
Abstract
Objectives
Research has highlighted poorer experiences of cancer care amongst ethnically minoritised groups. Whilst significant strides have been made in understanding cancer experiences of minoritised adults, there exists a knowledge gap in understanding how cancer impacts on minoritised young people, many of whom are faced with complex developmental challenges. This study aimed to understand the experiences of cancer and cancer care amongst minoritised youths in the UK.
Method
Nine young people aged between 16 to 24 with diverse types of cancer diagnoses, who self-identified as ethnically minoritised shared their cancer experiences in semi-structured interviews. Participants’ stories were analysed using thematic narrative analysis.
Results
Findings identified three core narratives reflecting participants’ emotional journey through cancer, their cultural stories and cancer care experiences, encompassing 12 themes. Their journeys shared common themes of: Feeling Dismissed; Shock and Turmoil; Grieving Self and Changes; Isolated and Helpless; Adapting in Adversity; and “Changed for the better”. Cultural narratives revealed diverging views towards family support, while cultural influences on treatment options and feelings of being othered also complicated their cancer experiences. Overall, participants shared positive experiences of cancer care. Despite a protracted journey to diagnosis, personalised, accessible care and experiences of feeling seen were valued.
Conclusion
The findings shed light on cultural influences towards minoritised young people’s experiences of cancer and care. Implications around strengthening cultural sensitivity and visibility were highlighted. Future research may be helpful to hone into minoritised cancer experiences at different stages during one’s cancer journey including survivorship across more diverse socio-cultural contexts and how systemic factors may impact on the provision of culturally competent care.
Plain Language Summary
This study explored ethnically minoritised young people’s experiences of cancer and cancer care. Nine participants were invited to share stories of their cancer journey, which were analysed using thematic narrative analysis. The themes showed the difficulties and loneliness that minoritised young people faced as cancer changed their lives and the way they saw themselves. Cultural stories described how conflicts within families, cultural beliefs about treatment and feeling othered impacted on their experiences. Young people shared positive stories of their cancer care, but some felt frustrated by perceived discrimination, a lack of cancer awareness and cultural insensitivity, which led to delayed diagnosis. Future research and important points for improving clinical practice were identified.
Keywords
Introduction
Cancer health disparities across ethnic groups have been widely documented, prompting a closer examination into the intersectionality between cancer and ethnicity (Delon et al., 2022). Low awareness of cancer symptoms, low participation in clinical trials and delayed help-seeking behaviours were more likely to be observed in ethnically minoritised groups (Waller et al., 2009). UK national studies have highlighted lower satisfaction and poorer care experiences reported by minoritised cancer patients (Pinder et al., 2016). In particular, non-White and younger patients consistently reported inferior quality of care compared to older adults (Bone et al., 2014; Furness et al., 2017). It therefore seems unsurprising that higher levels of mistrust towards healthcare professionals have also been noted amongst ethnic minorities (Bustillo et al., 2017). This suggests the need to understand the experiences of minoritised young people’s cancer journey to achieve equitable care.
Young People with Cancer
The transition from childhood to adulthood is a pivotal developmental stage where teenagers and young adults (TYAs) navigate the crises of ‘identity’ and ‘intimacy’ to establish their personal identity and committed relationships (Erikson, 1968). Yet, the arrival of chronic illness interferes with their social, occupational roles and is perceived as a biographical disruption that threatens self-coherence (Bury, 1982). This initiates a meaning making process referred to as narrative reconstruction by Williams (1984), where individuals renegotiate identity and reconstruct a new sense of order in the world that contributes to an adaptive growth. McAdams’s narrative identity theory (1988) added that through constructing life stories, individuals can integrate past experiences to create a coherent sense of self and navigate life transitions. This has influenced the movement towards narrative-based medicine, which shifts from dominant medical perspectives to prioritising patients’ narratives as a resource to understand and deliver patient-centred care (Kalitzkus & Matthiessen, 2009).
Research has explored the unmet needs of TYAs with cancer, where fertility concerns, the need for age-appropriate information, communication and social support were frequently quoted (Bibby et al., 2017). Moreover, ethnically minoritised patients are more likely to have additional unmet needs, poorer quality of life and prognosis than the White ethnic group (Moke et al., 2019; Murphy et al., 2021). Keegan et al. (2012) found that minoritised TYAs were more likely to have at least six or more unmet needs than non-Hispanic Whites relating to recurrence concerns, treatment options and financial support. Having more unmet informational or service needs was in turn associated with poorer physical and mental quality of life (DeRouen et al., 2015; Smith et al., 2013). This underscores the adverse impact of ethnic discrepancies in needs and service provisions that warrant attention. This population is faced with a ‘double disparity’, where they struggle with challenges of cancer at a transitional age in tandem with barriers associated with identifying as ethnically marginalised (Munoz et al., 2016). Young minoritised patients were also less likely to take part in research than White patients (Harlan et al., 2011), highlighting the underrepresentation of minoritised TYAs’ voices and presents a knowledge gap. Little qualitative research has been conducted into how ethnically marginalised TYAs make sense of their cancer, its impact and their cancer care. This underlines the limits of current literature in understanding the differential and compounded impacts created by structural differences.
