
Abstract
Young people often rely on family carers to access support for their mental health. However, stigma can be a barrier to help seeking for young people and families. Little research has been undertaken with young people who experience highly stigmatised symptoms, such as psychosis spectrum symptoms, and even less research has been conducted with parents and carers, meaning barriers to help go unchallenged. Therefore, this narrative review aimed to explore stories of family experiences of seeking help for young people with symptoms associated with the psychosis spectrum. Sources searched were PsycINFO and PubMed. Reference lists of the selected papers were also cross-checked to ensure the search had not missed potential papers for inclusion. Searches returned 139 results, of which 12 were identified for inclusion. A narrative analytic approach was adopted to synthesise qualitative findings to provide a nuanced interpretation of help-seeking experiences. The narrative synthesis provided an opportunity to identify differences, similarities, and patterns across the studies to tell a cumulative emancipatory narrative of family experiences of seeking help for psychosis spectrum symptoms. Help-seeking experiences had a relational impact on families, with stress adding to conflict and anxieties inhibiting hopefulness, although families could emerge stronger and assertively with compassionate support.
Introduction
Early-onset psychosis (EOP) denotes the development of a first episode of psychosis before 18-years-old (Morrison et al., 2020). EOP can be a frightening, disabling experience. Symptoms include ‘positive symptoms’, such as hallucinations and delusions, and ‘negative symptoms’ including emotional apathy, self-neglect, and social withdrawal (National Collaborating Centre for Mental Health, 2013). Whilst EOP is rare, associated sensory experiences, such as visual and auditory hallucinations, are relatively common in childhood and do not usually indicate EOP (Maijer et al., 2019; Parry & Varese, 2021a, 2021b; van Os & Linscott, 2012). However, stigma surrounding psychosis and associated symptoms can lead to increased symptom-related distress for young people and their families (Colizzi et al., 2020), at which point they often seek mental health support (Parry & Varese, 2021a, 2021b).
Many terms are used to refer to multi-sensorial experiences within the literature, such as unusual experiences (Jolley et al., 2018), subclinical psychotic symptoms (Laurens et al., 2020) and psychotic-like symptoms (Kelleher et al., 2012). In most cases, these experiences are transient. However, approximately 20% of individuals experience adverse effects, including distress and functional-impairment (Van Os & Reininghaus, (2016); Jolley et al., 2018). Therefore, for the purpose of this review, symptoms associated with EOP at a subclinical level will be referred to as unusual sensory experiences (USEs).
Although most children with USEs or young people considered at clinically high risk of psychosis will never require a psychosis diagnosis (De Loore et al., 2011; Poulton et al., 2000), there are many experiential parallels in terms of symptoms, symptom-related distress, and challenges when seeking mental health support. Consequently, the current review explores help-seeking through the lens of psychosis-spectrum symptoms to encapsulate the collective experience, separated from diagnoses of psychosis spectrum conditions.
Sourcing Tailored Support
Currently, recommended treatment pathways for psychosis are largely based upon adult-focused research. Without suitable adaptations for age and developmental stage, these approaches may not be appropriate or transferable across younger age groups (Parry & Varese, 2021a, 2021b; Stain et al., 2016). Furthermore, pathways from CAMHS to early intervention for psychosis services are often problematic, due to a lack of psychosis specific expertise within CAMHS and limited developmental expertise in psychosis services (Jolley et al., 2018). This highlights a need for more research focussed on improving the understanding of help-seeking amongst under 18 s to improve tailored models of support (Gin et al., 2021).
Family Involvement
For young people, parents often play critical roles in identifying changes in wellbeing, obtaining support, and facilitating continued receipt of services (Haine-Schlagel & Walsh, 2015). Family support is particularly relevant for EOP as onset of symptoms generally occurs whilst living in the family home (Jansen et al., 2015). Qualitative enquiry with 13-18-year-olds indicates reliance on family to help interpret experiences (Parry & Varese, 2021a, 2021b), highlighting the importance of family engagement with services. As family members play a key role, understanding their experiences is crucial when aiming to refine help-seeking processes (Cairns et al., 2015). However, little research has considered familial recommendations for improving service delivery thus far (Kapur et al., 2014; Parry & Varese, 2021a, 2021b).
