
Abstract
Objectives
To characterize health related quality of life (HRQOL) for Canadians aged 16 to 25 (adolescents and young adults, AYAs) seeking care for mood and anxiety concerns at the First Episode Mood and Anxiety Program, in London, Ontario and to identify factors associated with HRQOL in this population.
Methods
AYAs completed demographic, psychometric, and HRQOL questionnaires. We calculated 36-Item Short-Form Health Survey (SF-36) scores standardized to Canadian and US population norms. We computed Short Form 6 Dimension (SF-6D) utilities conducting multivariable linear regression analysis, adjusting for age, sex, ethnoracial minority status, parental marital/cohabitation status, parental education, the Anxiety Sensitivity Index (ASI-R), Montgomery-Åsberg Depression Rating Scale Self-Report (MADRS-S), Sheehan Disability Scale (SDS), and a modified Inventory of College Students’ Recent Life Experiences (ICSRLE-M).
Results
Amongst 182 AYAs who completed questionnaires, mean physical component summary (PCS), mental component summary (MCS) and SF-6D utility scores were low, 43.8 (SD = 16.6), 19.0 (SD = 11.9) and .576 (SD = .074), respectively. Maternal post-secondary education, depression (MADRS-S) and functional impairment (SDS) were significantly associated with SF-6D utility.
Conclusion
This cohort of mental healthcare-seeking AYAs had significantly impaired psychometric and utility-based measures of quality of life, underscoring the importance of timely access to healthcare services for this population.
Keywords
Introduction
One in five Canadians suffer from mental illness during their lifetimes (Smetanin et al., 2011). Furthermore, three-quarters of mental illnesses start at or before the age of 24 (Kessler et al., 2005). Mental illness can seriously impair lifetime health-related quality of life (HRQOL) (Osuch et al., 2016). Globally, affective disorders are the most prevalent, with depression being one of the largest single causes of disability (World Health Organization [WHO], 2021). Forecasts estimate that mental illness will be the leading cause of disability in Canada and other developed nations by 2030 (Mathers & Loncar, 2006). Early intervention programs for mood and anxiety disorders can be highly effective (Anderson et al., 2019). However, such programs have not been widely implemented (Osuch et al., 2016).
Social determinants of health (SDH), namely physical environment, individual behavior, and social circumstances, are estimated to account for 67% of an individual’s health and wellness (Choi & Juhan, 2017). Factors like age, gender, and socioeconomic status have been linked to morbidity and HRQOL in the literature: Guertin et al. (2018) found that HRQOL varied with age and sex; Melchior et al. (2010) found lower socioeconomic status to be associated with more severe symptoms of mood and anxiety disorders; and Chong et al. (2012) found less education and economic inactivity were associated with higher rates of morbidity. Despite this, few studies have measured HRQOL in younger populations at the point of seeking care for mental health concerns.
The Public Health Agency of Canada (PHAC) defines social determinants of health (SDH) as the socioeconomic factors that determine individual and population health (Public Health Agency of Canada [PHAC], 2023). In the present study, we collected information on social determinants of health from AYAs who were seeking care. The information collected pertains to income and social status, childhood experiences, physical environments, social support and coping skills, gender, culture, and race. Other SDH included in the PHAC framework but not analyzed in this study include employment and working conditions, education and literacy, healthy behaviors, and access to health services (PHAC, 2023).
The link between mood and anxiety disorders and poor health related quality of life has been well established (IsHak et al., 2011; da Rocha et al., 2009). Population-based studies have demonstrated that the presence and severity of depressive symptoms are associated with poor HRQOL (Ayuso-Mateos et al., 2010; de Sá Junior et al., 2018). Individuals with diagnosed mood and anxiety disorders have significantly worse HRQOL than the general population (Tang & Thomas, 2020). Treatment for mood and anxiety disorders has also been linked to improvements in HRQOL (IsHak et al., 2015; Wiesenger et al., 2023). Furthermore, social support has been identified as a predictor of treatment response and symptomatology for individuals with major depressive disorder (Lara et al., 1997). While HRQOL among young adults is significantly impaired in the presence of mood and anxiety disorders (de Sá Junior et al., 2018; Tang et al., 2019), less is known about HRQOL in AYA seeking care for mental health concerns.