Rationale and Aims
Understanding minoritised young people’s experiences of cancer has the potential to drive quality improvement in healthcare. Amplifying their voices promotes empowerment and representative care through increased cultural understanding and competence.
The present study aims to explore the cancer stories experienced by ethnically minoritised TYAs through the following research questions: 1. What stories do ethnically minoritised TYAs tell about their experiences of cancer? 2. How are cultural narratives depicted in minoritised TYAs’ cancer stories? 3. What stories do minoritised TYAs tell about their perceived barriers and facilitators to cancer care?
Methods
Design
A qualitative design was employed, referencing thematic narrative analysis methodologies from Hjulstad et al. (2023) and Riessman (2008) to elicit ‘what’ participants’ illness stories are about. The study also attended to structural elements informed by Frank’s (1995) typology of narratives to understand how TYAs constructed their stories and identities through individual interviews.
Ethical Considerations
This study received approvals from an NHS Research Ethics Committee and the Health Research Authority (Ref: 23/ES/0012). Informed consent was sought from all participants prior to the interviews, where voluntary participation, anonymity and confidentiality were emphasised.
Participants
Purposive sampling was adopted to recruit TYAs aged between 16 to 24 with a diagnosis of cancer (any stage), who self-identified as belonging to an ethnically minoritised group through an NHS TYA Cancer Service, social media and charities. This age range aligns with the UK clinical service structure and guidelines (National Institute for Health and Care Excellence, 2014). Non-English speakers were excluded to ensure effective communication to avoid misinterpretation of narratives.
Procedure
Eligible participants were given an information sheet and offered the opportunity to ask questions regarding the study. Following consent, they were invited to complete a demographics questionnaire. All participants opted to attend the interview online with the same interviewer (LC), which had an average duration of 77 minutes. Following the interview, participants were offered a debrief space and given information about accessing psychological support if needed.
Interview
The interview schedule acted as a guide that covered three areas pertaining to the research questions: cancer experiences, cultural narratives and cancer care. Kim (2015) suggested that a narrative interview should elicit a process of storytelling and have minimal influence from the interviewer. The interview followed Kim’s (2015) two proposed phases: the narration phase encouraged participants to tell their stories without interruption from the interviewer and the conversation phase allowed the interviewer to ask clarifying questions and elicit additional narratives.
Analysis
A narrative unit constituted of participants’ illness stories, hence accounts were preserved and analysed as a whole unit to reduce risk of losing meanings in the stories. The process involved five stages: (a) interviews were transcribed and “cleaned up” to remove dysfluencies, (b) familiarisation of narratives through re-reading, (c) coding narrative segments and developing core narratives for each participant, (d) organising coded narratives into themes, and (e) identifying similarities and differences in themes within and between participants’ accounts. The data was coded independently by two authors (LC, AW) and organised into themes. These were reviewed and refined through discussions with all authors for coherence and validity. The results were grounded in direct quotes to ensure transparency and rigour.
Quality Assurance
Narrative approaches are rooted in social constructionism, which emphasises that reality is socially constructed though language, discourse and meaning making (Clandinin & Connelly, 2000), hence reality emerges from the stories told. A reflexive interview was carried out to enhance reflexivity in exploring any preconception or assumptions to minimize interpretation biases. The interviewer had no prior clinical contact nor cultural familiarity with the participants. A reflective journal was maintained to document self-reflection and enhance methodological transparency.
