
Abstract
Doctors, including general practitioners, experience higher levels of mental illness than the general population. General practitioners who are partners in their practices may face heightened stress. In total, 10 general practitioner partners living with work-related distress were interviewed, and transcripts were analysed using interpretative phenomenological analysis. Three major themes arose: (1) extreme distress, (2) conflicted doctor identity and (3) toxic versus supportive workplace relationships. Participants detailed symptoms of depression, anxiety and burnout; reported conflicted identities; and discussed the impact of bullying partnerships. We recommend that organisational interventions tackling issues such as bullying be implemented and opportunities to debrief be offered as protected time activities to general practitioner partners.
Introduction
Doctors in the United Kingdom, including general practitioners (GPs), are working under increasing pressure and with decreasing resources (Cheshire et al., 2017; Fletcher et al., 2017). They report low job satisfaction (Croxson et al., 2017; Hobbs et al., 2016), high rates of depression, anxiety (Murray et al., 2015; Wallace et al., 2009) and burnout (Cheshire et al., 2017). Doctors internationally, including GPs, are more vulnerable to suicide than the rest of the population (Fox et al., 2011; Schernhammer and Colditz, 2004).
A recent UK survey found that 70 per cent of polled GPs planned to make a career change within the next 5 years, which has the potential to negatively impact primary care provision in England (Fletcher et al., 2017). A nationwide mixed methods study asked early GP leavers why they had left the profession (Doran et al., 2016); respondents cited increases in workload, which negatively impacted on doctor–patient relationships (Doran et al., 2016). It is therefore imperative that more is done to understand and support GPs living and working in the United Kingdom (Spiers et al., 2016).
Known sources of distress for GPs include an increasingly high workload due to increasing patient needs and expectations, the changing relationship between primary and secondary care, and high levels of bureaucracy (Croxson et al., 2017). In addition, the high emotional demands of GP work (Brooks et al., 2011) can be a cause of distress for some. Others report difficulties around the moral implications of being a ‘good doctor’ in the context of bureaucratic tasks such as those required by the Care Quality Commission (CQC), which reduce the ability to spend time with patients (Cheshire et al., 2017).
GP partners maybe particularly vulnerable to distress since, in addition to patient care, they must juggle additional responsibilities such as personnel and management roles, cope with the financial pressure of being small business owners (Baird et al., 2016), and strive to maintain good working relationships with their partners and staff (Garelick and Fagin, 2004).
Partnership is currently not attractive to younger doctors, who may feel the position is too risky in terms of finances and job security (Baird et al., 2016; Fletcher et al., 2017). However, GP partners are necessary for the smooth running of primary care in its current form, so an understanding of the challenges that face this group is vital. Despite this, there is little existing qualitative work exclusively investigating the experiences of GP partners.
This study employed the qualitative method interpretative phenomenological analysis (IPA; Smith et al., 2009) to explore the experiences of 10 GP partners. IPA offers a detailed, nuanced analysis of the personal lived experience of a phenomenon (Smith et al., 2009). The method is especially valuable where topics are complex and affectively laden, and for areas about which little is currently known. It therefore lends itself well to an exploration of GP partners’ experiences, since this is an under-researched area.
This study is part of a wider qualitative research project examining the barriers and facilitators to help-seeking for GPs in distress (Riley et al., 2017, 2018; Spiers et al., 2017). Existing papers based on a thematic analysis of this wider dataset present wider analyses of the experiences of the whole sample. This current IPA analysis digs deeper into the experiences of GP partners, a narrower subset of the participants, since these accounts were found to be especially rich and contained important and troubling data.
Methods
Design and participants
The data for this study are a subset of data collected for a larger study (Riley et al., 2017, 2018; Spiers et al., 2017), for which a total of 47 in-depth, participant-led interviews with GPs living and working in England were conducted by the first and senior authors, who took informed consent from participants at the time of the interview. Potential participants were contacted via emails to doctors attending a specialist service, as well as adverts to Local Medical Committees (LMCs) nationally, in GP publications and on social media. GPs who self-identified as living with, or having lived with, anxiety, depression, stress and burnout as well as those who did not have poor mental health, but were interested in the topic, were purposively sampled for the main study.
