
Abstract
While adolescent voice-hearing is relatively common, little is known about the experiences of their siblings. This study explored the perspectives of 14 siblings from the UK, USA, and Australia through an online qualitative survey. Using Foucauldian-informed Narrative Analysis (Parry & Varese, 2021a), an approach that accounts for how social power, discourse, and dominant cultural narratives shape lived experience, the research examined how stigmatized societal narratives around voice-hearing influenced siblings’ perspectives. Findings revealed emotional journeys involving initial shock, evolving roles, relationship strains, and limited support. Many siblings faced isolation, yet also described opportunities for growth and stronger connections through open communication. The study highlights siblings’ complex roles and underscores their need for recognition and tailored support. Recommendations include creating dedicated sibling support spaces, providing psychoeducation, and involving siblings in family interventions. Recognising and including siblings in care can enhance their wellbeing and strengthen the support system around young voice-hearers.
Plain Language Summary
Growing Up with a Sibling Who Hears Voices That Others Cannot: Sibling Stories: Hearing voices, experiencing sounds or voices that others do not hear, is relatively common during adolescence. While research often focuses on the young people who hear voices, we know very little about the experiences of their siblings. This study explored the perspectives of 14 siblings from the UK, USA, and Australia using an online survey. The research looked at how society’s negative ideas and stereotypes about hearing voices affected siblings. Many described an emotional journey, starting with shock or surprise, adjusting to new responsibilities, and sometimes feeling strains in their relationships with the sibling who hears voices. Support from others was often limited, and some siblings felt isolated. At the same time, several participants described opportunities for personal growth and closer connections within the family, particularly when communication was open and honest. The study highlights the complex roles that siblings often take on and the challenges they face. It emphasises the importance of recognising sibling experiences and providing support tailored to their needs. Suggestions from this research include creating spaces where siblings can receive guidance and support, providing education about hearing voices, and involving siblings in family-based interventions. Recognising and including siblings in care not only supports their well being but also strengthens the network of support around young people who hear voices. By listening to and supporting siblings, families and services can help everyone involved navigate the challenges and opportunities that come with hearing voices in adolescence.
Introduction
Early-onset psychosis (EOP) denotes the development of a first episode of psychosis before 18-years-old (Morrison et al., 2020). Whilst EOP is uncommon, associated symptoms, like voice-hearing, are thought to affect many more young people who do not seek help from mental health services (Maijer et al., 2019; Parry & Varese, 2021a). Meta-analyses estimate prevalence rates range from 7.5% to 35% in young people (Kelleher et al., 2012; Laurens et al., 2020; Maijer et al., 2018). Furthermore, a pilot study in the UK found that up to half of young people under child and adolescent mental health services (CAMHS) in the UK report hearing, seeing, or sensing things that others do not (Jolley et al., 2018), suggesting a potentially higher prevalence amongst those with existing mental health difficulties.
The literature uses various terms for multi-sensorial experiences, such as ‘unusual experiences’ (Jolley et al., 2018), ‘subclinical psychotic symptoms’ (Laurens et al., 2020) and ‘psychotic-like symptoms’ (Kelleher et al., 2012). Following consultation with those with lived experience, referring to these experiences as ‘unusual’ is felt to take credibility away from their common nature and hinder efforts to demystify the phenomenon. Additionally, using language like ‘psychosis’ and ‘psychotic’ may suggest a leaning to a more pathologised experience, when this is often not the case (De Loore et al., 2011). Therefore, as this research is focussed on symptoms associated with EOP at a subclinical level, associated symptoms will be referred to as ‘voice-hearing’, which encapsulates a range of experiences. For instance, hearing, sensing, and seeing things that others do not, or experiences that may be difficult to describe (Voice Collective, 2021), like felt presences, characterised by a feeling someone is present without any clear sensory content (Alderson-Day et al., 2021).
Voice-Hearing Experiences for Young People
Although commonly associated with symptoms of serious mental health problems, such as EOP, voice-hearing experiences for young people usually spontaneously resolve (Bartels-Velthuis et al., 2011). However, young people and their families can find these experiences distressing (Parry et al., 2021; Parry & Varese, 2021a, 2021b) and highly stigmatising (Bogen-Johnston et al., 2019; Colizzi et al., 2020; Rodell & Parry, 2023), which may contribute to the voices persisting (De Leede-Smith & Barkus, 2013). Therefore, more research as a phenomenon separate to psychosis among young people is appropriate and necessary. Consequently, the current study qualitatively explores experiences through the lens of non-pathologised voice-hearing to encapsulate the collective experience, separated from diagnoses of psychosis spectrum conditions. Qualitative enquiry can gather rich, reflective narratives and has shown to be successful previously within the voice-hearing community (e.g. Parry & Varese, 2021a, 2021b; Woods et al., 2015).
