
Abstract
Psychiatric hospitalization of a child or adolescent is a highly stressful time for parents, who play a central role in their child’s mental illness and recovery. Little is known of evidence-based interventions to support parents during their child’s admission. This scoping review aims to examine the evidence for existing parent-focused interventions in the acute inpatient child and adolescent psychiatry setting. A literature search was conducted across six databases. Three authors were involved in screening and data extraction procedures. Results were categorized by (1) intervention format, (2) intervention content and treatment targets, (3) feasibility outcomes, and (4) parent outcomes. Nine studies encompassing 9 interventions were included in the final review. Interventions included parent groups (n = 3), 1:1 peer support (n = 2), individualized family-based assessments and interventions (n = 2), an adolescent milieu curriculum (n = 1), and a website intervention (n = 1). Outcomes were heterogeneous which limited comparison between interventions. All interventions were well-received by parents. We conclude that results of this review do not support any one intervention, though all led to parent satisfaction. Some feasibility challenges were encountered, which should be considered in future implementation. More rigorous studies are needed to provide stronger evidence for any one type of parent-focused intervention in the acute inpatient child and adolescent setting.
Plain language summary
Having one’s child admitted into a mental health hospital is a highly stressful time for parents, who play a central role in their child’s mental health and mental health recovery. Little is known on how to effectively support parents during their child’s admission. The authors searched the literature to find what interventions have already done to support parents during their child’s short-term mental health hospital stay. To do this, a librarian first searched many databases for relevant articles. Three authors then narrowed down these articles and compiled their relevant information. Results were categorized by (1) intervention format, (2) intervention content and treatment targets, (3) intervention feasibility outcomes, and (4) parent outcomes of the intervention. Nine studies encompassing 9 interventions were included in the final review. Interventions included parent groups (n = 3), 1:1 peer support (n = 2), individualized family-based assessments and interventions (n = 2), a daily curriculum for an adolescent unit (n = 1), and a website (n = 1). Outcomes were highly varied which did not allow us to compare one intervention with another. All interventions were well-received by parents. We conclude that results of this review do not support any one intervention, though all seemed acceptable and satisfactory to parents. Some challenges in carrying out the intervention itself were encountered, which should be considered in future implementation. Overall, more robust research is needed to see how different types of parent interventions might compare in how they best support parents while their child is admitted at a mental health hospital.
Introduction
It is widely understood that parents and caregivers (hereafter referred to as parents, unless referred to as otherwise by a referenced primary source) play a crucial role in their child’s mental health. The prevalence of mental illness in children and adolescents has increased over time, resulting in greater mental health service utilization (Agency for Healthcare Research and Quality (US), 2022). The highest and most restrictive level of care is acute psychiatric hospitalization, in which youth receive intensive treatment and stabilization in the hospital setting for several days, largely separate from their parent and family. Given the central role of parents in child and adolescent mental health treatment outcomes, parent engagement during an acute psychiatric crisis is important to understand.
Systematic reviews consistently find that parental factors, such as abuse, lack of warmth, over-involvement, inter-parental conflict, and aversiveness toward their child influence their child’s depressive, anxious, and internalizing symptoms (Yap et al., 2014; Yap & Jorm, 2015). In other studies, parent psychopathology and punitive parenting styles increased the risk of child and adolescent psychiatric disorders up to three-fold (Fatori et al., 2013; Vostanis et al., 2006). Further, parenting behaviors are associated with the development of, or are even protective of, externalizing behavior disorders (Hutchings & Lane, 2005).