Recent narratives suggest family reactions to disclosures surrounding voice-hearing can impact the content and nature of the voices themselves (Parry & Varese, 2021a, 2021b), which may contribute to distress and strains in parent-child relationships (Romelli & Pozzi, 2016). While the importance of caregivers providing acceptance has been emphasised (Escher et al., 2002), family members report this being difficult if they feel disempowered, under-skilled and under-supported (Parry & Varese, 2021a, 2021b), further illustrating the need to gain understanding of family members’ perspectives in order to reduce distress for young people and their families. Caregivers are at increased risk of economic, emotional, and psychological difficulties (Kuipers et al., 2010; Onwumere et al., 2015). Despite this, family members’ own needs are often neglected in research and services (Claxton et al., 2017; Lavis et al., 2015).
Reviewing lived experiences is essential to shape interventions aimed at meeting unmet needs of families (Sin et al., 2005; Cairns et al., 2015), while also informing service delivery strategies to support children experiencing EOP and USEs. Findings from individual qualitative studies provide rich insight into lived experiences of this under-researched area, which can be further enriched through analytic synthesis of those original narratives (Sandelowski et al., 1997). Therefore, a narrative review and synthesis was conducted to explore stories of family experiences of seeking help for a young person with psychosis-spectrum symptoms and experiences to explore barriers, facilitators and turning points in their journey.
Method
Eligibility Criteria
Characteristics of Reviewed Studies.
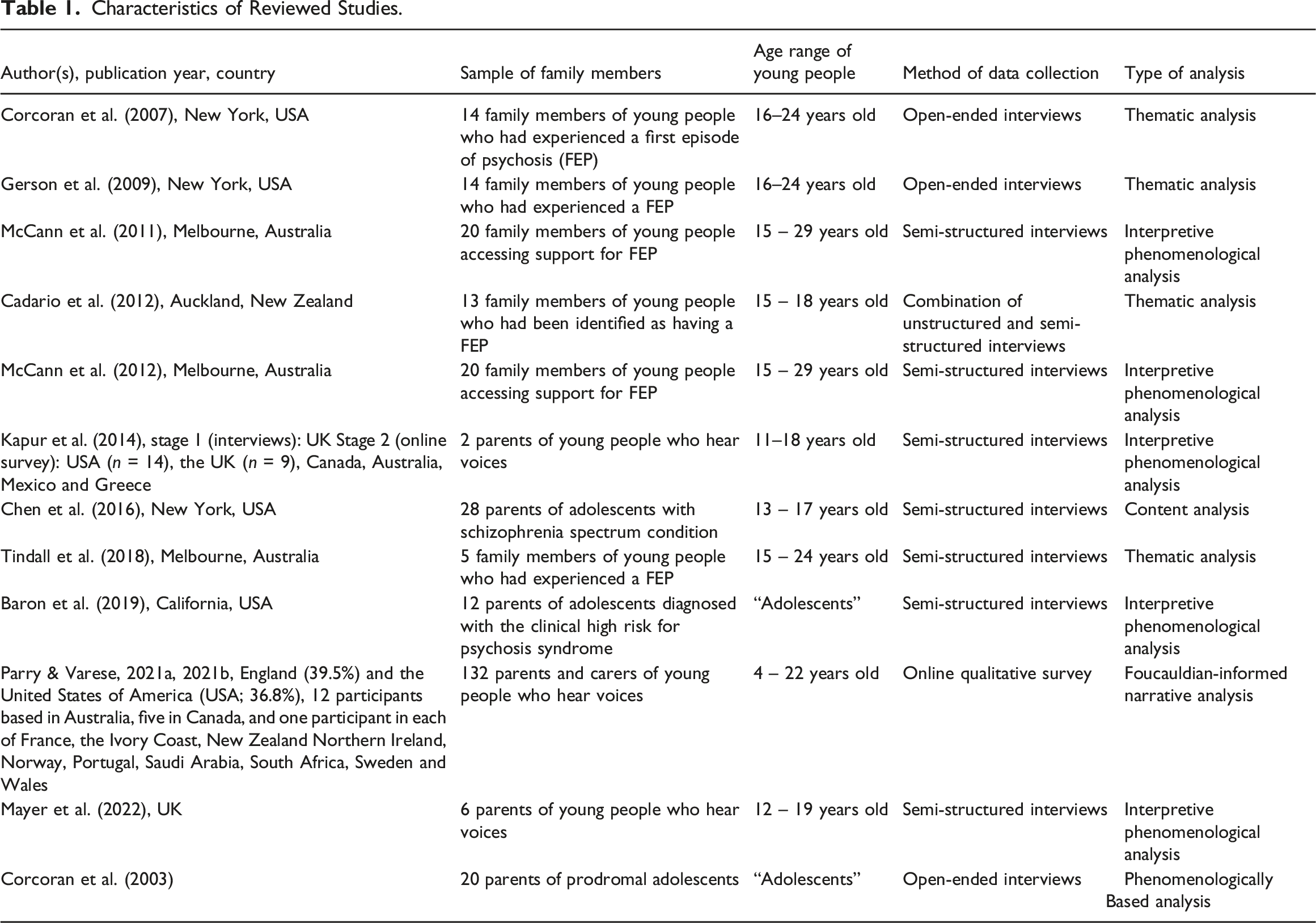
Information Sources
Sources searched were PsycINFO and PubMed. Reference lists of the selected papers were also cross-checked to ensure the search had not missed potential papers for inclusion.