Importance of Family Involvement
For young people, families often play a critical role in identifying changes, obtaining support, and facilitating continued receipt of services (Haine-Schlagel & Walsh, 2015). Qualitative enquiry with adolescents indicates their perspectives surrounding their voice-hearing are influenced by family members’ responses to their experiences (Parry & Varese, 2021a). Responding to disclosures of voice-hearing in a distressed and threatening manner (often through the lens of a mental illness) leads to higher levels of distress for the voice-hearer (Peters et al., 2017; Tsang et al., 2021), whereas normalising and calm reactions tend to be associated with more favourable outcomes (Parry & Varese, 2021a). This is line with cognitive models of voice-hearing, which emphasise the central role of appraisals (the way people make sense of experiences) in determining the impact of voice-hearing (Freeman, 2016; Morrison, 2001). Therefore, family member reactions to disclosures of voice-hearing should be an area of focus.
Young people are often reliant on their family to help them interpret and formulate life experiences, including experiences of voice-hearing (Jardri et al., 2019). However, family members report providing accepting appraisals difficult if they feel disempowered, under-skilled and under-supported (Parry & Varese, 2021b). This illustrates the need to gain understanding of family members’ perspectives to improve support for families and reduce distress for them and their loved one.
Family Members’ Experiences of Supporting a Loved One Who Hears Voices
An emerging body of literature has examined the impact of supporting a family member who hears voices (Kapur et al., 2014; Parry & Varese, 2021b). Specifically, a recent narrative synthesis of 12 qualitative studies has highlighted that help-seeking experiences can have a relational and emotional impact on families, with stress adding to conflict and anxieties inhibiting hopefulness (Rodell & Parry, 2023). The stigma associated with voice-hearing can lead to concerns related to being labelled and feeling isolated from relatives, friends, and acquaintances (Hasan & Musleh, 2017; Oluwoye et al., 2020; Santos Martin et al., 2018).
Furthermore, parents of both adults (Landon et al., 2016) and children under the age of 18 (Parry & Varese, 2021b) who hear voices have stressed the need for better communication between themselves and mental health services, formal support and recognition of their important caring role. One of the few qualitative studies to explore parent and child experiences of accessing support for voice-hearing within CAMHS, indicated that many parents feel lost within the system and wished for care that was more holistic (Kapur et al., 2014). It is important to note that the majority of research into family experiences is centred on the experiences of parents, often omitting the voices of other family members who may also play important roles. This study therefore focuses specifically on the perspectives of siblings, a group whose voices are often forgotten in both research and service provision.
Siblings of Voice-Hearers
Although policy guidelines (NICE, 2013) advocate family involvement in Early Intervention in Psychosis Services (EIPS), this typically focuses on parents or main carers, often excluding siblings (Boydell et al., 2010; Sin et al., 2008). Research concerning siblings’ needs and experiences remains limited (Bowman et al., 2014), highlighting the value of qualitative enquiry to amplify this marginalised voice.
Sibling relationships hold formative importance in adolescence, offering lasting emotional and practical support (East, 2009). Such support is linked to better coping and adjustment after adversity (Oliva et al., 2009), higher self-esteem (Milevsky, 2005), reduced anxiety (Branje et al., 2004), and improved early adult mental health (Oliva et al., 2009). Given social isolation’s prevalence in voice-hearing communities (Sundermann et al., 2014) and its link to psychosis risk (Lincoln et al., 2021), sibling support may be an underused protective factor (Bowman et al., 2015). However, its role in voice-hearing contexts is under-researched (Bowman et al., 2014; Graves et al., 2022; Sin et al., 2012).
Existing studies have focussed on siblings of those diagnosed with psychosis, noting exposure to hospitalisation, violence, and self-harm (Bowman et al., 2017). Siblings report guilt (Gerace et al., 1993; Graves et al., 2020), grief for pre-psychosis relationships (Graves et al., 2022; Sin et al., 2012), stigma, fear, isolation, and care burden (Bowman et al., 2017). It is reasonable to assume voice-hearing similarly affects sibling relationships (Bowman et al., 2014; Sin et al., 2012), particularly where families lack formal support.
Moreover, age and gender may influence sibling experiences. Older siblings are often reported to adopt protective or caregiving roles (McHale et al., 2012), and sisters may be more likely to assume emotional support responsibilities within families (Awad & Voruganti, 2008). However, little research has examined whether such factors shape sibling experiences of voice-hearing, underlining the value of exploratory qualitative enquiry in this area. Exploring siblings’ lived experiences is crucial for informing interventions (Cairns et al., 2015; Sin et al., 2008) and service provision for young voice-hearers. This study aimed to extend current evidence by gathering qualitative narratives about support experiences, relational impacts, and understandings of voice-hearing.
Methods
Design and Procedure
A narrative inquiry methodology was employed, recognising the value of meaning-making through personal stories within healthcare contexts (Beuthin, 2015; Sandelowski, 1999). Narratives offer an accessible, culturally universal means of understanding experience (Barwell, 2009; Hall & Powell, 2011) and have proven effective in research involving diverse populations (Shkedi, 2004; Tsianakas et al., 2012). Qualitative online surveys have successfully engaged voice-hearing communities (Woods et al., 2015) and families supporting voice-hearers (Parry & Varese, 2021b). Accordingly, a qualitative survey was developed to gather narrative accounts.
