
Abstract
Psychological trauma and post-traumatic stress disorder (PTSD) are under-researched in autistic individuals. We explored the experience of trauma and PTSD symptoms in a sample of autistic adolescents (n = 30) aged 10–16 years (without a maltreatment history; 47% female), compared to a group of typically-developing (TD; n = 29) and a group of (non-autistic) maltreatment-exposed adolescents (n = 28), matched on key demographics. Caregiver reports indicated that a wide range of events were deemed traumatic to autistic adolescents, including those not meeting DSM-5’s Criterion A for trauma for a PTSD diagnosis (e.g., bullying and bereavement). Caregiver- and self-reports converged to show more severe PTSD symptoms, and higher rates of probable PTSD, in autistic adolescents (43–57%) relative to the TD adolescents (7–32%). Symptom severity and rates of probable PTSD were comparable between the autistic and maltreatment-exposed adolescents (50–54%), except that, for autistic adolescents, the index trauma mostly did not match DSM-5 criteria, whereas it did for maltreatment-exposed adolescents. This short report’s early findings supports the need for improved assessment of trauma exposure and PTSD symptoms in autistic adolescents. A flexible approach to how trauma is defined in this population may be needed, considering subjective experiences and autism-related processing differences.
Plain Language Summary
Psychological trauma and post-traumatic stress disorder (PTSD) are not well studied in autistic young people. We looked at experiences of trauma and PTSD symptoms in autistic adolescents aged 10–16 years (n = 30; 47% female) who did not have a history of maltreatment. We compared them with two groups of adolescents: typically developing (TD; n = 29) and maltreatment-exposed (n = 28), with similar ages and other key characteristics. Caregivers reported that autistic adolescents experienced a wide range of events as traumatic, including events that would not usually count as trauma under standard PTSD rules (DSM-5), such as bullying or the death of a loved one. Both caregiver and adolescent reports showed that autistic adolescents had more severe PTSD symptoms and higher rates of probable PTSD (43–57%) compared with TD adolescents (7–32%). Interestingly, the severity of symptoms and rates of probable PTSD in autistic adolescents were similar to those in the maltreatment-exposed group (50–54%). However, while the maltreatment group’s trauma usually met DSM-5 criteria, the traumatic experiences in the autistic group often did not. These early findings highlight the importance of recognising trauma and PTSD symptoms in autistic adolescents, even when the events do not meet standard definitions of trauma. Assessments may need to be more flexible and consider each young person’s subjective experience, as well as differences in how autistic adolescents process events. Overall, the study suggests that autistic adolescents can be highly affected by stressful or upsetting experiences, and mental health support should take their unique perspectives into account.
Introduction
Psychological trauma and post-traumatic stress disorder (PTSD) have historically been under-researched in autistic people (Hernández-González et al., 2023), but are increasingly recognised as a research priority by the autism community. PTSD appears to affect approximately 14% of autistic children and adolescents and 44% of autistic adults (Quinton et al., 2024; Rumball, 2018), compared to 7.8% developing PTSD by age 18 in non-autistic samples (Lewis et al., 2019) and 6.8–-9.2% of adults in the general population (Goldstein et al., 2016; Kessler & Berglund, 2005). Such estimates overall must be interpreted with caution, as they could be biased/inflated due to methodological issues, including confounding factors, lack of control comparisons, clinical sample recruitment, and reliance on single informants. Only one previous study has considered child self-report (Hoover & Romero, 2019) – an essential perspective as internalising symptoms can often be missed by informants (e.g., Lei et al., 2024). Further, maltreatment history is a major risk for PTSD (Copeland et al., 2007) and frequently co-occurs with autism (Davidson et al., 2022; Gajwani & Minnis, 2023) but is seldom accounted for.
What is perceived as “trauma” may be different for autistic people, and strict definitions of trauma could risk poor identification and support (Brewin et al., 2019; van den Berg et al., 2017). Rumball and colleagues (2020) found that over 40% of autistic adults met criteria for probable PTSD in response to events deemed as subjectively “traumatic” (e.g., bullying, bereavement, and relationship difficulties), but which did not meet the definition of trauma required for a PTSD diagnosis in the DSM-5 Criterion A – “exposure to actual or threatened death, serious injury, or sexual violence” (APA; American Psychiatric Association, 2013). Similarly, autistic adults and caregivers of autistic children, interviewed by Kerns and colleagues (2022), described various experiences as traumatic outside of standardised measures, including ones which reflected a conflict between autistic characteristics and the environment (e.g., sensory traumas). There has yet to be a quantitative exploration of PTSD symptoms associated with such experiences of trauma exposure in autistic individuals during adolescence, a period of peak mental health vulnerability (Solmi et al., 2021).
