
Abstract
Background
Communication is a key component in successful talking therapies. Furthermore, the association between Speech, Language and Communication Needs (SLCN) and mental-health problems is well-established and we might expect this group to have increased difficulties accessing services. Despite this, research into potential communication barriers within Child and Adolescent Mental Health Services (CAMHS) is lacking, both generally and for SLCN children specifically.
Aim
This study explored the views of caregivers of children with and without SLCN to identify perceived barriers to accessing CAMHS. Key factors were considered: caregivers’ understanding of the language used by CAMHS; communication strategies used by professionals; and caregiver views of children’s mental health outcomes after accessing CAMHS.
Methods
An online caregiver survey was used to collect views. The survey was completed by 61 caregivers of children who had been referred to CAMHS, for reasons other than communication, 32 of whom cared for a child with SLCN.
Results
Caregivers generally understood the language used with them by CAMHS, although a minority reported difficulties. They were less positive about communication adjustments, discharge processes, and outcomes after accessing CAMHS. Caregivers of children with SLCN were more likely to report that their child’s mental health was poorer after CAMHS. No other differences were found between the SLCN/non-SLCN groups with communication presenting some barriers across both.
Conclusions
All children accessing CAMHS would benefit from increased communication adjustments in order to achieve the most effective intervention.
Plain Language Summary
Good communication is essential in talking therapies, but children who have Speech, Language and Communication Needs (SLCN) may face extra challenges when accessing mental health support. This study explored how caregivers of children with and without SLCN experience communication within Child and Adolescent Mental Health Services (CAMHS). It aimed to find out whether these families face specific barriers when trying to get help, how easy it is for them to understand CAMHS communication, what strategies professionals use to support children with communication difficulties, and how caregivers view their child’s mental health after receiving services. An online survey was shared on social media and completed by 61 caregivers whose children had been referred to CAMHS. Just over half of these children had diagnosed SLCN. Overall, most caregivers said that the language used by CAMHS staff was easy to understand, but some still reported difficulties. Caregivers were less satisfied with how professionals adjusted for communication difficulties and were dissatisfied with discharge and with mental health outcomes. Communication barriers appeared to affect all families, not just those with SLCN. However, caregivers of children with SLCN were more likely to say that their child’s mental health was worse after receiving CAMHS support. One possible reason may be practice and policy decisions that mean mental health and communication problems are rarely treated together. The study suggests that CAMHS professionals should receive more training about communication barriers and the specific needs of children with SLCN. However, our findings suggest that improving understanding and communication strategies could help ensure that all children and their caregivers can access effective support and achieve better mental health outcomes.
Keywords
Introduction
It is widely acknowledged that most adult mental health illnesses start during childhood or adolescence (Wolpert et al., 2014). Mental health difficulties during childhood and adolescence can have an adverse and ongoing impact (Murphy & Fonagy, 2012). This negative impact includes increased risk of school absence and disruption to education (Meltzer et al., 2005), problems with social relationships, increased risk of offending, and drug and alcohol misuse (Richards & Abbott, 2009). Furthermore, mental health conditions during childhood or adolescence are common, with global epidemiological data reporting that suicide is the third most common cause of death for adolescents, and that up to 20% of children and adolescents experience a disabling mental illness (Belfer, 2008).
Timely and appropriate intervention is therefore vital to minimise the impact of mental health difficulties and improve wider life outcomes (Royal College of Paediatrics and Child Health, 2014). Recent evidence suggests that Child and Adolescent Mental Health Services (CAMHS) can provide psychological talking therapies that are effective long term (Pilling et al., 2020). In the UK, CAMHS are available to all young people experiencing emotional or behavioural difficulties, and comprise multidisciplinary teams which include psychiatrists, psychologists, and nurses (National Health Service (NHS), 2019). The core roles of CAMHS are detecting, assessing, supporting, referring young people, and training other relevant professionals (National Institute for Health and Care Excellence (NICE), 2019). However, there is geographical variation in the access to services available across the country (Department of Health and Department for Education and Skills, 2006) and there has also been increased demand for services which has proven difficult to meet (Evans et al., 2023) in the context of withdrawal of investment in local authority CAMHS spending (YoungMinds, 2013).
Since most of the psychological interventions offered are talking therapies, communication is a key element to treatment. Yet communication has also been reported as a key barrier to accessing support (Coyne et al., 2015; Hansen et al., 2021), with over a third of studies citing difficulties in verbalising the need for help and talking about mental health issues (Radez et al., 2021). The relationship between communication and social-emotional difficulties is also well established (Cantwell & Baker, 1987; Dall et al., 2022; Donolato et al., 2022). Despite this, there is a dearth of integrated care models that support the co-occurrence of mental health and communication difficulties (Xue et al., 2025). Children with Speech, Language and Communication Needs (SLCN) are therefore a group that warrant focussed investigation in terms of accessing support as they may experience increased challenges accessing support. SLCN is an umbrella term that includes a diverse range of children. The current study focusses on children with and without two of the most prevalent subtypes of SLCN: Developmental Language Disorder (DLD) and Autism. Although these groups are distinct, and often have different clinical needs in some respects, there are also marked overlaps with structural language difficulties in these populations (Georgiou & Spanoudis, 2021; Huang & Finestack, 2020). Furthermore, semantic-pragmatic language difficulties have been reclassified from autism (ICD-10) to DLD (ICD-11) in some diagnostic manuals reflecting the overlap between these conditions (World Health Organisation (WHO), ICD10: 2004 and ICD11: 2022).
Individuals with DLD demonstrate significant difficulties with spoken language which cannot be explained by intellectual disability, hearing loss or neurological damage (ICD-11, WHO, 2022; CATALISE consortium, Bishop et al.,2016). 1 These difficulties persist into adulthood (Botting, 2020), impacting on everyday life and education (see Dubois et al., 2020; Wilmot et al., 2024) as well as health related quality of life (Le et al., 2021) and adult mental health (Botting et al., 2016). DLD is common compared to other developmental disorders, affecting around 7% of school age children (Norbury et al., 2016; Tomblin et al., 1997). In light of this high prevalence, it is noteworthy that the term DLD is relatively new, the result of consideration by multi-national, multi-disciplinary professionals to gain a consensus about the criteria for diagnosis and agreed terminology (Bishop et al., 2016). Crucially, these changes in criteria and terminology may also have implications for the awareness of DLD amongst CAMHS professionals, and the provisions made for this cohort of young people. Nevertheless, despite the high prevalence and long-term nature of DLD, this group are markedly under-represented and services beyond early childhood are lacking (McGregor, 2020).