Results
Participant Demographics
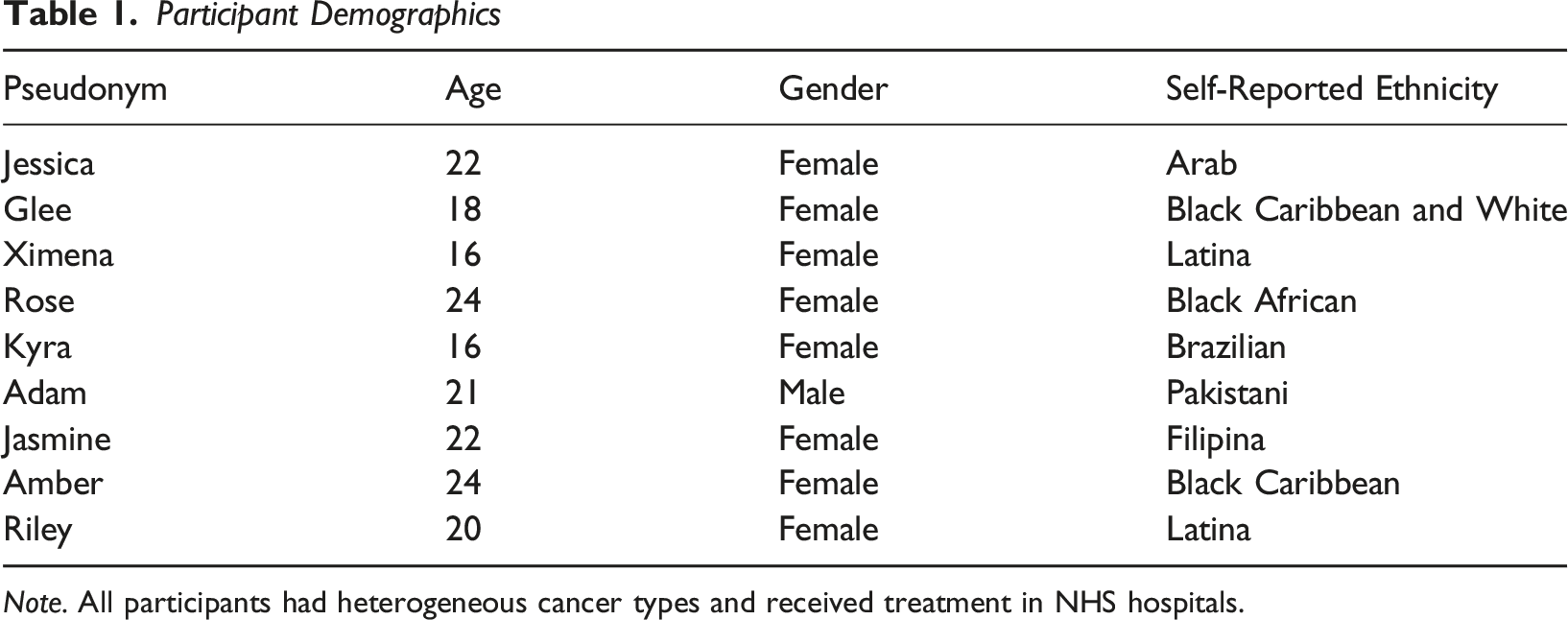
Note. All participants had heterogeneous cancer types and received treatment in NHS hospitals.
Cancer Experiences
All participants began their stories when they first noticed signs and sought medical attention.
Dismissed
Six participants described their experiences of presenting to services and were “not taken seriously”. Their concerns were “not listened to” and reported repeated visits where they were dismissed back home. “She told me maybe I'm stressed, or it's anxiety. I felt like I wasn't being taken seriously because she wanted me to go home with just painkillers, but I knew something was wrong...” – Jasmine
Rose expressed frustration at the limited medical attention she received. She linked her experiences to news reports of discrimination faced by Black people in hospitals, citing higher mortality rates and different treatments. Not a single person checked my eye pressure, no CT scan, no MRI scan or just a simple blood test whatsoever…I even had to argue with them to get them to prescribe me stronger painkillers. – Rose
Amber attributed her experiences to her young age, but also alluded to a running theme of perceived discrimination within her family, where members felt unheard by doctors which delayed diagnosis. “It wasn't really taken seriously, I think cause of my age, I was so young…my grandmothers both passed of pancreatic cancer, both of them were back and forth from the doctors testing for everything but cancer, saying “oh it’s their bowels”, but it just wasn’t, they weren't listening and they didn’t run the right test that they needed.” – Amber
Some began harbouring mistrust towards the system. “They don’t take me seriously and I don’t trust what they say either.” – Rose
Shock and Turmoil
All participants described the “shock” upon receiving the diagnosis. Some expressed fear and confusion, while others revealed strength and determination that emerged in the face of uncertainty. For some, it spurred a need to make sense of why they had cancer. “I just couldn’t believe it 'cause I've always been so healthy my whole life.” – Riley
For Glee, Kyra and Adam, the delayed realisation only came after they saw others’ reactions that prompted them to recognise the severity of their condition. When I saw my parents cry, cause both my parents are very strong minded…then I realised how serious it was. – Adam
For many, this marked a pivotal point in their life that heralded anxieties and uncertainties about the future. “I was scared because I didn't know the extent, I didn't know what was gonna happen. I didn't know what I was gonna be on. And then I started worrying about, am I gonna lose all my hair? What's gonna be the complication?” – Glee
Grieving Self and Changes
All participants spoke about the emotional turmoil of grieving their former self and navigating changes brought about by cancer. They described the physical destruction from intensive treatment and the side-effects that continued to linger post-treatment. “If I was in rugby now, I’d snapped in half… I miss that healthier looking body. Now I'm much more frail, like my muscles have shrivelled up and dried.” – Riley
Jasmine, Glee, Adam and Kyra articulated the impact of losing their hair which represented the loss of their identity and confidence. This led to feelings of insecurities about their appearance and self-esteem. It changed my self-confidence a lot because I lost my hair… it just felt like I lost a big part of my identity. Even though my hair is grown back, it's still a constant reminder of what's happened and all the trauma that I went through. – Jasmine
Rose echoed the sense of loss, insecurities and grieved the confident person she was. When I try to do things that I used to enjoy before, I had a life, I was a person…I was confident. I literally cried when going out because I find it so hard to be in social situations. – Rose
For Ximena, the changes were so overwhelming that they shattered her sense of self, leading to an existential crisis of feeling hopeless and despair. “I want to die… because it is no was (it was not a) normal Ximena. It was a different Ximena.” – Ximena