Our aim was to build on this important prior work to raise the possibility that our understanding of PTSD in autistic adolescents may need to consider a wider range of stressors. Drawing on a small yet unique dataset, we conducted an exploration of experiences of trauma and PTSD symptoms and, for the first time in autistic adolescents, distinguished DSM-5 versus no-DSM-5-qualifying events, combined self- and caregiver-reports, and explored selected individual differences previously linked to autistic cognition (Rumball, 2018). Our autism group had no maltreatment history, and as trauma/PTSD were not mentioned in recruitment materials, we somewhat minimised potential inflation of probable PTSD rates. Contrasting this group with a demographically-matched control group and a maltreatment-exposed (non-autistic) group provided preliminary indications of how autism may uniquely relate to PTSD risk.
Methods
Participants
Background Variables Including Demographics and Clinical Measures, by Group
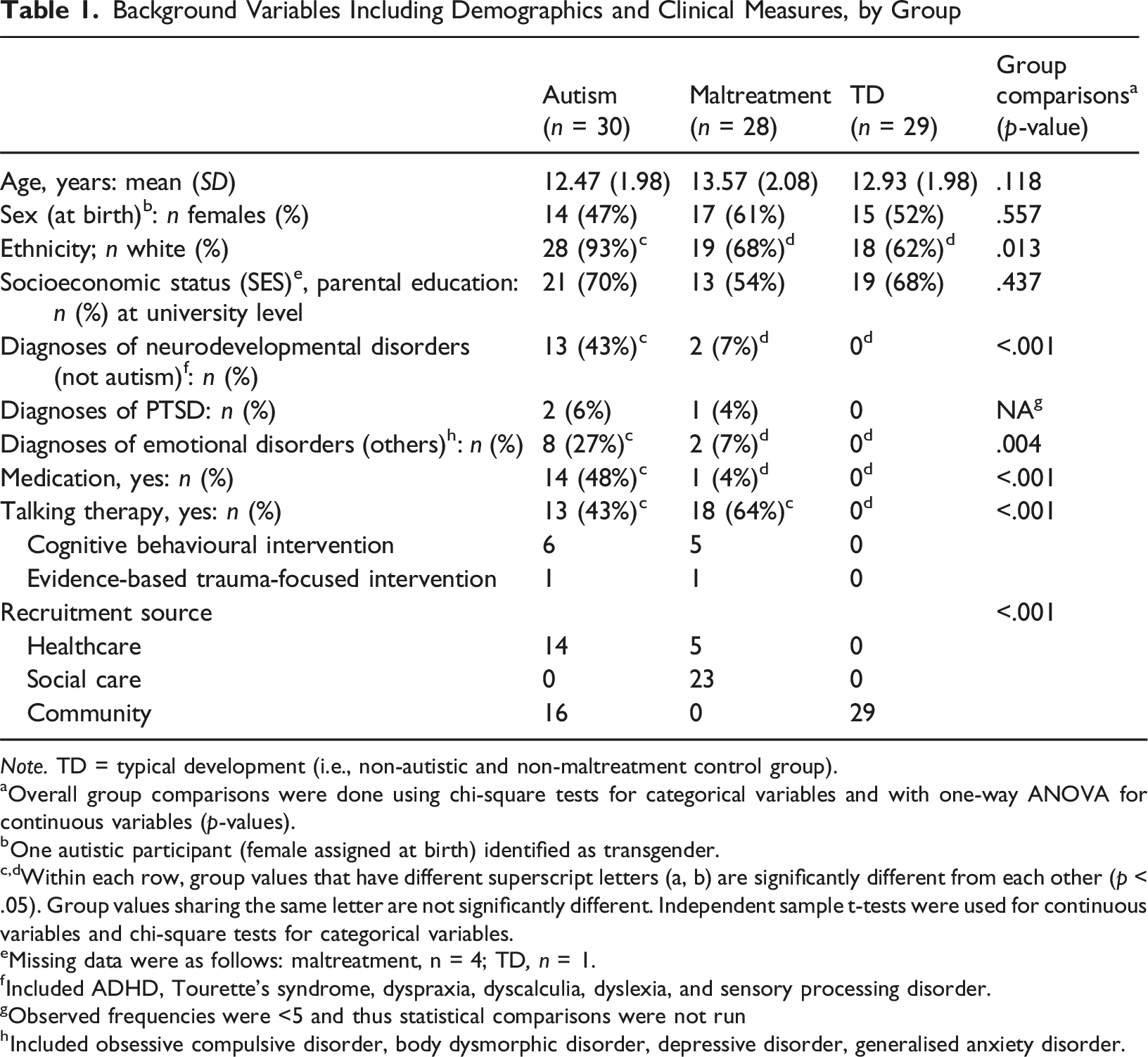
Note. TD = typical development (i.e., non-autistic and non-maltreatment control group).
