
Abstract
This study aimed to examine the relationship between school mental health service use in high school and educational outcomes of adolescents with psychiatric disorders. The sample included 2617 adolescents who were enrolled in eighth grade in a large urban school district in the United States, were enrolled in Medicaid during eighth grade, and had a mental health diagnosis. Psychiatric hospitalization, school enrollment, school absences, out-of-school suspensions, school dropouts, and school exits for negative reasons were examined as mental health and educational outcomes. Compared with adolescents who used school mental health services for 2 years following eighth grade, adolescents who did not use school mental health service during the high school years had a significantly lower annual number of days enrolled in school and higher rates of exiting school for negative reasons such as school dropout and long-term hospitalization. Our findings support the positive role of school mental health care delivery in high schools in preventing negative educational outcomes for adolescents with psychiatric disorder.
Keywords
Introduction
Adolescence is a critical developmental stage for mental wellbeing (World Health Organization, 2021). Major changes occur in school environments, peer relationships and academic curriculum during this developmental stage (Langenkamp, 2010; Longobardi et al., 2016) and these changes can lead adolescents to experience anxiety, emotional distress, depressive symptoms and feelings of loneliness (Benner et al., 2017). Adolescents with psychiatric disorders experience additional challenges such as attention problems in academic learning (Breslau et al., 2009), difficulties in social functioning (Fletcher et al., 2008), and diminished motivation (Breslau et al., 2011). Previous research has reported that adolescents with psychiatric disorders, compared to their peers without psychiatric disorders, have more negative educational outcomes including lower academic achievement, lower school attendance (Finning et al., 2019), higher risk of school dropout (Goulding et al., 2010; Quiroga et al., 2013), and higher risk of failing to graduate high school on time (Breslau et al., 2011).
The report by Merikangas et al. (2010) that 49.5% of U.S. adolescents aged 13–18 are estimated to have a mental disorder and 22.2% of them have severe impairment confirms the great need for mental health treatment in the adolescent population. Federal, state and local policymakers in the U.S. make efforts to increase access to school mental health services by expanding federal funding and leveraging Medicaid, the primary funding source for school mental health care for students from low-income families (U.S. Department of Education, 2022).
School mental health services have shown effectiveness in improving student outcomes, including reducing mental health problems (Sanchez et al., 2018), and improving school outcomes, such as disciplinary referrals and out-of-school suspensions (Bierman, 2002; Gray et al., 2017; Kang-Yi et al., 2013, 2018; Walter et al., 2011). However, only 42% of public schools (35,200 schools) in the U.S. provide mental health treatment to children with psychiatric disorders (National Center for Education Statistics, 2022).
School mental health care delivery and research on school mental health programs have predominantly focused on elementary and middle school aged children. There is limited evidence regarding the mental health services use of adolescents with psychiatric disorders in high school and the relationship between school mental health service use and mental health and educational outcomes in this population. Studies that examine these outcomes on a large scale could better inform local policymakers and practitioners who lead the current efforts focused on expanding school mental health service delivery.
To address this need, we conducted a longitudinal cohort study of adolescents with psychiatric disorders who transitioned from middle school to high school in a large urban school district in the U.S. In this district, more than three quarters of students are eligible for Medicaid based on family income. However, most adolescents enrolled in public high schools are not provided with mental health services funded through Medicaid in high school. Other than a few pilot programs in several high schools and mental health services provided for adolescents with autism and developmental disorders, school mental health services funded through Medicaid are not provided in high schools in the school district due to limited resources, shortage of school mental health service providers, and a local mental health care policy that primarily focuses on younger children.
To better understand the implications of school mental health service use at the transition to high school, we examined the relationship between school mental health services use, psychiatric hospitalization, and educational outcomes (i.e., school enrollment, school absences, out-of-school suspensions, school exits for negative reasons) of adolescents with psychiatric disorders. We compared the outcomes between adolescent groups by the status of school mental health services use during eighth grade and 2 years following.
Methods
Study Sample
The study sample included 2617 adolescents who were enrolled in eighth grade in public middle schools in an urban area in the northeast region of the U.S. All adolescents included in the study were enrolled in Medicaid throughout eighth grade and had a mental health diagnosis during the 2 years prior to eighth grade. Adolescents who were not enrolled in Medicaid during eighth grade were excluded. Adolescents who were not enrolled in a public school during eighth grade were also excluded.