A second key group that we focus on in this article is autistic children. Autism represents a diverse range of neurodevelopmental features, historically defined by difficulties in social interaction and communication, combined with atypical patterns of activities and behaviours, such as challenges transitioning between different activities (WHO, 2023). Autism prevalence has been reported recently to average around 1% of all children globally (Zeidan et al., 2022). In addition, there has been an increased recorded incidence of autism diagnosis reported in the UK in the last twenty years, attributed to rising diagnosis amongst previously under-diagnosed groups including adults and females (Russell et al., 2022). Autistic people may have communication differences that impact their ability to access talking therapy. For example, different verbal and non-verbal language skills (such as voice tone and gesture); minimal-verbal skills, or difficulty understanding non-verbal language (National Autistic Society, 2025).
SLCN and Mental Health
Several cohort studies have confirmed that individuals with communication related conditions such as DLD and autism are more at risk of experiencing mental health issues, that are not caused by their communication needs per se, but which co-occur. This association has been reported across a range of countries (e.g.,
Importantly, this relationship has been noted as bidirectional (Tamayo et al., 2024): Children and young people who require mental health services, also show higher rates of language difficulty (between 28% and 55% of those referred to psychiatric and psychological services; Cohen et al., 1993; Norbury et al., 2024); and those who have experienced psychosocial adversity are also more likely to have language impairments (Andrews & Botting, 2020; Savi-Karayol et al., 2025; Snow, 2021). Toseeb and colleagues (2023) recently showed that young people with DLD were more likely than those without DLD to feature in polygenetically determined groups who had persistent high risk of mental health difficulties throughout development. This suggests that there may be a common genetic factor for psychological and communication disorders. Although the literature has established this relationship between DLD and mental health difficulties in young people, little research attention has been given to engagement with CAMH services, or the views of families who are referred. The heterogeneous nature of DLD, and the lack of research generally regarding this group (McGregor, 2020), may contribute to the lack of literature considering children and adolescents’ access to and experiences of CAMHS.
Similar to those with DLD, autistic children have also been shown to have increased risk of associated mental health difficulties (Lundström et al., 2011; Simonoff et al., 2008; Tick et al., 2016). Autism usually involves increased communication difficulties and often associates with mental health needs, especially anxiety and depression with co-occurrence estimates around 35% and 18% respectively (Micai et al., 2023; Jolliffe et al., 2023; Lai et al., 2019). Some attention has been given in the literature to CAMHS engagement by parents of autistic children (Meltzer et al., 2005) and a number of adjustments to enable autistic children through the CAMHS process have usefully been identified (Pemovska et al., 2024). Nevertheless, a study by Ashworth and colleagues (2025) still reported that parents felt they had been offered therapies that were ineffective and which did not incorporate reasonable adjustments.
SLCN and Access to Child and Adolescent Mental Health Services
Thus far, not enough attention has been given regarding communication barriers for children with and without SLCN when accessing CAMHS (Ashworth et al., 2025); or to the processes for identifying and adjusting for unrecognised language difficulties in children referred to mental health services (Norbury et al., 2024). Indeed, there has been surprisingly little research in general regarding the impact of young people’s language skills impact their experiences of these services. This is especially pertinent since health literacy is vital to patient engagement: If patients cannot gather, process, and comprehend health information, it impacts their ability to care for themselves effectively and make appropriate decisions (Coulter & Ellins, 2006). It is important to note that children with SLCN access CAMHS with co-occurring mental health issues, not to address the SLCN itself; and that exploring the experiences of clients with SLCN further might offer a window into communication barriers more widely.
One area that has been considered by the literature is the readability of the written language used in the letters sent by CAMHS to families. NIHR evidence suggests that the average reading age of UK adults is 9–11 years of age (NIHR Evidence, 2022). Bennett et al. (2012) analysed the letters sent out by their service and found that they would be difficult for their pcontext of withdrawal of investment in localatients (profiled as adolescents aged between 13 and 18, without general learning difficulties) to read. However, there is little direct acknowledgement of patients who have primary language difficulties, who would likely find the letters even more challenging to read). In a recent landmark study by Hobson et al. (2022) parents’ opinions of mental health and DLD were collected via survey and interview methods. Their study highlighted a number of themes, including: Practical aspects of therapy; the view that standard approaches to intervention might not be appropriate; and the effects of language difficulties on the child’s presentation of mental health needs. Caregivers often reported a lack of professional understanding about DLD and communication difficulties and felt that this substantially affected mental health intervention. Despite the fact that much of the CAMHS process involves various forms of verbal and non-verbal communication, there is a lack of research into the potential communication barriers as perceived by caregivers of children with communication difficulties, especially at the point of receipt. As such, their perspectives may not be contributing optimally to service delivery, and some barriers may remain hidden.
Caregiver Views of Child and Adolescent Mental Health Services in the General Population
Caregivers play a vital role in recognising their child’s distress, deciding to seek out professional help, and navigating mental health services (Logan & King, 2001). Therefore, their opinions about CAMHS have vital implications (Coyne et al., 2015; Hobson et al., 2022; Ronzoni & Dogra, 2012). Furthermore, positive caregiver opinions of CAMH services have been strongly associated with functional improvements (Garland et al., 2007) and the completion of treatment plans (Oruche et al., 2014). Therefore, engaging with parents’ views, and ensuring those views are favourable, plays a key role in delivering an effective CAMH service. Coyne et al. (2015) reported that caregivers and adolescents identified that the lack of information available was a barrier to accessing and engaging with CAMHS. These wider studies speak to the need to ensure that optimum communication for all groups is considered, and may indicate that clients with SLCN are disproportionately impacted by barriers.