Family participation in driving child and adolescent mental health care has also historically and consistently shown benefit (Spencer et al., 2010). Involving parents in child psychotherapy improves child treatment outcomes (Dowell & Ogles, 2010) and reduces functional impairment. Various family interventions have shown to be helpful with child psychopathology (Sharma & Sargent, 2015). Behavior-based parent interventions have been found to be effective in reducing disruptive behavior in children (Hutchings & Lane, 2005), and even improve parent outcomes (Dekkers et al., 2022). Emotion-focused parenting interventions have also been found to be effective in improving anxiety, depression, attachment, emotion regulation, etc (Havighurst et al., 2020). Various parent-focused interventions have also been associated with improved child and adolescent eating disorder psychopathology (Le Grange et al., 2016; Rosello et al., 2021). High-quality preventive parenting programs also exist, though are inconsistently carried out in practice (Hutchings & Lane, 2005). These family interventions usually last weeks to months.
Caring for children and adolescents with psychiatric disorders is associated with high levels of parenting stress, burden, and burnout, especially when many of them also struggle with psychiatric illness themselves (Dada et al., 2011; Molebatsi et al., 2017). A 2013 meta-analysis showed greater stress in parents of children with ADHD when compared with non-clinical controls; children with comorbid conduct disorder further increased stress (Theule et al., 2013). High depression and burnout levels have been found among parents of children with autism spectrum disorder (Chua et al., 2023; Kutuk et al., 2021), and with anorexia nervosa (Duclos et al., 2023). Parents may carry self-blame and guilt around their child’s mental health diagnosis, face stigma from others toward their children and themselves, struggle socioeconomically in trying to meet their child’s needs, feel overwhelmed by their lack of understanding of their child’s mental illness, and feel inadequately supported by the health care system (Pereira et al., 2024).
Parents also experience increased stress when their child is admitted to a psychiatric unit for an acute crisis. Reasons for admission may include acute suicidality or self-harm, psychosis, mania, or other resurgence in psychiatric symptoms posing a threat of harm to themselves or others. The goal of a psychiatric admission is to achieve acute safety and stabilization, which typically takes place in a locked unit separated from their parents, with lengths of stay around several days. In these episodes of care, parents may experience financial or occupational hardship, strains in family relationships, feeling judged, embarrassed, or at fault (Merayo-Sereno et al., 2023), and challenges with dealing with the mental health system (D’Angelo et al., 2023). Parents often seek higher level of care for their child due to difficulties at home (So et al., 2021), and hope to address these difficulties during an inpatient stay (Bradley & Clark, 1993). Thus, hospitalization may present a time where supporting parents in managing their child’s emotional and behavioral difficulties feels most relevant to them, especially while their children are being supported in the safe and secure environment of an inpatient setting.
There may be important benefits to engaging families in their child’s treatment when they are admitted for an inpatient psychiatric stay. One study found that family engagement in the child and adolescent inpatient setting led to lower rates of rehospitalization of youth (Brinkmeyer et al., 2004). Models of family engagement have been proposed in the inpatient setting, from short-term family interventions (Sourander & Piha, 1996) to having parents admitted with their children (Cousins & Holmes, 2021). A few studies have also explored inpatient parent interventions lasting 4–5 weeks, showing benefits in parenting and parent mental health (Ise et al., 2015; Schwenck et al., 2016). There is the need to systemically aggregate and summarize this literature to better understand the evidence on these interventions for acute inpatient stays. The purpose of this scoping review is to summarize evidence on parent interventions in the acute inpatient child and adolescent psychiatry setting.
Methods
The scoping review was conducted following guidelines by Levac et al. (2010) and Arksey and O’Malley (2005). A scoping review is a useful way to map the current state of the literature in a field where the range of research activity is not well-known. It is also the preferred methodology to identify research gaps, determine the feasibility of a full systematic review, and summarize and disseminate research findings. The review protocol was registered in the Open Science Framework registries on February 16, 2024 (https://osf.io/pefxm).
