
Abstract
Young people in OOHC have complex mental health concerns, therefore the South Western Sydney Local Health District (SWSLHD) has trialled a tiered model of mental health care. Under this model the OOHC mental health team (OOHC-MHT) provides specialist tier four service delivery for those with the most severe, intense mental health needs. OOHC consumers with a reduced level of severity access services at a tier three centre-based iCAMHS. This study aims to understand the characteristics of young people in OOHC accessing different service provision options in Sydney, Australia. Sixty-six OOHC consumers 8–17 years accessing mental health services across SWSLHD from January 2020–December 2021 participated in the study. Group differences in OOHC-MHT and iCAMHS outcome measures were compared. HoNOSCA scores were significantly worse for OOHC-MHT than iCAMHS, indicating more severe psychopathology for OOHC-MHT at baseline. In OOHC-MHT, HoNOSCA decreased significantly from admission to discharge and scores on the CGAS increased significantly, indicating significant improvements in psychopathology and functioning. In the iCAMHS group scores on the HoNOSCA significantly decreased indicating improved psychopathology over this period. These findings support a tiered model of service delivery for OOHC consumers, with this tailored level of care resulting in significantly improved outcomes across a range of complexity.
Keywords
Introduction
Annually, there are over 46,000 young people in Australia placed in Out-Of-Home-Care (OOHC) (Australian Institute of Health and Welfare, 2022) due to child protection concerns related to violence, abuse and neglect. There is higher proportion of Indigenous children represented in OOHC with the national rate estimated to be 11 times more than that for non-Indigenous children, although Indigenous children account for less than 6% of the overall child population (Australian Institute of Health and Welfare, 2022). Early trauma and disrupted attachments with primary caregivers have significant implications for the mental health and functioning of these vulnerable young people.
Young people in OOHC are 5.3 times more likely to have been diagnosed with a mental disorder compared to same-aged peers with no child protection history (Green et al., 2020). For those children placed in OOHC in early childhood, by middle childhood they are 12.3 times more likely to have a diagnosis of Attention Deficit Hyperactivity Disorder (ADHD), 11.8 times more likely to have a diagnosis of conduct disorder (CD), and 10 times more likely to be diagnosed with stress reactions (physical or psychological changes occurring in response to a stressful event, such as changes in heart rate, blood pressure, anxiety or irritability). Overall, between 50 and 80% of children in OOHC meet criteria for a mental health disorder (Delvin et al., 2022; Farmer et al., 2001; Leslie et al., 2005).
The multifaceted mental health concerns for the young people in OOHC necessitate more complex service provision than standard mental health care (Foord et al., 2022). Recommendations for service provision for this population include: specialised service provision with a narrow scope of practice (i.e. those in OOHC only); a practice framework which encompasses a clinical psychosocial-developmental model, rather than solely clinical; clinicians who demonstrate expertise in trauma and the associated difficulties, including attachment disruptions; long-term engagement; strong and frequent systemic collaborations with all stakeholders involved with the young person, and; ease of access to the service for the young person (Tarren-Sweeney, 2010).
Owing to the complex service needs of young people in OOHC, South Western Sydney Local Health District (SWSLHD) trialled a tiered model of care with specific adjustments to cater for these unique needs. The tiered framework was originally recommended in the UK by the NHS Health Advisory Service Report (NHS Health Advisory Service, 1995). Under this framework, mental health services are distributed across four tiers with increasing levels of service provision complexity and specialisation. The OOHC Mental Health Team (MHT) is a specialist tier 4 service model which employs assertive outreach to the young person and their carers in their preferred place of service engagement (e.g. placement/home, school, a local café or park). Tier 4 services aim to meet the needs of young people with the most complex, severe and persistent mental health needs and provide highly specialised services for specific niche demographics (McDougall et al., 2008). Clinicians on the team have had training in attachment and family-based interventions, and have expertise in trauma-informed care. Caseloads are reduced to support clinicians to engage in intense systemic collaboration and frequent inter-agency contact (meetings, case conferences, phone calls, joint visits), as well as client advocacy and more frequent and/or intensive client support. Improved mental health outcomes and reduced psychosocial impairment for young people in OOHC accessing the service have been found (Devlin et al., 2022).
