
Abstract
Background
Parents can be slow to recognise that an adolescent needs help from a mental health professional, yet the factors affecting their help-seeking intentions are not well understood. The aim of this study was to test the application of the Common-Sense Model (CSM) of Illness Representations to parents’ perception of adolescent distress and intentions to seek help.
Method
The study employed an experimental design using video vignettes. Parents (N = 1,176; female N = 993) of adolescents (10–19 years) were asked to self-report key demographic information, an illness perceptions questionnaire, and a measure of stigma.
Results
Results demonstrated that the CSM model explained 38% of the variance in help-seeking intentions. Parents were more likely to report intentions to seek help if they believed that treatment could control the adolescent’s problem (OR = 1.39), or if they believed the problem would have negative consequences (OR = 1.41). Parents who believed the problem was in the control of the adolescent, had lower help-seeking intentions (OR = .87).
Conclusion
The CSM provides a useful model of help-seeking intentions to guide parental education. Perceiving treatment as controlling distress or that distress would have negative consequences for an adolescent, were key predictors of parental help-seeking intentions.
Plain Language Summary
The majority of lifetime mental health problems first emerge during adolescence. Getting professional help promptly reduces the chances that problems will become more serious. Unfortunately research evidence indicates that adolescents typically do not seek help for themselves, thus increasing their vulnerability. Parents have a key role as gatekeepers to professional help for adolescents who are below the legal age to seek help themselves and as observers of changes in behaviour or thinking that may signal an emerging mental health problem. Our study set out to understand the circumstances which influence parents to recommend help-seeking for an adolescent who is distressed. Over 1000 parents of adolescents took part in an online experiment in which they were randomly assigned to view a video in which a ‘parent’ described either a moderate or a serious mental health difficulty being experienced by their son or daughter. In half of the videos a possible reason was given for the adolescent’s difficulty and in the other half there was no reason given. Parent participants were asked for their opinions on the difficulties described and whether the ‘parent’ in the video should seek help. The results indicated that participants were more likely to recommend help-seeking if they believed that treatment would help to control the problem and if they thought the problem would have negative consequences. Participants were less likely to recommend help-seeking if they thought that the problem was within the control of the adolescent. The findings indicate that parents of adolescents might best be encouraged to seek help for an adolescent with a mental health difficulty if they are provided with information to the effect that: (i) mental health difficulties may not be within the control of an adolescent; (ii) getting help will reduce the difficulties that the young person is experiencing; and (iii) there are potential long term negative consequences of not getting help.
Keywords
Introduction
Adolescence is a period in the lifespan where physical health is at its best, and it is the lowest point of mortality (Patton et al., 2016). However, the opposite can be said for mental health, and it is when the majority of mental health difficulties 1 have their onset (McGorry et al., 2007). Research indicates that 50% of mental disorders emerge prior to the age of 15, and 75% by the age of 25 (Killackey et al., 2020). What is most concerning is adolescents’ underutilisation of formal services, often referred to as the “service gap” (Islam et al., 2022; Raviv et al., 2009). Adolescents do not, and in some countries cannot (McNary, 2014), seek professional help for a mental health difficulty on their own and as a result are reliant on their parents to support and direct them to services. Parents’ knowledge and beliefs about the causes of an adolescent mental health difficulty can influence their ability to recognise distress in their adolescent and, in turn, shape how they approach treatment pathways (Honey et al., 2015). Parents themselves can find it challenging to recognise that an adolescent is in distress and needs help (Wahlin & Deane, 2012). Very often the symptoms of mental distress could be interpreted as normative adolescent turmoil and it can be challenging for parents to distinguish when support may be needed (Logan & King, 2001; Reardon et al., 2017; Stuckey et al., 2021).
A number of models to explain parental help-seeking have been proposed in the literature (Costello et al., 1998; Godoy et al., 2014; Logan & King, 2001), however, these models have been contested for a variety of reasons. In particular, critics have argued that parental help-seeking is not a straightforward process as these models appear to suggest. Instead, parents may access multiple services at different time-points to get appropriate help for their child (Shanley et al., 2008). However, one stage in the help-seeking process that is consistently identified and that all agree is essential to initiating parental help-seeking is parents’ ability to recognise that the adolescent needs help (Fröjd et al., 2007; Hassett et al., 2018; Sayal, 2006). However, little is known about how their initial perception of the problem, predicts their likelihood of seeking help (Reardon et al., 2017).
