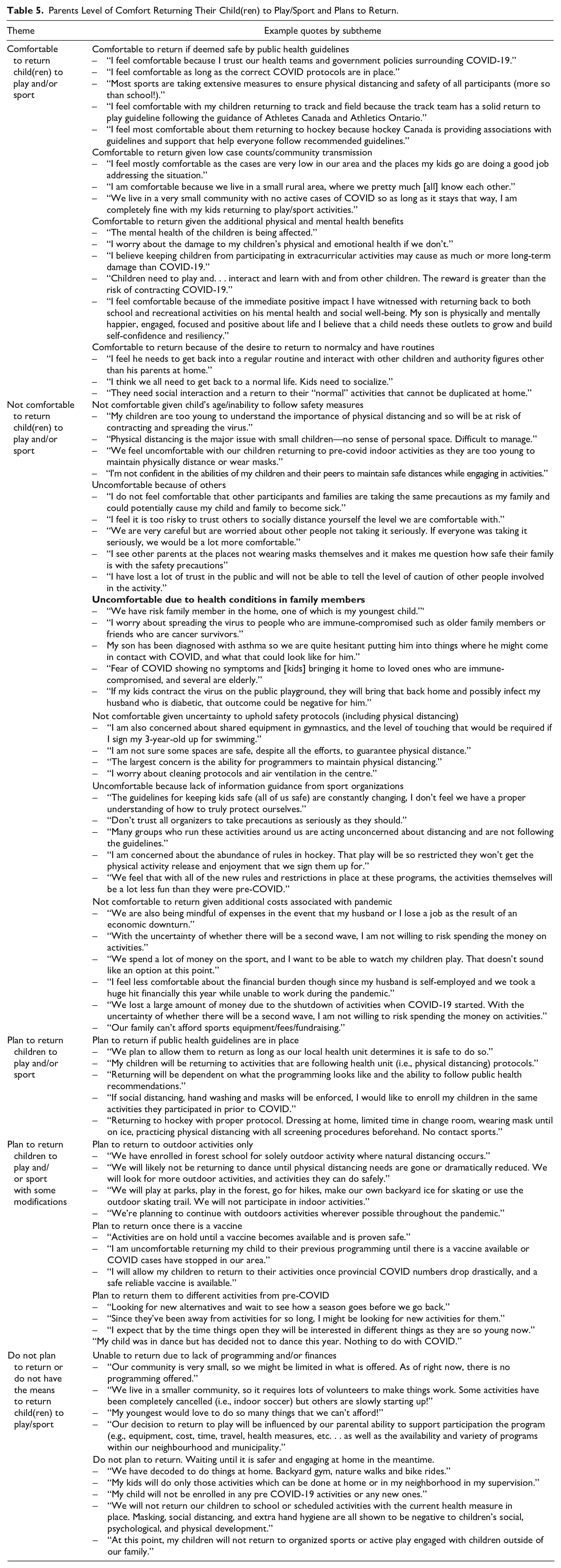
Regarding parents’ level of comfort returning children to play/sport, there was a range of views. The most common parent reasons for feeling comfortable included: if it was deemed safe per COVID-19-related public health guidelines in Ontario; low case numbers in their respective communities; a desire to return to normalcy and routine; comfort to return to outdoor activities only; and to support the physical and mental health of their children. Reasons for not feeling comfortable included children being too young to properly follow and understand public health guidelines (e.g., distancing); fear of others (e.g., other children and other families) not following guidelines and consequently spreading the virus; concern for vulnerable children or other family members; the uncertainty of facilities’ abilities to uphold safety protocols (including physical distancing); and increased costs of activities and general financial strain associated with the pandemic. Similar themes were noted regarding parents’ plans to return their children to play/sport (e.g., plan to return to outdoor activities only, plan to return if deemed safe by public health guidelines, etc.) with the addition of “plan to return only once there is a vaccine available.” See Table 5 for themes, subthemes, and supporting quotes concerning parents’ level of comfort and plans for their child(ren)’s return to play/sport.
Parents Level of Comfort Returning Their Child(ren) to Play/Sport and Plans to Return.
Discussion
The COVID-19 pandemic has led to extended public health measures in Ontario, Canada, as a means of limiting the spread of the infectious virus. Given the important association between physical activity-related activities (e.g., play and sport), and children’s overall health (Carson et al., 2017), the purpose of this study was to explore parents’ attitudes regarding their children’s return to these activities. Furthermore, it was examined whether demographic factors and/or parent-reported physical activity and risk tolerance influenced attitudes.