The majority of young people in OOHC across SWSLHD do not meet the level of complexity required to access services at a tier 4 level, and consequently access mental health support via their tier 3 local infant, Child and Adolescent Mental Health Service (iCAMHS) teams or via tier 2 community health services. Clients can then be referred to the tier 4 level OOHC-MHT team if their needs are not able to be met through the lower acuity model of care or if their individual and/or systemic risk is so significant that it is deemed unlikely that their complex needs would be adequately met by a centre based iCAMHS. iCAMHS teams provide tier 3 specialist child and adolescent mental health assessment and interventions for the general community including those in OOHC. Referrals are received from tier one services such as General Practitioners, allied health, school psychologists/nurses or tier two services such as tier two services such as headspace (a publicly funded not-for-profit service for young people 12–25 with mild-to-moderate mental health concerns) and community health services or as a result of presentation to a local Emergency Department (ED). iCAMHS services are predominantly clinic-based, with usually hour-long sessions with clinicians having high caseloads (usually around 20 or more) which are typically double that of clinicians on the OOHC-MHT.
The current study aims to understand the characteristics of young people in OOHC accessing different service provision options in South West Sydney. Specifically, we aim to compare the demographic characteristics of young people in OOHC accessing general iCAMHS teams with those accessing services in the specialised OOHC-MHT. We would expect that those young people referred to OOHC-MHT are more complex, with significantly worse psychiatric and functional impairment at admission, in keeping with the tiered model of care of mental health services in SWSLHD.
We also aim to investigate the degree of change of routinely collected psychiatric measures of young people in OOHC accessing MH services in SWSLHD from admission to discharge, hypothesizing that these would indicate significant improvements in functioning for both OOHC-MHT and iCAMHS teams. This finding would be supportive of proportionate universalism – treatment as usual plus targeted additional support commensurate with individual needs.
Methods
This is a longitudinal cohort study using data derived from New South Wales (NSW) Health routinely collected outcome measures and demographic data. Ethics approval was granted from South Western Sydney Local Health District Human Research Ethics Committee (2020/ETH00863).
Services
SWSLHD covers a vast area of metropolitan Sydney with about 1.1 million people and upwards of 260,000 under 18 years of age. There are also approximately 2,400 children in OOHC in this region South Western Sydney District Data Profile, 2019). Triage information is usually entered by the clinician on intake and is discussed in a multi-disciplinary meeting attended by the service manager, psychiatrists and other allied health and nursing professionals. Severity is characterised by significant emotional and behavioural issues and their impact on functioning in placement, school and community, causing significant distress. The presence of psychiatric comorbidities, trauma, and risk are considered when deciding where to allocate consumers. Only the most severe clients and those who are unlikely to be able to be managed by the mainstream CAMHS service are allocated to OOHC MHT.
OOHC MHT
The OOHC-MHT is a tier 4 mental health service in the public setting including a ‘Whole of Family Team’ providing a preventative service for children at risk. Eighteen clinicians work across both teams from various multidisciplinary backgrounds: psychiatry, psychology, neuropsychology, mental health nursing, social work, drug health and Aboriginal mental health. Referrals are made via the statutory child-protection service in the district, Department of Communities and Justice (DCJ). Referrals are made for young people in OOHC who have complex and significant mental health concerns which are unable to be managed at a lower acuity general iCAMHS service. The service offers comprehensive multi-disciplinary systemic assessment, shared formulations and recommendations for multiple parts of the system, direct interventions such as Dyadic Developmental Psychotherapy, Dialectical Behaviour Therapy, Cognitive Behavioural Therapy, Narrative Therapy, Family Therapy, Art, Play Therapy and Pharmacotherapy among others. All interventions are attachment based and trauma-informed. Interventions are targeted across the individual, dyadic and systemic levels as per the unique needs of the young person. Intense and frequent collaboration, advocacy and systemic support is provided as part of routine practice. For this reason, caseloads are capped at about eight clients per clinician with acuity and complexity being the service entry drivers. Client capacity of the team is driven by acuity and need of those being referred. There is capacity to go above service capacity numbers temporarily until the least acute clients can be stepped down to a tier 3 service. Treatment duration is determined by the presentation and needs of the young person and usually continues until the young person and their supporting system feel that their needs can be safely met by a lower intensity service. Further details relating to the service have been described by Foord et al. (2022).