The Common Sense Model (CSM) is a conceptually strong and widely used model in the health psychology literature to explain the process by which an individual perceives, understands and responds to a complex health threat (Dempster et al., 2015). The model proposes that when faced with such a threat an individual develops beliefs known as “illness representations” or “illness perceptions” about their condition which drives their coping and emotional response. These “illness perceptions” are formed from past experience (with the symptoms/illness), knowledge, current experience with symptoms and cultural values (Shanley & Reid, 2015). Based on these emotional and cognitive representations the individual decides on an action plan to manage their symptoms (Leventhal et al., 2016). The model has five core cognitive components (Hagger & Orbell, 2003) including cause, timeline, control (treatment and personal), identity and consequence and was adapted by Moss-Morris et al. (2002) to incorporate two emotional components: illness coherence and emotional representation. An advantage of the model is that it incorporates the emotional reaction alongside the objective rational response, thus providing a more complete understanding of an individual’s response to a health threat (Harvey & Lawson, 2009).
The CSM has been applied extensively with physical illnesses and is a significant predictor of coping behaviours such as treatment seeking, adherence to treatments, psychological well-being and social functioning (Dempster et al., 2015; Hagger and Orbell., 2003; Petrie et al., 2008). Researchers have been advocating for the application of CSM to mental health difficulties in order to interpret individuals’ understanding and management of their symptoms (Petrie et al., 2008). To date, CSM has been successfully applied to understanding how mental health difficulties are perceived by those close to the individual including family/carers, and in turn how this influences how they cope with their family member’s mental health difficulty (Baines & Wittkowski, 2013). The model has also been demonstrated to predict help-seeking intentions in adults with depressive symptoms (McLaren et al., 2023). To date the model has not been applied to understand how parents’ perceptions of an adolescent mental health difficulty predict help-seeking intentions.
Despite the absence of a model, a number of factors are known to be associated with parents’ help-seeking attitudes and illness perceptions. Problem severity is one of the strongest influences on parental help-seeking behaviours (Logan & King, 2001). Parents are also quicker to seek help for externalising problems in comparison to internalising problems (Sayal, 2006). Cohen et al. (1991) found that for conduct disorders and oppositional defiant disorders, parents were likely to seek help from a mental health professional. However, for emotional problems and for ADHD, parents sought help from mental health professionals alongside non-professional sources such as teachers and the clergy. Unsurprisingly, if parents have previous experiences accessing mental health care for their child they are more likely to seek help again in the future (Logan & King, 2001).
Research has also demonstrated that parent and adolescent gender may influence parents’ willingness to seek professional help. For example, evidence suggests that mothers may be more willing than fathers to seek help for a child or teenager with a mental health difficulty (Kusaka et al., 2024), a finding which may be explained by gender differences in perceptions of the severity (Raviv et al., 2009) and aetiology of the problem (Kusaka et al., 2024; Raviv et al., 2009). Therefore, any analysis exploring parent help-seeking should explore the role of the parent’s gender.
Stigma has consistently been shown to be a significant barrier to seeking help for both young people and their parents (Mukolo et al., 2010). Parents who have higher levels of stigma are more likely to respond to an adolescent with depression with criticism and are less supportive (Johnco et al., 2018); stigma can also be a barrier to problem recognition (Villatorio et al., 2018). Therefore, stigma is another important variable to consider when evaluating parental help-seeking.
Present Study
To date there is no widely accepted theory or model to explain how parents’ perceptions of an adolescent mental health difficulty predicts help-seeking and this is a potential barrier to developing targeted interventions. The CSM is a suitable model to apply for several reasons. It is the only social cognitive theory that addresses the emotional alongside the cognitive aspect of illness representations. The CSM has been widely used and applied to understand beliefs about physical illness and how this is related to illness behaviours and there is emerging evidence that it is a useful model to apply in the mental health context and with parents (Lobban et al., 2005). The aim of the present study is to apply the CSM to explain parental help-seeking intentions. To address this, the present study employed an experimental design using video vignettes with the following aims: (1) To test the structure of the illness perception model in relation to parents’ intentions to seek help for adolescents with mental health problems. (2) To determine whether parents’ illness perceptions (treatment control, personal control, illness coherence, emotional representation, consequence, timeline acute/cyclical) predict help-seeking intentions.
