
Abstract
Background
Qualitative research has explored how some testicular cancer survivors (TCS) experience the psychological impacts of diagnosis and treatment. More research into the impacts of testicular cancer (TC) on adolescent and young adults (AYA) is needed due to the critical period of identity development. The present study aimed to explore how AYA with TC appraise and make sense of their experience and to develop a greater understanding of psychosexual identity development in AYA TCS.
Method
Eight AYA TCS were interviewed. The results were analysed using Interpretative Phenomenological Analysis. The questions explored the experiences relating to diagnosis and treatment, how it affected their psychosexual identity development (e.g., sexual relationships and self-image) and the meanings attached to the experiences.
Analysis
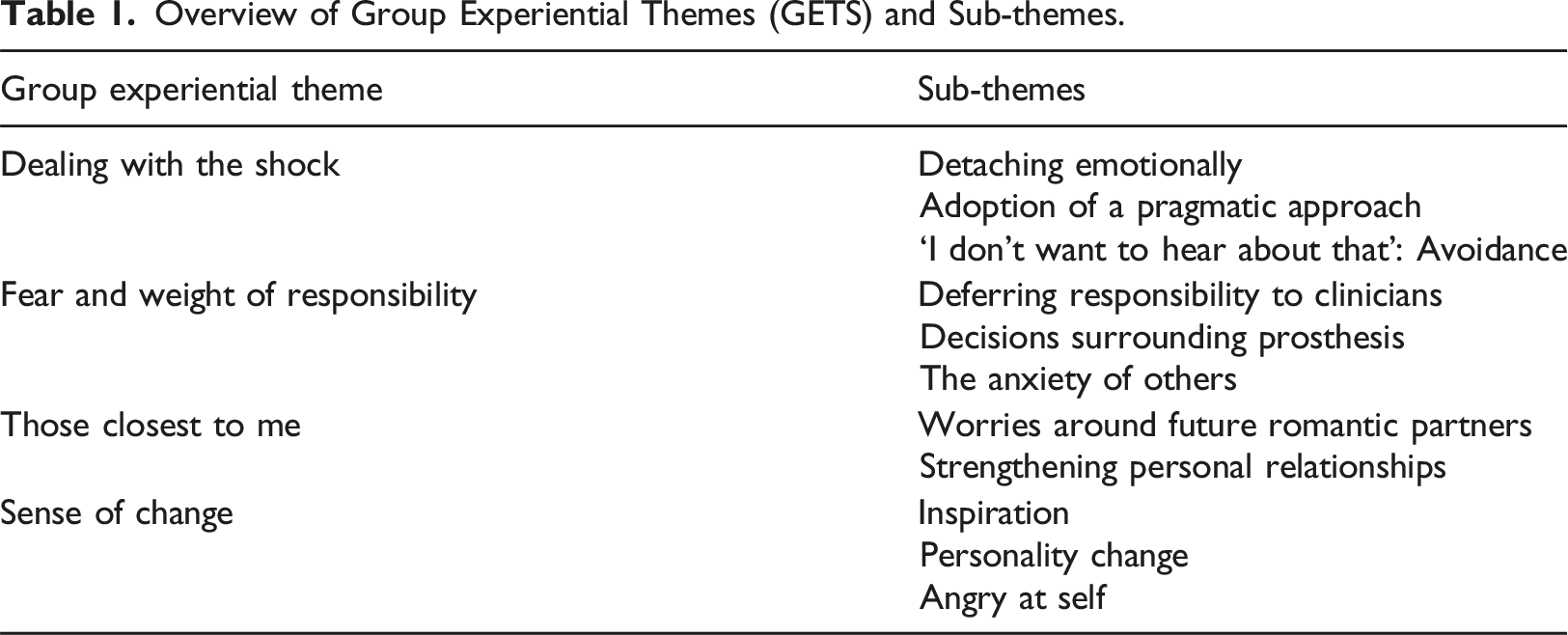
Four Group Experiential Themes were developed from the data; ‘Dealing with the shock’, ‘Fear and weight of responsibility’, ‘those closest to me’ and ‘sense of change’.