aOverall group comparisons were done using chi-square tests for categorical variables and with one-way ANOVA for continuous variables (p-values).
bOne autistic participant (female assigned at birth) identified as transgender.
c,dWithin each row, group values that have different superscript letters (a, b) are significantly different from each other (p < .05). Group values sharing the same letter are not significantly different. Independent sample t-tests were used for continuous variables and chi-square tests for categorical variables.
eMissing data were as follows: maltreatment, n = 4; TD, n = 1.
fIncluded ADHD, Tourette’s syndrome, dyspraxia, dyscalculia, dyslexia, and sensory processing disorder.
gObserved frequencies were <5 and thus statistical comparisons were not run
hIncluded obsessive compulsive disorder, body dysmorphic disorder, depressive disorder, generalised anxiety disorder.
Measures
See Supplemental Materials for additional details on measures.
Trauma Exposure
The Child and Adolescent Trauma Screen – Caregiver Version (CATS; Sachser et al., 2017) has 14 items assessing potentially traumatic events based on DSM-5 criteria, including physical harm, sexual assault and natural disasters. To assess non-DSM-5 traumas, two additional questions (following Rumball et al., 2020) asked: “any other events that have happened to your child that they would consider stressful, scary, traumatic or extremely unpleasant?” and/or “… causing nightmares or memories of the event(s) to come back into their mind, when they did not want to think about them?”. Caregivers were asked to identify a specific index event before reporting PTSD symptoms in the CATS, which was also checked to see if it matched the DSM-5 criteria.
PTSD Symptomatology
The CATS (Sachser et al., 2017) provides caregiver report for 20 items measuring symptom frequency on intrusion, avoidance, negative mood/cognition, and hyperarousal, with a cut-off score for probable PTSD of ≥ 21 (Nilsson et al., 2020). A novel exploratory item on vocal/motor tics was added after consultation with caregivers of autistic adolescents. The 8-item Children’s Revised Impact of Event Scale (CRIES; Perrin et al., 2005) was selected for adolescent self-report due to its brevity to minimise completion burden. This covers symptoms of re-experiencing and avoidance, with a cut-off score for probable PTSD of ≥ 17 (Perrin et al., 2005). Symptoms in the CRIES are reported without the need for the adolescent to self-describe the index trauma.
Individual Differences
Autistic traits were measured with the Social Communication Questionnaire – Current Form (Rutter et al., 2003). Cognitive traits considered were executive functioning, using the Dysexecutive Questionnaire – Children (Emslie et al., 2003); general cognitive ability, using the abbreviated 9-item form of the Raven’s Standard Progressive Matrices Test (Bilker et al., 2012); and trait imagery vividness, using the Plymouth Sensory Imagery Questionnaire (Andrade et al., 2014).
Procedure
Adolescents and their caregivers completed separate online questionnaires. These were reviewed for suitability (ease of comprehension and perceived burden) by autistic/maltreatment-exposed adolescents and caregivers/practitioners. Recruitment materials did not mention trauma/PTSD in autism. See Supplemental Materials for additional details.
Analytical Approach
Data were checked for normality and outliers. Group differences were assessed with ANOVAs, independent-sample/Welch’s t-tests (for continuous variables), and Chi-square/Fisher’s exact tests (for categorical variables, e.g., yes vs. no experience of each traumatic event separately). Associations were assessed with Pearson’s/Spearman’s correlations (for continuous variables), and Chi-square tests (for categorical variables). Parametric tests for nonnormal data are reported when these converged with nonparametric tests, unless otherwise stated. Fisher’s Exact Tests were used to compare correlation sizes. Qualitative descriptions of traumatic events (unlinked to group membership) were double-coded (by ALZ and RRD; yes vs. no) as whether each met DSM-5 Criterion A required for a PTSD diagnosis (APA, 2013), with almost perfect agreement, Cohen’s kappa = 0.91 (Altman, 1991).