Method
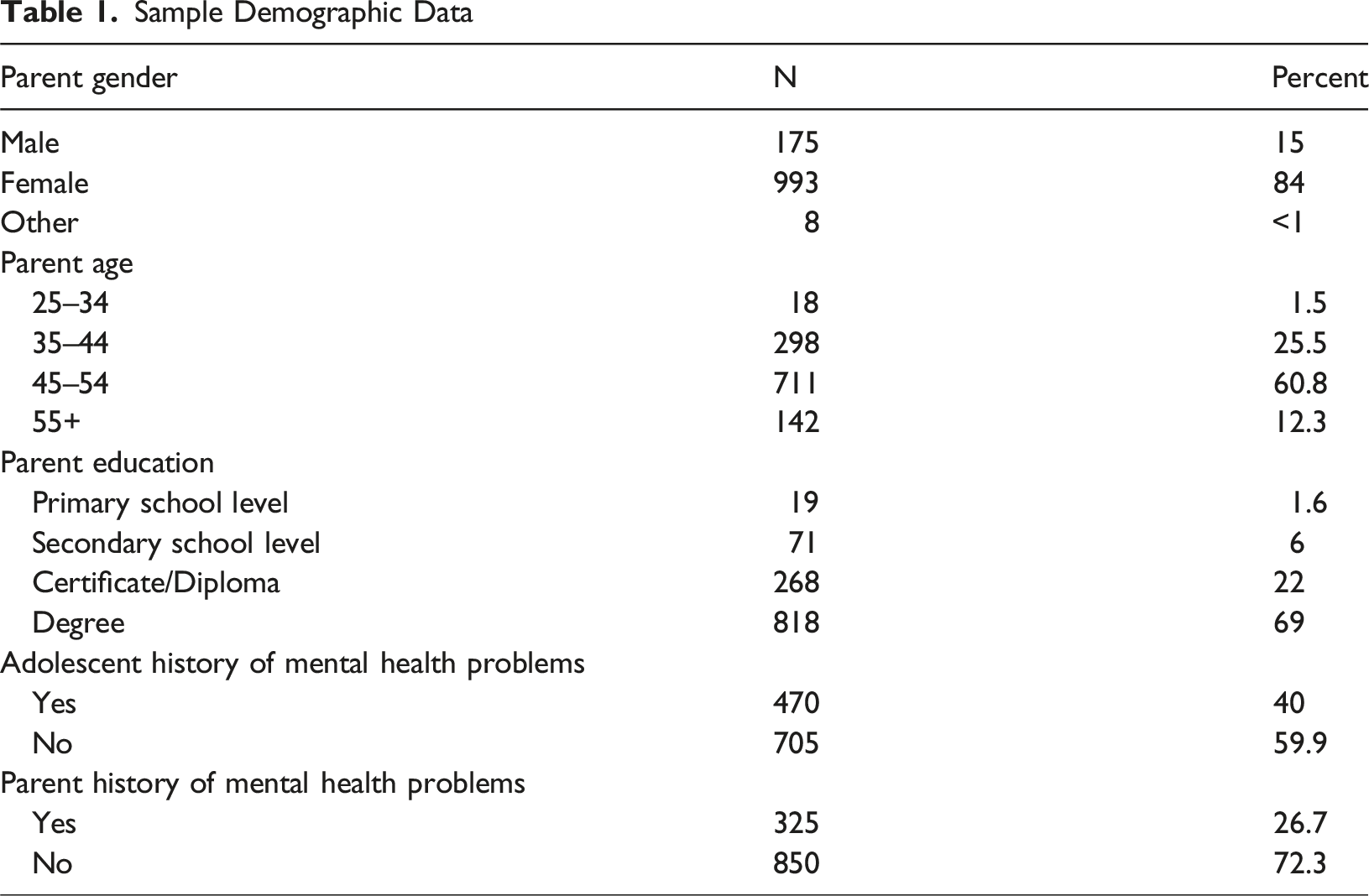
Sample Demographic Data
Predictor Variables
Vignettes
The vignettes depicted a mother (played by an actor) talking about her adolescent who was experiencing a recent change in their mood and behaviour (vignette transcripts are available in Supporting Information). The vignette scripts were based on analysis of interviews completed with parents who described their own experiences with their adolescent in the early stages of a mental health difficulty. There were 8 vignettes in total and each varied by: severity of the difficulty (mild/moderate; serious); whether the parent could attribute a cause for the difficulty described (cause; no cause); and the gender of the adolescent (female; male). In this study the causal component of the CSM was incorporated into the vignette. The vignettes were sent to twenty clinicians to check the credibility of the vignette and confirm the severity of the difficulty. For the mild to moderate vignette, all clinicians rated the vignette as mild to moderate. When asked if it was the type of problem they encountered in their professional practice 50% said sometimes and 50% said very often. For the serious difficulty vignette 75% rated it as moderate to severe. When asked if it was the type of problem they encountered in their professional practice 45% said sometimes and 45% said very often.