Data sources and strategies
A search strategy was derived by a librarian (RW) based on the research question, “What interventions exist for parents and caregivers in an acute inpatient child and adolescent psychiatry setting during their child’s hospitalization?” A comprehensive search was conducted using PubMed (NLM), Embase (Elsevier), CINAHL (EBSCOhost), PsycINFO (ProQuest), Web of Science (Clarivate), and Cochrane Library (Wiley) in February 2024. Results were limited to English language and publication after 1995; this date was chosen because it was determined that the average length of a psychiatric hospitalization for a child and adolescent since that year is similar to what it is in current practice, if assumed to be 7 days (Case et al., 2007). We also conducted manual searches of reference lists of relevant review articles. We sought only published primary materials; thus, grey literature was not included. Full search strategies can be found in the Supplementary Materials, Appendix S1.
Eligibility criteria
Inclusion criteria consisted of the following: (1) the intervention targeted parents and caregivers of children and adolescents currently psychiatrically hospitalized; (2) at least 50% of the intervention was delivered during the hospitalization; (3) peer-reviewed publications in the English language, publication in or after 1995. Original research, reviews, case studies, and case reports were included. Studies were excluded if: (1) the population did not primarily consist of parent and caregivers of psychiatrically hospitalized youth; (2) the intervention did not occur in/during their child’s acute inpatient hospitalization (e.g., outpatient clinics, partial or intensive outpatient programs, homes, or school); (3) interventions in residential facilities or admissions where average length of stay was at least a month; (4) publication prior to 1995.
Study selection process
Results from the search strategy were imported into Covidence Systematic Review Software (2022) on February 13, 2024. All references first underwent title and abstract screening by two authors independently (among KH, KG, and KT). They met periodically throughout the screening process to reconcile discrepant screening decisions. Any discrepancies that were unable to be reconciled went to a third author (AB), who is an expert in research among family and caregiver populations. After duplicates were removed, 5453 references underwent title and abstract screening. Of these, 122 references proceeded to full text review. All full texts were again screened by two authors at a time independently (among KH, KG, and KT), with unresolved discrepancies going to a third author (AB). Nine studies were included in the final review (Figure 1). PRISMA flow diagram.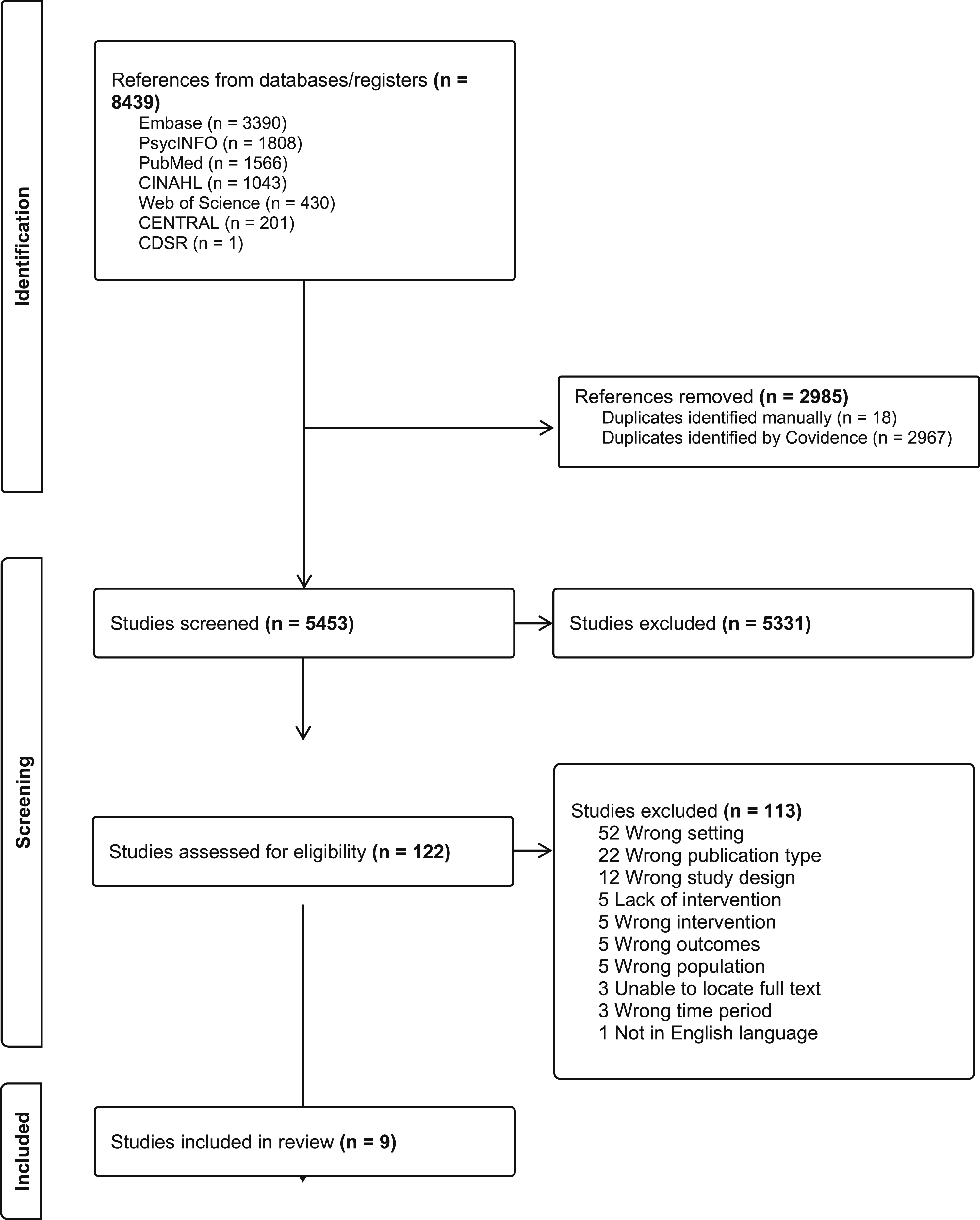