Ethical clearance was granted by Lancaster University’s Research Ethics Committee. Given the stigma and misunderstanding surrounding voice-hearing, the survey questions were formulated through consultation with people with lived experience and professionals working with the voice-hearing community to ensure that questions were both sensitive and accessible. They were designed to be open-ended and narrative in style, encouraging participants to reflect on their journeys of understanding, meaning-making, and relational impact. The questions explored initial reactions, evolving interpretations, emotional and relational consequences, and experiences of support. This design was guided by the study’s aim to capture siblings’ perspectives in a non-pathologising way, while eliciting insights that could inform support for families.
Participants were recruited via opportunity sampling through UK peer support networks (e.g. Hearing Voices Network, Voice Collective) and social media. Specifically, study advertisements were shared on organisational platforms, including the Voice Collective X page and Hearing Voices Network (HVN) sibling support forums. Posts were also circulated through relevant professional and personal networks to broaden reach. This approach aimed to engage siblings across different contexts while ensuring accessibility.
Demographic Details of Sibling Participants
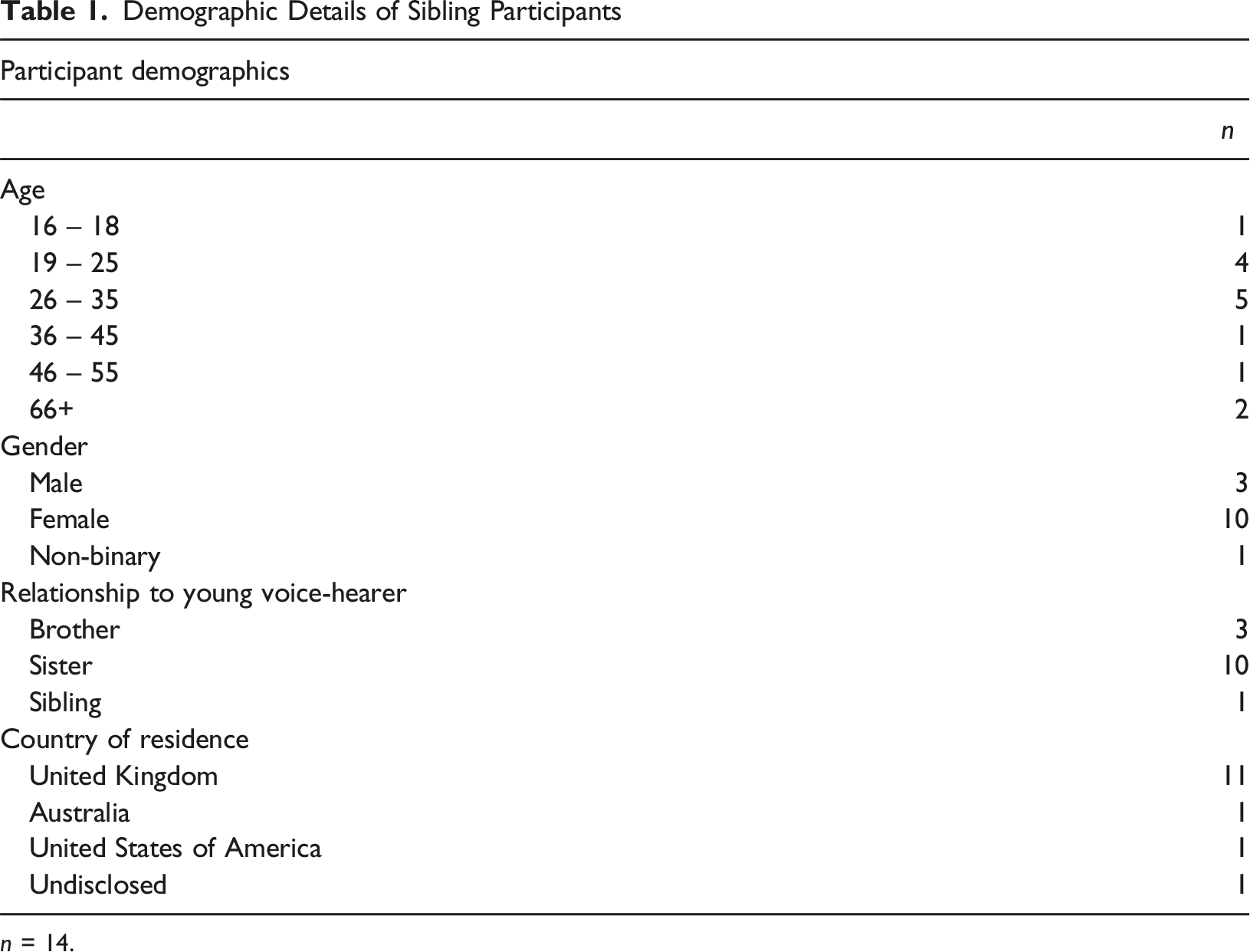
n = 14.
Participants
Fourteen participants completed the majority of the survey (10 sisters, 3 brothers, 1 unspecified gender), with an average competition rate of 85.71% of qualitative questions (ranging from 18.18% to 100%). Participants were advised that they could provide as much or as little information as they wished. Nine participants chose to provide additional thoughts, feelings, or comments at the end of the survey. Thirteen participants referred to one sibling who heard voices, while one participant noted their experience with two voice-hearing siblings. Participants provided their ethnicity in their own words. One participant self-identified as White, six as White British, one as White – Other, three as Caucasian, one as Black British, and one as Black. Participants were invited to provide a pseudonym to protect their identity, although not all chose to do so.