Illness Perception Scale
Illness perception was measured using the Revised Illness Perception scale (Moss-Morris et al., 2002). The scale consisted of 38 items rated on a 5-point scale from 1 “strongly agree” to 5 “strongly disagree”. The items measured three cognitive components and the two emotional components of the CSM. These include timeline (cyclical and acute), control (personal and treatment), emotional representation, illness coherence and consequence (Leventhal et al., 2016; Moss-Morris et al., 2002). In the acute subscale there were 6 items (e.g. “The problem will last a short time”). In the cyclical subscale there were 4 items (e.g. “The problem is very unpredictable”). In the personal control subscale there were 6 items (e.g. “The adolescent has the power to influence the problem”). In the treatment subscale there were 5 items (e.g. “Treatment can control the problem”). The emotional representation subscale had 6 items (e.g. “The problem does not worry me”). The illness coherence subscale had 5 items (e.g. “The problem is puzzling to me”). The consequence subscale had 6 items (e.g. “The problem is a serious condition”). Similar to other studies the scale was modified whereby the word “illness” was replaced with “problem” and the questions were framed for the parent’s perspective (Shanley & Reid, 2015; Witteman et al., 2011). In the present study the causal component of the CSM was incorporated into the vignette: in half of the vignettes the mother mentioned an event that might have precipitated a change in the adolescent’s mood and behaviour i.e. a falling out with a friend. This was chosen as it is a common cause of upset in adolescents (Efeoglu & Sen, 2021). The scale has good reliability when used with parents of children (α = .72 to .89; Shanley & Reid, 2015). The scale has also demonstrated good discriminant and predictive validity in the physical health context (Moss-Morris et al., 2002).
Covariates
A number of factors that have been found to impact parents’ help-seeking attitudes and illness perceptions were used as covariates. These include stigma, parent’s gender (1 = Male, 0 = Female), and previous engagement with the mental health system (1 = Yes, 0 = No) (Frauenholtz, et al., 2015). Parents were asked to indicate their gender and whether their child had previously engaged with mental health services. Stigma was measured using the Stigma Towards Seeking Psychological Help subscale of the Parental Attitudes Towards Psychological Services Inventory (PATPSI) (Turner, 2012). The subscale measured the extent to which parents were concerned about what others might think if they knew they were seeking professional help for their child. The sub-scale contained 8 items and was scored on a Likert scale from 1 “strongly disagree” to 5 “strongly agree”.
Outcome Variables
Help-seeking Intentions: The parent was asked, based on the description of behaviour provided by the mother in the video, whether if it was their child would they seek help (1 = yes, 0 = no).
Data Analysis
Confirmatory Factor Analysis: To test whether the Illness Perception scale used with this sample had the same factor structure as the original (Moss-Morris et al., 2002), confirmatory factor analysis in MPlus 8.2 was conducted (Muthén & Muthén, 2017). The robust weighted least squares estimator (WLSMV) based on the polychoric correlation matrix of latent continuous response variables was used as the data was ordered-categorical Likert response format. Model fit was assessed using several goodness-of-fit statistics; the chi-square (χ2) statistic, comparative fit index (CFI), Tucker-Lewis Index (TLI), root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). Using standard cut-off criteria (Hu & Bentler, 1999), a non-significant χ2 test (p > .05) indicates acceptable model fit; CFI and TLI values ≥.90 and ≥.95 indicate acceptable and excellent model fit respectively; RMSEA values ≤.08 and ≤.05 indicate acceptable and excellent model fit respectively; and SRMR values ≤.08 indicate good fit.
Regression Analysis: Preliminary analysis and inferential statistics were carried out using SPSS Version 24. A binary logistic regression analysis using maximum likelihood estimation and forced entry method was used initially to determine the significant relationships between the summed scores on the illness perceptions scale and the binary outcome variable of intentions to seek help. Bootstrapping was applied to the confidence intervals on both regression models to provide more simple robust estimates (Haukoos & Lewis, 2005).