Data Source
We used Medicaid behavioral health claims for school years 2008–2016 and school records for school years 2010–2016. This study was approved by the institutional review boards of appropriate parties including the University of Pennsylvania, the city’s public health department, and the school district.
Variables
Adolescents’ mental health diagnoses, mental health services use, and educational outcomes were identified. International Classification of Diseases (ICD-9 and ICD-10) codes corresponding to an anxiety disorder, mood disorder, attention deficit hyperactivity disorder (ADHD), conduct disorder/oppositional defiant disorder (Conduct/ODD), autism/developmental delay/intellectual disability (autism/DD/ID), adjustment disorder, substance use disorder, and other mental health diagnosis were used to identify mental health diagnoses. The primary or secondary mental health diagnoses found in the Medicaid behavioral health claims for 2 years prior to eighth grade were defined as baseline mental health diagnoses and recorded as binary variables (Yes vs. No). Overall, 41.7% of the study sample had multiple mental health diagnoses.
School mental health services use status was categorized into: used school mental health services during eighth grade and 2 years following eighth grade; used school mental health services during eighth grade and stopped using school mental health services 2 years following eighth grade; and never used school mental health service during eighth grade and 2 years following.
Mental health services use was measured as any community-based mental health service use (Yes vs. No). Community-based mental health service use was defined as using one or more of school mental health services, wraparound services, and outpatient therapy funded through Medicaid. One or more days of psychiatric hospitalization funded through Medicaid was coded as having psychiatric hospitalization.
Educational outcomes consisted of annual school enrollment status (Yes vs. No), annual number of days enrolled in school, annual percentage of unexcused absent days, annual number of days with out-of-school suspension, and school exit status. School enrollment status was recoded as “yes” if the adolescent had one or more days enrolled in school during each school year. The intention was to identify adolescents who were not enrolled in school at all. Students’ school exit status was used to identify how each student ended each school year. All students were expected to exit their school year with “school year end.” For students with multiple school exits noted during a school year, there were a variety of reasons for the exits (e.g., relocation within the school district, moved, disciplinary transfer). We computed a variable capturing school exists for negative reasons, which aggregated exits for the following reasons: disciplinary transfer, whereabouts unknown, placed in a juvenile residential facility, nonpublic school transfer, long-term hospitalization, exiting disciplinary school, child welfare involvement, alternative school, runaway, extenuating circumstances, overage school dropout, temporary expulsion, disciplinary hearing pending, school dropout, job corps, parental intervention, deceased, and placed in an adult incarceration facility.
Sex was recoded as female or male and race/ethnicity was recoded into African American, Hispanic, White, and Other.
Analysis
Statistical analyses were conducted using SAS 9.4. Descriptive statistics including means and percentages were conducted. Adolescents’ community-based mental health service use, psychiatric hospitalization, and educational outcomes were examined for 2 years following eighth grade. We used logistic regression models and generalized linear regression models to examine whether community-based mental health service use, psychiatric hospitalization, annual mean number of days enrolled in school, annual percentage of unexcused absent days during a school year, and annual mean number of days with out-of-school suspension significantly differed by status of school mental health service use in each school year, controlling for sex and race/ethnicity.
Results
Demographic Characteristics
Demographic characteristics and mental health diagnoses of adolescents by school mental health service use status.