Health utility is a measure of the strength of preference for a “health state”. This measure can be used to weight life expectancy in clinical decision analysis and economic evaluation. In general, a health utility of 1 is equivalent to perfect health while a health utility of zero is equivalent to death. Some measures of health utility, like the EuroQol Five Dimensions (EQ(5D)) and the Health Utilities Index Mark 3 (HUI3), can accommodate negative health utility values to indicate states worse than death. Based on the standard gamble utility elicitation method, the Short-Form Six-Dimensions (SF-6D) utility conveys the public’s strength of preference for the health states. The responses from a subset of the SF-36 items describe the health state of the respondent in six dimensions, including Physical Functioning, Role Limitation, Social Functioning, Bodily Pain, Mental Health, and Vitality (Brazier et al., 2002).
We aimed to characterize HRQOL in a population of adolescents and young adults (AYAs) seeking care for mood and anxiety concerns and to explore the association of social determinants of health, symptom severity and functioning with HRQOL in this population.
Materials and methods
Study setting
Based in London, Ontario, Canada, the First Episode Mood and Anxiety Program (FEMAP) was designed to improve access to early intervention for mood and anxiety disorders among AYAs between the ages of 16 and 25. Individuals may be referred to FEMAP through social workers or clinicians, or seek treatment independently (Osuch et al., 2016). An exclusion for consideration for FEMAP is lifetime psychiatric medication use of over 18 months. Thus, this population is considered to be in the early stages of their psychiatric condition. Between July 2017 and June 2018, 182 consecutive individuals seeking care at FEMAP were screened and completed questionnaires prior to an intake assessment for appropriateness of entry into treatment. Questionnaires were part of a process evaluation that requested individuals to fill out demographic, socioeconomic, symptomatology, and quality of life questionnaires (Osuch et al., 2019). The current study is a retrospective analysis of the cross-sectional assessment at pre-intake provided by these 182 AYAs with mood and anxiety concerns who sought treatment at FEMAP.
Measures
Demographic and socioeconomic characteristics
We took a theory-driven approach to determine which SDH variables to include in the analysis. Drawing on this retrospective sample, the factors investigated in this study included age, sex-at-birth, ethnoracial minority status, parental education, and parental marital/cohabilitation status. Parental marital status approximates social environment, familial stability and access to resources (Saunders, 2016). Parental level of education, particularly maternal education, has been associated with financial security and good mental health (Coleman et al., 1966). Even as individuals age and live independently of their parents, parental measures influence social determinants of health through the relationship to income, social status, childhood experiences, social supports, coping skills, and physical environments.
Age was dichotomized as “16-18″ and “19-25″ to distinguish between adolescents and young adults. Individuals typically complete their secondary education at the age of 18 and legally transition into adulthood, signifying a considerable life transformation.
Participants self-reported their ethnicities, and we categorized them into the eight Canadian census categories. Participants who indicated their ethnicity as “White Canadian or American'', or “White European'' were categorized as “White”. This cohort largely identified as being in the White ethnoracial category (n = 140, 76.9%), followed by Mixed (n = 14, 7.7%), Middle Eastern (n = 8, 4.4%), Latin American (n = 7, 3.8%), Black (n = 5, 2.7%) and other ethnicities. According to the 2016 census, 19.9% of individuals living in London, Ontario identified as being part of a visible minority population (Statistics, 2017). In keeping with the PHAC framework, we dichotomized ethnicity into the ethnoracial minority status variable, coded as “No” for participants who were categorized as “White” and “Yes” for all other participants. The ethnoracial minority status approximates the potential impacts of racialization, in addition to social and cultural isolation, on HRQOL (PHAC, 2023).
Parental level of education was dichotomized as “No Post-Secondary Degree” or “Some Post-Secondary Degree”. Individuals with parents having “Part College or Specialized Training” were included in the “No Post-Secondary Degree” group. Parental marital/cohabitation status was coded as “Together” for participants whose parents were married, common law or unmarried and living together and “Apart” for participants with separated, divorced, or widowed parents. Participants who checked “Not Applicable” for parental education or marital/cohabitation status were coded as “Missing”. These groupings reflect those used in previous research on FEMAP cohorts (Saunders, 2016).