Results
Descriptive Statistics
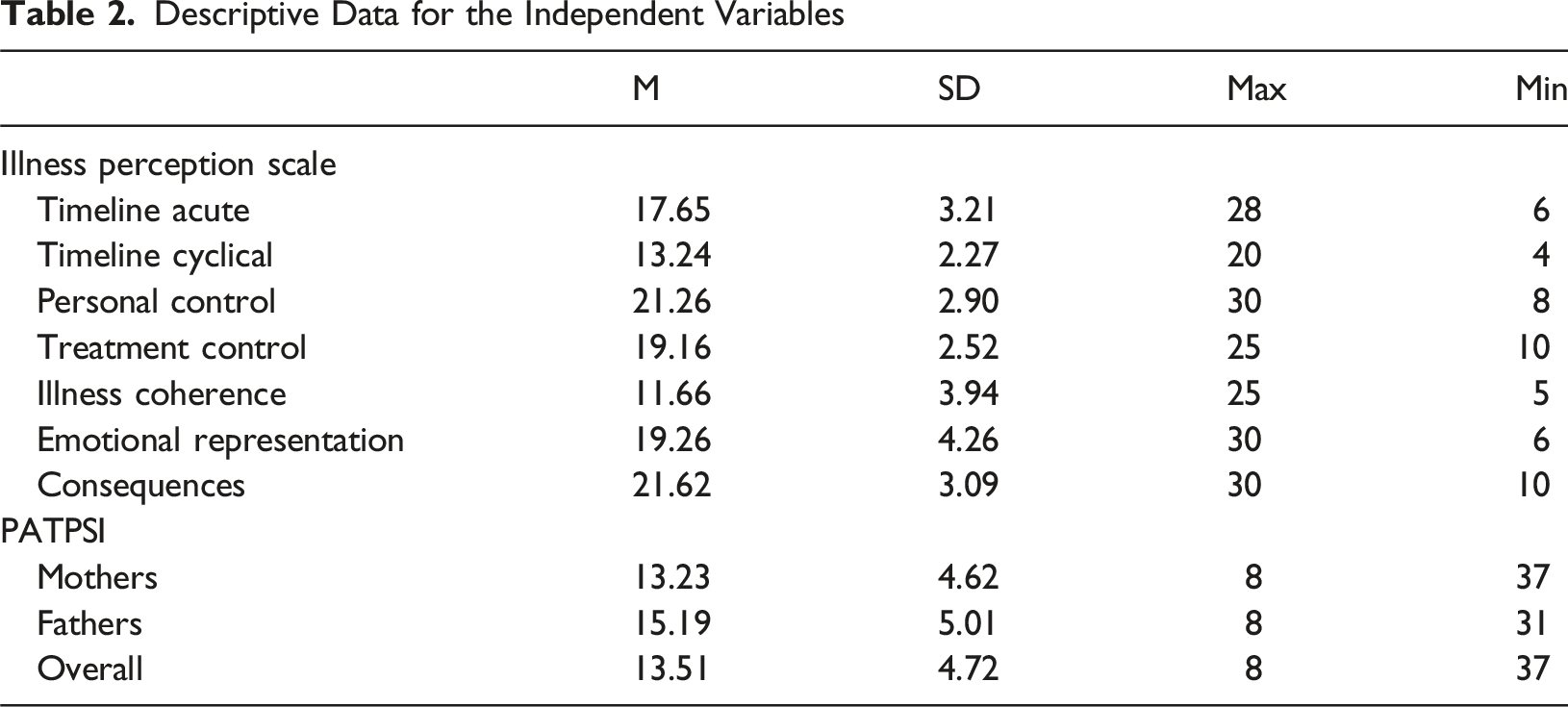
Descriptive Data for the Independent Variables
Confirmatory Factor Analysis
Model Fit Indices
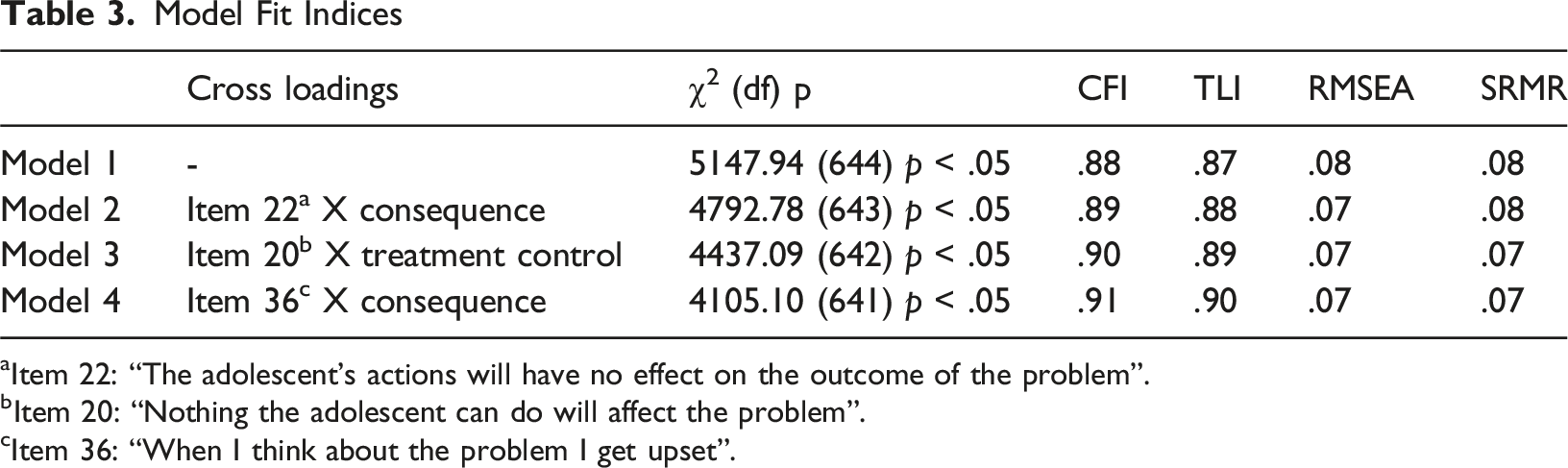
aItem 22: “The adolescent’s actions will have no effect on the outcome of the problem”.
bItem 20: “Nothing the adolescent can do will affect the problem”.
cItem 36: “When I think about the problem I get upset”.
Logistic Regression
Preliminary analysis and inferential statistics were carried out using SPSS Version 24. A binary logistic regression analysis using maximum likelihood estimation and forced entry method was used initially to determine the significant relationships between the summed scores on the illness perceptions sub-scales and the binary outcome variable of intentions to seek help. In order to generate a parsimonious model those predictors that were not statistically significant in this initial model (timeline cyclical, timeline acute, cause and illness coherence) were removed and the model re-estimated. Bootstrapping was applied to the confidence intervals on both regression models to provide more simple robust estimates (Haukoos & Lewis, 2005). The logistic regression model was repeated with the inclusion of covariates: fathers (to compare with mothers), stigma, and whether the adolescent previously had a mental health difficulty (to compare with those who did not)).
All predictor variables were significant. Parents who had higher scores on treatment control (OR: 1.24 95% CIs [1.24–1.55]) and emotional representation (OR:1.082 CIs [1.013–1.157]) were more likely to report intending to seek help. Higher score on personal control (i.e., the parent thought the adolescent was in control of the problem) was associated with lower intentions towards seeking help (OR: .87 CIs [.78–.96]). While expecting the problem to have negative consequences for the adolescent was also associated with higher intention to seek help (OR: 1.41 CIs: [1.27–1.55]). In terms of the covariates, being a father (OR: .255 [CIs .13–.40]), or having a higher stigma score (OR: .911 [CIs: .87–.96]) were associated with a lower intention to seek help. If their adolescent previously had a mental health difficulty it was associated with a higher intention to seek help (OR: 3.74 CIs [1.87–7.43]). See Table 3 for detailed model information.