iCAMHS teams across SWSLHD
There are five iCAMHS teams across SWSLHD with boundaries as per the local government area (LGA) jurisdictions. These teams provide services to children and adolescents with moderate to severe mental illnesses and their family/carers. Each team is multidisciplinary, including: psychiatrists, psychologists, social workers, mental health nurses, and occupational therapists. Referrals are made through the primary care providers (e.g. General Practitioner), paediatricians, school psychologists, DCJ, headspace services, community health, directly from the ED and from child and adolescent inpatient mental health services and paediatric wards. Services are predominantly centre-based and typically a session is an hour in duration. Case-loads are usually upwards of 20 clients for a full-time clinician. These teams typically receive 10–20 referrals each week and generally are under constant pressure to transfer care of their less severe clientele in order to accommodate those who have more acute needs.
Participants
All young people in OOHC accessing mental health services in SWSLHD from January 2020 – December 2021 were recruited to the study. Ages ranged from 8 to 17 years (inclusive). For the purpose of this study, OOHC was defined as foster care, kinship care, previously removed and now self-placed with biological parent(s), group home, single or emergency placement.
In total, there were 66 young people included in the analysis, 22 of which were allocated to the OOHC-MHT group, and 44 of which were allocated to the iCAMHS group.
Socioeconomic status of participants was identified using the Socio-Economic Indexes for Areas (SEIFA; ABO, 2016), which is an aggregate measure based on the area of residence. The SEIFA score is a decile score of advantage and disadvantage using the postal code or locality of the young person.
Measures
NSW Health provides a list of mandated outcome measures to be collected from consumers at admission, 13-week intervals throughout engagement, and finally at discharge. For young people aged 8–17 years, clinicians must complete: The Health of the Nations Outcome Scaler for Children and Adolescents (HoNOSCA), Children’s Global Assessment Scale (CGAS) and the Strength and Difficulties Questionnaire (SDQ) – Parent Report and Self Report (for those aged 11–17).
HoNOSCA
The HoNOSCA (Gowers et al., 1999) is a clinician-rated measure of the psychiatric outcomes of a young person aged 5–18 years. It consists of 15 items which enquire about clinical and psychosocial functioning. Responses are made on a 5-point Likert scale (0 = no problems, 4 = severe problems). A score between 2 and 4 is of clinical significance and indicates a need for monitoring or intervention. The HoNOSCA has good-very good reliability, and is sensitive to change over a 3-month period (Brann et al., 2001).
CGAS
The CGAS (Shaffer et al., 1983) is a clinician-rated measure of global psychosocial adjustment and functioning. It is a score from 0 to 100, where lower scores indicate worse functioning. Scores greater than 70 are indicative of no clinically significant functional impairment. The inter-rater reliability of the CGAS is moderate when used in a clinical setting with clinician raters (Lundh et al., 2010).
SDQ – parent/carer report, self-report (11 – 17)
The SDQ (Goodman, 1997) is a consumer-rated screening measure of emotional and behavioural functioning. It is made up of 25 questions requiring answers on a 3-point scale (0 = note true, 1 = sometimes true, 2 = certainly true). The questions are derived from five subscales: emotional symptoms, conduct problems, hyperactivity/inattention, peer relationships and prosocial behaviour. There are separate forms for the parent/carer report and the self-report of the young person aged 11–17 years. There is no self-report correlate for those aged 10 years and younger. Strong longitudinal factorial invariance has been found for the SDQ (Sosu and Schmidt, 2017), supporting its use in research across time.
Procedure
OOHC consumers aged 8–17 years (inclusive) accessing mental health services across SWSLHD were identified and selected to participate in the study. All participants were allocated a participant number to ensure all data was de-identified. Participants were categorised according to their treatment group, either OOHC-MHT or iCAMHS (encompassing all centre-based iCAMHS services). Electronic medical records were scanned to obtain basic demographic information (sex, age, Aboriginal/Torres Strait Islander status, postcode to calculate SEIFA score, number of diagnoses, number of ED presentations for mental health in the year prior to service engagement). A research assistant also scanned medical records and triage information to obtain information pertaining to exposure to trauma, abuse and neglect, specifically: exposure to domestic violence, substance use, deliberate self-harm, suicide attempt. An informed consent waiver was obtained from the SWSLHD Ethics committee, given that all collected data was de-identified and there was no identifiable harm from inclusion in the study.