Overall, parents reported higher scores toward taking time out of their day to support their children’s physical activity (i.e., reported via support-related attitude). This is important, as prepandemic research supports the association between parents’ role-modeling and support on children’s likelihood to engage in healthy movement behaviors (Garriguet et al., 2017). For example, research conducted by Jago et al. (2011) found that higher levels of parental support with regard to promoting children’s physical activity (e.g., providing transportation) was related to greater physical activity among children (Jago et al., 2011). This is one of the first studies, to our knowledge, that explores the influence of parents’ support-related attitudes toward their child(ren)’s play/sport during the COVID-19 pandemic. Parental attitudes for supporting children’s activity during times when there is limited access to physical activity-supporting environments (e.g., gyms, sports) are important to consider.
Parents in the present study reported being eager to allow their child(ren) to interact with others (i.e., reported via socialization-related attitudes and open-ended responses). This may imply that some parents see value in the benefits of play/sport activities and their child(ren)’s socialization with others. It could also be an indication that parents need relief from parenting and homeschooling demands, as this has been previously identified by parents in Ontario during the pandemic (Szpunar et al., 2021). Allowing children to play with others during the pandemic may lead to higher levels of child-led, unstructured play, as this behavior has been found to have increased during COVID-19 (Dunton et al., 2020; Pelletier et al., 2021). The inclination reported by parents to return children to play/sport in the present study may have been due to the timeframe in which this study was conducted, with most participants in Phase 3 of re-opening (i.e., pre-Delta and Omicron waves; Public Health Ontario, n.d.).
Parents agreed that they felt their child(ren) had missed out on important health benefits associated with extracurricular activities due to staying at home for extended periods of time amid the pandemic (i.e., as reported via safety-related attitude). Furthermore, some qualitative findings from the present study revealed that parents felt they would like to return their children to play and sport programming as soon as possible. Compared with other periods where children may be home for extended periods (e.g., summer holidays from school, winter holiday break), public health measures because of COVID-19 may pose additional challenges for families as children are unable to play with others or engage in activity outside of the home as they typically would do during pre-COVID-19 extended stay-at-home periods (e.g., in the context of time away from school). Increased research is needed regarding the types of supports that can be put in place for families with children during times of extended stay-at-home periods, specifically when public health measures (e.g., physical distancing rules) are in place.
Risk tolerance was not significant regarding its influence on participants’ safety-related attitudes. This was contrary to expectations, as researchers have found that parental attitudes (e.g., fears, intentions), most frequently those of mothers, are a primary obstacle to child(ren)’s engagement in activities that involve risk (e.g., climbing a tree, playing without supervision; Boxberger & Reimers, 2019; Lee et al., 2015). However, given the TRiPS tool is a general risk tolerance scale, not one specifically designed for COVID-19 (or any pandemic), it is possible that risk was being influenced by factors that were not captured on this tool. Furthermore, parents in this study expressed that having their children at home with them during the pandemic made them feel safe. It is important to note that at the time of data collection for this study, there was no vaccine approved for children younger than 12 years of age in Canada, and many adults were not yet vaccinated (apart from front line and health care workers). Thus, it is possible that parents felt fear, or increased worry about the risk of transmission, and risk of their children contracting COVID-19 at the time of completing the survey and preferred to have them isolated at home with minimal contact. All these considerations may have led to the highest attitudes reported by participants in the present study being found for safety-related attitude items. These findings were emphasized via open-ended items, where some participants noted they did not feel comfortable or did not plan to return their children due to fears of others (i.e., other children and other families) not following proper health protocols, and because of the uncertainty of organizations/facilities being able to uphold safety protocols (and facilitate social distancing). In addition, some parents reported they were not yet willing to return their children to play/sport until a vaccine became available. Although risk tolerance did not influence support or socialization-related attitudes, we hypothesize this as a consequence of COVID-19 being more closely aligned with one’s perception of safety than their ability to support their children’s physical activity or socialization opportunities.