Results
Trauma Exposure
DSM-5 Traumatic Events
Relative to the TD group, both the autism and maltreatment groups reported higher incidence of physical assaults, traumatic bereavements and stressful medical procedures (p’s < .05; Figure 1). The maltreatment group additionally reported higher incidence of familial physical violence, sexual harm, or community violence (p’s < .05). The median number of DSM-5 events endorsed was 1 (IQR = 2) for autistic adolescents; 3 (IQR = 4) for maltreatment-exposed adolescents; and 0 (IQR = 0) for TD adolescents. Percentage of DSM-5 and non-DSM-5 traumatic events (within groups) reported by caregivers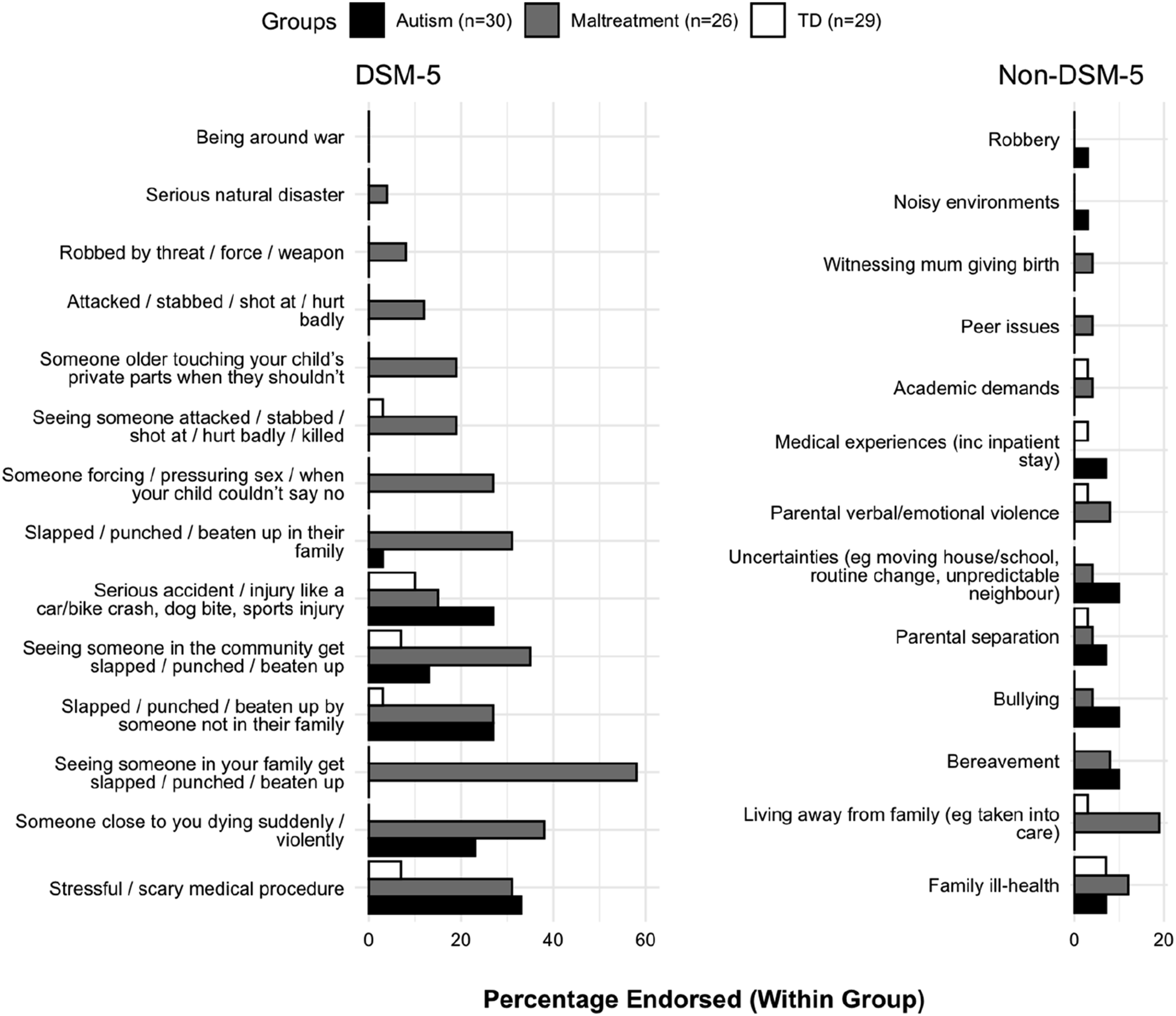
Non-DSM-5 Traumatic Events
Caregivers of 17 autistic (56.7%), 18 maltreatment-exposed (69.2%), and 8 TD (27.6%) adolescents, reported an event that the adolescents found traumatic, but which did not match DSM-5 criterion (Figure 1). The most reported events were bullying, bereavements, and events involving change/uncertainty in the autism group; and events related to out-of-home care in the maltreatment-exposed group.