Search Strategy
The search period was November 2021 to February 2022. The first set of terms were: “child”, “young person” or “adolescent” and “psychosis”, “psychotic symptoms”, “schizophrenia”, “paranoia”, “delusions”, “hallucinations”, “positive symptoms”, “negative symptoms”, “voice hearing” or “distressing sensory experience”. This second set of terms were: “family”, “relative”, “sibling”, “mother”, “father”, “parent” or “caregiver” and “help seek*“, “treatment”, or “services”. Terms were chosen with the aim of capturing as many family members’ experiences of supporting a young person with EOP and USEs as possible. This search returned 139 results. Titles and abstracts were screened for eligibility for inclusion and 11 papers were identified for inclusion. Upon advice, we then ran an additional search to check for relevant papers that used the terminology ‘clinical high risk’. One further paper was identified through this search.
Analytic Approach to Qualitative Synthesis
A narrative approach was adopted to synthesise qualitative findings to provide a nuanced interpretation of lived experiences. Texts were reviewed narratively to ‘tell a story’ informed by the stories of original participants. A narrative synthesis provided an opportunity to identify differences, similarities, and patterns within the studies (Lisy & Porritt, 2016). The findings of each text were read for relevant data, which was then coded for themes and narrative pathways. These pathways were then synthesised to form a reconstructed narrative across three distinct emancipated and interconnected layers.
Narrative Synthesis
The synthesis identified three emancipatory narrative layers, which are individually distinct, although the layers should be viewed as a cumulative account of how families decide whether to access support and their experiences, rather than viewing each in isolation (Figure 1). Narrative layers of family experiences in supporting a loved one with early-onset psychosis and distressing sensory experiences.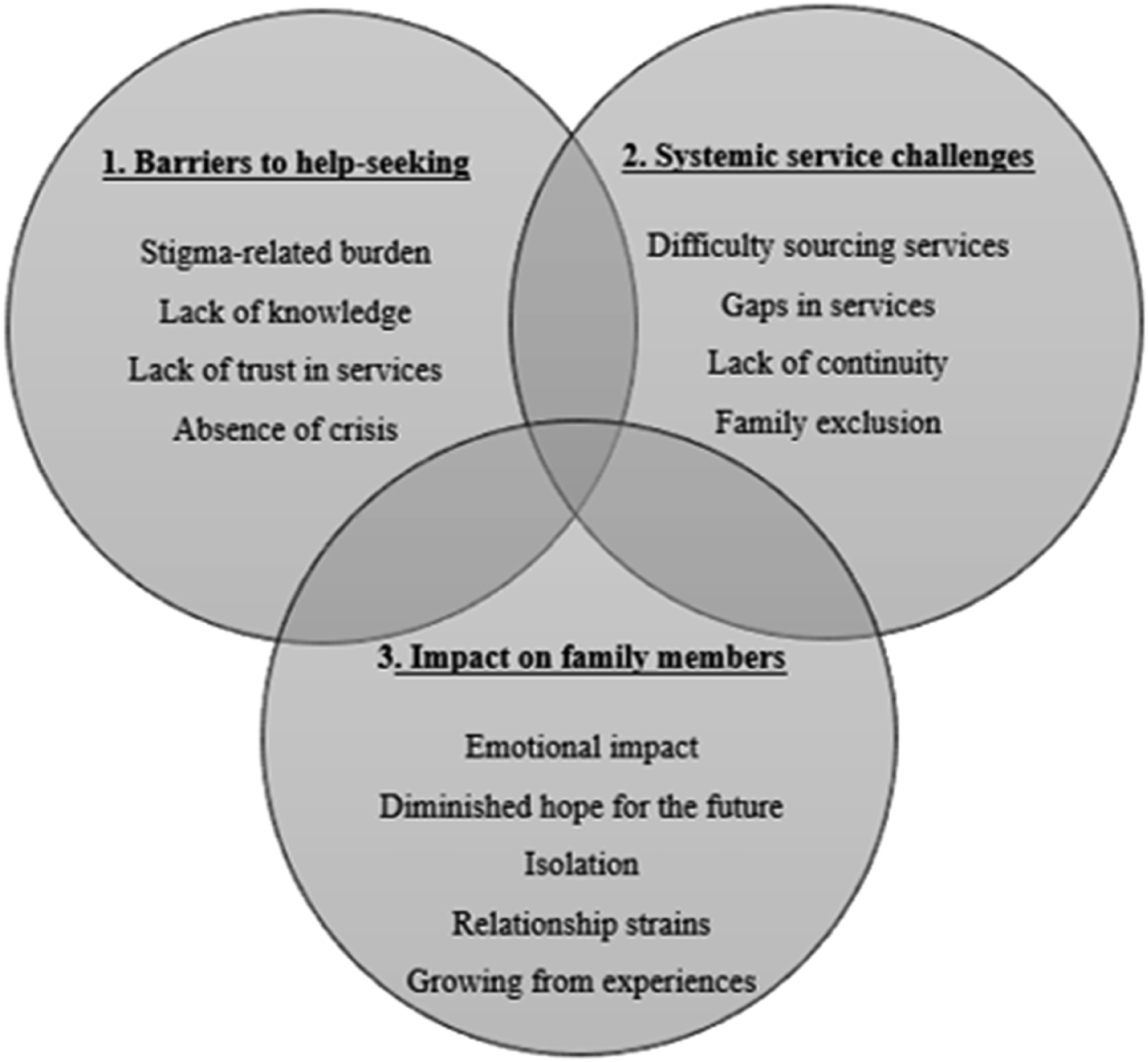
Narrative Layer One: Help-Seeking Barriers
“I always thought mental illness was something you didn’t talk about because there was so much shame” (Baron et al., 2019, p.763, p.763)
Stigma-Related Burden