Psychometric measures of symptom severity and functioning
Severity of symptoms and daily functioning were measured using: (i) the Anxiety Sensitivity Index Revised (ASI-R), (ii) Montgomery-Asberg Depression Rating Scale Self-Report (MADRS-S), (iii) Sheehan Disability Scale (SDS), and (iv) a modified Inventory of College Students Recent Life Experiences (ICSRLE-M) scores. These measures, with the exception of the modifications to the ICSRLE (described below), have been validated in the literature (Kohn, et al., 1990; Leon et al., 1992; Ruedel et al., 2010; Taylor & Cox, 1998). Anxiety sensitivity is defined as the extent to which an individual believes that their experience of anxiety will lead to harmful consequences. The ASI-R, a self-report scale, measures anxiety sensitivity and ranges between zero and 144 (Taylor & Cox, 1998). The MADRS-S measures the severity of depressive symptoms and ranges between zero and 27 (Ruedel et al., 2010). The SDS assesses functional impairment and ranges between zero and 30 (Leon et al., 1992). The ICSRLE measures the impact of daily stressors or hassles and can range between 49 and 196 (Kohn, et al., 1990). We modified the ICSRLE to exclude 2 items relating to sexual activity since not all FEMAP patients were sexually active, and those who were not tended to leave the item blank in previous analyses at FEMAP, reducing the number of useable scores. The resultant modified ICSRLE ranges between 47 and 188 (Saunders, 2016). For all four indicators higher scores reflect poorer health or functioning (Kohn, et al., 1990; Leon et al., 1992; Ruedel et al., 2010; Saunders, 2016; Taylor & Cox, 1998). In the regression analysis, the psychometric indicators were centered at the sample mean.
SF-36 domains and SF-6D utility
The 36-Item Short Form Health Survey (SF-36) is a psychometric measure of health-related quality of life and is the most widely-used measure of generic health status used in clinical research (Ware et al., 1993). Study participants completed version 1 of the SF-36 questionnaire, which measures general health in eight domains represented by distinct subsets of questionnaire items. The eight domains include Physical Functioning (PF), Physical Role Limitation (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Emotional Role Limitation (RE), and Mental Health (MH). Domain scores range between zero (worst) and 100 (best) (Ware et al., 1993). The eight domain scores are also used to compute two summary scores: the Physical Component Summary (PCS) and Mental Component Summary (MCS) scores. Summary scores are standardized against a reference population with a mean of 50 and a standard deviation of 10 with scores above 50 representing better physical or mental health (Ware et al., 1994). We computed summary scores using two reference populations: a random sample of Canadian adolescents and young adults aged 16-24 (our primary reference) and a standard US normative sample to facilitate international comparisons (Hopman et al., 2009; Ware et al., 1994).
Since there are no Canadian preference-weights for computing SF-6D utilities, we used the US preference-weights. This allowed us to obtain a single measure of the strength of preference of the US general population for the health states expressed by the study participants. SF-6D utility computed using the US preference weights range from .301 to 1 (Brazier et al., 2002). That is, the health utility associated with the worst health across all six domains is .301.
T-distribution 95% confidence intervals for means were computed for SF-36 domain scores, SF-36 summary scores, and SF-6D utilities. Means, T-distribution 95% confidence intervals, and p-values for the SF-36 domain scores, Z-score normalized with reference to Canadian AYAs and the US population were also calculated.