Discussion
The AYA TCS experiences may result in adoption of traditional masculine traits (e.g., stoicism) or abandonment of traditionally masculine traits (E.g. violence and aggression). AYA TCS also described feelings of insecurity when compared to other men. Psychology input could help manage stoicism and feelings of inferiority when compared to men with two testicles.
Plain language summary
Background
Qualitative research has explored how some testicular cancer survivors (TCS) cope with the psychological impacts of diagnosis and treatment. However, there is a need for more research on the effects of testicular cancer (TC) specifically in adolescent and young adults (AYA), given the critical period of identity development during this stage. The present study aimed to explore how AYA with TC perceive and make sense of their experiences, with a focus on psychosexual identity development.
Method
Eight AYA TCS were interviewed, and their responses were analyzed using Interpretative Phenomenological Analysis. The interviews covered topics related to diagnosis, treatment, and how these experiences influenced their psychosexual identity (including sexual relationships and self-image).
Analysis
Four main themes emerged from the data: “Dealing with the shock”: Participants discussed their initial reactions to the diagnosis. “Fear and weight of responsibility”: AYA TCS grappled with fear and the burden of managing their health. “Those closest to me”: Relationships with family and friends played a significant role in their experiences. “Sense of change”: Participants described how their cancer journey impacted their sense of self.
Discussion
AYA TCS may either adopt traditional masculine traits (such as stoicism) or abandon them (e.g., violence and aggression). Additionally, they expressed feelings of insecurity when comparing themselves to other men. Psychology support could help manage stoicism and address feelings of inferiority when compared to men with two testicles.
Scott et al. (2020), found that testicular cancer (TC) was the most common cancer diagnosis in adolescent and young adult (AYA) with testicles. Between 2016-2018, TC was the most prevalent form of cancer in AYAs aged between 16-24 (Cancer Research UK, 2015). Current medical treatments for TC are centred around three approaches: orchidectomy, (removal of a testicle), chemotherapy and radiotherapy. AYA’s are at a critical period of identity development, involving the development of a sexual-self (Biro & Dorn, 2005), starting sexual relationships (Collins & Sroufe, 1999) and general physical sexual maturity. The onset of puberty comes with various anxieties, including self-image (Ofer et al., 2013). Diagnosis and treatment of TC may add further complications as it can give rise to negative self-judgment of appearance and reduced sexual functioning – with the effects continuing years after recovery. Treatment involving orchidectomy may impact the individual, regardless of their age or physical health (Skoogh et al., 2011) especially AYA patients undergoing puberty. Qualitative research has described how some testicular cancer survivors (TCS) experience the psychological impacts of diagnosis and treatment. This includes sexual difficulties including communicating with sexual partners and asserting oneself sexually and fear of judgment from others (Dobinson et al., 2016). Carpentier et al., (2011) found TCS perceive their own bodies to be ‘damaged’ following treatment although Fleer (2006) found TCS were not more vulnerable to impaired quality of life.
Current psychological treatment recommendations focus on improving peer support and maintaining the AYA’s sense of identity (e.g., Park & Rosenstein, 2015). However, other challenges may go unaddressed with current approaches. Dobinson et al. (2016) developed a grounded theory of the psychosexual needs of TCS aged between 15–35 and found that several needs went unmet.These include gender identity (or self-perceived gender), sexual functioning, relationship support and sexuality, specifically regarding age incongruity between their self-perceived and chronological age, changes in intimate relationships, disclosure to others and reconciling identity conflict. Dobinson et al., 2016). Gender has been described as socially and psychologically constructed and involves understanding societal roles, characteristics, behaviours, and the social norms regarded as ‘suitable’ for the determined gender (Ryan, 2007). This suggests that the development of conceptual gender is complex, with previous notions of binary gendered development deemed outdated (Hanssen, 2017). It is yet unclear if TC has an impact on gender development, particularly when diagnosed as an AYA.