Stigma was implicitly and explicitly mentioned across all papers reviewed. Several accounts attributed stigma as an overarching barrier to help-seeking attempts (McCann et al., 2011; Baron et al., 2019). In three studies, family members spoke of how their own stigmatised attitudes toward psychosis acted as initial barriers to help-seeking. Stigma associated feelings included shame, fear, and embarrassment (McCann et al., 2011; Baron et al., 2019; Mayer et al., 2022). These feeling fuelled fear of judgement from others, including extended family members, friends, and neighbours (McCann et al., 2011; Kapur et al., 2014; Mayer et al., 2022). Caregivers recalled a fear of being blamed for something going “wrong”, which acted as a deterrent from seeking informal support from those closest to them (McCann et al., 2011, p.549). Feelings of shame held by the young person themselves were also discussed: “I think he was embarrassed” (Baron et al., 2019, p.763). Stigma was echoed in narratives suggesting their loved one was hostile toward their efforts to seek help on their behalf (Corcoran et al., 2007), with self-stigma acting as a further barrier to accessing timely care.
Limited Knowledge of Psychosis Spectrum Symptoms
A sense of ‘not knowing’ surrounding psychosis and USEs was frequently highlighted: “I didn’t know anything about it” (Cadario et al., 2012, p.91). Factors associated with the cause of psychosis and USEs included age and stage of development (Corcoran et al., 2003, 2007; Cadario et al., 2012), stress (Parry & Varese, 2021a, 2021b; Mayer et al., 2022) and substance use (Corcoran et al., 2007; Mayer et al., 2022). These attributions often led to delays in seeking help due to dual stigmas associated with parenting and circumstances. Furthermore, limited mental health literacy contributed to uncertainty surrounding how and where to access support, delaying help-seeking further (Cadario et al., 2012; Chen et al., 2016).
Lack of Trust in Services
One study highlighted family members who actively avoided medical and mental health services for fear of the outcome: “GPs will not be very informed, will not refer you to the right services” (Parry & Varese, 2021a, 2021b, p.213). While another found that negative past experiences of inpatient mental health services contributed to lasting distrust and reluctance to seek help from similar services on subsequent occasions (Gerson et al., 2009).