During the initial analysis, the first author kept a list of interviews suitable for IPA, that is, transcripts containing novel stories, insights and/or language. In total, 30 of the original 47 interviews were placed on this list.
IPA researchers work with homogeneous samples (Smith et al., 2009). This is first because generalisations cannot be drawn from the small samples of in-depth qualitative methods, so it can be useful to drill down into specifics. Second, using groups with fairly uniform demographics, it becomes possible to make more meaningful statements about any psychological variation in the group (Smith et al., 2009). As such, the identified list of rich transcripts was analysed to search for a demographically homogeneous group of GPs.
A total of 11 of the 30 richer transcripts were from GP partners living with distress who had been in practice for more than 10 years. From the 11 transcripts, five interviews with female GP partners and five from male GP partners were selected by the first author to form the corpus for this article. One transcript was rejected as it was considered that this participant was not living and working with their own experiences of distress, but was instead discussing colleagues’ experiences, so their experience was not therefore homogeneous.
This sample size is large enough to include an enlightening variety of convergence and divergence, yet small enough to allow for the in-depth analysis characteristic of IPA and to offer an alternate lens from the wide yet briefer analysis of our previous work (Riley et al., 2017, 2018; Spiers et al., 2017).
Ethics and data collection
Ethical approval was granted by the South West–Frenchay Research Ethics Committee (reference number: 15/SW/0350). Participants were told that they were free to stop the interview or withdraw their data at any time should they wish.
Interviews were undertaken by the first and senior authors and took place either face-to-face or on the telephone. Participants were asked about their experiences of living, working and seeking help for distress. Interviews lasted between 27 and 126 minutes (mean = 69 minutes), and were recorded and transcribed verbatim. All data have been anonymised.
Analysis
Analysis followed the procedures outlined for IPA by Smith et al. (2009). In keeping with IPA’s commitment to the idiographic (i.e. a focus on the particular; Smith et al., 2009), each transcript was analysed line-by-line, searching for points of descriptive, linguistic and conceptual interest. Initial notes were transformed into emotive emerging themes designed to capture the core of participants’ experiences. Themes for each case were clustered together and transformed into individual tables of themes. Finally, these themes were compared by searching for convergences and divergences, resulting in a master table for all participants.
The first author took the lead in the analysis, which was audited by two other authors. All authors, two of whom are academic GPs and therefore experts in the field, contributed to writing up and commented on interpretations, helping to ensure rigour. IPA subscribes to the concept of the double hermeneutic, meaning that the researcher is making sense of the participants’ sense-making (Smith et al., 2009). This means that different analyses from different researchers have the potential to draw out different elements of participants’ accounts. As such, our collaborative approach to analysis ensured the credibility of the final write-up, rather than guaranteeing that our findings are the only ‘absolute truth’ (Brocki and Wearden, 2005). Analysis continued during the writing of the article.