The Current Study
In sum, therefore, our rationale is that (a) communication is central to talking therapy; and therefore (b) that difficulties with communication are likely to lead to poor access to CAMHS; and yet (c) there is very little research directly addressing this point. In particular there is a lack of evidence addressing whether children with SLCN are especially disadvantaged, or whether communication barriers are experienced across all families. Given that children and adolescents with SLCN are more likely to have co-occurring mental health difficulties, and the fact that general associations between communication and mental health have been identified even when SLCN has not been formally identified, further exploration of this issue is warranted. In the last few years, there has almost a 30% rise in referrals of children with neurodevelopmental conditions to CAMHS (Children’s Commissioner’s Office, UK Government, 2025).
The present study therefore reports on the views of CAMHS from caregivers of children with and without SLCN
2
, in order to explore both caregiver- and child-relevant communication barriers, and to consider the possible relationships between communication difficulties and therapy pathways. Specifically, the following questions were asked: (1) According to caregivers, how effective is communication between themselves and their CAMHS teams? Does this differ for caregivers of children with SLCN? (2) How well do caregivers think CAMHS staff communicate with their children? Do caregivers believe CAMHS staff understood and made reasonable adjustments for their child’s communication level, and does this differ across SLCN and non-SLCN families? (3) How do caregivers describe their child’s mental health after accessing CAMH services, and how do the groups compare?
Method
Recruitment
The survey data was obtained using a convenience sample. The survey was hosted on Qualtrics and made available to participants via social media platforms. It was posted on groups for parents of children with Special Educational Needs (SEN) and for parents of children referred to UK CAMHS, where they were invited to complete the online survey via a secure City St George's, University of London Qualtrics link.
Participants were not incentivised to take part in the study, and their responses were anonymous. If participants indicated that they did not have a child who had been referred to CAMHS, they exited the survey following that question. Participants were also excluded if they did not live in the UK. In total, 85 participants were included in the study.
Participants
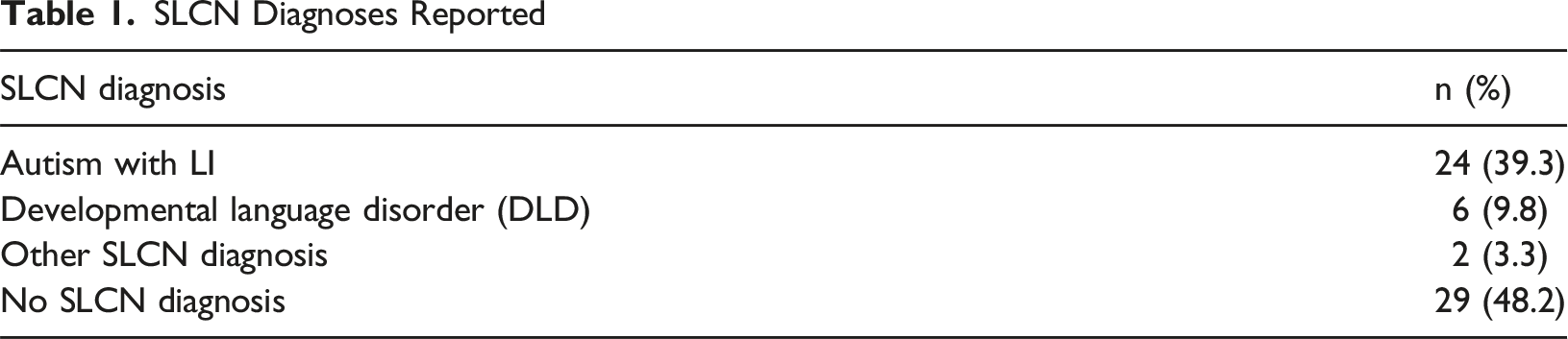
SLCN Diagnoses Reported
Participant Demographics
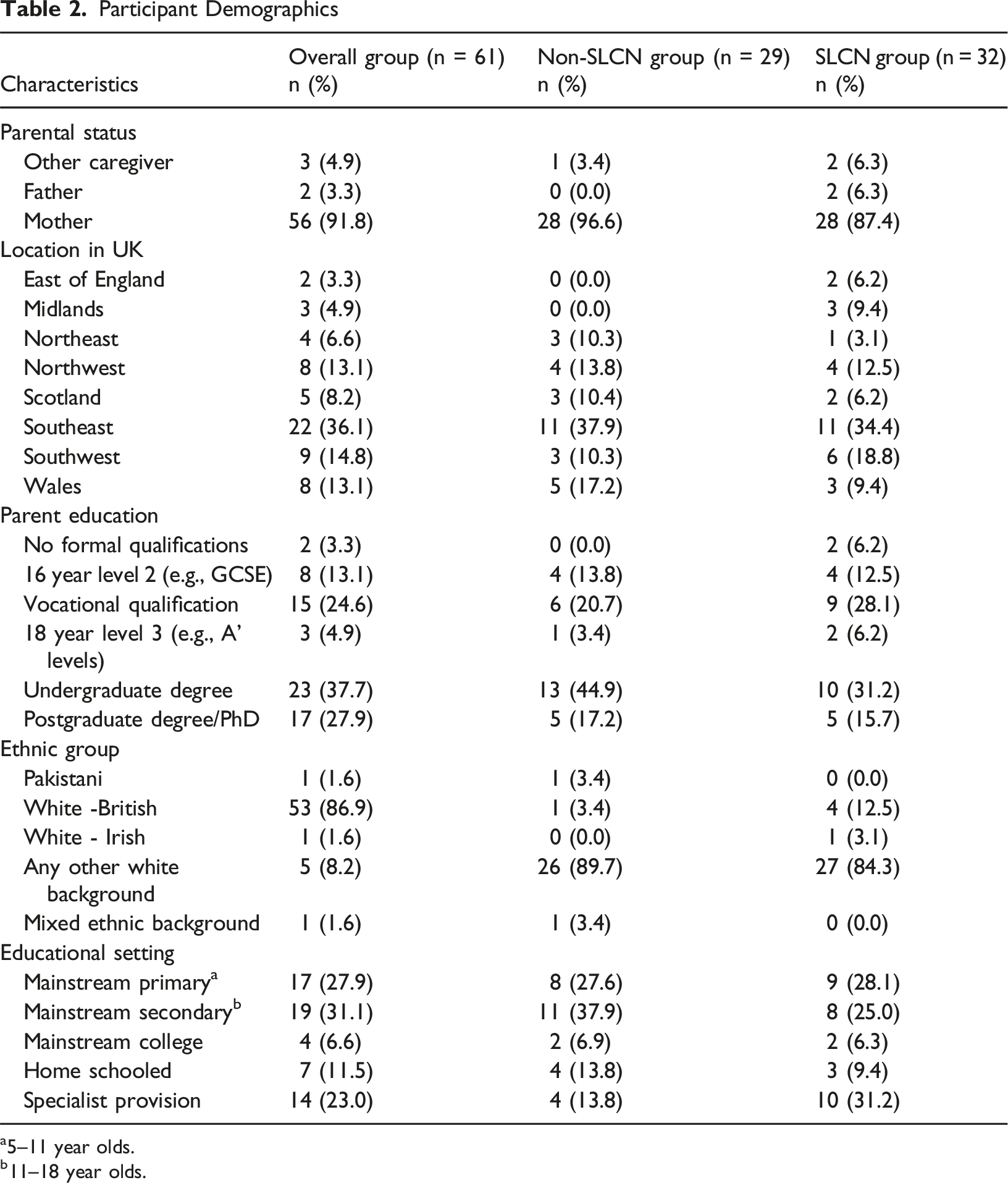
a5–11 year olds.