Absence of Crisis
Five out of the 12 studies reviewed discussed the reaching of a ‘crisis point’ as a catalyst to seeking support from mental health services (Corcoran et al., 2007; Gerson et al., 2009; Cadario et al., 2012; Chen et al., 2016; Tindall et al., 2018). This crisis point tended to result from an escalation in symptoms, which caused families to feel overwhelmed: “My putting him in the hospital was my cry for help too” (Gerson et al., 2009, p.813). Reaching a crisis point appeared to provoke dramatic increases in help-seeking, seemingly helping families overcome barriers to help-seeking, such as stigma: “When she made a suicide attempt…it was like she just has to get help…I didn’t care about labels” (Chen et al., 2016, p.125). Therefore, the absence of crisis may act as a barrier to help-seeking. Formal mental-health support may be considered earlier by families if psychosis and USEs were less stigmatised, and if the importance of early intervention for symptom management were better understood (Corcoran et al., 2007).
Narrative Layer Two: Systemic Service Challenges
“adequate supports are not there” (Parry & Varese, 2021a, 2021b, p.213, p.213)
Difficulty Sourcing Services
Sourcing support involved multiple agencies and significant wait times (Cadario et al., 2012). Family experiences of UK CAMHS echoed this frustration: “CAMHS is a long wait and hard to get through to” (Parry & Varese, 2021a, 2021b, p.214). However, upon finding services, family members often experienced relief, characterised by expressing strong emotions: “I just burst into tears” (McCann et al., 2012, p.227). In cases where engagement involved involuntary admission to hospital, family members experienced this relief as “traumatic yet necessary” (Gerson et al., 2009, p.813). Interestingly, exhaustion and grief did lead to seeking help from family and religious sources in one study (Corcoran et al., 2003).
Gaps in Services
A significant gap in services was observed for young people: “zero services are available for someone experiencing voices so young” (Parry & Varese, 2021a, 2021b, p.213). Age-related difficulties surrounding diagnoses and accurate medication prescription were also reported (Chen et al., 2016). Being unable to access targeted support raised concerns surrounding whether care received was age-appropriate: “no way he should ever have been in a place like that when he was 16…but they had nowhere else to put him” (Cadario et al., 2012, p.90). Narratives from parents in one paper suggested their teenage child was treated as an adult: “I think [clinicians] just assume that because they’re [accessing services] they’re adults and they’re old enough to deal with their own things” (McCann et al., 2012, p.228). For individuals living in the UK, where specialist support is not typically available for USEs until age 14, obtaining appropriate support was especially difficult, contributing to a narrative of frustration and injustice: “…support is almost non-existent and I just can’t understand how that’s OK” (Parry & Varese, 2021a, 2021b, p.213). An overwhelming desire for services to be tailored to younger children was detected throughout four of the 12 papers reviewed (McCann et al., 2011, 2012; Cadario et al., 2012; Parry & Varese, 2021a, 2021b).
Lack of Continuity
A lack of continuity in services was voiced in five studies (Cadario et al., 2012; Kapur et al., 2014; Chen et al., 2016; Tindall et al., 2018; Parry & Varese, 2021a, 2021b): “We kept on getting sick of telling our same story to different people” (Cadario et al., 2012, p.100). This lack of continuity was also highlighted between services and suggested limited knowledge of psychosis spectrum symptoms and USEs amongst primary medical services: “[GP] wasn’t very helpful. She kind of just was like ‘Right. I don’t know how to handle you’” (Tindall et al., 2018, p.180). Themes of limited continuity were especially prominent following discharge from inpatient services, with family members reporting unclear arrangements and information (Kapur et al., 2014). This resulted in family members feeling under-supported, “very alone, and having to fend for themselves” (Chen et al., 2016, p.126).
Family Exclusion
Within family narratives, feeling excluded from provisions of care was expressed in seven studies (Corcoran et al., 2003; Corcoran et al., 2007; Gerson et al., 2009; McCan et al., 2012; Kapur et al., 2014; Tindall et al., 2018; Parry & Varese, 2021a, 2021b): “I feel like I’m being left out” (Kapur et al., 2014, p.7). Although the importance of confidentiality was recognised, frustration was expressed nonetheless: “There’s issues of patient confidentiality…but then there’s the issue of parents out there, who have no clue as to what is happening with their child” (Gerson et al., 2009, p.814). This concern raised conflict, as they often regarded themselves as ultimately responsible for the young person’s wellbeing (McCann et al., 2012). In turn, family members described how their wellbeing could be compromised by feeling excluded, suggesting their important contribution as carers was often dismissed: “I don’t want to just be the taxi” (Tindall et al., 2018, p.182). When asked for recommendations for improving services, family members wished to feel empowered and involved throughout treatment (Parry & Varese, 2021a, 2021b).