Many described the hardest part was adjusting to the life changes as cancer became their “full time job”. For some, this meant prioritising their health and changing the way they socialised, which left them isolated. “I can't count on everyone knowing that they have to stay away from me if they're sick… I miss just being able to eat, now I have to think about what I eat.” – Riley
All participants shared disruptions to their lives that meant they had to put their life on hold and became unable to fulfil their expected social roles. “I'm not gonna go back as normal and I'm not gonna do the interview that I thought I would.” – Jessica
Amber and Rose attempted to make sense of their new reality, but felt lost in finding their identity, purpose and place in the world after treatment. “What am I? Where does my life go now? What am I doing now? … because it changes you so much, you don't really know who you are. – Amber
Many also shared heightened anxiety and a fear of re-occurrence that pervaded their life. “I'm scared of headaches now, 'cause I'm thinking, is it growing?” – Glee
Isolated and Helpless
Isolation was a theme that penetrated across all narratives. Adam and Amber described being hospitalised during COVID which kept them physically isolated. Many highlighted the disconnection from peers and felt excluded from the typical trajectory of TYA lives. It was like being back in COVID, but it was only me on lockdown and everyone else was free to do whatever they wanted. – Riley
Some spoke about the lack of representation in age and ethnic background in cancer support groups they attended that exacerbated feelings of isolation. “Nobody looks like me. Nobody's my age. No one's my skin colour, even when they are my skin colour, they're not my age…So there's no one I can relate to and that makes it so lonely.” – Rose
For Jessica and Riley, having a rare cancer further marginalised them as they navigated an untrodden path fraught with uncertainties. “Because it's such a rare tumour, very little is known about it. A big part of it is I feel like I'm just experimenting and that is not very reassuring. There's not much research out there saying what will happen.” – Jessica
Rose, Jasmine, Amber and Riley reflected on the loss of relationships whilst going through cancer as peers failed to understand and support them. Sentiments of resentment were shared, though they were able to recognise real friends who “stepped up” for them. “My friends chose to do things (go party) like that, over staying with me in the hospital or keeping me company because they probably didn't understand how it feels to be stuck in a hospital room for five days straight….I lost a few friends whilst I had cancer, but it was for the better.” – Jasmine
Similarly, Adam, Riley and Jasmine felt unsupported by their school and workplace, which left them feeling disappointed and helpless. “My teachers didn't consider at all what I had gone through…and he gave me a terrible grade.” – Adam
Adapting in Adversity
All participants emphasised the importance of family and friends who supported them through cancer. “My brother and my dad shaved their heads and that would make me feel a bit better.” – Kyra
Many appreciated charities and healthcare professionals that gave emotional as well as practical support. Glee, Rose and Kyra also mentioned spirituality as a source of comfort. Some described personal resilience that enabled them to power through the difficult times. “It's really easy to get into the slump…then feeling sorry for myself. But being sad doesn't change anything, and I was thinking might as well try to enjoy the time I do have and do things to better myself.” – Riley
Keeping occupied and maintaining normality were discussed as distractions and ways to regain some sense of control. “I guess trying to keep as much of a normal life as I could, even though nothing was normal anymore.” – Riley
Some shared that being open to talk about their experiences allowed them to “unpack” and make sense of their feelings. Amber added that “taking one day at a time” and staying informed helped as “sometimes the not knowing is worse.”