Masculine Identity development can begin during adolescence and change throughout the lifetime as the body changes (Connell, 2001). Research has shown the importance of the physical body when constructing a sense of masculinity during adolescence (Mora, 2012), therefore any changes to the body during this time may also impact one’s sense of masculinity. Following orchidectomy, sex-role and quality of life can remain intact, however the loss of sexual function was reported to be psychologically distressing (Marilyn et al., (1995)). This suggests a sense of masculinity may still be impacted through diagnosis and treatment of TC, but unrelated to physical alterations in the body. More recent research has emphasised the importance of close interpersonal relationships in shaping an AYA’s sense of masculinity (Rogers et al., 2021). The researchers suggest that the physical body may provide an indirect influence on one’s sense of masculinity, particularly where AYA’s who are smaller in frame may struggle more with their sense of identity development.
Pappas (2019) described a ‘harmful’ construct of ‘traditional’ masculinity as including dominance, aggression, competitiveness and stoicism, potentially relating to bigoted views and behaviours, such as misogynistic or harassing (De Boise, 2019). In contrast Pleck et al., (1993) suggested a more ‘general’ culturally specific masculine construct is defined by how much individuals endorse and internalise cultural expectations on masculinity – thus, unbound by specific criterion.
There are also societal/environmental contributors to one’s sense of psychosexual identity development, particularly when features such as a disposition to engage in ‘high risk’ activities that may result in injury are higher in those who hold a masculine identity that is more ‘traditional’ (Javouhey et al., 2006). As AYA’s are found to be more likely than other age groups to engage in high-risk behaviours (Spring et al., 2012), this provides another example of how psychosexual development of AYAs may be prone to influence from societal factors.
There is a lack of understanding and sense making of the lived experience of AYA TCS. Whilst some recommendations involve more education on sexuality issues (e.g., (Moore et al., 2013), he lack of research detailing psychological needs is apparent. Kelly (2013) recommended an increased awareness in addressing age-appropriate psychosexual support age especially as testicular cancer and its treatments impact biological factors and the individual’s sense of identity and sexuality. The present study aimed to gain an in-depth understanding of how AYA with TC appraise and make sense of their experience and to develop a greater understanding of psychosexual identity development in AYA TCS. This includes how they make sense of their diagnosis, treatments, and other impacts such as with close and romantic relationships.
Method
Design
The study used a qualitative design involving an interpretative phenomenological analysis (IPA) (Smith et al., 2009) of semi structured interviews.
IPA aims to observe individuals’ experiences and perceptions relating to often transformative events - in this instance, diagnosis and treatment of TC. This research aimed to explore the experiences and meaning making of a homogenous sample of TCS. IPA also adopts a ‘double hermeneutic’ process (Smith et al., 2009) whereby the researcher’s role in interpretation of the participant’s experience is considered within the research itself. Following the TCS’ interpretation of their experience, the researcher’s interpretation of the TCS account occurs.
Interview schedule
An expert by experience (EBE) was consulted in this project. The EBE was an AYA TCS and represented the type of participants recruited in the research, thus their involvement was essential to ensure the research robustness. The EBE was involved in the construction of the interview schedule and in checking the credibility of the analysis by the lead researcher (Smith et al., 2022). The EBE’s involvement with the interview schedule included adapting questions to provide a richer, more accurate account of the TCS experience. The questions were designed to help the TCS explore their experiences relating to the meanings surrounding diagnosis, impacts on self, relationships, sexual difficulties relating to communication and experience, the development of the sexual self and masculinity development. This includes support offered/not offered (including prosthetics), recalled conversations with professionals and possible changes to the sense of self following the experience. These are explored through open-ended questions, influenced by current research findings described in the introduction.
Recruitment
Eight participants were purposively sampled from a London NHS teaching hospital Adolescent Oncology department. Their consultant assessed and verified the potential participants capacity to consent prior to their details being forwarded to the lead researcher.
Inclusion criteria
The AYA TCS all met the following inclusion criteria: • Aged between 16-25 • Diagnosed with testicular cancer between the ages of 14 and 19 • Diagnosed and treated in the UK • Completed treatment for testicular cancer • Their participation in the interview could be facilitated without an interpreter.
Participants
Smaller sample sizes are suggested for IPA due to the qualitative nature of the research (Smith et al., 2009). IPA recommendations for sample size (Pietkiewicz & Smith, 2014) and the requirements for doctoral level research led to an a-priori recruitment target of 8 participants. IPA utilised homogenous samples to determine common themes, providing a rich analysis of the experiences more valid results regarding the research aims (Pietkiewicz & Smith, 2014).