Overlap in Traumatic Events
Each trauma-exposed adolescent across groups was categorised based on event types endorsed (i.e., DSM-5-only, non-DSM-5-only, or both). Autistic (n = 14/30, 46.7%) and maltreatment-exposed adolescents (n = 15/26, 57.7%) reported both DSM-5 and non-DSM-5 traumas simultaneously more frequently than TD adolescents (n = 2/29, 6.9%; p’s < .002). Autistic, maltreatment-exposed and TD groups were compared by their frequencies of reporting DSM-5-only (n’s = 2–8; 6.9–32.0%) or non-DSM-5-only events (n’s = 2–5, 7.7–17.2%) and did not differ significantly (p’s > .05).
PTSD Symptomatology
PTSD Symptoms by Caregiver and Self Report, by Group
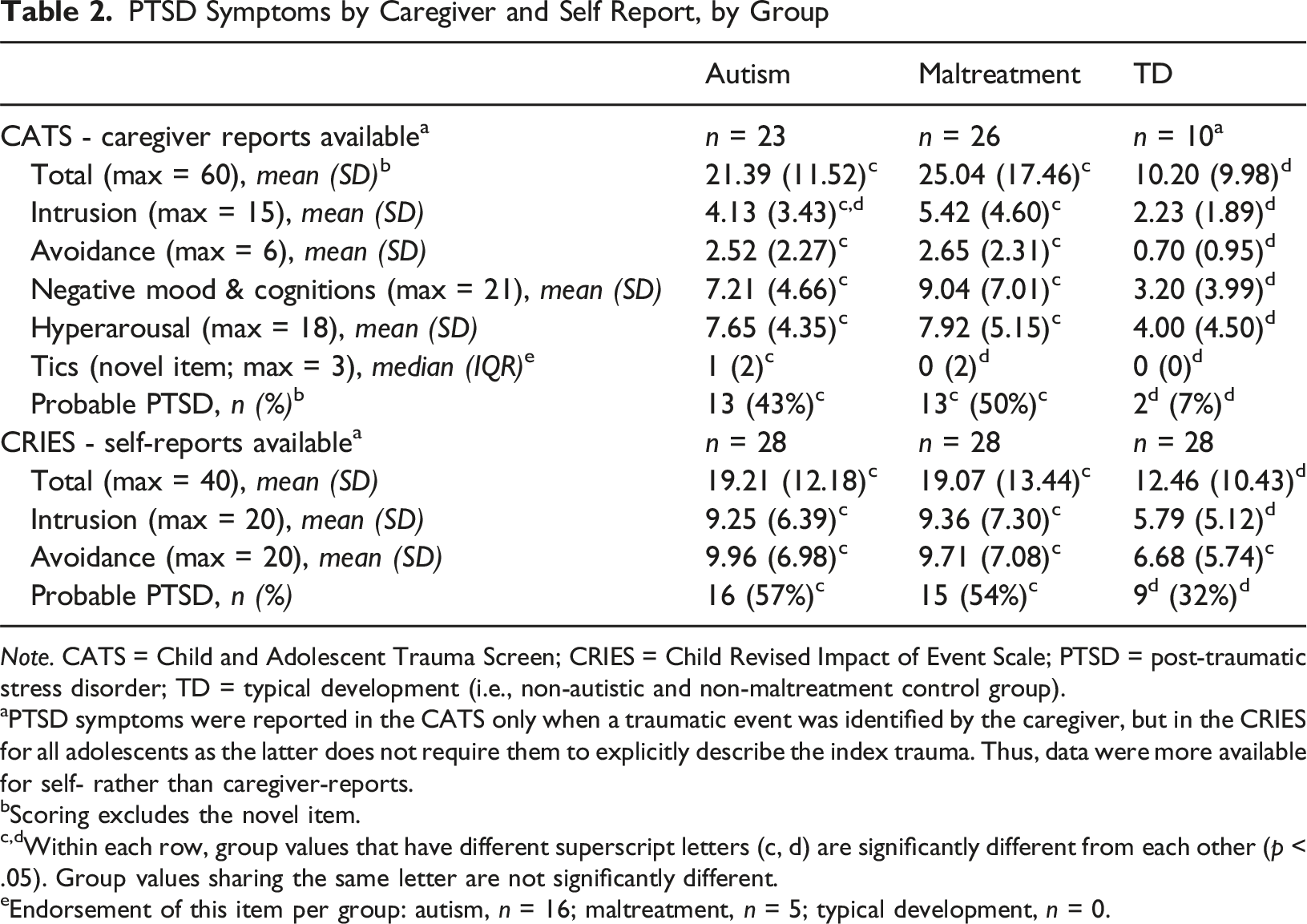
Note. CATS = Child and Adolescent Trauma Screen; CRIES = Child Revised Impact of Event Scale; PTSD = post-traumatic stress disorder; TD = typical development (i.e., non-autistic and non-maltreatment control group).