The regression modeling identified a number of predictors (i.e., housing type, child(ren)’s age, parent’s physical activity levels, etc.) that significantly influenced parents’ attitudes for their children’s play/sport. For example, parents’ levels of MVPA during COVID-19 influenced all three attitude categories, with those more active having more positive attitudes, specifically in the socialization category. In addition, community type, specifically living in an urban community, had a significant influence on safety attitudes. Previous research exploring the influence of community type and dog ownership on children’s physical activity levels identified that children living in rural communities and ownership of a dog had higher levels of physical activity compared to those living in urban areas, and those without a dog (Moore et al., 2020; Zenic et al., 2020); thus, our finding that living in an urban environment and not having a dog was an important predictor for safety-related attitudes was surprising and contradicts previous findings. Finally, the influence of community is important to note, as de Lannoy and colleagues (2020) found that compared to other regions in Canada, Ontario experienced the greatest decline in children’s time spent outdoors and in outdoor play compared with other provinces (de Lannoy et al., 2020). This can likely be attributed to the fact that Ontario was one of the hardest hit provinces by COVID-19 at the time of data collection, alongside Quebec, which both had the largest case counts and strictest restrictions (de Lannoy et al., 2020). In addition, because Canada has four seasons, rates of play/sport may have been influenced by environmental factors such as weather (i.e., lower physical activity levels in winter because of inclement weather, and higher physical activity during summer; Tucker et al., 2009), although this was not explored in the present study.
It is imperative that researchers further explore the effects of the pandemic on children’s future physical activity-related behaviors and the challenging decisions parents need to make with returning their children to these activities (or not). With such a small percentage of children meeting physical activity guidelines during the pandemic (Moore et al., 2020), there is a larger risk posed for developing chronic health conditions in later life. As COVID-19 continues to spread, with new variants of concern, increased support for at-home and contactless activity is needed. In addition, consideration for overcoming barriers/concerns raised by parents to support children’s physical activity participation is warranted.
Limitations
Strengths of the present study include the early launch of the baseline survey at the start of COVID-19, the large sample of Ontario parents, the inclusion of both quantitative and qualitative data, and the use of LASSO modeling to identify predictors of parents’ attitudes. Despite noted strengths, there are also some limitations of note. First, although our efforts to recruit as many Ontario parents as possible, only 819 participants completed the survey in its entirety. In addition, the length of the survey and the participant burden related to completion time may have led to incomplete data from some participants. Moreover, the survey respondents were primarily female, Caucasian, double parent, with higher average household incomes, which limits the generalizability of the findings. Finally, the lack of validity and reliability of the survey (with the exception of the Tolerance of Risk in Play Scale; Hill & Bundy, 2014) due to its creation by the research team and self-report nature of the survey also acts as a limitation. Given the responses were self-reported by participants, responses may have been influenced by social desirability bias (i.e., parents may have felt pressured to select a more desirable option for some questions). Finally, because this study took place during early COVID-19 when vaccines were not yet widely available, the survey did not capture the vaccination status of participants, or the consideration this might have for parents play/sport decision-making. In addition, it is important to note that several factors beyond those that were explored in the present study could have influenced parents’ attitudes of children’s play/sport, including but not limited to case counts in participants’ communities.
Conclusion
This study identified Ontario parents’ support, safety, and socialization-related attitudes toward their children’s return to play/sport during COVID-19. Parents had the highest attitudes toward safety-related items. In addition, important predictors of parents’ attitudes were highlighted, such as the influence of parents’ MVPA levels on attitudes. An equal divide was found between Ontario parents who feel comfortable returning their children to sport and those who do not. Future investigations are needed to explore what types of supports are needed to ensure children’s seamless transition back into physical activity-supportive environments (e.g., sport arenas, community centers, and playgrounds) as public health measures in Ontario ease and society adjusts to new parameters and norms. Moreover, future investigations are needed to assess if parents’ perspectives of their children’s play/sport during and following COVID-19 change as vaccines for children under 12 years become available.
Footnotes
Acknowledgements
We would like to thank all parents for participating in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Social Sciences and Humanities Research Council (SSHRC) Internal Explore Grant from Western University, which supported various study procedures (e.g., tokens of appreciations for participants). L.M.V. holds a trainee award from the Children’s Health Research Institute. P.T. holds an Early Researcher Award from the Ministry of Research and Innovation. B.A.B. was supported by a Social Sciences and Humanities Research Council of Canada Joseph-Armand Bombardier Canada Graduate Scholarship.