All participants were unpartnered at the time of interview and described ‘extensive’ familial involvement in their treatment and support both during and post-treatment. They all described developing an expertise on TC diagnosis and treatment following their own diagnosis – which was not present prior to their experience.
Procedure
Following the participant expressing an interest, a Zoom appointment was arranged. Between the initial contact and the arranged appointment, participants could read the emailed information sheet and sign the consent form. Participants could also ask questions during the appointment (before the interview). The recorded semi-structured interview took place over Zoom in a location where the participant (and researcher) could speak privately for up to 60 minutes. The interview length ranged between 25 – 60 minutes depending on the responses to questions, speed of speech and level of detail the participant could divulge. All participants disclosed feeling happy to take part and engaged seemingly without distress.
Data analysis
The data analysis was structured utilising Smith et al.’s (2022) recommendations. Interviews were transcribed by the lead researcher following completion, who then immersed themselves in the transcript through reading whilst simultaneously listening to the audio. Transcripts were read twice in this manner before Exploratory Notes (EN) were made, which were descriptive, linguistic or more analytical initial interpretations. ENs were then grouped according to connections identified by the lead researcher. These formed Experiential Statements (ES), or concepts more relevant to psychological constructs (Smith et al., 2022). This was done individually for all transcripts, developing ‘Personal Experiential Themes’ (PET) from the ES. The researcher then determined Group Experiential Themes (GET) that seemed to apply to the AYA TCS, along with the subthemes that are encompassed by the GET (Smith et al., 2022). Some PETs were regrouped, reconceptualised, or left out so that the analysis could capture as broad a picture of the experience.
Ethical considerations
The study was approved on: • 16/09/2020 by Salomons Institute Independent Research Review Panel ( • 19/04/2021 by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) ( • 13/04/2022 by the University College London Hospital (UCLH) Research and Development (RAND) (
All participants provided informed consent to taking part in the interview and having the interview audio recorded for transcription purposes.
Results
Overview of Group Experiential Themes (GETS) and Sub-themes.
Dealing with the shock
There was an impression that aspects of the participants experience were shocking. Although some participants described already ‘knowing’ about their diagnosis before medical confirmation, many still described feeling stressed about what could happen.
Detaching emotionally
Participants described either ignoring or ‘switching off’ emotions during initial diagnosis to help manage the shock. There was a sense that this may have helped facilitate daily activities or a return to ‘normality’: ‘I just ignored my emotions and carried on with my day to day…’ (Derek)
There seemed to be a sense that feeling these emotions was not an option. David expressed a pull towards thinking emotionally, but an awareness that this may have inhibited his ability to consider his prognosis: ‘I think for me it would have made me think too much about the emotional side of things and that meant I wouldn't have thought straight about the treatments and the solutions…’ (David)
Adoption of pragmatic approach
Most participants appeared to focus on treatments, solutions and recovery throughout their experience. This seemed related to treatment decisions and shifted focus away from worrying, or other emotions. ‘I just wanted to get on with my life, I just focussed on beating it and then ended up coming out the other side winning.’ (Roger)
Roger seemed to describe how a pragmatic approach helped regain a sense of normality in his life, and a sense of a causal relationship between thinking pragmatically and overcoming TC. This is echoed by David, who seemed to describe how a pragmatic approach, helped the situation gain clarity and thus, alleviate some of the shock and stress. ‘…there's no point breaking down and being all emotional about it, this is the situation - you move on, you think about the solution.’ (David)
There was also a sense of downplaying the severity of TC, which may have been a result of emotional suppression and the adoption of a pragmatic approach offsetting the shock and stress. ‘I don’t want to hear about that’
Some participants would actively avoid various aspects of their experience at the time, in particular disclosure to others, seemingly to simulate a return to normality. ‘I would just go out with my friends and chill. They wouldn't know anything, but I just acted like things were completely normal and would just chill.’ (Henry)
Henry’s friends seemed to represent normality, and thus a longing to return to this. It seemed that Henry was able to relax with his friends, and their ignorance to his situation may have helped to temporarily avoid the shock and stress associated with it.