b11–18 year olds.
Participants described their children as ranging in age between 4 and 24 years (mean = 12.2, SD = 3.9 3 ) The children consisted of 43 males (70.5%; 24 SLCN) and 18 females (29.5%; 8 SLCN). The average age at which children were referred to CAMHS was 8.4 years (SD = 3.5). Reasons for referral were reported as mood issues (32; 52.5%); behavioural issues (22; 36.1%); or other reasons (7; 11.5%). Information about number of referrals revealed that most children (35/61; 57.4%) had only been referred once, with 8 (13.1%) referred twice, and 14 (23.0%) referred 3 times. Four people (6.5%) did not answer this question. As noted above, there were no differences between the SLCN and non-SLCN families on any child or demographic variables.
Materials
The wider survey was developed by staff and Speech and Language Therapy students from City St George's, University of London. The aim of developing the survey was to gather quantitative information about the views of parents whose children had accessed CAMHS. The survey was exploratory in nature and focussed on the views of caregivers of children with and without SLCN, the impact of those difficulties on accessing and engaging with CAMHS, and treatment outcomes. Two members of the research team had lived experience of children with SLCN who had accessed CAMHS which informed the questions, but no other co-design or Patient and Public Involvement and Engagement (PPIE) was employed.
The current paper focusses mainly on survey questions relating to communication specifically as well as the perceived impact of CAMHS involvement for children with and without SLCN. However, the complete survey which contained 55 items, can be found in Supplementary Materials. The specific research questions outlined in this paper were addressed by exploring the following survey items.
RQ1: Communication Between Caregivers and CAMHS
To address parents’ views of the language used by CAMHS, and if the views of parents of children with DLD were different to parents of children from the other SLCN diagnosis groups, the survey asked, ‘How easy was it to understand the language used in discussion, letters or advice given to you about your child?’. There were seven possible ranked options with ‘Extremely easy’ scoring 1 to ‘Extremely difficult’ scoring 7. A series of six yes/no questions on caregiver-facing communication were also asked. These covered whether the structure of sessions was made clear; whether caregivers felt they had been told what the aims of the intervention were; whether they were given enough time to ask questions; whether respondents felt that their views had been gathered and respected; and whether caregivers felt they had been listened to; and finally whether caregivers felt informed generally about what CAMHS could provide.
RQ2: Communication Between Children and CAMHS
Participants were asked to indicate their level of agreement with the following six statements, on a 7-point scale, where ‘Strongly disagree’ scored 1 and ‘Strongly agree’ scored 7. Because of the large overlap between communication needs and mental health issues, some of which may go unidentified, all parents were asked the questions about communication and their child. However respondent numbers varied on these questions from 52 to 63. *The CAMHS team therapists attempt to compensate for my child’s communication needs *The CAMHS team use a number of strategies to compensate for my child’s communication needs *My child’s CAMHS therapist understood their particular language and communication needs and how they impact on MH *My CAMHS therapist seemed knowledgeable about the impact of communication needs on everyday life *The CAMHS team always notices when my child does not understand something. *My child’s language and communication needs were a barrier to getting the most out of therapy.
RQ3: Mental Health after Accessing CAMHS
We were interested to hear caregiver perceptions of any improvements after accessing CAMHS. Two key questions were asked again using a 7-point scale from ‘much worse’ to much better’. The first question was about the child’s ability to talk about their feelings/emotions as a result of accessing CAMHS; the second asked how caregivers would describe their child’s mental health after accessing the service. We also asked how successful parents perceived CAMHS to have been rated as ‘not successful’; ‘it helped a little bit’ or ‘very successful’.
Procedure
The survey reported in this paper was approved by the City St George’s, University of London research ethics committee (Ethics no: ETH1819-1975). The survey was opened on 26 November 2019 and closed on 17 January 2020. The survey was preceded by an information page for participants. They were informed that the survey would take approximately 15 minutes to complete, that they could stop responding at any time, and that responses were anonymous. Prior to carrying out the survey, participants were required to indicate that they understood the study requirements, how the data would be held and used, that the information was anonymous and confidential, and that participation was voluntary. Consent was gained at the start of the survey using ‘required choice’ feature so that they could not progress until all boxes were confirmed.
Statistical Analysis
Descriptive statistics were used initially to consider the data for the sample as a whole. Independent t-tests and chi-square analyses were then performed to examine differences between groups. A two-tailed significance level of p<0.05 was applied across tests. Note that varying numbers of participants answered each question, thus, each analysis states the number of respondents reported. In addition to the scales above, caregivers were given the opportunity to give free text responses. In total, 18 caregivers left open-text comments, and these are used to support quantitative data where appropriate. Each comment is from a different respondent.