aPTSD symptoms were reported in the CATS only when a traumatic event was identified by the caregiver, but in the CRIES for all adolescents as the latter does not require them to explicitly describe the index trauma. Thus, data were more available for self- rather than caregiver-reports.
bScoring excludes the novel item.
c,dWithin each row, group values that have different superscript letters (c, d) are significantly different from each other (p < .05). Group values sharing the same letter are not significantly different.
eEndorsement of this item per group: autism, n = 16; maltreatment, n = 5; typical development, n = 0.
Reports from different respondents on overall symptom severity showed large and medium correlations in the maltreatment and autism group, respectively. The correlation between informant reports for intrusion (but not avoidance) was significantly bigger for the maltreatment-exposed than the autism group. We did not compute the corresponding correlation in the TD group because caregiver reports were insufficient (n = 10), reflecting low caregiver-reported trauma exposure in this group (see Table 2).
Autistic and maltreatment-exposed adolescents showed higher rates of probable PTSD than TD (Figure 2). Based on their caregiver’s selection of the index trauma, probable PTSD was mostly in response to non-DSM-5 events in autistic adolescents but was mostly in response to DSM-5 events in maltreatment-exposed adolescent. The association between groups and if the trauma was DSM-5 event or not was significant (p < .001). Percentage of cases endorsing trauma exposure and/or crossing cut-offs for probable PTSD, per group.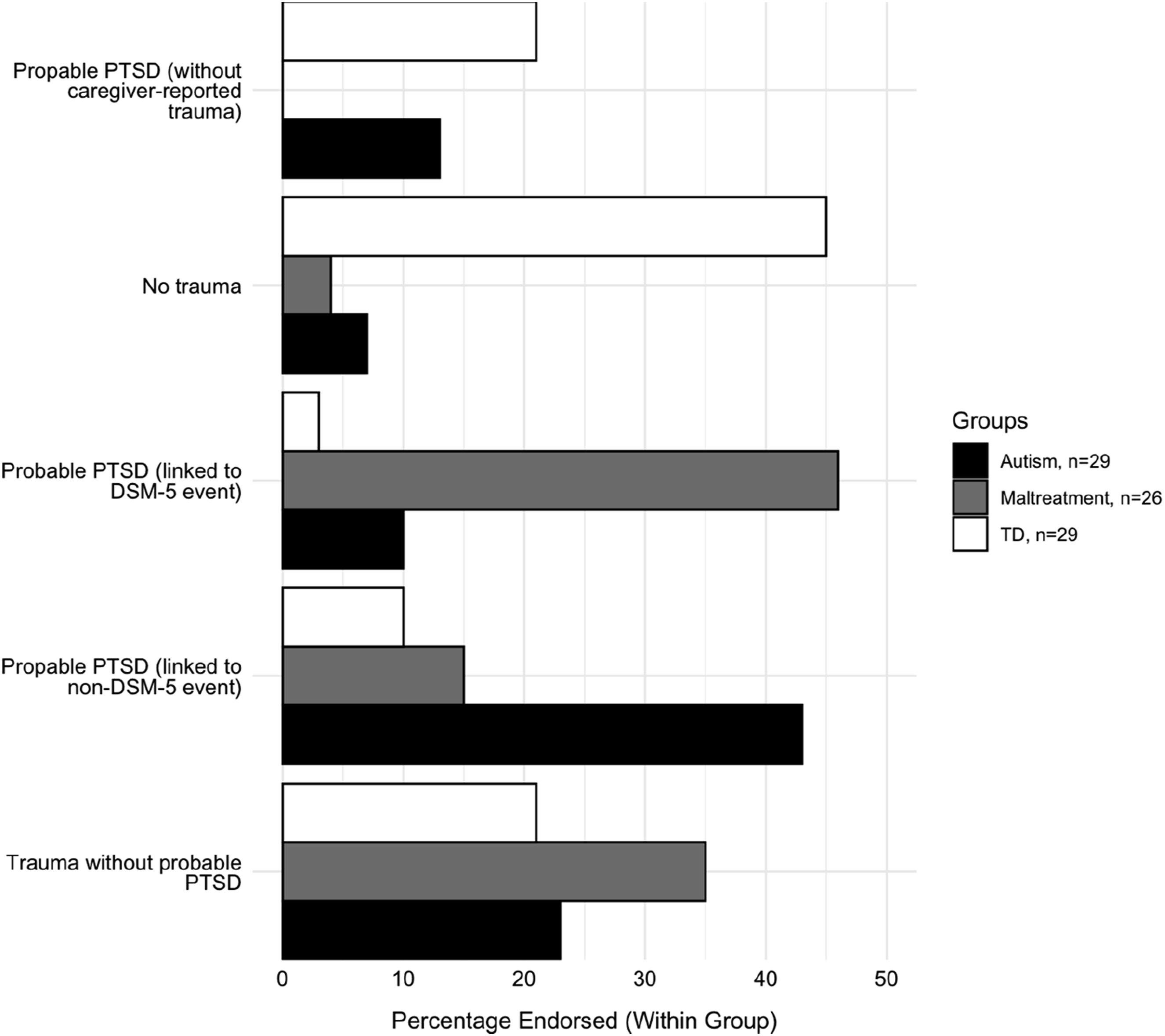
See Supplemental Materials for detailed results.
Exploring Individual Differences
Across groups, more severe PTSD symptomatology was positively and significantly correlated with executive dysfunction and female sex. These correlations were not significant when restricting to each group only, likely owing to reduced power (except for the correlation with sex in the maltreatment group). Correlations (across and within groups) were not significant between PTSD symptoms and remaining individual difference variables (i.e., autistic traits, cognitive ability, and trait imagery) and between exposure to DSM-5/non-DSM-5 traumas and sex. See Supplemental Materials for detailed results.
Discussion