At other times, Henry seemed to avoid the use of certain words, such as ‘sperm’. ‘My productivity as well. It was reduced, but that's why I had to do the banking…. but it did reduce but not massively. But it was still enough.’ (Henry)
This may have suggested that the shock of his situation was driving some behaviours. In short, the shock was unavoidable, but what could be avoided was perpetuators or reminders of reality. Avoidance of reality may serve to provide short term relief, as Henry described before he had received diagnosis. ‘Well, it ended up going massive... I randomly saw one of them was large… So, I was very, very embarrassed about it. And I thought, nah, this isn't right. But I didn't speak out on that. I just let it be and I kept to myself. And they go larger and larger and painful....’ (Henry)
Henry not only avoided seeking help when he noticed something was wrong, he also avoided using the word ‘testicle’ whilst recounting his experience. It seems the avoidance, possibly like the pragmatic adoption, may persist after treatment has ended.
A consequence of the avoidance may also be that some participants’ reality is impacted, such as with David who described a difficulty in saying the word ‘cancer’. ‘Since telling people I have found it quite hard to say the word cancer … and because I physically can't say the word…’ (David)
It seemed David was unsure as to why he was unable to say the word, describing his difficulty as more than psychological but also a physical inability that is outside of his awareness.
Fear and weight of responsibility
Participants often described a fear of certain responsibilities during their experience. This ranged from an awareness of their own intellectual limitations surrounding treatment decisions, to even whom to disclose to.
Deferring responsibility to clinicians
Some participants seemed to rely on the clinicians when it came to making the best treatment decisions. There was a sense of complacency, almost a submission to the will of another. ‘It was very much ‘we will go with whatever the consultant thinks is the best option for my health’ going forward.’ (David)
David seemed to acknowledge that the situation was willingly out of his control, and that he had relied on the consultant to make the best choices in his interest. Others seemed to feel clinicians were responsible for whether the participant needed psychological support. ‘I’m pretty sure she could tell I wasn’t in psychological distress or anything… So maybe that’s why they decided not to - you know - refer me to a therapist.’ (Mish)
There was also a sense of uncertainty over some of the clinical decisions. Mish described an idea as to why he was not referred for psychological input but was uncertain. Nevertheless, he described an attempt to make sense of the consultant’s (“she”) decision, even after deferring responsibility.
Decisions surrounding prosthesis
Some participants felt that the responsibility over whether to have a prosthetic implanted remained with others, even if this contrasted the participant’s desire. ‘No, I didn't have a choice. My parents were the main choosers because I was 15…I would want a fake one actually. Why not? Actually, if I was given the chance, I would have one.’ (Richter)
Richter described how his parents held responsibility around choosing whether to have a prosthetic implanted. He alludes to his age when discussing why he did not get a choice, but there is also a sense of regret over the decision his parents had made for him. This is also echoed by Henry: ‘But the basis on why I wanted the prosthetic. Is basically because I'm very insecure… I just wasn't offered the prosthetic at the time’
Henry seems to describe decisions surrounding prosthesis remaining with clinicians, however this responsibility was not deferred from Henry. Henry expressed wanting the prosthesis at the time, feeling it would help manage his distress, but he was not offered it.
The anxiety of others
Although responsibility has been discussed in relation to others, the participants all seemed to experience the weight of feeling responsible for the emotional experience of close others. This involved a sense of feeling a causal relationship to how others feel, and a sense of taking on a reassuring role to others, which at times seemed burdensome. ‘Even though I knew I was going to be fine, they weren’t really emotionally there… they were really distressed by it, and I was more supporting them, and they did support me but at certain times’ (Mish)
Mish seemed to be describing an awareness of the situation, but that others (in this instance, his parents) were ‘not there’. There was a sense of differing levels of awareness, and thus the role of support was adopted by Mish to get his parents to where he was emotionally.
However, some participants described experiencing positive benefits to taking on a reassuring role. ‘…but it was nice telling people and reassuring them, it felt ok but as a whole.’ (Andrew)
It seems Andrew did not feel the same as Nish, however the reference of ‘as a whole’ creates a sense that ultimately it was pleasant, but there were aspects of the role that may have been burdensome. There is a sense of the ends justifying the means.