Results
RQ1: Communication Between CAMHS Teams and Parents
Participants’ Ease of Understanding of General Communication by CAMHS
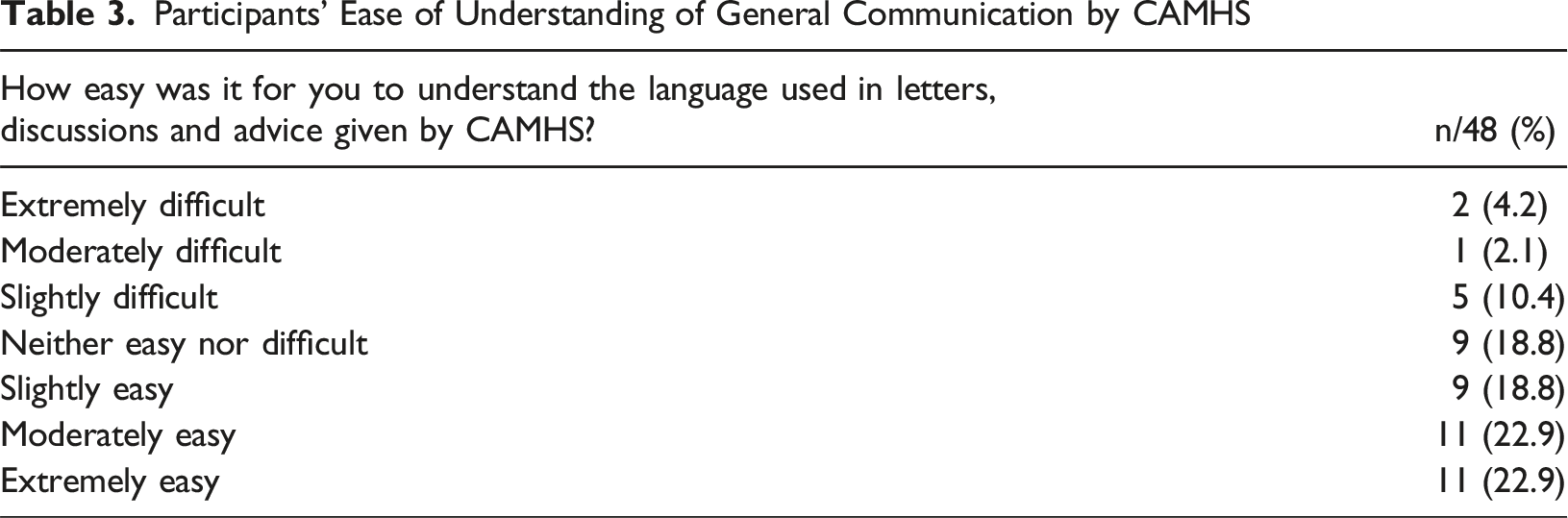
In addition, some parents commented about the content of information in the free text item: “Personal information about my daughter was sent to us after being told that would not be the case”; “Whilst waiting, we were initially discharged; then I made a complaint and they agreed to reconsider. I heard that they are discharging again, but the letter contains inaccurate information and is flawed”.
Caregivers also answered yes/no questions on parent-facing communication. In total, 29/48 (60.4%) said the structure of sessions was not made clear; 29 (60.4%) did not feel they had been told what the aims of the intervention were; 31/48 (64.6%) said they were not given enough time to ask questions. and two thirds did not feel they had been given enough information to get extra support (32/48; 66.6%). Using a three-point scale, 12/48 (25%) of respondents felt that their views had not been gathered and respected; while 26 (54%) reported that they felt ‘somewhat uninformed’ or ‘very uninformed’ generally about what CAMHS could provide. There was no difference between SLCN and non-SLCN families (all p values >0.72).
RQ2: Communication Between CAMHS Teams and Children
Ratings for Communication Knowledge and Adjustments as Perceived by Caregivers (n = /61; %)
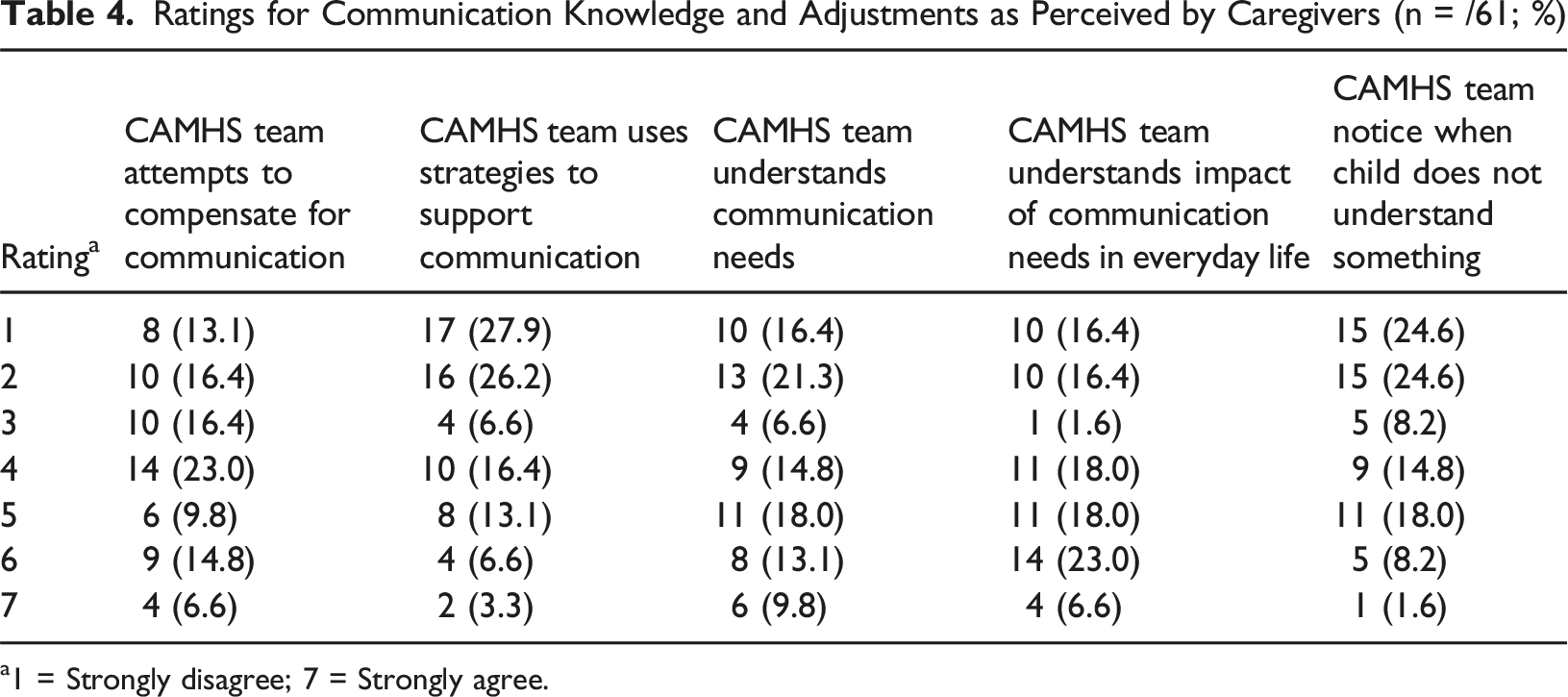
a1 = Strongly disagree; 7 = Strongly agree.