Analytic Approach
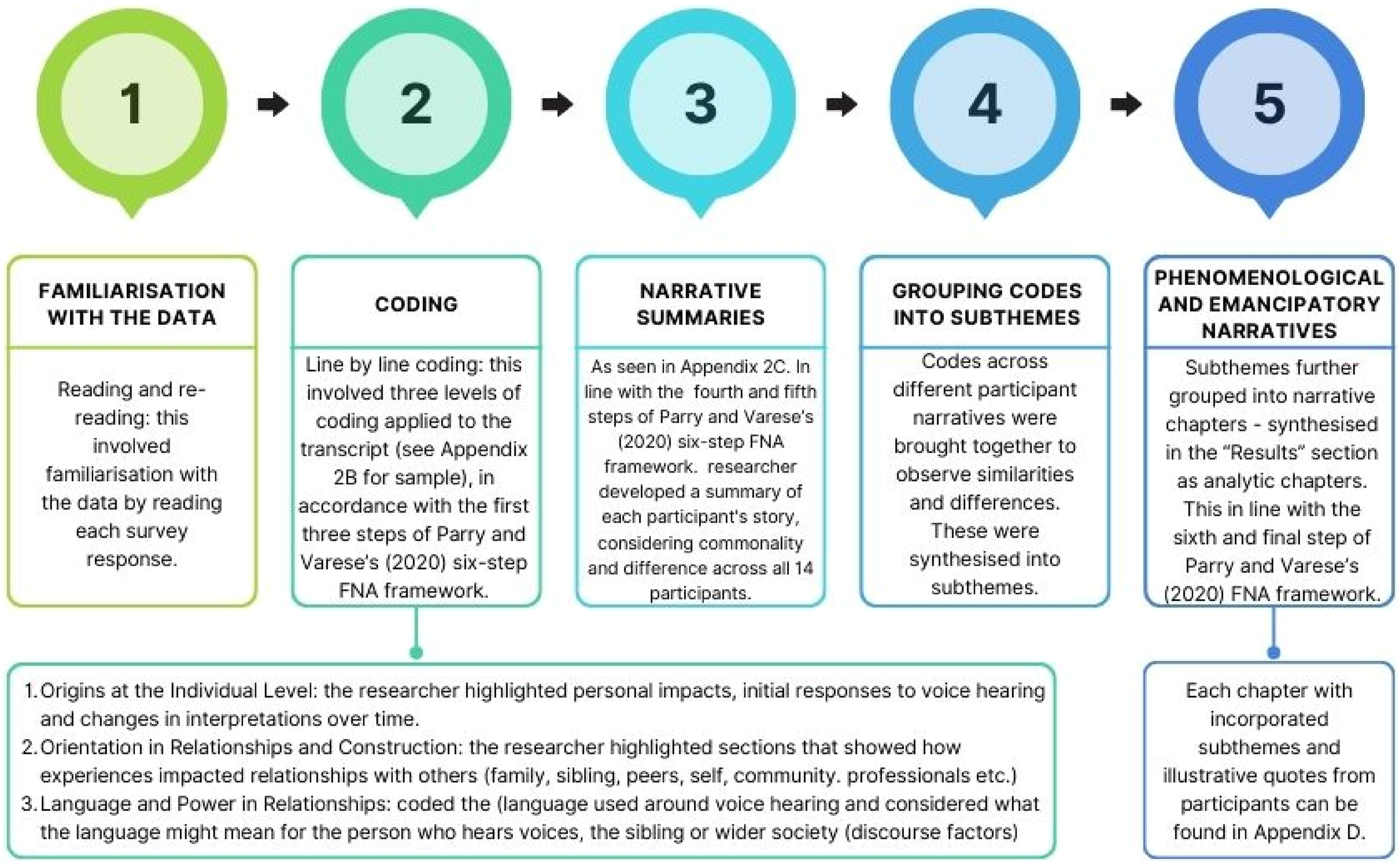
This study adopted a critical constructivist epistemology, recognising knowledge as socially constructed and shaped by systemic influences (Brydon-Miller & Coghlan, 2014). Parry and Varese’s (2021a) six-step Foucauldian-informed Narrative Analysis (FNA) framework guided the analysis, suited to examining power dynamics and sociocultural assumptions surrounding voice-hearing (Parry & Varese, 2021a, 2021b). This approach was selected because it aligns closely with the study’s aim of examining siblings’ experiences in the context of stigma and dominant cultural narratives of mental health. Unlike other narrative approaches that focus primarily on personal identity, a Foucauldian perspective emphasises how individual meaning-making is shaped by wider power relations, discourses, and societal assumptions. Given that participants frequently referred to the impact of stigma, psychiatric labelling, and cultural understandings of voice-hearing, FNA provided a suitable framework for exploring how these broader influences informed their lived experiences. Analysis progressed from individual narrative features to systemic influences. Rigour was ensured through supervision, peer review, and iterative feedback, with participant narratives reviewed against summaries and illustrated using verbatim quotes to enhance transparency and credibility.