Data extraction and analysis
Among the final included studies, two authors (among KH, KG, and KT) independently extracted data from each study for the following variables: study dates, study design, study setting and location, characteristics of the parent population, characteristics of the child and adolescent population, description of the intervention, description of comparator groups, intervention duration/timing/frequency, and parent outcomes. Any unresolved discrepancies were brought to a third author (AB) for reconciliation. Results of data extraction were compiled into tables reviewed by all authors.
Results
Overview of study interventions.
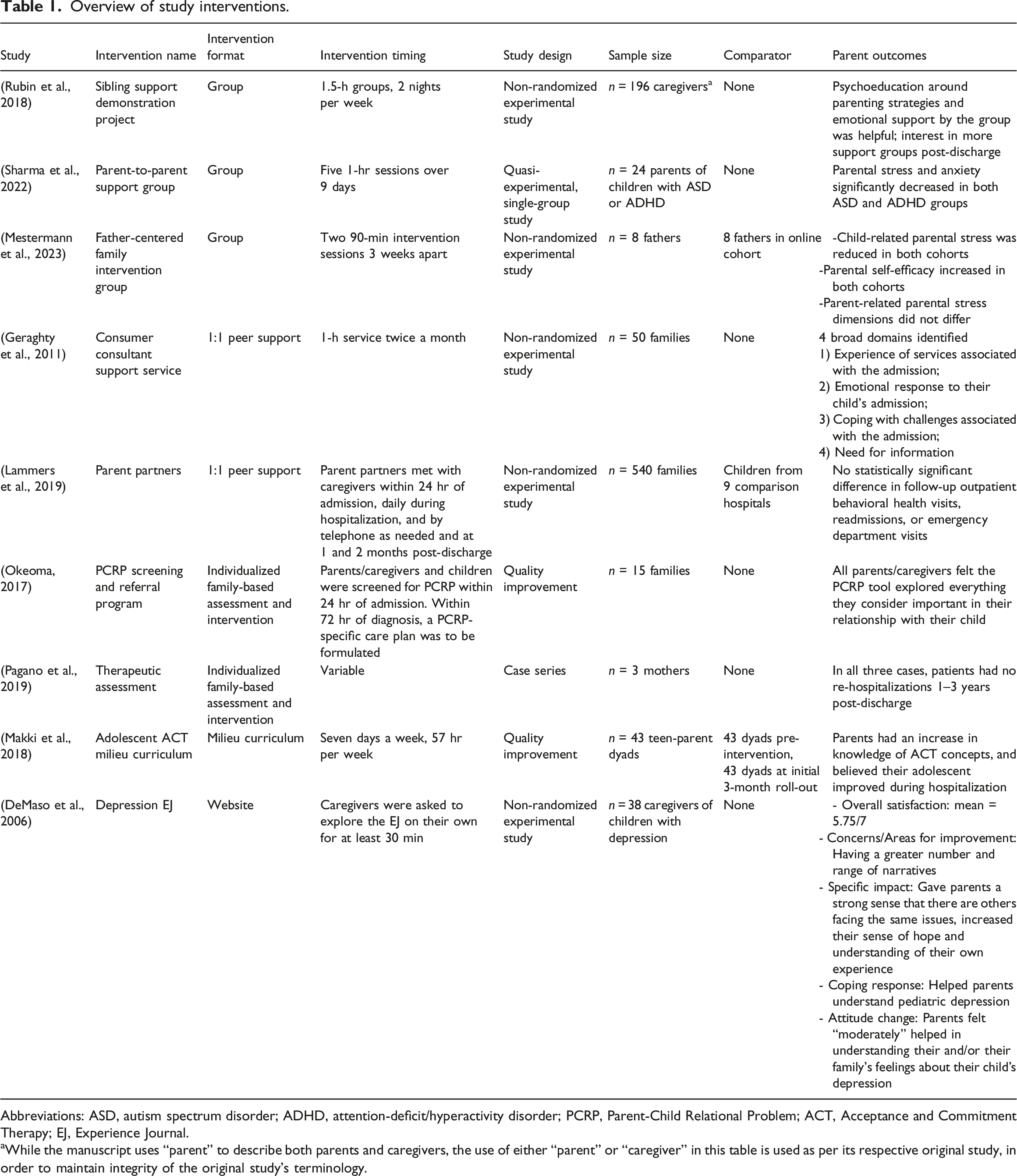
Abbreviations: ASD, autism spectrum disorder; ADHD, attention-deficit/hyperactivity disorder; PCRP, Parent-Child Relational Problem; ACT, Acceptance and Commitment Therapy; EJ, Experience Journal.
aWhile the manuscript uses “parent” to describe both parents and caregivers, the use of either “parent” or “caregiver” in this table is used as per its respective original study, in order to maintain integrity of the original study’s terminology.