Those closest to me
This GET included relationship changes or perceived difficulties in the future and the surrounding impacts.
Worries around future romantic partners
Some participants felt that their experience suggested that they were inferior to other men in the eyes of others, with particular focus on future sexual partners. ‘Well, there are other boys out there with two testicles, so why would anyone want me with only one?’ (Richter)
Richter seems to be alluding to a sense of inferiority. The fact that he has one testicle suggested less desirability compared to others with two testicles. Richter seemed to conclude that another person would prefer someone ‘better.’ This is exacerbated when Richter describes feeling inferior to other men: ‘I feel different to everyone else now. I feel like I'm cut in half.’
Having one testicle seemed to be understood by Richter as meaning he is half as valuable. There is also a sense of feeling alone in this, as he references ‘everyone else’. This sense of abnormality is shared in other participants, with a perception that they are no longer ‘normal.’ ‘A lot more awkward, definitely… But it's just the awkwardness of how you're not normal, basically.’ (Henry)
Strengthening personal relationships
Participants also described a strengthening of relationships that they perceived were ‘close’ prior to their experience. This strengthening also related to familial relationships with one-another (i.e., not towards the participant). ‘It brought all sides of my family together, even if they didn’t like each other, because they all wanted to be there for me and help me no matter what.’ (Roger)
There seemed a sense of reparation of relationships in Roger’s account, describing a unification of all those with the same goal. This is echoed by Andrew: ‘These are friends that I still am in touch with to this day of course these are lifelong connections’
Andrew seemed to allude to a strengthening of already present relationships, and a desire to maintain these interactions in the long term.
Sense of change
All participants described feeling changed or at a stage of transformation. This ranged from positive, negative changes, and some shifts in personality.
Inspiration
A few participants described how their experience of diagnosis and treatment contributed to their desire to work in medically related fields. One described how the experience had contributed to their sense of purpose to become a doctor. ‘I want to get into medicine as well so … I was someone who had a story now, who had a much stronger defined purpose, and this is something that really did impact my self-respect’ (Andrew)
Andrew seemed to describe drawing inspiration from his experience. The sense of transformation comes from this idea that he was ‘someone who had a story now’. The inspiration is echoed in other participants, including David who described associating his experience with his career choice: ‘If I didn't have it I maybe I wouldn't be a doctor today’
It seems David’s understanding of his experience was that it provided the inspiration to pursue a medical career, and a perception that without the experience he may have been in a separate career.
Personality change
A few participants described a shift in personality following their experience. This particularly surrounded maturing emotionally. ‘I used to get in lots of fights as well, and after that I completely changed. I haven’t gotten into a fight ever since then’ (Mish)
Mish seemed to describe a change in aggression and temperament following their experience. This change of getting into lots of fights to suddenly none has an absolute quality to it, in that Mish understands that a part of him has changed ‘completely’. This is echoed in Roger’s interview: ‘I was just, always being disrespectful and like, being a rude person to parents and siblings, and like, just being very aggressive and everything… Yeah it’s changed a lot’ (Roger)
Roger appears to attribute his reduction in aggression to his experience also. There is a sense of identity change, as Roger referred to himself as ‘a rude person’ prior to his TC experience. Both these accounts allude to a partial transformation, with Mish later detailing more about the change: ‘And it definitely helped me mature a lot… the next year when I went on holiday they were like ‘who are you? Where’s MISH gone?’ (Mish)
It seems Mish associates his experience with a change in personality so drastic, that he became unrecognisable.
Angry at self
Many participants described a sense of feeling angry at themselves for their diagnosis. This contrasts with the positive transformations described above, but instead seemed to focus on feelings of blame and shame. ‘I used to drink a lot of Fanta… After being diagnosed, I just quit Fanta altogether. In the way I blamed Fanta, fizzy drinks in general.’ (Derek)
It seemed that Derek understood soft drinks (Fanta in particular) as being responsible for his TC. This suggests that Derek made sense of his diagnosis because of his lifestyle choices, and the abandoning of soft drinks in this instance seemed to represent a desire to never return to the experience. In some participants, this anger is turned inwardly: ‘…they supported me in the way to try and make me feel more realistic, because sometimes I hate myself over this...’ (Richter)
Richter seemed to hate himself over the fact he was diagnosed and treated for TC. This anger aimed inwardly appeared to be managed using others, suggesting a self-soothing approach would be fruitless. The sense of blaming himself is acknowledged as being ‘unrealistic,’ however Richter described an awareness of this and a sense that the anger is still aimed inwardly.