“Changed for the Better”
All participants, except Jessica who had not started treatment, shared a changed outlook on life that led to positive changes and growth. Jasmine, Adam and Amber reflected on how volatile and precious life was, urging them to make the most of every opportunity and be grateful. “I use that (cancer) as my strength… if I can get through that, I can get through anything and I can achieve anything that I want. Life's so short, I just go for it” – Amber New priorities emerged: “I really prioritise my health now a lot more and mental wise, I use my cancer to make me keep going basically, I just want to be healthy all the time.” – Adam
Empowerment was described by Ximena, Glee, Jessica and Adam as rejecting vulnerability, seeking independence and living a life beyond cancer. “Normally I go in wheelchair. But now I want to go alone to the college and I go with the crutch alone.” – Ximena “I didn't like how everyone just felt sorry for me all the time…I just wanted to be seen the same as everyone. – Adam
Participants also spoke about taking meaningful actions to influence others, including aspiring to become healthcare professionals to help people with cancer and acts of “giving back” via charity work and becoming cancer ambassadors to raise awareness. “When you go through something so traumatic, your voices, your power should be used in the best way.” – Jasmine
Cultural Narratives
All participants discussed intersections between family and their culture, though their narratives diverged greatly.
Family: Support or Burden?
Adam, Glee, Ximena, Kyra, Amber storied their large families as supportive and helpful. Cancer brought their families closer together and facilitated better relationships. Food was highlighted as a form of expressing care. “When you're not well, everything is solved via food. So every day I would have a different auntie coming to my house and dropping off a whole tray of food.” – Adam
Jessica and Riley resonated with feeling cared for, but also expressed ambivalence around the “over caring culture” which at times increased pressure on them. The culture is very family oriented. So having my family involved… that adds to the pressure…it only makes me more indecisive of what I wanna do. – Jessica
By contrast, Rose and Jasmine described cultural clashes leading to difficult family dynamics that burdened them on top of cancer. Rose spoke of the frustration from the “television view of cancer” in her community, which required her to fight for her preferred care. “They were trying to make me drink soursop tea…But it can interfere with chemotherapy. So I had to have that fight and battle with my family members, saying “I'm not going to try soursop tea... I understand that somebody's auntie who's tried it…but this is not how I want to do it”. That was super frustrating… having to justify my medical care to people… people within the African and Black community don't trust big Pharma …and “chemotherapy is killing you”, which is really heart-breaking because… I needed that chemotherapy to stay alive.” – Rose
Both echoed that the perceived societal scrutiny of ethnically minoritised parents at times compromised participants’ emotional needs. “My mum cares a lot about what other people think rather than how I feel, so she wouldn't want someone to see me crying in my hospital bed when I'm in their presence because she's worried about how she might look as a mum... Ethnic parents aren't really open to the idea that a young person could be depressed or anxious because to them, your stresses are really minor in comparison to what they experience…and it would become a competition of who's going through the worst thing.” – Jasmine
Their stories underscored the complex interplay between acculturation and familial relationships within minoritised communities. Acculturation exacerbated tensions within the family unit as traditional cultural beliefs clashed with Western views and contributed to conflicts.
Feeling Othered and Lonely
Participants described feeling lonely as they struggled to meet people culturally similar to them whom they could relate to, which underlined the lack of racial representation in cancer communities. “I've gone to support groups…but 9 times out of 10, I'm probably the only Black person in the room. It was difficult because none of them relate to me. Sometimes it just helps to have someone, talk to someone that looks like you, because there's certain things that can go unsaid.” – Amber
For Kyra, being of mixed heritage exacerbated this loneliness as she felt torn between her racial identities and did not feel belonged to either group. “I feel like none of those (ethnic categories) fit me 'cause I don't think people see me as that... just separated from the other kids.” – Kyra
For participants born outside the UK, loneliness was more pronounced as they were physically separated from their families and left to navigate their cancer journey on their own. “They're surrounded with their family. And I'm kind of here and my family is not here.” – Jessica
These examples illustrated that as cancer shattered participants’ sense of self and derailed their lives, their need to belong and find support within their ethnic communities became increasingly crucial to feel safe.
Cultural Influences
For Adam, Kyra, Jasmine, Riley, whose cultures were deeply intertwined with religion, cancer was viewed as a challenge from God. Adam, who ascribed to these views and believed that “it will make you a better person” found it helpful in coping with his illness. Others, however, rejected these views as whilst it served to reassure their families, it was “not always what I wanted to hear” and wished for more understanding. “I always hear “God puts his strongest soldiers through the hardest battles”. But sometimes you just want your feelings to be validated and understand that you're going through a hard time.” – Jasmine
For Jessica and Rose, cultural considerations weighed heavily on their treatment options. “Getting married, having kids is such a big cultural thing…chemo will affect your fertility…but that's stuck with me more, it's definitely on the bottom of the list for a treatment option.” – Jessica
Rose conveyed fear of the limited treatment options for her cancer type amongst minoritised populations that could compromise survival: “The likelihood of statistics around Black people on the stem cell transplant list is extremely low … it could take me years to find a match because the rate of it (transplant match) is so low for people from ethnic backgrounds, especially Black people.” – Rose
These stories demonstrated the diverse ways in which participants’ ethnic identity and culture shaped their perception of cancer and treatment options. These cultural narratives spoke to TYAs’ need to feel heard, held and for their plight to be acknowledged.