Intervention format
Intervention formats were highly heterogeneous and included parent groups (n = 3) (Mestermann et al., 2023; Rubin et al., 2018; Sharma et al., 2022), 1:1 peer support (n = 2) (Geraghty et al., 2011; Lammers et al., 2019), individualized family-based assessments and interventions (n = 2) (Okeoma, 2017; Pagano et al., 2019), an adolescent milieu curriculum (n = 1) (Makki et al., 2018), and a website intervention (n = 1) (DeMaso et al., 2006). Group formats varied from a single drop-in session during visitation, as in the Sibling Support Demonstration Project (Rubin et al., 2018), to a multiple-session curriculum, as in the Parent-to-Parent Support Group for parents of children with ASD and ADHD (Sharma et al., 2022) and the Father-Centered Family Intervention Group (Mestermann et al., 2023), the latter of which compared both an online and in-person cohort. 1:1 peer support also varied widely in their degree of parental involvement. The Consumer Consultancy Service was driven entirely by parent initiation to approach freely available consultants (Geraghty et al., 2011); in contrast, in the Parent Partners intervention, each parent partner was assigned one family, had personal contact with caregivers at least daily, and attended daily behavioral health team rounds. Like 1:1 peer support, the two individualized family-based assessments offered personalized attention. However, this attention was directed more toward the family unit, and there were also more formalized assessments. The Parent-Child Relational Problem (PCRP) screening and referral program involved a screening at admission followed by intervention and/or referral (Okeoma, 2017); the Therapeutic Assessment intervention involved a more comprehensive assessment by a psychologist or psychology trainee, followed by a family intervention session and feedback (Pagano et al., 2019). The Adolescent Acceptance and Commitment Therapy (ACT) milieu curriculum followed a 7-day rotation on the adolescent unit of evidence-based groups based on ACT principles which, while not involving parents directly, was intended to increase parental understanding of unit programming and of the skills their children were learning (Makki et al., 2018). Lastly, the Depression Experience Journal (EJ) offered a website to parents on admission that could be viewed at any time during the hospitalization (DeMaso et al., 2006).
Intervention content and treatment targets
The three group interventions all targeted different parent populations: parents whose hospitalized child had siblings (Rubin et al., 2018), parents of children with ADHD or ASD (Sharma et al., 2022), and fathers (Mestermann et al., 2023). Nevertheless, the content had similar themes: psychoeducation on child and adolescent mental health, parenting strategies, and mutual exchange and support among parents. These groups aimed to achieve parental satisfaction with the intervention, improve parental competency, and reduce parental anxiety and stress. The two 1:1 peer support interventions provided therapeutic support, practical advice, and assistance with navigating behavioral health services for their child. The studies examined the ways parents utilized the peer support resource, and if mental health services for their child were utilized upon discharge. The individualized family-based assessments focused on assessment of parent-child relationships, then provided an inpatient family intervention, and possible additional referral for treatment. These studies examined parental satisfaction with the intervention, and Pagano et al. (2019) gave anecdotal reports of post-hospitalization outcomes. The ACT milieu curriculum had daily adolescent community, mindfulness, media, and other ACT-specific groups. The intervention measured parent understanding of the inpatient model and their satisfaction with their child’s inpatient experience. Finally, the web-based intervention, Depression EJ, aimed to foster an electronic community for families of children with depression, by sharing stories from patients, parents, siblings, and hospital staff on a website. The goal of this intervention was for parents to feel supported and improve their coping and attitudes related to childhood depression.
Feasibility outcomes
Summary of feasibility outcomes are found in Supplementary Materials, Table S2. Eight of the nine included studies indicated that parents were satisfied with their respective intervention, with some notable comparisons. In the Father-Centered Family Intervention Group, fathers in the in-person cohort had significantly higher contentedness ratings than those online. In the Adolescent ACT milieu curriculum intervention, parent satisfaction increased after the intervention was implemented when compared to before. The Parent-to-Parent Support Group did not report on parent satisfaction, though the attrition rate of their intervention was zero and parents experienced positive outcomes. Regarding recruitment, between the two 1:1 peer support interventions, the Parent Partners intervention had 10 times the recruitment as the Consumer Consultancy Service (540 and 50 families, respectively) over two years. The Parent Partners intervention also found that 96% of caregivers offered the intervention enrolled and demonstrated “strong engagement” with the program. Notably, the intervention reported challenges with staffing parent partners, who had to tend to their own child(ren) with mental health problems, and with engaging behavioral health clinicians, with the latter improving over time. The PCRP screening and referral program also ran into recruitment challenges, where study staff were not always available to meet parents on admission. The referral part of the intervention was also not carried out, and families screening positive for PCRP received the same intervention as those without (i.e., therapy during hospitalization, without therapy referrals after discharge). With recruitment for the Depression EJ, 45% of eligible caregivers declined to participate due to being unable to present in-person (16%), feeling overwhelmed or disinterested (22%), or dealing with their own health problems (6%).