We report, for the first time, preliminary high rates of PTSD symptoms in a sample of autistic adolescents in response to events not qualifying DSM-5’s Criterion A for trauma. These included bullying, bereavement, events involving change/uncertainty, and family stresses, echoing findings in autistic adults (Kerns, Lankenau, et al., 2022; Rumball et al., 2020) and qualitative data from caregivers of autistic children (Kerns, Lankenau, et al., 2022). While our sample size was modest, findings were of medium-to-large effects and relatively consistent across informants.
Our sample rate of 43–57% probable PTSD for autistic adolescents is comparable to data with autistic adults (47%; Rumball et al., 2020), but higher than in our demographically-matched TD group (7–32%), and recent estimates with autistic (14%; Quinton et al., 2024) and non-autistic youth (1.6%; Kessler et al., 2012). However, a meta-analysis with strict inclusion criteria only found 0–3.6% PTSD diagnostic rates in autistic individuals (Lai et al., 2019). Also, despite our tentative high estimates, only two autistic participants reported a formal PTSD diagnosis (Table 1). Formal diagnoses, unlike symptom measures, may underestimate the impact of trauma in autistic populations. Alternatively, questionnaire measures may be oversensitive. Accurate estimates will require sensitive and specific PTSD assessment tools in autistic adolescents (including validation of existing tools), to avoid risks of “conceptual bracket creep” and overmedicalisation (McNally, 2003). Autism-specific manifestations (beyond exacerbation of existing traits) may also need considering (Kerns & Kendall, 2012; Kerns, Robins, et al., 2022), such as stereotyped behaviours, as hinted by the present study’s novel stakeholder-developed item.
Brewin and colleagues (2019) have argued that strict definitions of trauma could hamper diagnoses – most autistic adolescents’ symptoms in our study were anchored to a caregiver-reported non-DSM-5 event rather than a traditional DSM-5 events, as in the maltreatment group (Figure 2), despite comparable symptom levels. While the definition of “trauma” remains controversial (McNally, 2003), emerging data (Kerns, Lankenau, et al., 2022; Rumball et al., 2020), alongside our clinical and empirical observations, encourage us to better attend to autistic lived experiences of “trauma”.