Reflexivity
The authors have professional and research experience with voice-hearing communities and families, which informed interpretation. Reflexive practices included regular supervision, peer debriefing, and iterative review of narratives to mitigate personal bias and enhance transparency.
Results
Findings are structured into three narrative chapters. The first chapter illustrates participants’ first thoughts and reactions surrounding voice-hearing in the context of wider societal discourses, and how their understanding changed over time. The second chapter highlights shifts in roles and relationships both within and outside of the family context. The final chapter describes experiences of sourcing support for both their sibling and themselves. Together, these emancipatory chapters highlight participants’ journeys in their relationship with themselves, with others, and with voice-hearing.
These chapters are not intended to represent a strictly linear process experienced by all participants, but rather to capture key areas of meaning-making that recurred across their accounts. The structure reflects both the temporal flow evident in many stories (from first reactions, through relational changes, to seeking support) and the thematic emphases that emerged during analysis. In this way, the chapters provide an accessible narrative arc while remaining grounded in the recurring patterns across siblings’ diverse experiences.
Chapter One: First Thoughts, Feelings, and Reactions
“…I was embarrassed. There is such a stigma attached to mental illness…I think even more so when it comes to voice-hearing.” (Blossom)
Participants with close sibling relationships were often the first confidants of their sibling’s voice-hearing experiences. Rose recalled, “She [sister] told me first… I found it frightening,” while Blossom described the burden of secrecy: “I was highly disturbed – although kept to my word of keeping it a secret for her.” Others were informed via parents, typically following crises involving police or mental health services. Eve reflected, “…he went missing and the police phoned me… my mum told me he was hearing voices. I was scared, confused and sad.”
Initial emotional responses ranged from shock, fear, and confusion to disbelief. Some participants dismissed early disclosures as jokes or attention-seeking. James recalled, “…we all thought it was fun and games,” while Rose initially assumed it was “an internal monologue.” These early interpretations were often attempts to make sense of an unfamiliar experience.
Stigma played a significant role, with participants fearing associations with severe mental illness. Participant 5 recalled, “I remember googling it and all this stuff coming up about ‘schizophrenia’… I couldn’t fathom that could be happening to my sister.” Embarrassment, driven by social stigma, hindered openness: “There is such a stigma attached to mental illness… even more so with voice-hearing” (Blossom). A lack of accessible information further intensified anxieties, particularly around perceived limitations to their sibling’s potential and future safety.
The threatening nature of voices increased participants’ anxieties. Theresa described them as “very threatening and cruel,” while Eve expressed fear the voices might lead to fatal harm: “I was scared the voices would cause him to die as he was jumping out of windows.”
Participants’ meaning-making evolved over time. Some attributed the experiences to drug use (Paul) or biomedical explanations (Theresa), while others shifted towards trauma-informed perspectives. Barb reflected, “I now see it less in the medical model… I wish he had had less medical intervention.” Others identified voice-hearing as an emotional response to distress (Blossom).
Many participants expressed guilt over their initial reactions. Ruthie admitted, “I wish I was more compassionate towards him.” Several regretted not seeking information earlier, believing earlier awareness might have improved outcomes.
Despite early challenges, many described personal growth, broadening their understanding of voice-hearing and reducing stigmatised beliefs. Rose noted, “I have broadened my view… it’s much more common than people realise.” Open conversations contributed to acceptance, with Blossom reflecting, “She feels less ashamed… which in turn has helped me become more open.”
Chapter Two: Adapting to Shifts in Roles and Relationships
“It has been the centre of my family life…. like a dark cloud hanging over all my family relationships and friendships.” (Theresa)
A central theme emerging from participants’ narratives was the transformative impact of voice-hearing on the sibling relationship. Several described becoming their sibling’s closest confidant. Blossom shared, “It brought us closer together. I was the first person she confided in… I’m still the one she comes to now if she is struggling,” while Roo noted, “If anything it made us closer as I want to help and understand.” Many spoke of mutual, enduring support, with Irene reflecting, “I supported my sister in everything and still do, as she supports me.” Rose described how her siblings had “been there throughout my life… we moulded each other into the people we are now.”
A notable shift towards a more protective, often parental, role emerged, particularly among older siblings. Blossom explained, “…I went from being a sister to being this almost parent-like figure for her.” Rose described this change as difficult to undo: “She has attempted to rebalance our relationship and assert her autonomy… I will always worry more about her now.” Yet, despite their desire to protect, many participants felt powerless against the invisible nature of voice-hearing. Rose expressed, “It wasn’t like a bully or something external I could fix,” while Blossom reflected, “When the bad things can’t be seen, heard, touched physically, it puts you in a really powerless position.”
Some participants experienced negative impacts, with emotional distance arising as siblings withdrew. Eve shared, “He won’t see anyone but my mum… I miss him.” Others found communication difficult, creating a divide. Barb noted, “He isn’t able to talk fully about his experiences.” Frustration and misunderstanding sometimes led to estrangement, as Ruthie explained, “Initially we pushed each other away.” Changes in behaviour and personality contributed to a sense of loss: “I basically see my siblings as aliens now” (Paul). Grieving the relationship they once had, participants expressed sadness and longing. Eve shared, “I most of all miss him and our relationship before… I’d do anything to go back in time.”