Themes of disjointedness were also observed once services were accessed, characterised by an absence of age-appropriate support, feeling excluded from provisions of care, and a lack of continuity between each stage of signposting and receiving support. Families described feelings of dissatisfaction with support available and heightened impact upon family wellbeing.
Narrative layer Three: Impact on Family Members
“Stress, anxiety and trauma can occur in parents going through this experience so it’s vital there’s more… support” (p.214; Parry & Varese, 2021a, 2021b)
Emotional Impact
Upon early detection of change, experiences of feeling helpless and scared were raised: “It was really scary…there was nothing anyone could do” (Cadario et al., 2012, p.97). In one paper, while most family members were alarmed by specific symptoms, generally, the nature rather than the presence of USEs caused the greatest distress (Parry & Varese, 2021a, 2021b). In another, many family members’ accounts highlighted feelings of failure and guilt as they retrospectively reflected upon early signs they may have missed: “when you look back, it all added up” (Cadario et al., 2012, p.86). One source of anxiety amongst family members was caused by a lack of confidence and self-belief to help their loved one (Gerson et al., 2009), indicating feelings of disempowerment. A strong emotional impact on family members was reported across all of the reviewed literature.
Diminished Hope for the Future
One paper highlighted concerns about what a diagnosis meant in terms of prognosis and recovery: “I probably felt sorry for myself, thinking…what are we gonna do?” (Tindall et al., 2018, p.181), whereas another emphasised a strong sense of anger: “Now we have to deal with this ‘s' word [schizophrenia]… and I am angry” (Gerson et al., 2009, p.814). Even after accessing support from services, continued concern for their loved one and future prospects was prominent (Cadario et al., 2012), with lacking reliable information exacerbating these worries (Parry & Varese, 2021a, 2021b). There also seemed to be a tension between wanting to be hopeful, but describing ‘guarded hope’, for example “I want to be optimistic but I feel maybe she can only be helped so much and then this will happen again. I fear she will backslide. My only hope is that she will be happy and enjoy life” (Corcoran et al., 2003, p.329).
Isolation
There were mixed accounts surrounding whether sharing their loved one’s difficulties with a wider circle was beneficial; participant accounts from two papers suggested it allowed for social buffers to be built against stigma, reducing isolation (McCann et al., 2011; Chen et al., 2016), whereas others felt sharing with those who had stigmatised pre-conceptions could lead to further social exclusion (McCann et al., 2011), again highlighting the protruding impact of stigma. Families sought to find commonality, explaining the usefulness of gaining experiential knowledge from those with similar experiences (Cadario et al., 2012; Baron et al., 2019; Parry & Varese, 2021a, 2021b). Despite this, one paper indicated some families simultaneously disclosed a reluctance to access parent groups due to logistical challenges and not wanting to be “put on the same level” as others perceived as being in worse situations (Baron et al., 2019, p.764). While family members rarely voiced feeling isolated explicitly, isolation ran through their stories (Mayer et al., 2022).
Relationships Strains
Themes of close relational strains were raised across five papers (Corcoran et al., 2007; Gerson et al., 2009; Kapur et al., 2014; Parry & Varese, 2021a, 2021b; Mayer et al., 2022): “we argued behind closed doors about how we should react” (Parry & Varese, 2021a, 2021b; p.214). Mothers in particular voiced struggling to access support within the family system (Parry & Varese, 2021a, 2021b), some in one paper describing their partners as “emotionally absent” (Mayer et al., 2022, p.10). Very few discussed sibling involvement, however those that did, indicated strains on sibling relationships (Parry & Varese, 2021a, 2021b). Parent-child relationships were also impacted; parents described wanting to keep their child close (Mayer et al., 2022). However, escalation of symptoms frequently created a physical and emotional distance as primary care was handed over to specialist services, leaving a sense of loss: “one woman prayed to understand why her son had become like a stranger” (Corcoran et al., 2007, p.312). Family members wished for more holistic care from services to support with these difficulties (Corcoran et al., 2003; Kapur et al., 2014).
Growing from Experiences
Despite a large proportion of narratives suggesting a negative impact, in three papers, narratives indicated some alleviation of these impacts by feeling they had “grown from their experiences” through challenging their own negative pre-conceptions (Cadario et al., 2012; McCann et al., 2012; Mayer et al., 2022, p.11). Suggestions that their own personal involvement demystified the phenomenon and led to acceptance were prevalent: “it can happen to anyone” (Cadario et al., 2012, p.91). Others reported growth of self-confidence through developing an assertive approach to help-seeking, which provided hope for accessing future support (McCann et al., 2012).