Parent Outcomes
All three group interventions resulted in either reduction in parental stress or increased perceived emotional support post-intervention. Two also reported practical benefits (i.e., increased self-efficacy, gaining parenting resources and strategies). The Father-Centered Family Intervention Group showed similar reductions in-person and online in child-related parental stress and self-efficacy. Outcomes of the Consumer Consultant Service brought insight to parent needs and experiences during their child’s hospitalization – parents used the space to express their dissatisfaction with mental health services (59%), share feelings of guilt (36%) and anxiety (29%) and family challenges (35%), and expressed a need to learn more about their child’s mental illness (24%). The Parent Partners intervention evaluated follow-up care 30–90 days from discharge and found no differences when compared with control hospitals. The Therapeutic Assessment was the only intervention reporting long-term outcomes one to three years post-hospitalization, with no re-hospitalizations while remaining in outpatient treatment, though these outcomes were based on anecdotal reports and from just three case reports. The Adolescent ACT milieu curriculum study reported increased parental knowledge of group programming and ACT concepts, and that parents believed their adolescent had improved during the hospitalization. The Depression EJ helped families feel that they are not alone in raising a child with depression (mean = 6.44/7), increased their understanding of their own experience (mean = 5.4/7), and helped 76% of parents understand the symptoms of pediatric depression.
Discussion
This scoping review summarizes research findings of parent interventions in the acute inpatient child and adolescent psychiatric setting. We found only nine peer-reviewed manuscripts describing these interventions, which varied in format, content, and outcomes measured. Outcomes measured were also inconsistent, making it difficult to make meaningful comparisons. While parents reported being satisfied with these interventions, overall results do not support any one type of intervention for parents in the acute inpatient setting. However, review findings do allow us to understand the strengths and limitations of existing interventions and offer important insights into future directions for developing effective parent interventions in acute inpatient settings.
Groups were the most common type of intervention in this review. While target populations varied, each group provided psychoeducation, mutual parental support, and coping skills. Groups may be particularly well-suited for the inpatient setting, as they connect parents with shared experiences, are more efficient, and require less staffing to deliver. Groups do require trained clinical staff to facilitate and can be challenging to match parent availability. Literature condones groups as a powerful source of support for parents of children with mental health problems; they can be a promising approach to use in the psychiatric hospital setting (O’Brien, 2002).
The two methods of 1:1 peer support in this review were very different. The degree of parental involvement varied from having a one-time drop-in session, to daily interactions with an assigned parent partner, showing that diverse approaches can be employed. A peer support model that more heavily involves parents and peer workers may face implementation challenges related to buy-in from clinicians and maintaining staffing. On the other hand, too little parental involvement may not be sustainable long term. Aside from these challenges, 1:1 peer support can offer valuable, individually tailored therapeutic and practical benefits.
Individualized family-based assessments in this review had weaker study designs, making conclusions difficult to draw. In theory, the personalized, family orientation of the Therapeutic Assessment would be ideal for children and adolescents in acute crises (Spencer et al., 2010). However, these interventions may be more labor-intensive and require greater expertise and training. Ethical dilemmas from conducting family therapy in inpatient settings include ability to consent free from coercion, relationships between families and hospital staff, and the limited duration of a psychiatric hospitalization (Namyslowska & Siewierska, 2008).
The uncertainty of the care provided on a psychiatric unit is a challenging experience for parents (Merayo-Sereno et al., 2023). Having a predictable milieu curriculum that is shared with parents may alleviate this uncertainty, offer reassurance on their child’s care, and even provide psychoeducation on evidence-based therapies. Its disadvantages are the limited direct parent intervention (though one can consider modifying milieu curricula to include parents), need for leadership and staff buy-in and training, and need for structural change.