Beyond sibling relationships, many faced challenges accessing family support. Several felt overlooked as parental attention centred on their unwell sibling. Theresa remarked, “My parents didn’t have any capacity to meet my needs.” Barb recalled, “I don’t matter as much… my parents were always very worried about my brother.” This imbalance strained relationships with parents. Some even adopted caregiving roles towards their parents. Rose reflected, “In some ways, I became their parent too,” while Eve admitted, “I have to emotionally support my mum.”
Nonetheless, positive shifts also occurred. Shared experiences sometimes drew families closer. Participant 5 noted, “I think my mum and I got closer because we had that shared experience of being really worried about [sister].” Ruthie added, “It’s brought our family unit closer together… almost like a team.”
Relational challenges extended beyond the family, affecting friendships. Blossom explained, “I put my friendships aside for a while,” while Eve felt isolated from peers, envying their ordinary sibling relationships: “I feel jealous of how my friends are rude about their siblings for petty reasons.” In summary, participants described profound changes in family roles, protective instincts, and relational dynamics, navigating both emotional challenges and opportunities for connection and growth.
Chapter Three: Navigating Sources of Support
“We are always forgotten …When our siblings are in pain, we might be shunted to the side, but it doesn't mean we aren't suffering too…” (Rose)
When reflecting on support, participants’ narratives often focused on their sibling rather than themselves, indicating a sense that their own needs were secondary. Stigma was a significant barrier to help-seeking, making many reluctant to speak about their sibling’s voice-hearing. For example, Ruthie explained, “I’m still reluctant to talk about it openly… I don’t want people thinking my brother is crazy.” Limited access to credible information reinforced stigma, with participants expressing a need for accessible, non-judgemental resources. “Even just leaflets to explain what your loved one is going through,” suggested Participant 5. Blossom advocated for open conversations to challenge stereotypes: “I want people to feel open about talking about their voices without fearing being labelled as ‘crazy’.”
Participants described difficulties accessing support services for their siblings, particularly in crises. “There were just no services to support her other than the GP” (Participant 5). Eve expressed constant anxiety, fearing harm to others or self-destruction: “I’m constantly worried everyday he’s going to kill my mum or himself.” The lack of services for younger children was also noted. Richard observed, “Support wasn’t as good in younger years.” Overall, participants hoped for timely, compassionate care for their siblings to benefit the entire family.
Interactions with healthcare services were mixed, with many reporting dismissive or unhelpful attitudes. Rose shared, “Professionals were not very interested, helpful or concerned.” Paul criticised how substance misuse issues led to further neglect: “Once you bring in drug addiction, they’re usually thrown into the ‘too hard basket’.” The dominance of a medication-heavy approach caused concern. Barb recalled, “He had a lot of heavy medication and maybe 20 ECTs… the medical side loomed large.” Paul reflected on the lasting consequences of long-term prescriptions: “My brother’s been on methadone for nearly 30 years without any weaning attempts.”
Siblings often felt excluded from services and vital information, exacerbating anxiety and confusion. As Blossom explained, “I felt very alone, like I was coping with all of these thoughts and feelings by myself.” For some, this led to desperate online searches, as Participant 5 described: “You can snowball into this Google thread of awful things…” They explained that without professional reassurance, online information often felt overwhelming and stigmatising. Further, a lack of involvement in care decisions felt “bewildering and painful” (Barb), leading participants to call for holistic, family-inclusive care.
Within families, information was frequently withheld in attempts to protect siblings, leaving many confused. Participant 5 recalled, “My mum would say ‘she’s just stressed’… I think it made me more confused.” Participants longed for open communication and felt their wellbeing was compromised by exclusion.
Many spoke of the deep emotional and identity impact of their sibling’s experiences. Blossom noted, “My sense of self is centred on my sister — sister, carer, protector, not just ‘me.’” Theresa described her brother’s voice-hearing as “the defining feature” of her life, attributing personal struggles to this. Despite these challenges, most faced them alone. Blossom admitted, “I felt very alone, like I was coping with these thoughts by myself.” Participants described feeling overlooked by both families and services. Rose summed up, “We are always forgotten… it doesn’t mean we aren’t suffering too.” Most welcomed the idea of dedicated sibling support, valuing a safe, separate space to share experiences without guilt or risking their sibling’s care.
Discussion
This study sought to explore the reflective experiences of individuals with a voice-hearing sibling, offering insight into a largely overlooked area of mental health research. Participants shared complex emotional reactions to their sibling’s voice-hearing, including shame, secrecy, and fear - feelings shaped by cultural stigma and a broader societal discomfort surrounding mental illness. The findings echo wider literature documenting the relational and emotional toll of voice-hearing within families, underscoring how stigma and judgement profoundly shape family narratives and coping strategies.