Statistical analysis
We studied whether demographic and socioeconomic factors (coded as dichotomous variables) and psychometric indicators (centered at the mean) were associated with SF-6D health utility in a multivariable linear regression model. The model estimated associated changes in SF-6D utility in relation to included demographic factors, socioeconomic factors, and psychometric indicator scores. Since health utility in our sample was neither left nor right censored (Figure 1), we did not adjust our model for censorship. Missing values were imputed using Multivariate Imputation by Chained Equations (MICE), using ten imputation sets (van Buuren & Groothuis-Oudshoorn, 2011). Imputed models were pooled for the final regression model. We assessed the model for normality of residuals, heteroskedasticity, multicollinearity, and high leverage points. Normality of residuals and heteroskedasticity were assessed visually, using plots. Multicollinearity was assessed using variance inflation factors (VIF), with a threshold VIF of 5 indicating multicollinearity. Leverage was assessed using Cook’s distances, with a threshold of 1 indicating high leverage. All statistical analysis was carried out using RStudio V4.1.2 (R Core Team, 2021). Sample distribution of SF-6D scores with kernel density (in red) and a normal distribution (in green) with sample mean (.576) and standard deviation (.074) (N = 182).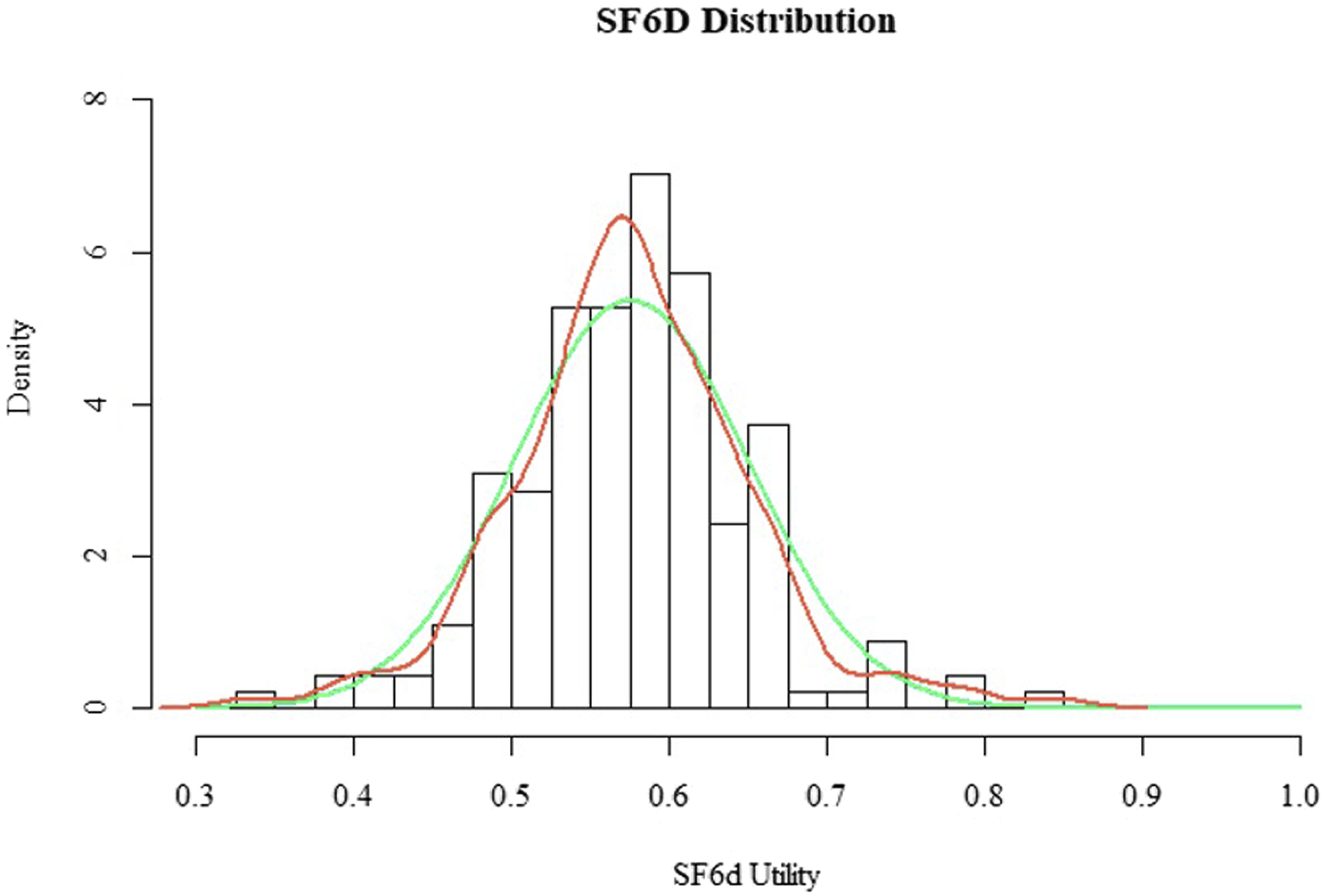
The Research Ethics Board of Western University approved this study.