There were no differences between SLCN and non-SLCN families on any of these scales (all p values >0.49). However, the lack of adjustments was highlighted in one powerful SLCN caregiver comment: “Refused several times until tribunals. Still dismissed, as CAMHS said the talking therapy CAMHS offer was not suitable for kids with DLD. SLT not involved and don’t talk with CAMHS. So no support. Just left to rot.”
Another parent added: “My child barely leaves the house yet was expected to attend clinic appointments, wait in a busy waiting room with much younger children and clearly distressed teens. As she finds this difficult, she was labelled as ‘not engaging’ with CAMHS and threatened with discharge from the service with no help offered”.
When asked what adjustments were used by CAMHS that caregivers were aware of, there were 36 responses: 9/36 reported short sentences, 9/36 simplified language, 5/36 visual prompts, and 13 ‘other’ (unspecified) adjustments. The remaining participants did not respond to this item.
The issue of overshadowing of mental health difficulties by communication diagnoses was not asked about directly in the survey, however families commented on this in the free text. One wrote: “Our CAMHS will not treat a child for mental health if they have DLD or autism”; and another said “CAMHS will not offer any work for anxiety for my son because they say it’s autism- related, implying that autistic YP don’t develop MH issues”. However, some more positive responses from caregivers were also noted “CAMHS noticed very quickly that although my child is verbal but he wouldn’t communicate with them and found it very stressful, they provided me with the strategies I needed to support him at home. I was at ease that he wasn’t going to be forced into a situation that could make his anxiety, vocal and motor tics worse”.
RQ 3: Discharge and Mental Health after Accessing CAMHS
For this research question, 54 caregivers responded to the three items (SLCN = 27; non-SLCN = 27). In total, 24 participants (42.9%) viewed their child’s mental health to be ‘about the same’ following CAMHS therapy. Furthermore, over a third of participants in total reported that their child’s mental health had got worse (20/54; 35.7%); ‘much worse’ (7/56; 12.5%), ‘moderately worse’ (9/56; 16.1%) or ‘slightly worse’ (4/56; 7.14%) (see Figure 1). Child’s mental health after accessing CAMHS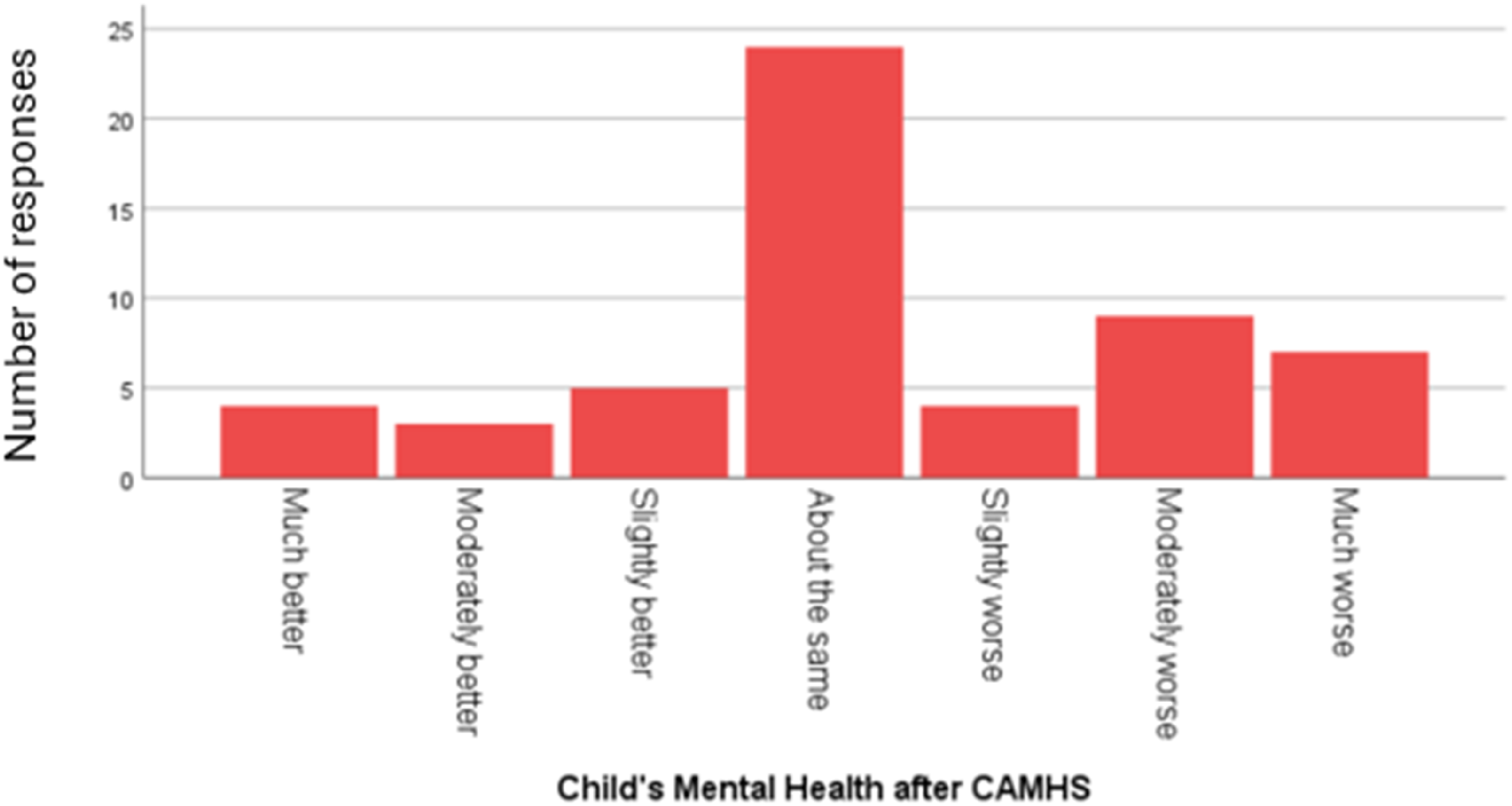
Similarly, when asked whether children were more able to talk about their feelings and emotions after CAMHS contact, 14 (26%) reported that this had worsened, 33 (61%) said it was about the same, and for 7 (13%) things had improved. For this item, caregivers of children with SLCN reported a significantly poorer picture with 10/27 SLCN children reportedly ‘worse’ compared to 4/27 non-SLCN children (χ2 (5) = 14.7, p = 0.012). This was the only difference found between SLCN and non-SLCN children. Furthermore, some parents commented that their child’s communication disorder diagnosis appeared to be preventing access to CAMHS or precipitating discharge: “Only received assessment then discharged without input - difficulties because of ASD therefore ‘nothing could be done’”; “CAMHS simply diagnose ASD or ADHD, and post diagnosis then strike you off their lists”; “She was refused to be seen until both parents have been on an ASD course. She is out of school due to anxiety currently”.
Discussion
This paper explicitly investigates the role of communication in perceived barriers to mental health services for children. Although the association between mental health problems and communication difficulties is known, the experiences children with SLCN and their families accessing CAMHS for co-occurring mental health issues, are still not well understood. The findings raise several key issues related to the importance of communication at all levels, and for all clients.
Communication to Parents