Admission scores on HoNOSCA, CGAS and SDQ were recorded. Duration of intervention and discharge measures were also collected at the end of engagement. Case records were kept despite missing data for many of the outcome measures.
Data analysis
All analyses were completed using SPSS 26.
Demographic statistics and comparisons between the OOHC-MHT and iCAMHS groups were completed initially. Data was explored on: gender, age, Aboriginal and/or Torres Strait Islander status, duration of treatment, socioeconomic status (SEIFA score), number of diagnoses, previous psychological intervention and ED presentations in the 12 months prior to admission. We also looked at key indicators of trauma and abuse as documented in medical records at the time of referral. Specifically, we explored data relating to: exposure to domestic violence, substance use, deliberate self-harm, suicide attempt and previous mental health ED presentation/s over the year prior to service admission. Chi-squared tests were used for categorical variables (with Fishers Exact Test correction) and t-tests were used for continuous variables.
At the time of admission, t test comparisons between OOHC-MHT and iCAMHS groups were made for the three quantitative outcome measures: HoNOSCA, CGAS and SDQ.
OOHC-MHT and iCAMHS groups were analysed for change over time separately given the inherent differences in complexity between the groups due to the tiered model of service delivery. Outcomes were assessed for the two groups using Paired-Samples t-tests for admission and discharge scores for HoNOSCA, CGAS and SDQ measures.
Results
Demographic characteristics
Descriptive statistics
Mean age at admission was 14.5 years (SD 2.1) and 13.3 years (SD 2.3) for iCAMHS and OOHC-MHT groups respectively. OOHC-MHT consumers were significantly younger in age compared to those in the iCAMHS group (t(38.673) = 2.166, p = .037).
SEIFA score for the iCAMHS group was 4.55 (SD 2.7), whilst SEIFA score for the OOHC-MHT group was 3.23 (SD 2.3). Lower SEIFA scores are indicative of socioeconomic disadvantage. The OOHC-MHT group had significantly more socioeconomic disadvantage compared to the iCAMHS group (t(48.5) = 2.028, p = .048).