Results
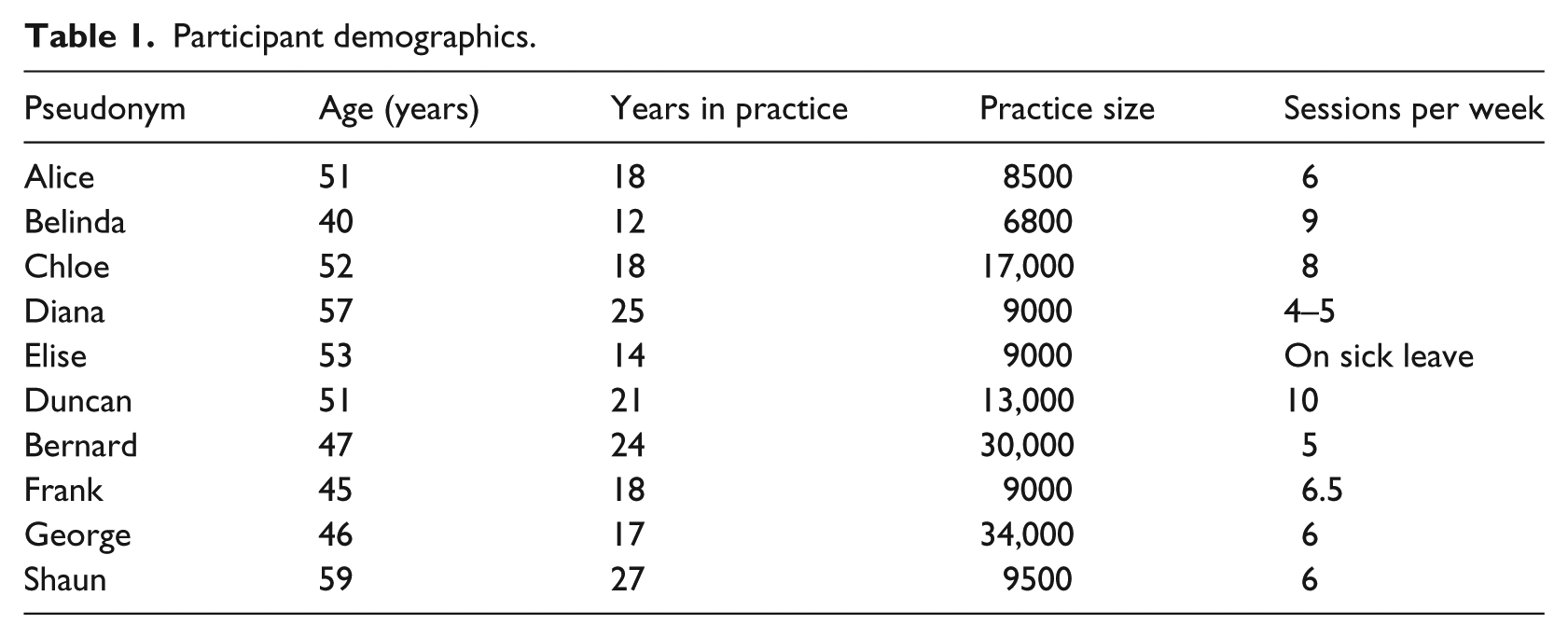
Participants were all GP partners living and working in the United Kingdom. Demographic information is given in Table 1. Three major themes arose: (1) experience of extreme distress, (2) conflicted doctor identity and (3) toxic versus supportive workplace partnerships. All participants contributed material to all three themes. Note that […] within quotes refers to editorial elision, often interjections from the interviewer.
Participant demographics.
Experience of extreme distress
All participants gave examples of extreme emotional distress experienced at, or resulting from, their work. Some participants discussed their perception of being stigmatised as a result of this distress. Some described feeling ‘numb’ as a result of their extreme distress, while others talked about the importance of understanding and acknowledging these difficult feelings.
Emotional distress
Participants described experiencing strong, difficult emotions, as with Bernard and his anxiety: Oh, I was very, very anxious, very. […] I was very much in a sort of hurry up mode, everything had to be done at 90 miles an hour. And I was really – I mean my analogy was like a spring coiled up inside.
Note the repetitive, exaggerated language Bernard used. His description of living life at breakneck speed is evocative of anxious arousal, while the analogy creates an image of a constant expectation of disaster.
Elise’s burnout manifested as a combination of physical and emotional symptoms: I couldn’t stop shaking. […] It was a very physical thing. I just felt absolutely exhausted, like I’d run a marathon, you know. And just really (pause) I, I knew something was wrong psychologically.
Elise’s language emphasises the extreme physical impact of burnout, following endurance of a huge workload.
Frank’s depression impacted his confidence as a GP. He used a punitive, self-critical voice, and experienced feelings of shame and diminished self-esteem: I started getting this general feeling of shame as I was speaking to patients or I was trying to sort things out that, ‘What I’m saying has no value’.