In general, participants felt that they did not have enough information about the sessions, and that their views had not been gathered effectively. This reflects the report by Hansen et al. (2021) where 60% of caregivers felt they had a lack of information about where to seek help and a similar proportion said that professionals did not listen to them. This is an important message for clinical patient-collaboration initiatives going forward. However, it is notable that it was not the language per se that was used by CAMHS in discussion, letters or advice to be difficult which was a barrier. This contradicts Bennett et al.’s (2012) findings that the CAMHS letters sent to patients were not appropriately readable. There may be multiple reasons for this difference. Firstly, Bennett et al. (2012), analysed the letters to ascertain how readable they were for adolescent patients, using standard tools. In contrast, this study asked parents their opinions, using a broader question about their perspectives of the language used by CAMHS. In addition, Bennett et al.’s (2012) study focused on the clinical letters written by one CAMHS team, therefore their results may not be generalisable to the wider UK population. It may also be that letters and other communication have improved since the Bennett et al. study. Within our sample there was a significant minority who reported that the language used was ‘extremely difficult’ to understand, and there were reports of inaccuracies in the communication. Future studies could assess the specific features which made this communication so challenging for some, since communication to caregivers should be accessible to all families.
Communication with Children and Compensatory Strategies
Alongside limitations in caregiver communication, most participants did not think that any strategies had been used by the CAMHS team/therapist to compensate and accommodate for their child’s language needs. Surprisingly, this was true whether or not children had formal SLCN diagnoses. Similar to Ashworth and colleagues (2025), there was a perception from caregivers that there was limited professional knowledge of communication needs and how to support them, including feelings that team did not always notice when their child did not understand something. It is very important to note that this perception may not reflect actual practice, and may instead be due to lack of caregiver awareness about the adjustments being employed by CAMHS professionals. Nevertheless, a more informed and positive perception of clinicians by caregivers would be constructive in providing the most effective support. Caregivers often rely on support from CAMHS professionals to manage home life with children who have SLCN, and parental engagement in strategies to support the mental health of children with SLCN is recognised as beneficial in the literature (Prizant et al., 2003). A more integrated family approach is therefore likely to be useful to CAMH services, even though this is not always implemented (Stolper et al., 2024).
Mental Health After Accessing CAMHS
Over a third of caregivers in this survey believed their child’s mental health had become worse since accessing CAMHS. One explanation may be that limited resources have negatively impacted some experiences of CAMH service delivery, so that optimum support is not provided. According to the Children’s Society (2016) local authority spending on early intervention for children, young people and families fell by 31% between 2010 and 2014, and NHS CAMHS expenditure also decreased in real terms. This may mean that professionals do not have time or capacity to train or tailor sessions adequately in relation to communication difficulties. Caregiver perspectives may also be influenced by their own mental health or previous experiences with mental health services - the association between parent and child mental health difficulties are well reported (Low et al., 2012; Singh et al., 2011; Wilkinson et al., 2013). It is also possible that the parents in this study had unrealistic expectations about the impact that CAMHS intervention would have on their child’s mental health (Ronzoni & Dogra, 2012). Finally, it may be that the children’s mental health difficulties would have become even worse without CAMHS intervention. Studies need to employ control group methodology with children not currently accessing CAMHS to unpick this further. Nevertheless, as discussed above, family attitudes towards CAMHS are likely important for successful intervention. Communication focussed initiatives to address caregiver concerns could be a very cost-effective method of increasing patient satisfaction and removing barriers to therapy.