A key theme emerging from participants’ accounts was the significant emotional burden they carried, often marked by feelings of hopelessness, guilt, and anxiety about their sibling’s wellbeing. Participants described a sense of powerlessness in supporting their sibling, feeling ill-equipped and excluded from meaningful involvement in care decisions. These findings complement research involving parents of young voice-hearers, which similarly highlights the emotional cost of caregiving within families (Parry & Varese, 2021b). Importantly, this study confirms that these impacts are not confined to parents and that siblings, too, experience elevated distress within these family systems (Figures 1 and 2). Six-step foucauldian-informed narrative analysis framework Transparent process of analysis in the current study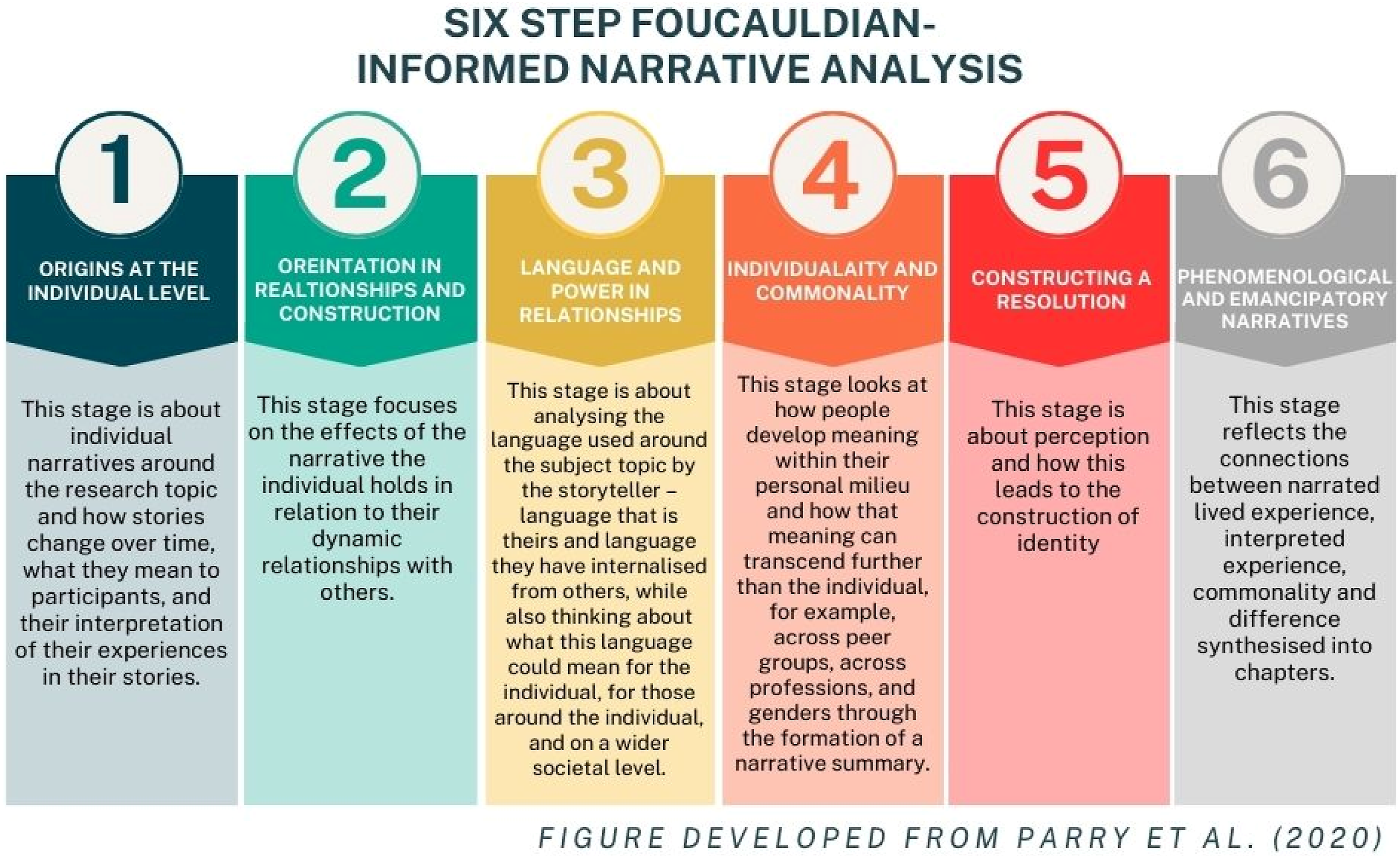
Participants reflected on how their understandings of voice-hearing evolved over time. Initially, most leaned towards biological and illness-based explanations, likely perceived as more concrete and socially sanctioned. However, through seeking information and connecting with their sibling’s lived experience, their perspectives often shifted towards more psychological and compassionate understandings. This process of sense-making is important, as family appraisals can influence how voice-hearing is experienced and managed. Research suggests that family reactions to disclosures of voice-hearing can either reduce or exacerbate distress (Parry & Varese, 2021a), making access to credible, recovery-oriented information essential. By highlighting how siblings’ perspectives evolved, this study extends recovery-oriented work, which emphasises personal meaning-making and moving beyond strictly medical models (Wiesepape et al., 2023). Recovery-oriented interventions recognise that fostering hopeful and non-stigmatising narratives can reduce distress and improve outcomes (Thongsalab et al., 2023). By demonstrating how siblings developed more hopeful and compassionate understandings of voice-hearing, this study highlights their potential role in supporting recovery through reframing experiences and providing validation.