Belinda considered taking her own life because of her depression and described her emotional reaction to patients who came to her also feeling suicidal: ‘I just can’t see what the point is. […] I agree with you’. I wouldn’t say that to them, but I would be just sat there thinking, ‘Well, you know, actually it’s probably quite a viable option’ […]. But I’d be going, ‘Oh no, we ought to call the Crisis Team, we ought to do this’. You know, so I was saying all the right things but I didn’t feel – I felt quite detached from it.
A sense of hopelessness comes across in this extract. Note that Belinda felt detached from patient care, a symptom of burnout. There is a tension here between her emotional connection with her depressed patients, and her detachment from her role as their GP. Despite this detachment, she reports continuing to carry out care in the way that she felt she should.
Perceived and internalised stigma around mental illness
Participants reported experiencing shame as a result of their stigmatised mental distress. Many perceived this stigma as occurring throughout the medical profession, as George describes: The profession […] historically, has (pause) had a view, we’re doctors, we get on with it. We should probably accept we’re mortals and we don’t. We just, y’know, it’s incredibly arrogant.
George suggests that doctors perceive themselves as immortal and immune to illness. It is easy to see why stigma around ill health, including mental illness, would result from a culture like this.
For others, the stigma is internalised. Shaun reports his previous time off sick for stress in an ambiguous fashion: The other thing was that while I was off sick, if you like, in inverted commas, quote/unquote.
Shaun qualifies this time off sick three times (‘if you like’, ‘inverted commas’, ‘quote/unquote’), suggesting that he is keen to emphasise that he didn’t really need to be off sick.
Bernard arranged study leave at a time when he was becoming unwell: Maybe I knew I was becoming unwell secretly, and it was maybe my get out of jail clause.
Who is Bernard keeping his illness a secret from? – Himself or others? Bernard’s use of the ‘get out of jail’ metaphor implies he experienced his illness as shameful, with study leave a lucky escape: a feeling that makes sense within the context of George’s depiction of general practice as a place for invulnerable GPs.
Numbed feelings
Some participants reported numbed feelings, perhaps a symptom of burnout. Diana felt medical school deliberately stripped away the emotions of doctors: You’re sort of taught to lose your feelings. Everything is taught in this very clinical, disembodied, […] way. Where you don’t feel anything. So you lose the ability to put your hand around someone and accept their feelings. […] That’s a nurse’s job.
Feelings here are framed as inferior, nurses’ work; Diana described being detached from her own emotions and those of others, depleting her sense of identity.
Belinda described numbed feelings as going hand in hand with her depression: I think it’s all a bit foggy now, (laughs) to be honest. […] I think it’s difficult, because you don’t feel like (pause) you don’t see that there’s any positive feature. […] And then, you know, that time has then passed. You don’t really feel it happening; you’re just trying to get through.
Note that Belinda uses ‘you’ rather than ‘I’ throughout this extract, increasing the impression of distance from the experience. Her life felt denuded of positivity for her at this point; she went through the motions without any emotion, indicating a loss of feeling and identity to a sense of depersonalisation and detachment.
Understanding and acknowledging distress
Some participants reported moving towards an understanding of their distress and how it should be addressed. George described how a mild physical illness helped him acknowledge the strength of the mental ill health he had been downplaying: Came back with a cold, which I normally wouldn’t have batted an eyelid about. But just felt lousy and not up to working. And so missed work with that. But it became clear that that was just the sort of the, the final straw and […] just couldn’t face going in to work.
Therapy helped Frank reach an understanding that, in contrast with George’s quote about immortal doctors, many of his colleagues were also potentially living with mental illness: There have been lots of endogenous depressives in general practice and in medicine, you know, because we’re fairly empathetic.
Seeing depression as something external to his situation helped Frank acknowledge and contextualise it.