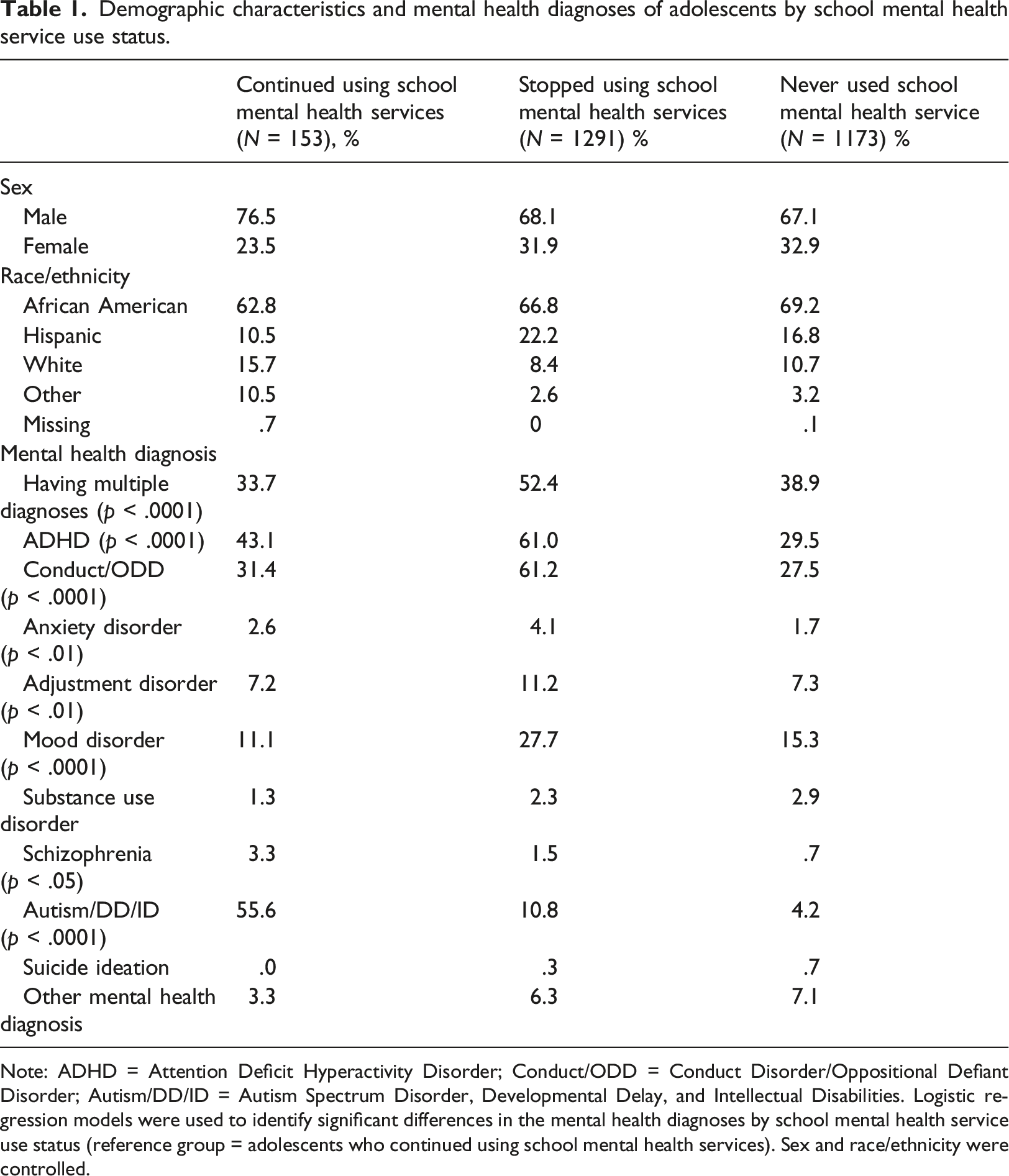
Note: ADHD = Attention Deficit Hyperactivity Disorder; Conduct/ODD = Conduct Disorder/Oppositional Defiant Disorder; Autism/DD/ID = Autism Spectrum Disorder, Developmental Delay, and Intellectual Disabilities. Logistic regression models were used to identify significant differences in the mental health diagnoses by school mental health service use status (reference group = adolescents who continued using school mental health services). Sex and race/ethnicity were controlled.
Mental Health Diagnoses
As shown in Table 1, the most common diagnosis among adolescents who continued using school mental health services was autism/DD/ID (55.6%). The most common diagnoses among those who stopped using school mental health services and those who never used school mental health service were ADHD (90.5% of the two groups) and conduct/ODD (88.7% of the two groups). The adolescents who stopped using school mental health services had the highest percentage of mood disorders (27.7%), compared to those who never used school mental health service (15.3%) and those who continued using school mental health services (11.1%, p < .0001).