There were no differences between the groups on sex (c2 = .525, df = 2, p = .769) or on any of the indicators of exposure to trauma (substance use, suicide attempt, deliberate self-harm, exposure to domestic violence, previous mental health ED admission in the past year). There were no differences between the groups on the number of psychiatric diagnoses, or on Aboriginality status after Fishers Exact Test correction.
The OOHC-MHT group had a significantly longer period of intervention compared to the iCAMHS group (t(48.643) = −2.666, p = .01, OOHC-MHT = 452 days (SD 185), iCAMHS = 315 days (SD 217)).
Outcome measure comparisons between OOHC-MHT and iCAMHS groups at admission
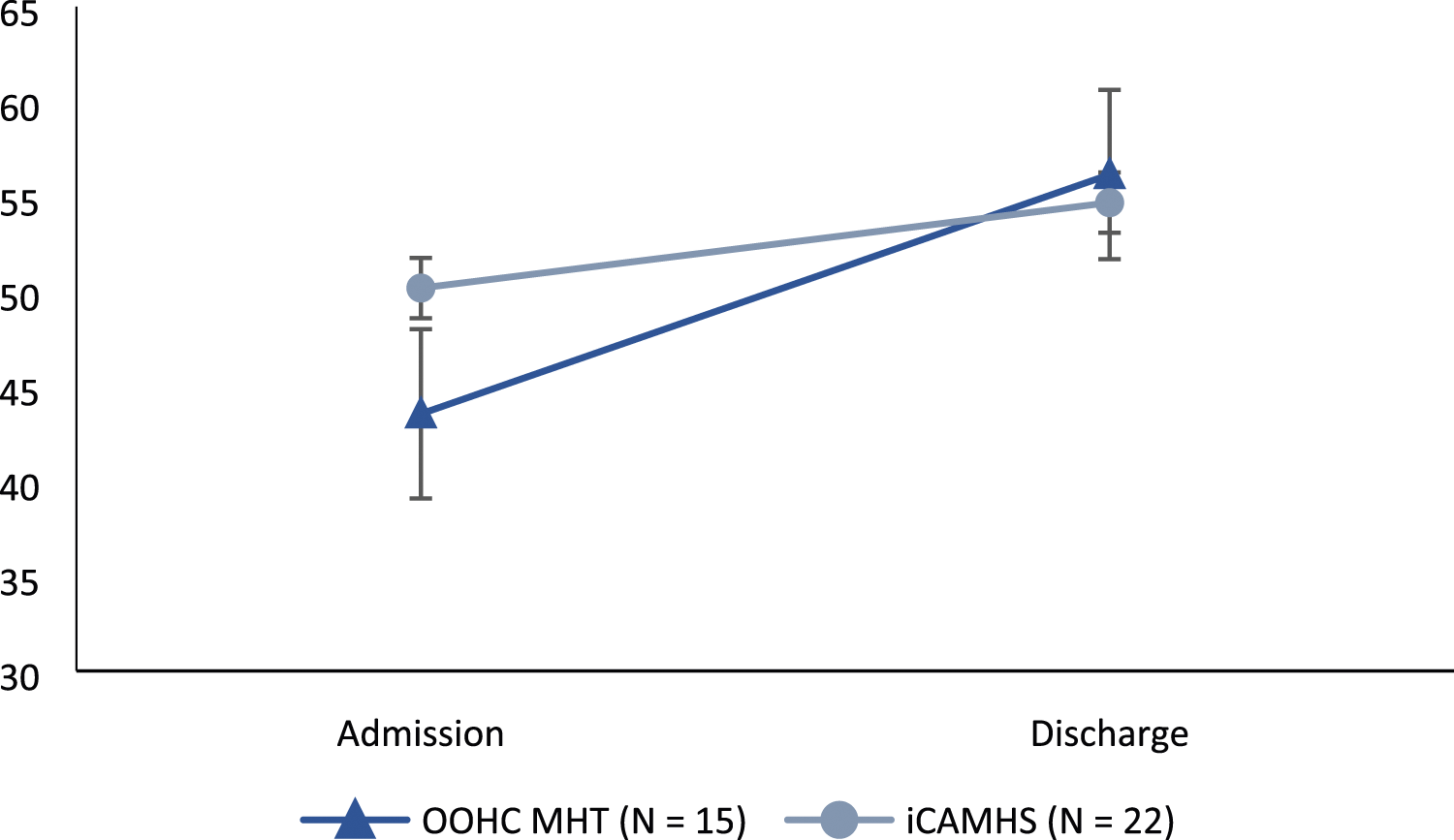
As expected, the OOHC-MHT group scored significantly worse on the HoNOSCA (t(37.094) = −3.155, p = .003; M (OOHC-MHT) = 22.65 (SD 6.97); M (iCAMHS) = 16.65 (SD 6.37)), CGAS (t(41.936) = 3.069, p = .004; M (OOHC-MHT) = 45.15 (SD 5.34); M (iCAMHS) = 53.61 (SD 13.84)), and SDQ (t(27.991) = −2.374, p = .025; M (OOHC-MHT) = 23.27 (SD 6.59); M (iCAMHS) = 17.6 (SD 6.48). For the HoNOSCA and SDQ, higher scores indicate worse functioning, whereas on the CGAS, higher scores indicate better functioning.
Change over time for psychiatric measures from admission to discharge
OOHC-MHT group
Scores on the HoNOSCA decreased significantly from admission (M = 21.8, SD 5.98) to discharge (M = 15.8, SD 7.51) (t(14) = 3.296, p = .005), and scores on the CGAS increased significantly from admission (M = 43.54, SD 4.68) to discharge (M = 56.15, SD 12.1) (t(12) = −4.032, p = .002), both indicating significant improvements in psychopathology and functioning for those in the OOHC-MHT over that time period. Scores on the SDQ also decreased from admission (M = 21.57, SD 5.62) to discharge (M = 14.43, SD 6.65), indicating improvements in functioning, however this result was only approaching significance (t(6) = 2.024, p = .089).