Barriers and Facilitators of Care
All participants storied their overall experience of cancer care as positive. However, for some, care in the initial stages of diagnosis, were disappointing.
Overlooked and Lost
Six participants described their concerns were “not taken seriously”, which reflected the lack of TYAs cancer awareness amongst professionals. For some, this late diagnosis impacted on their prognosis and treatment options. “Everything was quite overlooked at… when you look at the symptoms of lymphoma, the symptoms I had really aligned. So the fact I got told twice it was nothing and I got sent home with just painkillers, when I had a really big tumour in my chest... the lymphoma I had was really aggressive, I had to start my treatment straight away. So I never got to see a fertility doctor.” – Jasmine.
Rose, Amber and Riley underlined clinicians’ lack of cultural sensitivity in care that led them to be overlooked. “(Doctor) came to show me pictures of White people with styes and infected cysts and said how these looked the same to what I have…But I am Black and my eyes are black. Bruising in a White person would obviously look very different from bruising in a Black person with Black complexion.” – Rose
Jessica, Ximena and Riley expressed frustration from service mistakes. “They wanted me to redo my biopsy because they lost my biopsy slides…I started crying because I was just frustrated… cause you know appointments being lost, referrals being lost in the hindsight is not too bad. But for me to redo a whole biopsy, like no.” – Jessica
Communication gaps highlighted by Kyra and Riley left them uninformed and confused. “When I got diagnosed, I knew what it was, but I didn't understand, I’d rather they explained… Before my surgery, I remember I would cry a lot 'cause I didn't understand… I think no one explained any.” – Kyra “(charity) representatives came to see me and told me something about infertility because of chemo, and I didn't know that, no one told me that, no doctor told me that.” – Riley
Adam, Amber, Jasmine and Riley narrated encountering clinicians who were uncaring and patronising, which left them feeling disrespected and invalidated. “He just treated me like a kid, like I was dumb, but also very mean…And he was asking me my prognosis and if they had high hopes for me because there was no point doing the fertility preservation if I was going to die.” – Riley
Feelings of frustration and helplessness permeated these stories of care that left participants feeling unseen, disregarded and unsupported. This added stress and became barriers to receiving effective care.
Personalised and Accessible Care
All participants spoke to the importance of personalised care and appreciated support that tailored to TYAs’ specific needs. “Her (nurse) skin colour was similar to mine. So she was like, “our bodies, scars can heal in this way, and this type of scar can be more common in our skin type”… I think that was really specific and helpful…She even told me the name of the kind of scarring that it could come up as. I think personalised care is a good word for it.” – Jessica
Jasmine and Riley expressed that having age-appropriate facilities lightened them up during difficult times of treatment. “It was specifically for young people, they had a room where there was games, game boards, PlayStation, things to draw and paint on… So even though you're in hospital, you have some means to entertain yourself…so that was definitely helpful.” – Jasmine
Adam added that building personal connections with TYAs through conversations can enhance their experience of care. “Get to know them a bit more personally rather than just be like, “oh, you're here for this treatment”… because when you're very personal with someone like that, it makes the whole experience a lot better.” – Adam
Most participants highlighted accessible support and communication as facilitators in care that promoted a sense of control. “If I need any help, she would reply me quickly. Like I remember as soon as I got the hives… she literally replied to me, I don't think it was an hour, like they're very on the ball.” – Glee
Jasmine and Riley spoke about extending the accessibility of support beyond hospital settings and suggested written aids to overcome language barriers. “Medical words are so difficult to understand. It'd be nice if someone could translate into regular people language… if she had it written…it would be there…Sometimes I wish you could put on subtitles on people.” – Riley
Feeling Seen
For many, having emotional support and a peer support network that shared similar experiences and cultural heritage were storied as instrumental in fostering connection, validation and eased feelings of social isolation. “I met another girl who had the same type of cancer as me and she was Black, and I think that was helpful, because someone here had been through what I've been through and also (looked) like me.” – Kyra
Rose and Amber echoed this and felt that clinicians should acknowledge their differences and take initiative in connecting TYAs to relevant communities. “I wish healthcare professionals would educate themselves more to help…Like “all you might be going through something different, I don't understand this, but there's this group of people that might” because … being a Black woman does make this experience different. – Rose
Similarly, Jessica, Rose, Kyra, Amber, Riley and Jasmine highlighted the importance of cultural sensitivity in care that helped them feel seen and more relatable. “We got these dolls…and it was my kind of skin colour and hair colour and I just think that was nice. I think that was more important to me, just being seen.” – Kyra
Cared by a team who was “friendly”, “supportive” and “keep you in their best interest” was appreciated by all participants. Staff promoting choice and agency enabled participants to feel more empowered when their illness have stripped them of their autonomy and control. Ximena, Rose, Kyra and Amber spoke of being treated with respect that made them feel valued. “Clinicians bringing themselves down to my level… when I'd be on the bedside, they'd come down and they'd speak to me face to face. That was extremely powerful.” – Rose
Discussion
This study aimed to explore ethnically minoritised TYAs’ experiences of cancer and cancer care. The findings offered insights into how cultural influences shape the needs of minoritised TYAs to inform personalised support.