It is worth noting that families of children with SLCN were significantly more likely to report poorer outcomes after contact with CAMHS than non-SLCN families. Young people with SLCN are particularly at risk of experiencing anxiety (Botting et al., 2016). For example, approximately 40% of autistic people experience symptoms of at least one anxiety disorder at some point, compared with 15% of the general population (National Autistic Society, 2020) and are more likely to be referred for these difficulties (Meltzer et al., 2005) than non-autistic children. Given this, it is surprising that in the current study some caregivers reported a disregard for anxiety as an additional treatment need, once an autism diagnosis had been made. While it is likely that CAMHS staff are familiar with autism, due to mandatory training initiatives (e.g., The Oliver McGowan Mandatory Training on Learning Disability and Autism), awareness of other types of SLCN may be lower due to limited research in this area (McGregor, 2020). The recent changes in criteria and terminology for developmental language disorder (DLD) may increase practitioner understanding of this condition and positively impact CAMHS practice (Bishop & CATALISE team, 2016). Finally, staff training in communication and neurodiversity is often relatively broad-brush and untailored to healthcare role. Therefore, it may not adequately meet the complex training needs of CAMHS professionals (Babalola et al., 2025) and providers need to consider bespoke training packages. These need not necessarily be expensive ‘therapy modification’ programmes, rather more in-depth knowledge of language processing and communication strategies that can be applied in a complementary way existing to clinical expertise and practice. Further research is needed to understand these training needs in more detail.
Limitations and Areas for Future Research
This study is a relatively small and preliminary exploration of parent views of CAMHS in the context of SLCN, but it contributes important additional knowledge about the role of (both caregiver and child-facing) communication specifically. While the caregivers who took part represented a reasonable spread of educational and ethnic backgrounds, the online nature of this survey may have recruited a particular subsample of families, and excluded those with no easy access to the internet or who do not use social media (where our recruitment links were posted). It is especially important to note that CAMHS provision varies widely across geographical regions, and we did not request information about whether families encountered generalist or specialist services. We also have no information about primary languages spoken at home.
It is important to note, that it is not possible to definitively say whether the experiences reported are about communication barriers specifically or whether these were more holistic impressions reflecting the range of clinician expertise and service. Furthermore, some of the more negative findings may be an artefact of these self-selected participants, who may have had particularly poor experiences of CAMHS and/or had higher personal capacity and were thus motivated to have their voice heard through this research. Research using more objective measures of mental health progress in children and adolescents with and without SLCN is also warranted. Future research should focus on identifying a larger group of caregivers whose children have been referred to CAMHS. With increased statistical power, this may reveal significant differences between groups with different/no SLCN diagnosis. Furthermore, we have combined families with autistic children and those with children who have DLD in this paper. This was partly due to unequal numbers in the groups, but also because of reported language similarities (Huang & Finestack, 2020), and because our groups did not differ. Nevertheless, larger and more equally distributed samples would allow a more nuanced comparison of subgroups of children with SLCN. For example, communication barriers are likely to vary in line with the child’s age, diagnosis, and other important factors that could not be examined in detail here; caregiver- and child-facing communication strategies, while related, are also likely to be different. In-depth interview studies would also be beneficial to understanding these more complex relationships, and for elucidating caregiver’s perspectives around communication strategies in more depth.
Given our results, closer working with caregivers about communication adjustments and within therapy strategies would appear worthwhile. Lynch and colleagues (2023) highlight that caregivers can act as “dynamic and essential pathway agents in helping or hindering young people with accessing and staying engaged in professional mental health care” (p.3350). We acknowledge that this survey has not fully addressed the central role that caregivers can play as communication intermediaries during mental health care, and that further investigation of informal support is needed. Alternative and creative methods to support children with communication need to be considered. However, in order to develop resources, further research involving the CAMHS professionals’ perspectives of the compensatory strategies they use is needed, along with better documentation of the availability of SLCN training, existing guidelines, and support for staff working with children who have communication needs. Although CAMHS practitioners are often trained in interventions for learning disability and autism (Fonagy & Pugh, 2017), the need for specialist expertise for different groups of children with communication needs has been highlighted (Hindley & Whitaker, 2017). Outside of CAMHS, preventative and wait-list approaches such as play-based working, psychoeducation and other community-based support may be useful and may help to improve access and alleviate strain on mental health services (see Francis et al., 2022 for a review).
Finally, this study did not seek the opinions of young people themselves. However, actively engaging young people, including those with SLCN, is crucial to developing successful person-centred care (Boyden et al., 2013).
Implications and Conclusions
This study has highlighted some of the communication barriers when accessing CAMHS as perceived by caregivers. Talking therapy is a widely used intervention in CAMHS, and it is therefore essential that clients can access these regardless of whether they have SLCN. Even if families experiencing these barriers are in the minority, efforts are needed to ensure that all families can access treatment effectively. Contrary to our expectations, our findings suggest that it is not just children with a diagnosed SLCN who experience communication barriers within CAMHS. Thus, a more universal consideration of communication difficulties in children encountering mental health services deserves consideration including language screening as a routine part of CAMHS assessment. This would assist CAMHS professionals in making appropriate adjustments, increase their knowledge and understanding of SLCN, and ultimately better enable CAMHS teams to deliver effective and efficient intervention.
Supplemental Material
Supplemental Material - Caregiver Views of Communication Barriers Within Child and Adolescent Mental Health Services: Children With and Without Speech, Language and Communication Needs (SLCN)
Supplemental Material for Caregiver Views of Communication Barriers Within Child and Adolescent Mental Health Services: Children With and Without Speech, Language and Communication Needs (SLCN) by Sue Livermore, Jessica Botting, Nicola Botting in Clinical Child Psychology and Psychiatry.
Footnotes
Acknowledgments
The authors would like to thank the caregivers who took the time to complete the survey.
Ethical Considerations
The survey reported in this paper was approved by the City St George’s, University of London LCS proportionate ethics committee (Ethics no: ETH1819-1975). The survey was preceded by an information page for participants. They were informed that the survey would take approximately 15 minutes to complete, that they could stop responding at any time, and that responses were anonymous. Prior to carrying out the survey, participants were required to indicate that they understood the study requirements, how the data would be held and used, that the information was anonymous and confidential, and that participation was voluntary.
Consent to Participate
Consent was gained at the start of the survey using ‘required choice’ feature so that they could not progress until all boxes were confirmed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
An anonymised version of the dataset is available from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.