Discussion
Participants dealt with the initial shock of a diagnosis by detaching emotionally and adopting a pragmatic approach. They interpreted felt emotions as ‘inhibitory’ to their physical recovery and were anxious that their shock and stress could impair their ability to manage the situation, potentially resulting in the deferral of treatment responsibility to the medical teams. Recent research has shown that the deferral of treatment decisions is prevalent in adult prostate-cancer patients (Pan et al., 2022). Traetta and Doronzo (2022) have suggested suppression of distressing emotions acts as a mechanism to defend against the trauma of a cancer diagnosis and the associated stigma. However emotional detachment and pragmatic adoption may have also served other purposes whereby avoidance of expressing emotion in front of close others aims to preserve relationships. (Arteaga Perez, 2022). Participants in this study adopted a reassuring role to others with a strengthening of personal relationships. These mechanisms may serve an emotional regulation purpose whereby a pragmatic approach acts as short-term emotional management, postponing emotions until they have overcome the treatment (Palmieri et al., (2022); Wilkinson et al., (2011)).
The findings of this research support Marilyn et al. (1995) with varying degrees of sexual impact reported following diagnosis and treatment. This included feeling insecure and inferior to men with two testicles, whilst others described no negative sexual impacts. Some reported temporary reduced sexual interest following orchidectomy but seemed able to contextualise this as they were undergoing chemotherapy at the time, potentially reducing the negative impact of this change.
No participants mentioned concerns surrounding masculinity however, Mish and Roger described a shift away from characteristics associated with ‘traditional’ masculinity (reduced aggression and violent behaviours). This suggests that their experience facilitated a shift away from more harmful views of masculinity, possibly reducing their endorsement and internalisation of the belief that this is what masculinity involved. The cessation of ‘high risk’ activities associated with the masculine identity (Javouhey et al., 2006) may also suggest TC contributed to the development of a less ‘harmful’ masculine identity.
Various participants may have displayed ‘stoicism’ through their emotional detachment. This may suggest that TC indirectly facilitated their adoption of these harmful characteristics, thus the adoption of more ‘traditional’ masculinity. However, stoicism may have been adopted functionally to protect from the emotional impact of diagnosis and treatment (Vaillant, 1976).
These results are in line with Connell and Connell (2000) and Mora (2012) as the physical body displayed importance when constructing a sense of masculinity during adolescence. However, it is yet unclear if this is directly related to the body change through orchidectomy, as not all participants described adopting ‘traditional’ masculinity traits.
Several participants who did not receive a prosthesis described a sense of inferiority when compared to other men with two testicles. This suggests that accepting a prosthesis may manage the developmental challenges of these AYA TCS. This is particularly important for the AYA TCS interviewed whom described feeling different to others or no longer ‘normal.’ TCS similarly described feeling like ‘damaged goods’ in previous research (Carpentier et al., 2011). These concerns appeared to contribute to anxiety surrounding perception from romantic partners and a desire to conceal their ‘missing testicle.’ This insecurity surrounding their bodies and perception from others contributed to their anxiety surrounding future romantic relationships and to the anger they felt at themselves.
No participants engaged in psychological support. Some said it was unnecessary or was not offered by medical staff – believing that medical staff felt the AYA was ‘mentally fine’. Others felt this was due to an inability to relate to others who were not AYA TCS. This may also be explained by the adoption of a ‘stoic’ attitude, possibly influenced by medical staff through a lack of offering psychological support, which has been shown to have an impact on stoic attitudes (McAteer & Gillanders, 2019).
Many participants described positive familial and close-other support at the time of diagnosis and treatment. All described a strengthening of close relationships, a sense of close family connection following diagnosis and treatment, and described immediate family as key support mechanisms. This supports Rogers et al., (2021) as close interpersonal relationships may contribute to shaping the AYA’s sense of masculinity. Some participants were possibly influenced by family, whom through their own distress did not desire to speak about the experience with the participant, thus influencing the adoption of a stoic attitude.