The percentage of adolescents with substance use disorder was the highest among adolescents who never used school mental health service (2.9%) followed by those who stopped using school mental health services (2.3%) and those who continued using school mental health services (1.3%). The percentage of adolescents with suicide ideation was the highest among the adolescents who never used school mental health service (.7%). The percentage of adolescents with schizophrenia was the highest among adolescents who continued using school mental health services, followed by adolescents who stopped using school mental health services and adolescents who never used school mental health service (3.3%, 1.5%, and .7%, respectively at p < .05).
The percentage of adolescents with multiple mental health diagnoses was highest in the group of students who stopped using school mental health services (52.4%), followed by the group who never used school mental health service (38.9%) and the group who continued using school mental health services (33.7%); these differences were statistically significant (p < .0001).
Mental Health Services Use
Mental health service use and psychiatric hospitalization by school mental health service use status.
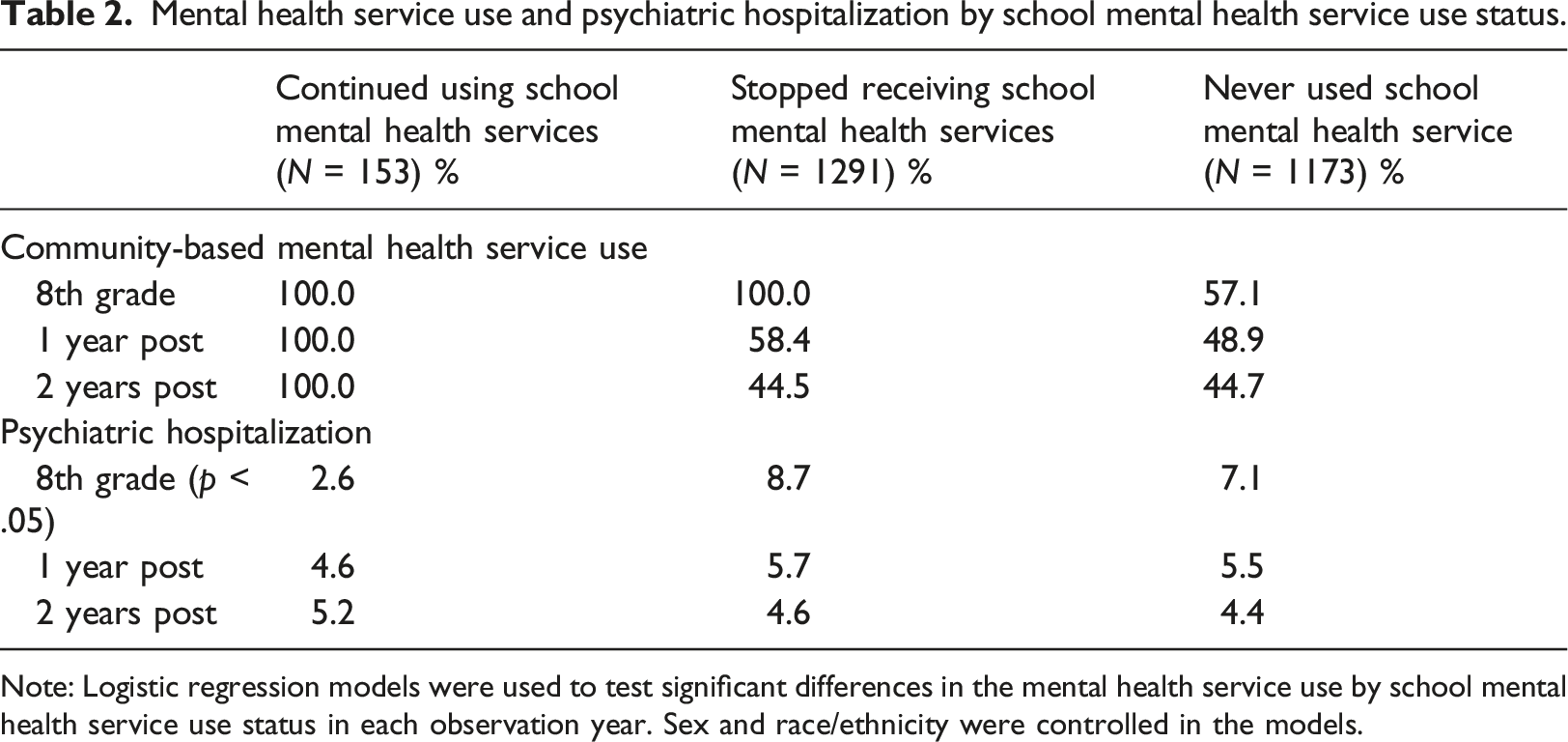
Note: Logistic regression models were used to test significant differences in the mental health service use by school mental health service use status in each observation year. Sex and race/ethnicity were controlled in the models.