Discussion
Coefficients of the Model Predicting Help-Seeking [95% BCa Bootstrap Confidence Interval Based on 1000 Samples in Brackets]
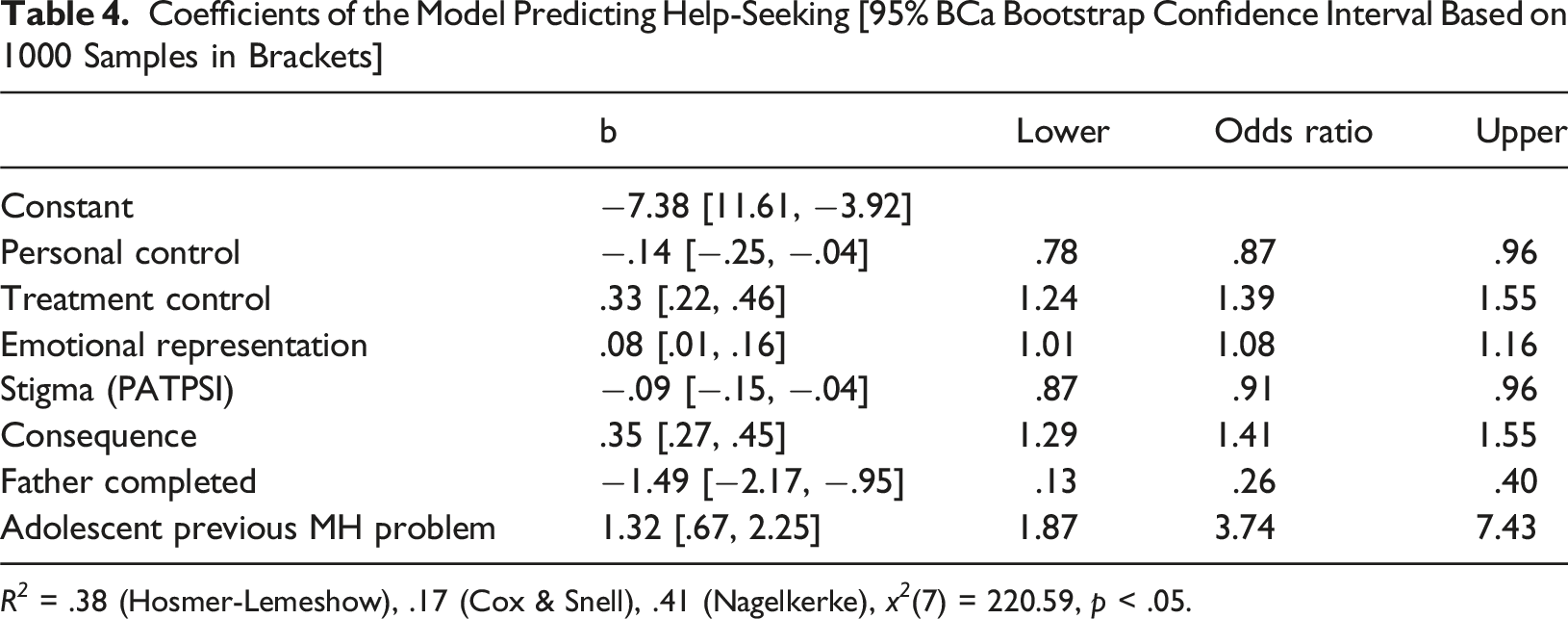
R 2 = .38 (Hosmer-Lemeshow), .17 (Cox & Snell), .41 (Nagelkerke), x 2 (7) = 220.59, p < .05.
Our findings regarding the application of the CSM to parents’ help seeking intentions are broadly similar to previous research on the relationship between illness perceptions and help-seeking from mental health services. Shanley and Reid (2015) explored how parents’ illness perceptions were related to the types of mental health treatment sought for their children. Their results indicated that parental perception of treatment control significantly predicted the type of treatments they sought; and parental emotional representation and beliefs about timelines (chronic) were significant predictors of seeking parent and family therapy.
Vanheusden et al. (2009) found similar results when exploring how young adults’ illness perceptions about mental health problems shaped their help-seeking behaviours: Perceiving a mental health difficulty as having negative consequences, belief that treatment would control the problem and that the problem was chronic, were associated with increased likelihood of service use; greater belief that the adolescent had personal control of the problem was associated with decreased likelihood of service use. These findings are interesting and suggest that parents and adolescents have broadly similar illness perceptions which in turn predicts help-seeking behaviours.
To date there have been very few models proposed in the literature to understand parental help-seeking behaviour and any models that have been proposed e.g. Logan and King (2001) have not been empirically tested. While the CSM is a useful framework for understanding health behaviours it has not yet been studied extensively in relation to mental health problems and even less to understand how parents’ illness representation influence decisions to seek professional mental health support for a child or adolescent. Understanding how parental perceptions influence their help-seeking intentions is important because they must initiate the help-seeking process before the young person is legally old enough to do so independently. Some of the limitations of the model that have previously been identified are, therefore, particularly relevant when the model is applied to parent help-seeking for mental health problems. For example, Fortune et al. (2005) argue that the model fails to address self-efficacy beliefs or how the individual appraises the stressfulness of the situation. Johnston (2019) has also highlighted the limitations of relying solely on a scale to measure illness representations because it is an approach that necessarily limits understanding of the richness of the individual’s beliefs. Johnston (2019) also notes the limitations inherent in a model that relies on conscious beliefs and does not account for unconscious forces that motivate behaviour. When considering how the CSM might be used to understand parent help-seeking for mental health problems, future research should explore aspects of the parent-adolescent relationship as this may also influence help-seeking intentions.