Technological applications have been rising in mental health intervention (National Institute of Mental Health, 2024). Technology may help to increase access to services, efficiently disseminate information, and provide means of connection with those who otherwise would have barriers to care. In this review, the Depression EJ provided an accessible way to share stories and experiences from various perspectives, which helped parents not only better understand their child’s depression but also feel less alone themselves. One consideration is how the sense of connectedness may differ with its in-person version. Use of technology-based interventions is further restricted to those who have internet access and know how to use it, which might disproportionately exclude disadvantaged populations (Fortuna, 2022; Saeed & Masters, 2021).
The review of the extant literature on parent-focused interventions in the child and adolescent inpatient setting elucidates important shortcomings that are potential targets for future research. First, outcomes were heterogeneous, which prevented meaningful comparison between interventions. For an acute setting, it is not clear what the most effective or meaningful outcomes to measure would be, for which future research is also needed. From this review, potential outcome variables may include parent satisfaction, perceived emotional support or self-efficacy, understanding of their child’s mental health, and parental mental health symptoms such as anxiety, depression, and stress. To determine the impact of these programs, one may also consider long-term outcomes, including rates of rehospitalization and emergency department visits. Further, most studies did not report on parent demographics; those that were reported were not consistent across studies and thus unable to be aggregated. Future studies should capture demographic variables such as sex and gender identity, race, household income, level of education, disability, etc. to ensure that populations from less represented and disadvantaged groups are being captured.
Second, randomized clinical trials are needed to improve our understanding of what interventions are most efficacious in this setting. Among our included studies, only three (Lammers et al., 2019; Makki et al., 2018; Mestermann et al., 2023) included a control group comparison. One-third of the studies were either case studies or quality improvement projects, which provide lower quality evidence. More rigorous study designs, ideally randomized controlled trials, are needed, though they present their own design challenges. The inability to blind participants in these interventions may overestimate treatment effects. The voluntary nature of recruitment also subjects outcomes to detection bias, as the parents who are more likely to consent are generally more motivated and open to receive support. Feelings of guilt, shame, and overwhelm, rates of mental illness and stress, and fear of stigma are common among this population and may be barriers to study participation, when these individuals seek to benefit from support interventions the most. These challenges should be considered in study designs to decrease risks of bias.
Third, just as important as the effectiveness of the intervention is its feasibility to be tested. Feasibility studies address the problem of how a more formal randomized controlled trial to test the intervention would be carried out. This includes assessing ability to recruit and randomize participants, and determining suitable outcome measures, sample size, follow-up and compliance rates, and others (Arain et al., 2010). Some feasibility challenges encountered by the interventions in this review that are worthy considerations in future interventions include engaging behavioral health clinicians, maintaining staffing, and ensuring that interventions are carried out as intended. Further efforts to increase study feasibility may improve effectiveness outcomes.
Conclusion
Evidence-based interventions for parents in the acute child and adolescent inpatient psychiatric setting are few, heterogeneous, and though generally well-received by parents, have limited rigorous study designs to determine what interventions may be most impactful in this setting. More research is needed to draw conclusions about what intervention modalities may be effective for parents of youth who are psychiatrically hospitalized. For clinicians interested in offering parents support in this setting, we recommend that they consider the advantages and disadvantages to each approach and how it may apply to their own institution. Clinicians may also refer to other parent-focused interventions outside of this setting for guidance on skills and approaches that have been useful for changing parent outcomes.
Supplemental Material
Supplemental material - Parent-focused interventions delivered in the inpatient child and adolescent psychiatry setting: A scoping review
Supplemental material for Parent-focused interventions delivered in the inpatient child and adolescent psychiatry setting: A scoping review by Kimberly S Hsiung, Kelly Geelan, Katherine Trapani, Rachel Walden, Jon S Ebert and Alexandra Bettis in Clinical Child Psychology and Psychiatry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
Data related to the findings of this study are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.