Discussion
This review aimed to explore family members’ lived experiences of seeking help for young people experiencing symptoms associated with the psychosis spectrum, including USEs; whose voices have occupied little space in the literature to date. Retelling original stories through narrative synthesis provided an additional degree of nuance, interpretation and perspective to the understanding of help-seeking for this population (Lisy & Porritt, 2016), identifying similarities and differences across the groups (Figure 2). Illustration of similarities and differences of help-seeking experiences between young people with USEs, and those with EOP or at CHR.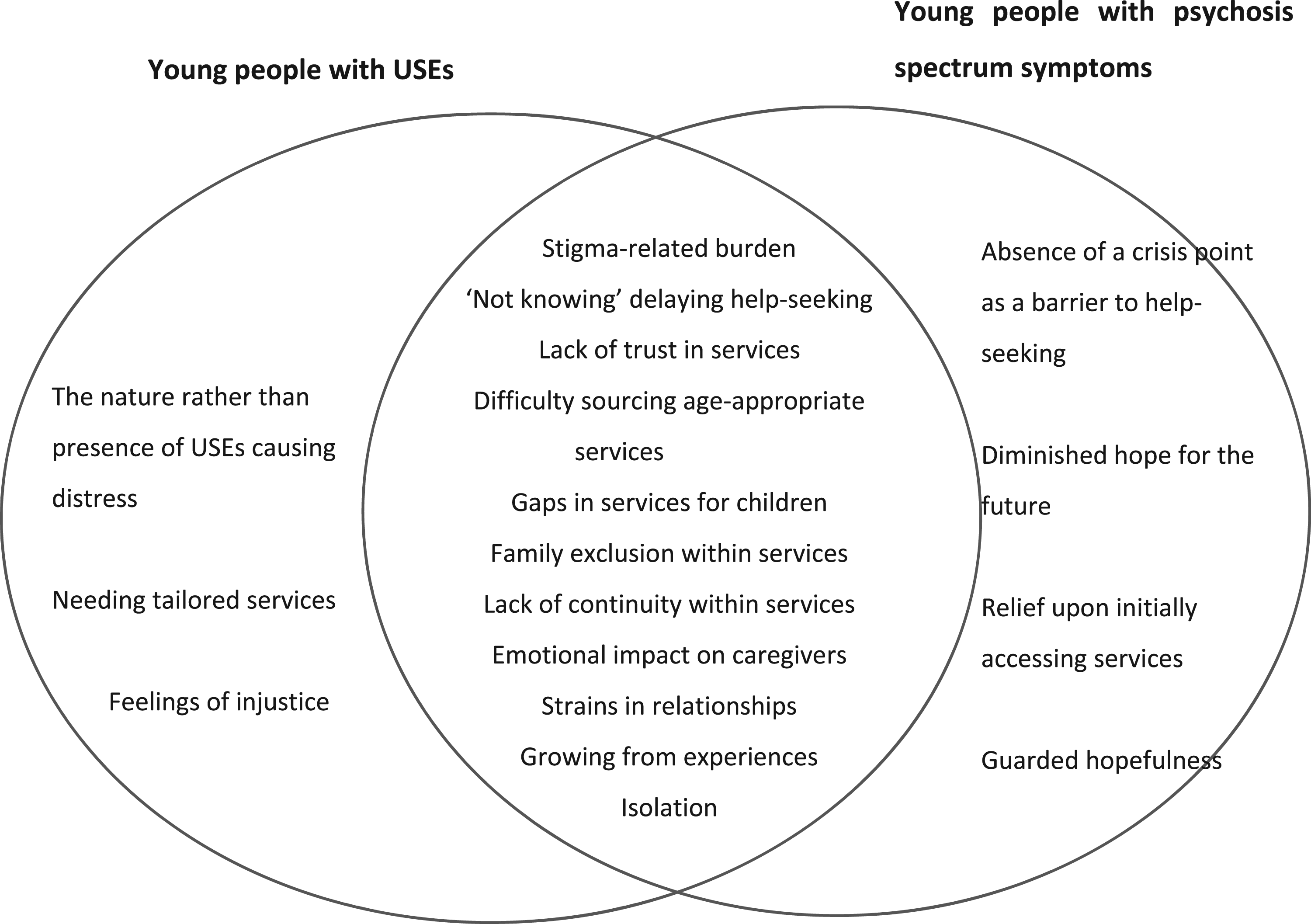
Help-Seeking Barriers
Initial barriers to seeking help included fearing stigma-related judgement, a lack of knowledge surrounding psychosis and USEs and limited trust in services. Additionally, like reviews exploring help-seeking processes amongst more adult populations (Cairns et al., 2015), this review found that help often was not sought until the young person was in crisis, with absence of crisis acting as a barrier. Waiting until this point to seek help may result in first interactions with services requiring hospitalisation (Gerson et al., 2009), often described as frightening for patients and their families (Fenton et al., 2014), leading to increased distrust of mental health services, which was identified as a further barrier to accessing support. This finding is a powerful reminder of the need for early intervention. Avoiding help-seeking until reaching crisis may also be due to misattribution of behaviours to typical adolescent behaviour, stress or drugs (Corcoran et al., 2007; Gerson et al., 2009; Cadario et al., 2012). This misattribution may also partly result from a reluctance to engage with stigma related to psychosis (Gerson et al., 2009; Baron et al., 2019).