Conflicted doctor identity
Participants described a conflicted sense of identity which, for some, manifested as a loss of self. Many participants felt that their own identity had been subsumed by the role of the ‘doctor’, while others talked about their attempts to reclaim a sense of self, separate from their professional role as a GP.
Loss of self
Several participants reported a perceived loss of self. Alice described a feeling of absolute identity failure following the death of a patient, an event that triggered her depression: It felt like failure as a person, as a mother, as a GP.
Elise’s challenge to her identity came from physical illness. She experienced voice loss during time off for stress arising from difficulties with her GP partners and saw a symbolic element in this symptom: A friend of mine said something afterwards about sort of, ‘Well, gosh, who was it who didn’t want you to speak?’
By literally losing her voice, Elise couldn’t speak. Her inferred symbolic reading suggests her views were being silenced. Perhaps, she perceived that her partners were symbolically drowning her voice out, or maybe it was an element of her own identity that wanted to speak out, but didn’t feel able to.
Subsuming, inescapable doctor role
Along with this loss of self, many participants described a sense that the doctor role took over their identity, leaving no room for any other roles. Diana gave an example of how doctoring left no room for her mothering role: I used to do 14 hour days when the kids were small […] So I just didn’t used to try and come home. (Pause) My, husband would put the babe, the kids to bed.
Similarly, Shaun had no time for home life: You just simply come home and have something to eat and then probably just go to bed and get ready for the next day. So you have to be really quite disciplined and make sure that that happens really.
Shaun’s use of the word discipline is strong; there is no space for relaxation.
For some, the impact of the subsuming doctor role tied in with their loss of a sense of self. Duncan felt he could have experienced other aspects of his identity but that doctoring took those away from him: I never ever stop being a doctor. […] That takes a big part of me away. I’ve only realised that with time spent with people who aren’t doctors, they seem to enjoy life more.
Duncan’s language implies a theft of a substantial, happier part of himself by the inescapable doctor role he permanently inhabits. His world consists of doctors and non-doctors; those on the other side of the fence have a far more carefree existence.
Chloe described regretting going into medicine and wished she had taken another career path. However, she felt trapped by the doctoring role. When asked to talk about why this might be, she said, It’s a very high commitment job and by the time you (laughs) get to a point where you can stop and take a breather, you’ve actually invested a good ten years of your life getting there. And to then say, ‘Oh, actually this is really horrible. I don’t want to do it’, it takes a huge amount of strength to do that.
GP training is portrayed here as a long, intense investment from which it is impossible to back away. The medical profession is cast as a system that has its hooks in Chloe, leaving her powerless to escape. She feels that she and other doctors are complicit in upholding this: The longer we go on pretending we can, the longer that the system is going to limp along and no one is actually going to address the issues.
General practice is pictured here as a broken machine which doctors prop up, meaning the profession itself is being trapped inside the all-consuming doctor role.
Reclaiming oneself from the doctor role
Several participants detailed ways in which they were taking back non-medical elements to their identities. Elise was on sick leave at the time of the interview and questioned whether to go back to general practice: ‘I don’t think I can be a doctor’. I had a couple of days of feeling a bit wobbly and thinking, ‘Well, if I’m not a doctor, what am I?’ Part of my identity, that’s the whole burnout thing, isn’t it, it’s professions that identify, you know, the work is who they are. […] And then after a couple of days I thought, ‘Actually, I don’t think I want to do it anymore really’. The kind of – the – I think it’s a mug’s game (laughs).
Initially, Elise articulates her anxiety over what would be left if her all-consuming doctor role is taken away. She then reframes her old role as undesirable and contemplates a deliberate move onto something new.
Bernard has found a happy medium. He owns and maintains some land and is able to use this role as a counterpoint to doctoring: I spent the whole morning working on my land, doing jobs (pause), fiddling with machinery, fiddling with a water pump that’s not working and, yeah, it’s a complete distraction from what I normally do.