What Stories do Minoritised TYAs Tell About Their Cancer Experiences?
Findings from this study illustrated protracted journeys to diagnosis in line with the literature. Gibson et al. (2013) examined young people’s pre-diagnosis experiences and revealed that repeated GP visits were disappointing as concerns were not acted upon. They highlighted common beliefs that ‘young people do not get cancer’ led to symptoms being minimised. The lack of awareness is likely compounded by subtle symptom nuances and perceived ethnic and age discrimination in minoritised TYAs, prolonging the diagnostic delay.
Findings highlighted the emotional turmoil experienced by TYAs in relation to the biographic disruption from cancer. Kim et al.’s (2016) meta-synthesis illustrated that disruption to fulfilling normative social roles evoked feelings of distress, guilt and uncertainties. Identity formation was further interrupted by physical changes that affect self-image and a reduced sense of control and autonomy, mirroring participants’ accounts of “feeling lost”. The theme ‘isolated and helpless’ resembled the literature in demonstrating that the life adjustments TYAs faced left them feeling socially excluded from peers (Drew et al., 2019), which was associated with poorer psychological well-being (Fox et al., 2023). This underscores the importance of peer network and emotional support at this developmental stage.
Williams’s (1984) idea of narrative reconstruction explored the cognitive reorganisation in relation to self and the society to reconstruct a sense of order from the illness-induced disruption. This resonated with participants’ narratives of keeping occupied and maintaining normality as ways to regain control. The theme “changed for the better” reflected the collective strength and resilience gained through adversity for most participants and supported evidence that demonstrated better wellbeing in survivorship than healthy peers (Jörngården et al., 2007). Participants’ narration in this study may have been therapeutic and promoted the meaning-making process (Atkinson & Rubinelli, 2012).
How are Cultural Narratives Depicted in TYAs’ Cancer Stories?
Whilst cultural stigma and taboo around cancer were frequently reported in adult literature (Ridge et al., 2023), such narratives did not present in this study. Not disclosing cancer was storied as not wanting to burden others, rather than avoid shame. This could suggest increased cancer knowledge in newer generations of minoritised populations, intersecting with the impact of acculturation may have mitigated stigma.
Findings highlighted discrepancies in how TYAs experienced family involvement as influenced by cultural perspectives. Whilst most valued family support, two participants found it burdening. Huang et al. (2022) examined family coping amongst racially minoritised groups and underlined effective family communication as adaptive coping. In some cultures, prioritising harmony and comfort led to communication avoidance, echoing Jasmine and Rose’s stories of cultural clashes that led to feelings of invalidation and frustration. These accounts aligns with Bronfenbrenner’s (1979) ecological systems theory in highlighting how different levels of interrelated systems shape our development. This framework strengthens the validity of findings and helps contextualise participants’ narratives through interacting layers of family, cultural and societal norms. Findings emphasised that the way TYAs storied their support were positioned within their socio-cultural context: their personal family dynamics in the microsystem interacted with the broader cultural and societal influences in the macrosystem to shape their narratives (Bronfenbrenner, 1979).
Cultural identity exacerbating loneliness was a recurring theme across narratives. The lack of representation in cancer communities resembled adult research, which reinforced feelings of ‘othered’ and left TYAs feeling unsupported (NHS England, 2020). A desire for better cultural visibility was communicated by participants to challenge the dominant culture of whiteness and foster validation.
What Stories do TYAs Tell About Their Perceived Barriers and Facilitators to Care?
Overall, participants described a positive experience of cancer care. Personalised and accessible care were identified as important facilitators to care. The provision of age-appropriate care suited to young people’s psychosocial needs, such as entertainment facilities and access to a youth worker, along with clear communication have been highlighted as key elements to good quality care (Furness et al., 2017). Individuals who indicated having their informational and service needs met were less likely to report fear of reoccurrence (Shay et al., 2016). This suggests accessible care can promote psychosocial wellbeing.