The group of adolescents who stopped using school mental health services had the highest percentage of adolescents with psychiatric hospitalization in eighth grade, followed by adolescents who never used school mental health service and the adolescents who continued using school mental health services. The risk of psychiatric hospitalization significantly differed by the status of school mental health service use in eighth grade, but not for the 2 years following. Psychiatric hospitalization increased for adolescents who continued using school mental health services for the 2 years following eighth grade, while it decreased for the other groups. The risk of psychiatric hospitalization for the 2 years following did not significantly differ by the status of school mental health service use.
School Outcomes
School outcomes by school mental health service use status.
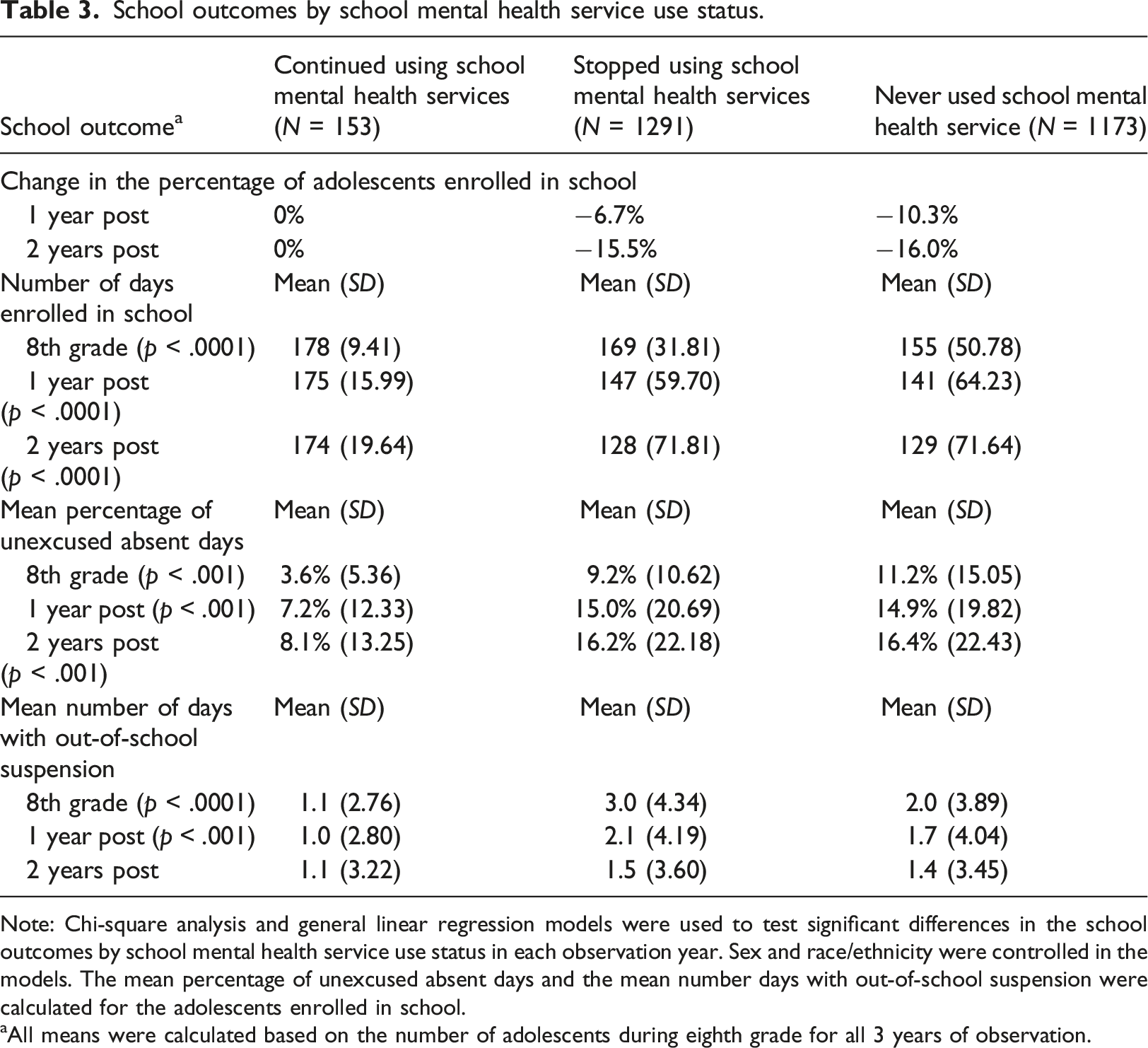
Note: Chi-square analysis and general linear regression models were used to test significant differences in the school outcomes by school mental health service use status in each observation year. Sex and race/ethnicity were controlled in the models. The mean percentage of unexcused absent days and the mean number days with out-of-school suspension were calculated for the adolescents enrolled in school.