Results
Sample Characteristics (N = 182).
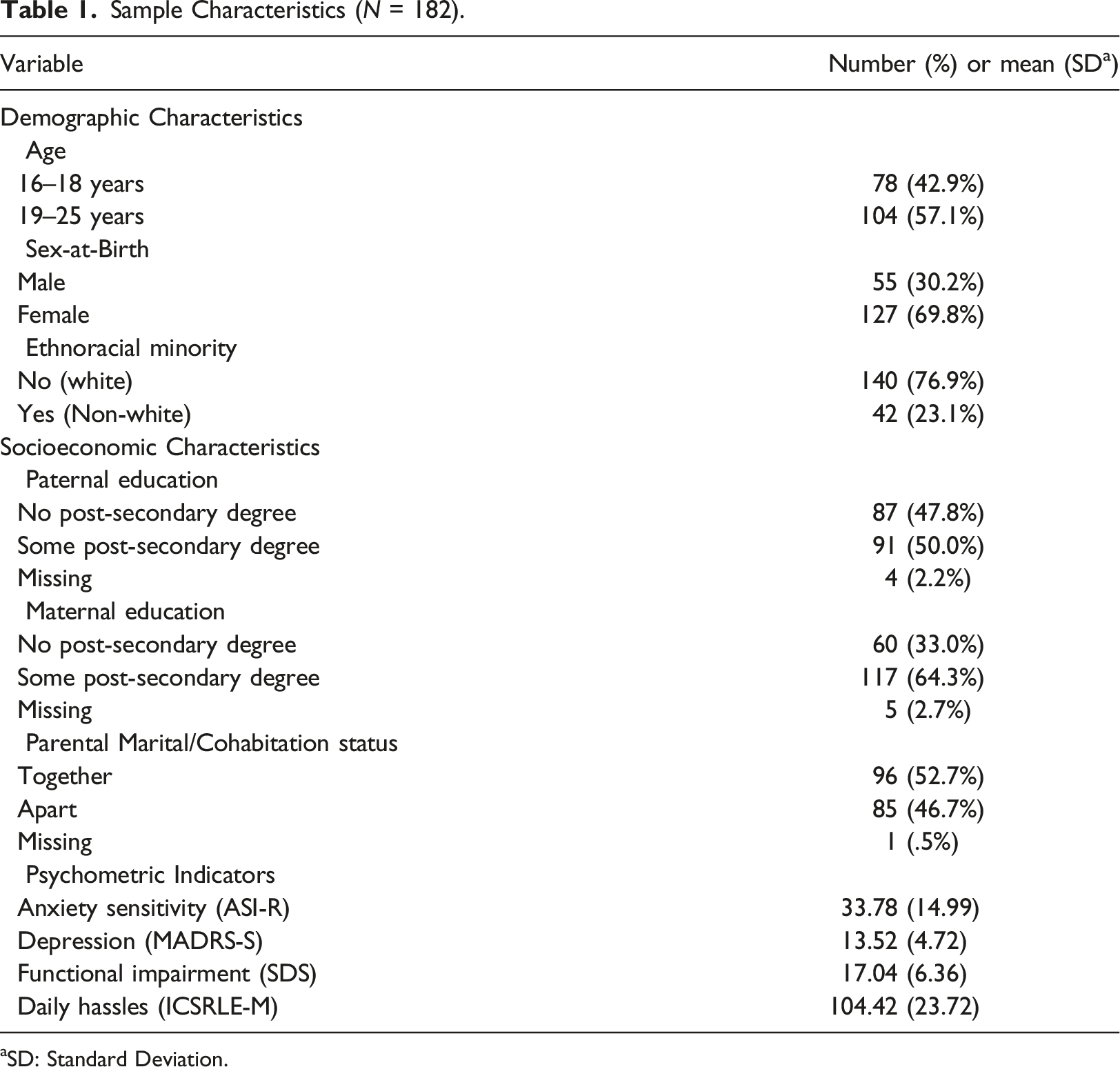
aSD: Standard Deviation.