Figure 1 above is a representation of the difference between groups at admission and discharge, with error bars representing the standard error at each time point. While the OOHC-MHT group had a significantly poorer functioning at admission differences between groups could not be detected at discharge. Figure 2, below, shows how CGAS scores were undistinguishable between groups across both time points, however the OOHC-MHT group improved significantly, whereas iCAMHS did not. Scores on the HoNOSCA for OOHC-MHT and iCAMHS groups from admission to discharge. Note. Lower scores indicate better functioning and less psychopathology. Scores on the CGAS for OOHC-MHT and iCAMHS groups from admission to discharge. Note. Higher scores indicate better functioning.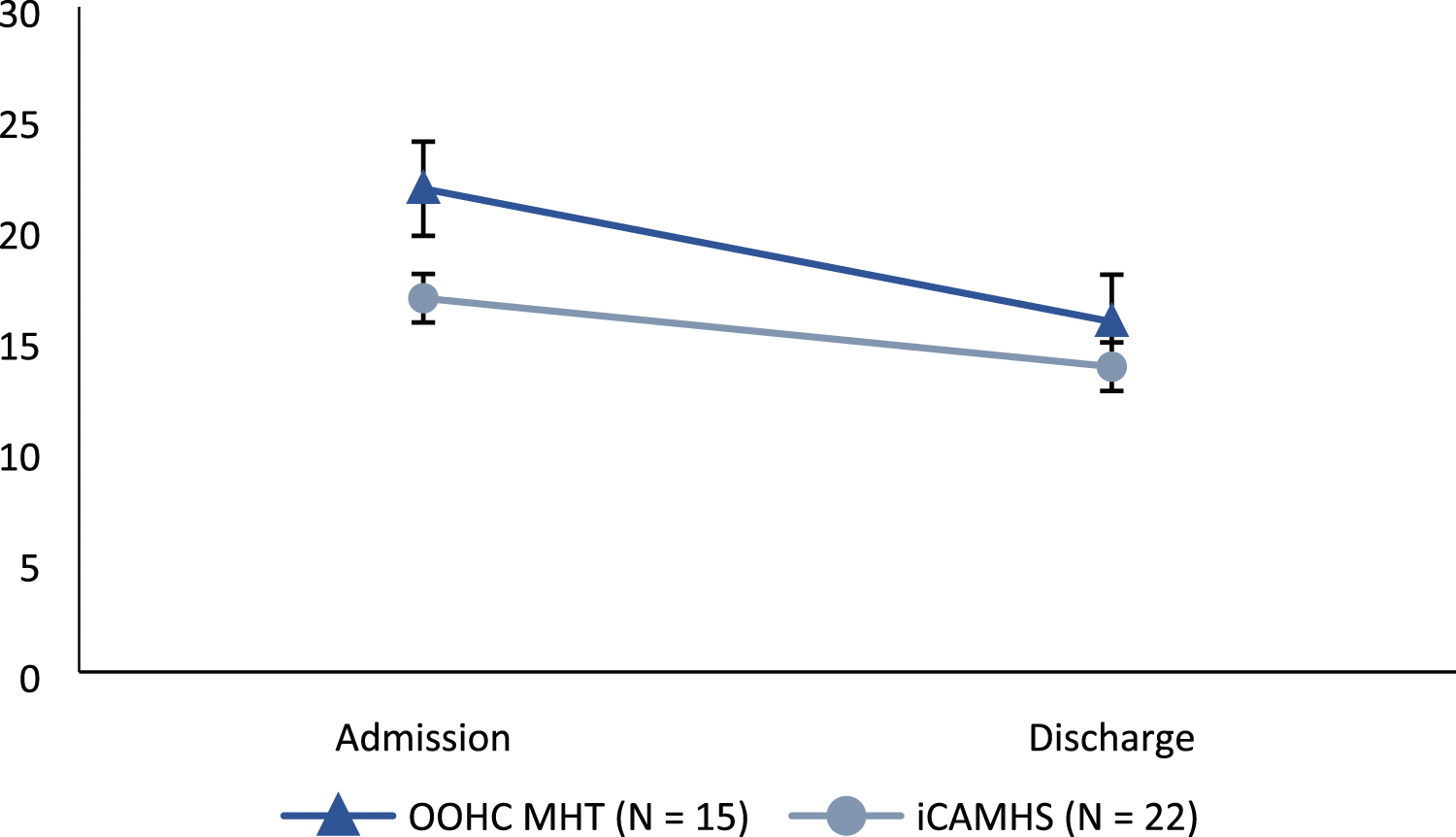
iCAMHS group
Frequency count of endorsed categorical descriptive group characteristics (%).