aAll means were calculated based on the number of adolescents during eighth grade for all 3 years of observation.
Adolescents who stopped using school mental health services and adolescents who never used school mental health service had significantly higher annual mean percentages of unexcused absent days compared with adolescents who continued using school mental health services for the 2 years following eighth grade (p < .0001). The mean annual percentages of unexcused absent days increased among adolescents who stopped using school mental health services and adolescents who never used school mental health service (from 9.2% to 16.2% and from 11.2% to 16.4%, respectively 2 years after eighth grade).
The adolescents who continued using school mental health services had a significantly lower annual numbers of days with out-of-school suspension in eighth grade (p < .0001) and 1 year following (p < .001) compared with the other groups. The annual number of days with out-of-school suspension of adolescents who continued using school mental health services decreased from 1.1 days to 1.0 days and then increased to 1.1. The annual number of days with out-of-school suspension of adolescents who stopped using school mental health services decreased from 3.0 days to 1.5 days after 2 years. The number of days with out-of-school suspension decreased among adolescents who never used school mental health services from 2.0 days to 1.4 days after 2 years.
Compared with adolescents who continued using school mental health services, adolescents who stopped using school mental health services and adolescents who never used school mental health service had higher rates of exiting school for negative reasons such as school dropout with overage (a voluntary school dropout at age over 16), disciplinary issues, incarceration, long-term hospitalization, admission to juvenile residential facility, child welfare system involvement, and other extenuating circumstances. The percentages of adolescents who transferred within the school district were also higher among adolescents who stopped using school mental health services and adolescents who never used school mental health service for all 3 years compared to adolescents who continued using school mental health services.
Discussion
Overall, we found that more than half of the adolescents who stopped using school mental health services and the adolescents who never used school mental health service eventually stopped all mental health services use within the 2 years following eighth grade. This finding is alarming considering the added challenges adolescents with psychiatric disorders face in academic learning (Breslau et al., 2009), social functioning (Fletcher et al., 2008) and competence (Breslau et al., 2011). Information on why adolescents discontinued mental health services use post eighth grade was unavailable. This finding may reflect the fact that school mental health services were limited in high schools in the school district during the time studied here. Additionally, barriers such as stigma (Avenevoli et al., 2015), lack of time to get mental health treatment given the more rigorous academic curriculum and establishing relationships with new teachers and peers in a new environment (Langenkamp, 2010; Longobardi et al., 2016) in high school, and not finding appropriate mental health services may be some of the reasons for the cessation of mental health services use after transitioning to high school. Staying engaged in mental health treatment for adolescents with no access to school mental health services provided in their high school can be challenging due to rigorous academic schedule. Appropriate care planning and connection to community mental health services prior to the transition to high school is important for adolescents who transition to high school with no school mental health services available.
Adolescents with ASD/DD/ID tend to use school mental health services for the long-term given their need for day-to-day behavioral and learning support in school (Kang-Yi et al., 2016). This also may reflect the local context of mental health service delivery funded through Medicaid or policies that require schools to provide mental health services for children and adolescents with ASD/DD/ID.