Strengths and Limitations
A strength of this research is the time taken to create and verify the interview schedule with the EBE, which resulted in research with more ecological validity. The British Psychological Society stresses the importance of expertise when carrying out qualitative research, emphasising that this improves the quality of the research and findings (BPS, 2022).
The present research met the four quality indicators of good IPA; 1. “Constructing a compelling, unfolding narrative” as the analysis creates a clear narrative formed from specific extracts from participant interviews. 2. “Developing a vigorous experiential account” 3. “Close analytic reading of the participants’ words” meet good criteria as an in-depth analysis around the meanings of participants’ accounts occurs in depth, based on specific quoted accounts. 4. “Attending to convergence and Divergence” as the quotes, meanings and experiences are commonly connected between different participant accounts (Nizza et al., 2021).
Considering the above criteria, it could also be argued that the present research attained ‘saturation’ (Saunders et al., 2018) as further analysis may not provide new and unaccounted themes.
A limitation of the present research in that the participants were recruited from one NHS centre and all participants held positive experiences of their interactions. It is possible that participants who did not have as positive an engagement or from other centres may have experienced more impairments in their psychosexual development.
Participants may have spoken positively of their experience through a sense of demand characteristics – or a belief that the lead researcher worked within the NHS centre and did not feel able to directly criticise their experience of care.
Clinical implications
NICE guidelines (2004) recommend psychological input based on the level of distress experienced by cancer patients, however this study identified other facets that may warrant input, such as the adoption of stoicism or the inability to say some words. The same guidelines acknowledge that psychological symptoms are often missed by medical staff, resulting in patients who may benefit from psychology input missing out. A recommendation is that psychologists can be more readily involved in identifying the adoption of concerning traits, such as stoicism, and provide an opportunity to discuss decisions being made on their behalf – to manage any potential distress.
Another clinical implication is how information about the prosthesis is communicated to the participant. Considering the presence of the prosthesis may impact the AYA TCS psychosexual development, this would suggest that medical teams discussing this treatment option can consider the potential benefits related to self-image and reassurance, especially considering the high levels of satisfaction with the prosthesis reported by TCS (Dieckmann et al., 2015). As some clinicians’ perspectives on prosthesis seemed key in the participants decisions around prosthesis, and that trust in the clinicians appears particularly high during this vulnerable period of the AYA TCS (and close others) life.
Implications for future research
The present research provides an initial step towards understanding the psychosexual identity development in AYA TCS. Future research could seek to establish clinicians’ perceptions of the various aspects of AYA TC diagnosis and treatment.
Future research could explore cultural differences in the development of psychosexual identity within this population. As previous research has shown masculine identity is heavily culture bound (e.g., Pleck et al., 1993), there may be key differences depending on cultural background.
Future research may also explore the adoption of stoicism in other cancer survivors, such as teenage cervical cancer survivors to explore gender differences. This would explore whether attributes associated with masculinity (e.g., stoicism) may equally apply to non-males.
Conclusion
This study demonstrated the influence of TC on psychosexual identity development in AYA TCS. The findings were consistent with previous literature, illustrating that masculine development may be contributed to by close relations and may be irrespective of physical changes to the body. The initial shock of diagnosis may contribute to adoption of harmful ‘traditional’ masculine traits, such as stoicism, which may manage the initial distress. This distress may be unresolved, potentially evidenced by the avoidance of verbalising words associated with testicles. The weight of responsibility can be difficult for AYA patients to manage, thus deferring responsibility surrounding treatment and prosthesis to clinicians and close others. These close others also seem to actively reassured by the AYA TCS throughout their experience. The experience may also strengthen close relationships, but creates anxiety surrounding future romantic partners – particularly in those who did not receive a prosthesis. Nonetheless, TC provided inspiration to some AYA to pursue medical careers or shifted their personalities away from ‘traditional’ masculine traits of violence and aggression. This study suggests that psychological input may help facilitate AYA TCS away from ‘traditional’ masculine traits and thus aid in their psychosexual identity development.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Dr
Dr
Dr
Dr