Limitations
The study’s limitations also have to be acknowledged. This study used video vignettes to explore parental beliefs about a distressed adolescent’s need for mental health support. No other channel (audio, text) was used and therefore, channel specific effects could not be controlled for. The symptoms presented were not matched to any specific disorder as defined in diagnostic manuals but were chosen to represent “a deviation from a person’s previous experience and behavior” (Yung & McGorry, 1996, pp. 353) and our consultation with clinicians indicated that the symptoms described are ones that they encounter regularly in their professional work. However, previous research findings indicate that there can be differences in individual’s illness perceptions depending on the mental health problem they are experiencing (Baines & Wittkowski, 2013), thus it is possible that there are differences in parents’ illness perceptions depending on the specific problem experienced by their child. A high proportion of parents in this study reported they would seek help for their adolescent if they were in the same situation as the vignette character. However, the hypothetical nature of a video vignette contrasts with the reality that many parents can find it difficult to recognise their adolescent is in distress (Teagle, 2002) and, therefore, not recognise that it would be appropriate to seek help. Furthermore, the parent included in the vignette was a mother. This may have resulted in gender differences in how the participant identified with the individual in the vignette and may also contribute to the gender related effect found in relation to help seeking intentions. Finally, this study only looks at intentions towards seeking help rather than help-seeking behaviour, however, there is some evidence that help seeking intentions predict help-seeking behaviour for adults with depressive symptoms (Tomczyk et al., 2020).
Despite the limitations of this study, the results have important implications for designing interventions or public health campaigns to promote parental help-seeking behaviour. While the research is limited regarding the role of interventions to shape illness perceptions, there is some limited evidence to suggest that an intervention designed to change illness perceptions can be effective in improving illness outcomes (Lee et al., 2015). The findings of the present study suggest that interventions would benefit from an emphasis on the importance of seeking treatment for adolescent mental health difficulties and the consequences for the adolescent if help is not sought. As shown from the results of this study, fathers are less likely to report help-seeking intentions. Fathers play an important role in their child’s life and if fathers have negative attitudes towards help-seeking this will undoubtedly have implications for their child.
Conclusions
This study makes an important theoretical contribution to our understanding of parental recognition of an adolescent mental health difficulty. A randomised experimental design was used to test whether CSM could explain parental help-seeking intentions. Perceived consequences, treatment control and emotional representations predicted higher intentions to seek help amongst parents. Greater perceptions of personal control predicted lower intentions to seek help. This study has important implications for how to support parents when deciding to seek help for an adolescent. Parents need education emphasising the benefits of treatment and the potential consequences if treatment is not sought for their adolescent. Future research could explore the effect illness perceptions including, consequences, treatment control and emotional representations, have on the parent supporting access to treatment for their adolescent, ensuring that their adolescent adheres to treatment and their engagement with recommendations relating to parental involvement.
Supplemental Material
Supplemental Material - Does the Common-Sense Model of Illness Representations Predict Parent Help-Seeking for Adolescent Mental Health Distress?
Supplemental Material for Does the Common-Sense Model of Illness Representations Predict Parent Help-Seeking for Adolescent Mental Health Distress? by Daráine Murphy, Caroline Heary, Mark Shevlin and Eilis Hennessy in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgements
Apart from the named authors no others were involved in the writing, preparation or editing of this manuscript.
Ethical Approval and Informed Consent statements
Ethical permission for this research was granted by University College Dublin Human. Research ethics committee (HS-21-06-Murphy-Hennessy). Participants were fully informed of the purpose of the study prior to participating and were asked to indicate their consent via an online form confirming they had read the information sheet and were happy to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Health Research Board Ireland (CDA-FA-2018-001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset is being prepared for submission to the Irish Social Science Data Archive from where it will be freely available. In the interim we are happy to provide copies of the dataset for legitimate purposes to other researchers and educators.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.