The risk of psychiatric hospitalization was significantly lower among the adolescents who continued school mental health services use in eighth grade, but it increased among the adolescents for the 2 years following eighth grade. Given that most adolescents who continued using school mental health services had ASD/DD/ID, the finding may indicate that adolescents with ASD/ID/DD face greater risk of psychiatric hospitalization during their high school age. We did not have information about clinical symptoms and quality of school mental health care. Further research is important to identify factors associated with the increased risk of psychiatric hospitalization among adolescents who have ASD/ID/DD. Examining implementation of school mental health services is important to guide school staff and mental health professionals (Lyon & Bruns, 2019) and, ultimately, to help reduce psychiatric hospitalization among adolescents receiving school mental health.
Consistent with previous research findings (Kang-Yi et al., 2013, 2018; Walter et al., 2011), we found that using school mental health services in high school is associated with better educational outcomes including higher number of enrolled days in school, reduced unexcused school absences and lower number of days with out-of-school suspension. The findings suggest that school mental health services may play an important role in preventing negative educational outcomes for high school-aged adolescents with psychiatric disorders.
We found that the adolescents who stopped using school mental health services and the adolescents who never used school mental health service had higher rates of exiting their school for negative reasons such as school dropout with overage, disciplinary issues, incarceration, long-term hospitalization, admission to juvenile residential facility, child welfare system involvement, and extenuating circumstances. Adolescents with ADHD and comorbid ODD or conduct disorder have been reported to have higher rates of expulsion and dropouts from school (Atherton et al., 2020; Erskine et al., 2016; Sesso et al., 2020). Given that most adolescents who stopped using school mental health services and adolescents who never used school mental health service predominantly had ADHD and conduct/ODD, providing training on behavior management skills to schoolteachers and staff is important. Embedding effective interagency partnership between teachers and staff and mental health professionals (Cortina et al., 2019) can promote teachers’ behavior management skills, which is important for addressing the needs of this group of students, even if there is no mental health treatment available in high schools.
Our study has a few limitations. The study included adolescents enrolled in public schools with more than two-thirds of students qualified for free lunch. The interpretation of the study findings is limited to geographic areas with similar sociodemographic and urban public-school conditions. Our study did not test temporality of the relationship between overall mental health services use, psychiatric hospitalization and educational outcomes. Future research that examines temporality of the relationship of school mental health services use status and adolescent mental health outcomes will provide more rigorous evidence. The study was limited to examining school mental health funded through Medicaid. Studies that examine mental health and educational outcomes of adolescents who are enrolled in private health insurance may reveal different findings from our study findings.
Despite the limitations, our study reveals insights into school mental health service use and educational outcomes of adolescents with psychiatric disorders. Adolescents who continue using school mental health services in high school, compared to adolescents with psychiatric disorders who do not use school mental health services in high school, have more positive educational outcomes including better school enrollment, lower unexcused absences, and less school exits for negative reasons. Our findings support the positive role of Medicaid-funded school mental health care delivery in high schools in reducing negative educational outcomes for adolescents with psychiatric disorders. However, it is important to note that we found that the number of adolescents with psychiatric hospitalization 2 years after eighth grade was the highest among the adolescents who continued using school mental health services in high school. This finding may reflect the diagnostic severity for the group of students who continue to receive school mental health services and suggest that these services do not effectively prevent psychiatric hospitalizations.
Leveraging available resources such as Medicaid and mixed funding of mental health and education funding to provide seamless mental health care during the transition from middle school to high school has the potential to improve adolescents’ mental health and educational outcomes. Generating further evidence through empirical research to inform policymakers and practitioners of effective mental health care delivery in high schools should precede the expansion of school mental health services. More specifically, investigating the reasons why adolescents discontinue all mental health service use post eighth grade despite their Medicaid eligibility can lead to concrete direction for improving mental health care delivery for adolescents. Future research should also expand the observation period to all high school years in order to more meaningfully investigate the longitudinal trajectory of school mental health service use and educational outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported in part by Philadelphia’s Department of Behavioral Health and Intellectual disAbility Services. The findings and conclusions presented in this paper are those of the authors and do not necessarily represent the views of the Department of Behavioral Health and disAbility Services.