The findings also illustrated the shifting relational roles siblings assume — often becoming caregivers, protectors, and advocates, sometimes at the expense of their own identity and wellbeing. Fractures in family relationships, increased strain with parents, and feelings of being ‘forgotten’ were common. While these themes have been identified in sibling experiences of psychosis (Graves et al., 2020), this study suggests similar dynamics occur when voice-hearing is present without formal diagnosis, highlighting the need for support irrespective of clinical status.
Notably, alongside these challenges, some participants reported relational gains and personal growth. For some, adversity strengthened sibling bonds and encouraged open conversations about mental health. This reflects findings that supportive sibling relationships in adolescence are linked to long-term emotional wellbeing (Hollifield & Conger, 2015). Personal growth, including greater empathy and reduced stigma, appeared to buffer some of the negative emotional impacts, aligning with models of post-traumatic growth, which propose that individuals can experience psychological growth following adversity through meaning-making and relational connection.
Yet, despite these gains, participants described pervasive feelings of isolation and exclusion, both from services and, at times, within their families. Many felt their needs were secondary to their sibling’s and reported minimal opportunities to process their experiences. This sense of invisibility is echoed in broader mental health research, where siblings often report being overlooked in care planning and support provision (Graves et al., 2022). Participants highlighted the importance of recognition for their emotional labour and advocated for holistic, family-inclusive approaches in mental health services.
A recurring concern was the stigma attached to voice-hearing, which contributed to initial fear and secrecy. Participants noted that societal narratives labelling voice-hearing as ‘madness’ shaped their reactions and prevented open conversations. Research indicates that stigma significantly impacts the help-seeking behaviours and social experiences of individuals who hear voices (Rammou et al., 2023a; Volpato et al., 2022). Interventions focused on psychoeducation and public health campaigns have shown promise in reducing stigma around voice-hearing (Rammou et al., 2023b; Reddyhough et al., 2021) and could be extended to include sibling-targeted resources, offering developmentally appropriate and hopeful messages about voice-hearing in young people.
Clinically, this study highlights several areas for service improvement. Participants valued the idea of having a dedicated space to explore their experiences independently, without fear of betraying their sibling’s confidence. They expressed a need for sibling-specific psychoeducation on voice-hearing, the emotional toll of caregiving, and coping strategies. Furthermore, involving siblings in care discussions, particularly where they play a substantial support role, may improve outcomes for the whole family unit.
Current evidence supports family-based interventions for psychosis, but siblings are frequently absent from these models (Sin, 2013). Given that young people with mental health difficulties may choose to confide in siblings over parents (Parry & Varese, 2021a), services could benefit from incorporating siblings into therapeutic conversations where appropriate. Peer-support groups were also suggested as a valuable way for siblings to reduce isolation and validate their experiences, echoing evidence from sibling support initiatives in psychosis care (Feriante et al., 2022).
A key limitation of the study was the inability to follow up for elaboration due to the online narrative method. While this allowed access to a marginalised group, richer data might have been obtained through interviews. Additionally, the sample lacked diversity, with most participants identifying as white and living in Western contexts. Cultural factors strongly influence experiences of mental health stigma and family roles; therefore, further research is needed in more diverse populations.
Conclusion
This study offers novel insight into the nuanced, emotionally complex experiences of siblings of young voice-hearers, highlighting the importance of their inclusion in mental health care discussions and interventions. Siblings’ accounts identified significant barriers, such as stigma, lack of accessible information, and exclusion from services. Rather than viewing these only as obstacles, these challenges point to opportunities for change. For example, stigma and secrecy highlight the need for accessible psychoeducation tailored specifically for siblings, which could reduce anxiety and promote understanding. Reports of being excluded from services indicate the value of creating dedicated sibling support spaces and involving siblings more consistently in family-based interventions. Similarly, the lack of clear information suggests opportunities for services to provide developmentally appropriate, non-pathologising resources that normalise voice-hearing and reduce fear.
By addressing these areas, mental health services can reframe barriers as catalysts for improvement, facilitating recognition of siblings’ needs, strengthening family resilience, and ultimately improving outcomes for young people who hear voices.
Supplemental Material
Supplemental Material - Exploring Experiences of People With Siblings Who Hear Voices During Adolescence: A Narrative Study
Supplemental Material for Exploring Experiences of People With Siblings Who Hear Voices During Adolescence: A Narrative Study by Sadie Rodell and Sarah Parry in Clinical Child Psychology and Psychiatry.
Footnotes
Acknowledgements
The authors would like to thank all the participants who generously shared their experiences for this study. We also acknowledge the support of colleagues who provided valuable feedback during the manuscript preparation. No third-party writing or editing assistance was received for this manuscript.
Ethical Considerations
This study was approved by Lancaster University’s Research Ethics Committee. All procedures were conducted in accordance with the ethical standards of the committee and with the 1964 Helsinki Declaration and its later amendments.
Consent to Participate
Informed consent was obtained electronically from all participants prior to participation. Participation was voluntary and confidential.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors, but the first author received funding for clinical psychology training through Health Education England and this study was completed during that contract.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to confidentiality agreements with participants but are available from the corresponding author on reasonable request.
Identifying Information
To preserve anonymity, no identifying information related to the authors, institutions, funders, or approval committees has been disclosed in this manuscript.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.