Toxic versus supportive partnerships
All participants talked about the impact of their working relationships on their mental health and well-being. Unsupportive or bullying environments were reported as harmful, whereas supportive partners and partnerships were appreciated and perceived to be helpful.
Unsupportive environments
Several participants reported unsupportive workplace partnerships. Chloe described an instance when, as a GP with only 2 years of experience, she was threatened in her room by a patient, resulting in the police being called. She reported the aftermath of this event: At the time where I was working – what happened was I was moved into another room and I went on with my surgery.
There was no suggestion of any acknowledgement or support offered by Chloe’s practice following this frightening incident. The passive language used (‘I was moved’) feels cold and impersonal, and strips Chloe of agency. The apparent lack of reaction from Chloe’s practice normalises the violence to which she was exposed and has the potential to reinforce a sense of isolation, leaving Chloe to individually manage any distress that may have arisen from the incident, such as increased anxiety.
Frank discussed the reaction his partners gave him when he gave them advanced warning that he would need some time off sick for his severe depression: ‘I’m going to have to take some time here, because I’m really, you know, I’m struggling and I’m being treated [for depression] and it’s hard’, and then they went, ‘Oh, bloody hell’, […] ‘I’m going to, in a month’s time I’m going to have to take two weeks’. And they said, ‘Oh blimey, why didn’t you give us a bit more notice?’ (laughs) Which is kind of exactly the thing that I had dreaded.
The anticipation of this reaction from Frank’s partners may have worked as a barrier, preventing him from taking the time off that he needed.
Bullying, manipulative partners
While some partnerships were perceived to be unsupportive, others appeared to be actively destructive. Shaun felt that he had been forced out of his previous practice following an enforced period off sick. One of his partners came to his house to tell him that he was not fit to continue practising at his surgery; something Shaun did not agree with. He tried to speak to his senior partner but was met with resistance: I wanted to see her and she said, ‘No, I’m dead against it’. […] She basically just said, ‘I don’t want to speak to you’. So she was absolutely no help at all. As a senior colleague, it was a disgraceful act actually, having worked with somebody for so many years.
This blocking behaviour did not allow Shaun to speak up for himself or ask questions about his situation.
Elise was bullied by her partners until she decided to leave her practice. She described a meeting meant to be about her return to work following time off sick with exhaustion. All names in this quote are pseudonyms: I went in and it was a blood bath. They were awful, absolutely awful. […] Sandra was shaking so much she couldn’t even look at me, and her hands were shaking as she was holding my email. She was absolutely livid. Stefan was stabbing his finger in the air at me, telling me I didn’t know what it meant to be a partner.
The language Elise uses here (‘Blood bath’, ‘awful’, ‘shaking’, ‘livid’, ‘stabbing’) sounds more fitting for a horror film than a partnership meeting.
Positive, supportive partners and partnerships
However, several participants described healthier partnerships, in which doctors and staff supported one another. Belinda talked about the supportive actions of practice staff during a period of stress: They were all really lovely and they would keep coming and bringing me cups of tea and chocolate and stuff and they were all really sweet.
The warm language here implies easy and genuine support from these staff members. George describes his partners’ reaction to his time off sick, which stands in stark contrast to the quote from Frank, above: I was quite well supported and well guided. My practice was very supportive, the practice manager was very helpful.
This show of support helped George feel more at ease with taking time off.
Duncan described a positive example of best practice within his supportive partnership, where the GPs take time out every fortnight to see a group counsellor together: You start to get quite, tired and upset and you know, just you feel like you can’t go on. So – and there’s no doubt that’s definitely helped, you know, by making, putting it in the fabric of the practice, by saying it’s compulsory attendance for all doctors every two weeks if they’re working that day. […] It has helped us to maintain our sanity.
This innovative use of supervision within a practice is portrayed as a helpful outlet for inevitable doctor distress and is a model more practices may benefit from adopting.
Discussion
This article has presented the accounts of 10 GP partners who each had more than 10 years of experience in this role and who were living with distress. As far as the authors are aware, this is the first qualitative article to focus specifically on this group, despite the increased stress they may experience compared to salaried or locum GPs (British Medical Association (BMA), 2013).