Autistic social communication differences may result in PTSD symptoms being missed by family and/or professionals, leading to potential under-recognition (Haruvi-Lamdan et al., 2018; Kerns et al., 2015). We also found lower concordance between self- and caregiver reports in the autistic relative to the maltreatment-exposed group, particularly on intrusion symptoms such as flashbacks/nightmares, often “invisible” to caregivers.
For individual differences, our finding of higher levels for (autistic) females is consistent with population findings (Olff, 2017). Executive dysfunction (but not autistic traits or cognitive abilities) was positively associated with more symptoms, aligning with adult data (Rumball et al., 2021). Unlike earlier suggestions (Bryant & Harvey, 1996), trait imagery ability did not seem important, but emotional aspects of imagery were not assessed (Di Simplicio et al., 2019; Iyadurai et al., 2019; Lau-Zhu et al., 2023). Potential mechanisms for (increased) PTSD symptoms in autism should be further investigated (e.g., detail-focused/sensory processing; see Hoover, 2015; Peterson et al., 2019; Rumball et al., 2021).
To better understand and assess PTSD symptoms in autistic adolescents, we may need to consider a less restrictive trauma definition (Brewin et al., 2019), multiple informants (including self-reports), and subjective experiences. Indeed, cognitive theories (Ehlers & Clark, 2000) and recent findings (Danese & Widom, 2020) highlight a subjective “sense of threat” as core to trauma. The International Statistical Classification of Diseases and Related Health Problems states that traumatic events within a PTSD diagnosis must be “extremely threatening or horrific” (ICD-11; World Health Organization, 2019), and does not impose standardised event types. As the debate of what is “trauma” in autistic people remains ongoing, a neurodevelopmentally-informed, formulation-based approach, which integrates autistic cognition and meaning-making (e.g., Stark et al., 2021), could be useful.
As evidence-based psychological interventions are acceptable and effective for autistic adolescents (Quinton et al., 2024; Rumball, 2018), these should be adapted appropriately (Peterson et al., 2019) and empirically tested in autistic individuals in relation to distress linked to non-DSM-5 traumas. Intrusive imagery symptoms may also benefit from focal approaches, such as using visuospatial tasks (Lau-Zhu & Chan, 2025; Lau-Zhu et al., 2019, 2021; Rackham & Lau-Zhu, 2021), which could harness common autistic strengths/preferences (Muth et al., 2014).
In sum, this brief report’s early findings – from a community sample during a pandemic period – add to the emerging literature suggesting that current definitions of psychological trauma may not fully capture autistic experiences (Kerns, Lankenau, et al., 2022; Rumball et al., 2020). A better understanding of autism-related processing differences and their impact of trauma will be critical. Future studies should use improved tools, more diverse and representative samples across contexts, and closely involve the autism community.
Supplemental Material
Supplemental Material - Experiences of Trauma and PTSD Symptoms in Autistic Adolescents: Preliminary Findings
Supplemental Material for Experiences of Trauma and PTSD Symptoms in Autistic Adolescents: Preliminary Findings by Alex Lau-Zhu, Alice Quinton, James Stacey, Rebecca Roberts-Davis, Myra Cooper, Carmen Chan, Francesca Happé in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgements
We would like to thank the sponsoring and supporting organisations for facilitating this work including advice on design and recruitment strategy (with key individuals highlighted): Berkshire Child and Adolescent Mental Health Services (Dr Alice Farrington); Oxfordshire County Council ATTACH (Dr Claire Holdaway); Parents Talking Asperger’s (Karen Irvani); SAFE! Support for Young Victims (Chloe Purcell); St Frideswides Primary School in Oxford (Zoe Goodin); Autism Family Support Oxford; Autistica; and MQ Charity. Finally, we are particularly grateful for participating young people and families for their time and enthusiasm for completing this study through the challenging time of a global pandemic.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alex Lau-Zhu reports support from Oxford Health NHS Foundation Trust for professional training in clinical psychology, Medical Research Council Clinician Scientist Fellowship [MR/Y009460/1], John Fell Fund from the Oxford University Press, National Institute of Health Research Biomedical Research Centre hosted at Oxford Health NHS Foundation Trust (which also funds Alice Quinton), Oxfordshire Health Service Research Committee, and Committee for Children Junior Research Fellowship at Linacre College. Francesca Happé is part-funded by the NIHR Maudsley Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. Rebecca Roberts-Davis reports support from a generous donation by Mr William Barnett CBE, facilitated by the University of Oxford Development Office.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.