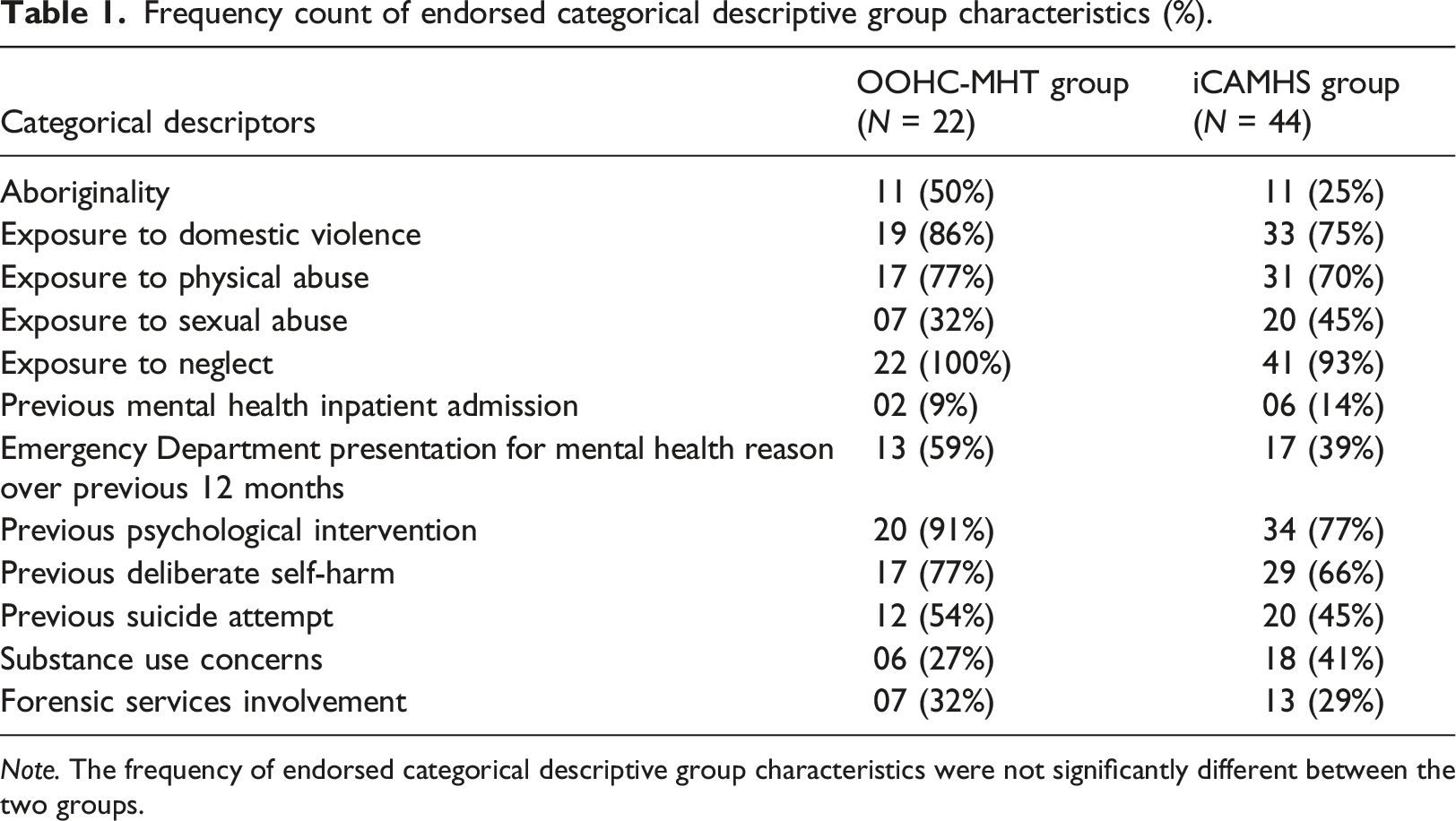
Note. The frequency of endorsed categorical descriptive group characteristics were not significantly different between the two groups.
Discussion
We explored the socio-demographic and clinical characteristics including levels of psychopathology and functioning of young people in OOHC accessing tiered mental health services across SWSLHD. We found that, whilst young people in the OOHC-MHT group did not significantly differ from those in the iCAMHS group on exposure to trauma variables, they did have significantly worse measures of psychopathology and functioning upon referral. Initial statistical analyses confirmed that the OOHC-MHT and iCAMHS groups were significantly different, with the OOHC-MHT scoring significantly worse on measures of psychopathology (HoNOSCA, SDQ) and functioning (CGAS). These results were indicative of successful tiered service allocation as per complexity and needs of young people in OOHC.