Participants spoke of high levels of distress, reporting depression, anxiety, burnout and suicidal ideation. These heightened emotions manifested as physical symptoms and impacted their confidence. These findings add to a growing body of literature demonstrating high levels of distress among doctors in General Practice (Cheshire et al., 2017; Doran et al., 2016; Hobbs et al., 2016; Vijendren et al., 2015).
Analysis revealed a perception of stigma around mental illness within the medical profession, which went hand in hand with a medical ‘culture of invulnerability’, in which doctors feel it is unacceptable to be unwell (Brooks et al., 2016). Stigma around mental illness flourishes within medical culture, even though mental ill health is the most common reason given for doctors taking time off sick (Vijendren et al., 2015). This is very concerning and highlights the need for a cultural shift within general practice.
Participants also described a loss of self, perhaps because of the all-consuming doctor role. It has been noted that doctors, including GPs, maybe self-critical and perfectionist (Brooks et al., 2011) and that, while they are able to see their patients holistically, they may struggle to give themselves the same due (Montgomery, 2014). Doctors tend to strongly identify with their profession (Cascón-Pereira et al., 2016), perhaps leading to a neglect of other aspects of their personalities, which may result in numbed feelings or a perceived loss of self. Our findings show that a strong association with the high-status doctor role may leave GP partners vulnerable to a loss of their sense of themselves as rounded individuals, and hence a conflicted sense of identity, especially when the doctor–patient boundary is blurred.
Some participants reported reclaiming a more integrated sense of themselves, separate from the doctor role, although for one participant this took the form of leaving the profession. This strategy for reclaiming a sense of identity maybe personally effective but, given the dramatic losses that the GP workforce maybe facing over the next five years (Fletcher et al., 2017), it is alarming in terms of the profession.
Participants also drew attention to unsupportive and bullying partnership environments. There is evidence that bullying exists within the National Health Service (NHS; Quine, 2002) as a whole, as well as in general practice (Doran et al., 2016). Our findings highlight the potential depth of that bullying and indicate that GP partnerships maybe particularly at risk of becoming hostile places to work. Medical education currently does not emphasise teamwork (Montgomery, 2014), despite evidence that good teamwork is essential for the successful delivery of healthcare (Huby et al., 2002).
Reassuringly, some participants gave examples of best practice within their partnerships, particularly in the case of one practice, which had created protected time for clinical supervision twice a month. Much existing literature has posited that clinical supervision would be beneficial for GPs but has also emphasised the difficulty of finding time for this (Checkland and Spooner, 2015; Huby et al., 2002). The findings here demonstrate that within the right environment, this model can work and have positive benefits.
Conclusion
IPA was used to examine the narratives of GP partners living with anxiety, depression, stress and/or burnout. The nuanced findings presented in this article allow the reader to step into the shoes of the participants and gain a detailed impression of their experiences. GP partners are at risk of experiencing extremely distressing emotions and a conflicted sense of self, particularly in the context of unsupportive or bullying practices. Given the current difficulties with recruiting GPs in general and partners in particular (Baird et al., 2016; Fletcher et al., 2017), it is crucial that we learn more about the experiences of GP partners and GPs in general, so that they can be supported within their working environment, and general practice sustained. Based on current and previous findings, the authors recommend that, in line with the GP Forward View (National Health Service (NHS), 2016), more GPs are recruited in order to alleviate time pressures (Hobbs et al., 2016; Richter et al., 2014), that researchers develop organisational interventions in order to address practice level issues such as bullying (Kinnunen-Amoroso, 2011; Montgomery, 2014; Romani and Ashkar, 2014), and that clinical supervision and debriefs are incorporated as protected time activities within general practice (Garelick and Fagin, 2004; Huby et al., 2002) on an ongoing basis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval for this research was granted by the South West–Frenchay Research Ethics Committee (reference number: 15/SW/0350).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.