Additional factors influencing participants’ perceptions of care included cultural sensitivity and feeling seen. Participants’ diagnostic experiences reflected ‘whiteness’ as the default in services, which failed to acknowledge cultural diversity. This ‘colour-blindness’ perpetuated structural inequalities in health outcomes and care experiences in minoritised populations (Cunningham & Scarlato, 2018). A recent review highlighted that amongst interactions between racially minoritised people and professionals, feeling connected, not ‘othered’ and recognising the whole person within their socio-cultural circumstances were valued (Ridge et al., 2023). Examples of these were cited by TYAs in the present study, where their cultural heritage was recognised through receiving dolls and wigs that aligned with their identity. Patient-perceived cultural sensitivity of professionals was linked with improved adherence to treatment (Tucker et al., 2011). This implies systemic approaches that display cultural appreciation and interpersonal warmth can create safety and connection for minoritised TYAs whilst promoting adaptive health behaviours. TYAs’ need to be heard and seen could be understood as attachment behaviours in helping them cope and anchor their stories, whilst they navigate turbulent cancer challenges. Likewise, peer contacts and emotional support were highlighted as important by all participants. These areas were consistently identified as essential needs in TYAs literature which reflect the fundamental tasks of constructing identity and social belonging at their developmental stage (Bibby et al., 2017). A sense of shared identity provides validation and reduces feelings of isolation.
Limitations
Many participants were recruited from South East England which presents a geographic sampling bias weakening the generalisability of findings to broader, less culturally diverse regions. Findings could, therefore, overlook critical factors that influence services’ cultural competence, directly impacting on patients’ access to support and care experiences. Vast differences exist across and within cultures which could not be fully elaborated, for instance intersectionality of acculturation, socioeconomic status and religious beliefs may contribute to distinctive cancer experiences. The gender bias with predominantly female participants also limited masculine cancer narratives, which lacked diverse perspectives on cultural attitudes of masculinity associated with emotional reticence, help-seeking and coping behaviours. Moreover, excluding those with language barriers failed to reflect the diverse realities of challenges faced by marginalised groups, such as miscommunication, compromised quality of care, access to services and patient satisfaction. This limits the study’s ability to inform culturally and linguistically sensitive practices, perpetuating health disparities.
Clinical Implications
The diagnostic obstacles reported highlight the need to challenge the Eurocentric approach to care by considering ethnic nuances in presentation and how distress and support are experienced within individuals’ socio-cultural context. The cultural narratives emerging from this study indicate that exploring the impact of cultural clashes and family communication may be beneficial in understanding TYAs’ psychosocial needs situated within their socio-cultural background. Current psychological assessment should be reviewed to ensure they capture constructs relevant to ethnically minoritised TYAs, such as cultural orientation, acculturation, family support, and suggest value in family sessions. Similarly, clinicians’ acknowledgement of their cultural position and differences to minoritised TYAs may facilitate engagement and trust. Minoritised TYAs’ narratives underlined a desire to connect and relate. Group interventions or community-based initiatives connecting ethnically diverse TYAs could foster a sense of community and support. These cross-sector collaborations have the potential to build minoritised community trust and hear underrepresented voices to address barriers to access support.
Future Research
TYAs’ evolving needs and challenges continue beyond remission, hence exploration of their survivorship experiences is warranted. Recruiting more male participants and delineating the impact of acculturation on TYAs’ experiences could allow a deeper understanding of how cancer and coping mechanisms are experienced in different socio-cultural contexts. The voices of marginalised TYAs with language barriers need to be heard. Research may benefit from exploring clinicians’ perspectives of working with minoritised TYAs to highlight any challenges or structural resistances to providing equitable care.
Conclusion
The findings reflected both the hardship and post-traumatic growth experienced by minoritised TYAs with cancer in line with the wider literature. Cultural narratives relating to feeling othered, family support and treatment options appeared to complicate their experiences. Personalised and accessible care, peer support and experiences of feeling seen were highlighted as key facilitators to cancer care. Findings underscored the importance of cultural sensitivity and visibility in services.
Supplemental Material
Supplemental material - Experiences of Cancer and Cancer Care Amongst Ethnically Minoritised Young People in the UK
Supplemental material for Experiences of Cancer and Cancer Care Amongst Ethnically Minoritised Young People in the UK by Lynette Wing Suen Chan, Alan Hebben-Wadey, Chandrika Kambakara Gedara, James McParland in Clinical Child Psychology and Psychiatry.
Footnotes
Author note
This research was completed in partial fulfilment of LWSC’s Doctorate in Clinical Psychology program.
Ethical Considerations
This study received approvals from an NHS Research Ethics Committee and the Health Research Authority (Ref: 23/ES/0012).
Consent to Participate
Written informed consent was sought from all participants prior to the interviews, where voluntary participation, anonymity and confidentiality were emphasised.
Author Contributions
All authors contributed to the study conception and design. LC collected the data and wrote the first draft of the manuscript. All authors contributed to data coding, analysis and reviewed the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Selected anonymised qualitative data from the interviews can be made available upon request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.