When looking at indicators of functioning over time from admission to discharge, it was found that there was significantly improved functioning for young people in OOHC accessing both services. Specifically, those young people in the OOHC-MHT group showed significant improvement on several measures of psychopathology and functioning (HoNOSCA, CGAS, approaching significance on SDQ). For those young people in the iCAMHS group, significant improvement over time was identified on the HoNOSCA but not in their level of functioning (CGAS). These findings again support a tiered model of service delivery for OOHC clients, with this tailored level of care resulting in significantly improved psychopathology outcomes for clients across a range of complexity, while also maximising best use of the available resources. It may be that we did not see a significant improvement in the level of functioning of those in the iCAMHS group, as these young people had higher baseline functioning, and therefore less room for improvement.
The OOHC-MHT was created as the local health district’s response to the inflated level of young people in OOHC in this region compared to other areas of the state (South Western Sydney District Data Profile, 2019). Research indicates that the features which contribute to better engagement for these young people in their mental health care is flexibility, collaboration, and stability over time (Kerns et al., 2014). The OOHC-MHT has been formulated to meet these key targets for those young people in OOHC who are most at risk. The goal of the service is to maximise engagement by providing services which are flexible, delivered via outreach to the young person, accessible over a wider geographical range (reducing the number of discharges due to placement change), and interventions which can be offered long-term providing critical continuity of care. The outcomes from the present study indicate that young people in OOHC accessing mental health services across the district are doing so in the way which was intended, with the most severe and at-risk young people in OOHC accessing treatment through the OOHC-MHT, thereby rationalising the allocation of scarce specialist mental health resources as per need.
Limitations of the study included incomplete data from clinical services and an associated insufficient number of responses available for more detailed analyses. Unfortunately, incomplete data entry is a clinical reality of real-world research, yet the scarcity of data on similar services highlights the need for further work in this area. Conducting research in real-world clinical settings brings inherent difficulties, including competing clinician demands, de-prioritisation for the completion of outcome measures, variable competence of staff in administering and scoring measures, and motivational issues relating to data collection. To bring about change in this area, mandatory training in the administration of outcome measures for all clinicians is crucial. Organisational and government sectors can also prioritise research outcomes by positively reinforcing clinicians who reach data targets. Clinician upskilling and support is required to continue research for these vulnerable youths.
The finding of significant differences in length of intervention was noteworthy, with young people accessing OOHC iCAMHS tier 4 intervention for significantly longer than standard centre-based care through iCAMHS. This is potentially due to OOHC-MHT service provision differences (assertive outreach, more flexible service delivery of higher intensity and duration, specialist complex trauma expertise), which have been identified as pivotal for successful engagement of young people in OOHC (e.g. Tarren-Sweeney, 2010). In addition, it is critical to consider the key elements which contribute to successful engagement and intervention with this very complex and challenging group of young people and their surrounding systems. These have been well detailed in a recent publication (Drever et al., 2022). One of the benefits of the OOHC-MHT is its provision of culturally informed service delivery which aims to meet the unique needs of this group. Aboriginal mental health clinicians form part of the OOHC-MHT and are present in all multidisciplinary meetings and provide direct culturally appropriate intervention to children and their carers who identify as aboriginal. In addition, it is important to consider other factors (e.g. duration of service involvement, number of placement changes) as alternative outcome measures, rather than relying solely on psychiatric symptom counts (Drever et al., 2022). We hope to explore and compare indices of engagement between services for young people in OOHC in future research.
This study provided valuable insights into the characteristics of young people in OOHC accessing mental health services, and how their level of functioning and psychopathology changed over time within a tiered model of care with interventions matching their needs. Future research delving deeper into the components of service delivery which maximise therapeutic engagement and subsequent clinical and functional improvement is needed. The finding of this study together with related recent and subsequent endeavours is crucial in order to provide guidance to the funders and service providers to develop fit-for-purpose service redesigns and enhancements to best meet the complex needs of probably the most vulnerable population in the developed world.
Footnotes
Acknowledgements
The authors declare that there are no funding bodies directly related to the content or preparation of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.