Systemic Service Challenges
While support offered by services tended to be met with relief, several systemic service challenges were observed, including a lack of child focussed information and gaps in services for younger children aligning with previous literature reviews (Kapur et al., 2014). This mirrors research suggesting poorer outcomes for younger referrals within services (Haddock et al., 2006; Tiffin & Welsh, 2013), highlighting need for more evaluations of interventions targeting symptoms associated with the psychosis spectrum and USEs with children and adolescents (Gin et al., 2021). Evaluating these experiences is important, as early ruptures in therapeutic relationships may negatively impact likelihood of continued engagement or future help-seeking (Stewart, 2013; Tindall et al., 2018).
Impact on Family Members
This review found significant relational and emotional impacts, which had consequences for self-belief and future hopes. Shame, desperation, and isolation are common features of USE accounts (Woods, 2017) and this review on help-seeking amongst families provided no exception. However further to this, possibly later in the help-seeking process, was a sense of acceptance and personal growth.
Clinical Implications
Prolonged duration of untreated psychosis is associated with increased symptom severity and poor social functioning (Penttilä et al., 2014; Drake et al., 2020). As stigma is a barrier to help-seeking, continued public education surrounding demystifying USEs and EOP is essential, including reducing stigmatised portrayals in the media (Delahunt-Smoleniec & Smith-Merry, 2020). Sourcing formal mental health support as a last resort may be less likely if more accurate depictions of psychosis spectrum conditions and USEs were conveyed, which would enhance understanding and reduce internalisation of stigma (Corcoran et al., 2007; Joa et al., 2008).
There is a need to develop services that engage families in an empowering and collaborative way. As family members play a key role in sourcing and facilitating support (Jansen et al., 2015), their views should be included in commissioning discussions surrounding CAMHS. The more emotional burden family members are facing, the more stressful family life is likely to be for the young person (Zanetti et al., 2018). Therefore, interventions need to extend beyond the young person to their families, enhancing resilience and helping them provide optimal care (Parry & Varese, 2021a, 2021b).
Limitations and Future Research
Due to a lack of consistency across studies regarding the age-range of young people, the findings are limited in generalisability. Some studies employed a sample of family members whose loved one was under 18-years-old alongside accounts of those supporting young adults (Corcoran et al., 2007; Gerson et al., 2009; Tindall et al., 2018; Parry & Varese, 2021a, 2021b). Additionally, there was a lack of continuity surrounding diagnoses used and how psychosis and USEs amongst this age group were defined, highlighting need for greater clarity of the similarities and differences between symptoms associated with the psychosis spectrum and USEs for children and young people. The limited impact of research into USEs and psychosis with children and adolescents to date may result from inconsistent definitions and populations (Maijer et al., 2018). For example, as EOP is defined as the development of a first episode of psychosis before 18-years-old (Morrison et al., 2020), more research is required exclusively involving families of young people within this age-bracket to explore the unique features of the experience, and how early intervention could support longer-term health. Further, studies were largely conducted in the Global North, so are unlikely to be relevant across cultures. It would be helpful to learn from a more global perspective as to how the organisational structure of formal and informal mental health services could better support young people and their families. However, the review offers novel insights into the barriers and facilitators experienced by families when trying to access support for children with symptoms associated with psychosis and highlights where further research is needed, which could prove valuable to the future development of early intervention studies to improve research clarity and long-term outcomes for young people and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by indirectly by Health Education England as part fulfilment of the Doctorate in Clinical Psychology