Sample means (95% CI a ) for scores Derived From the 36-Item Short Form Health Survey (SF-36) (N = 182).
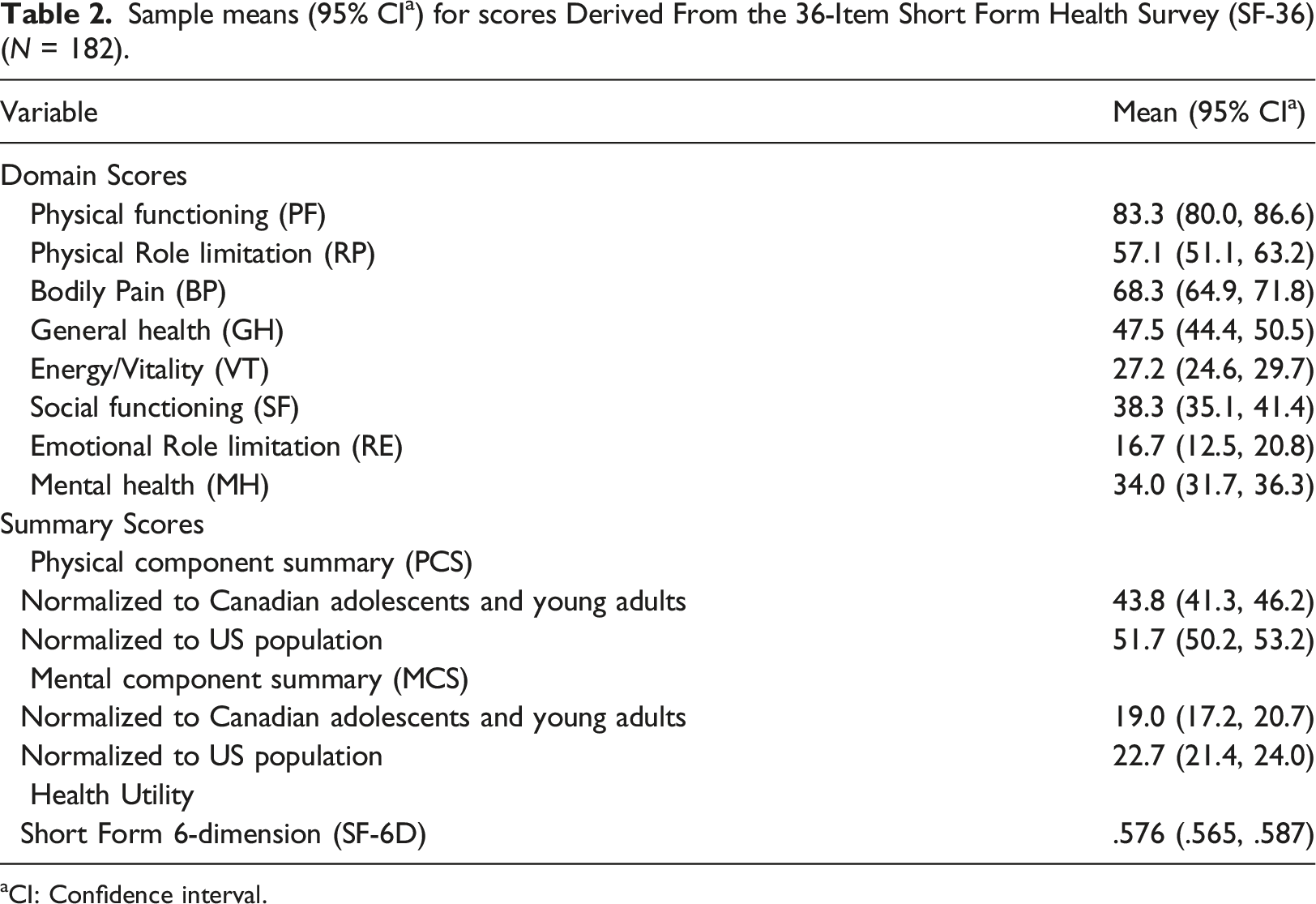
aCI: Confidence interval.
The SF-6D utility was normally distributed in our sample with a thin-tailed distribution (Figure 1). Our sample had a mean SF-6D utility of .576 (95% CI 0.565-.587) (Table 2).
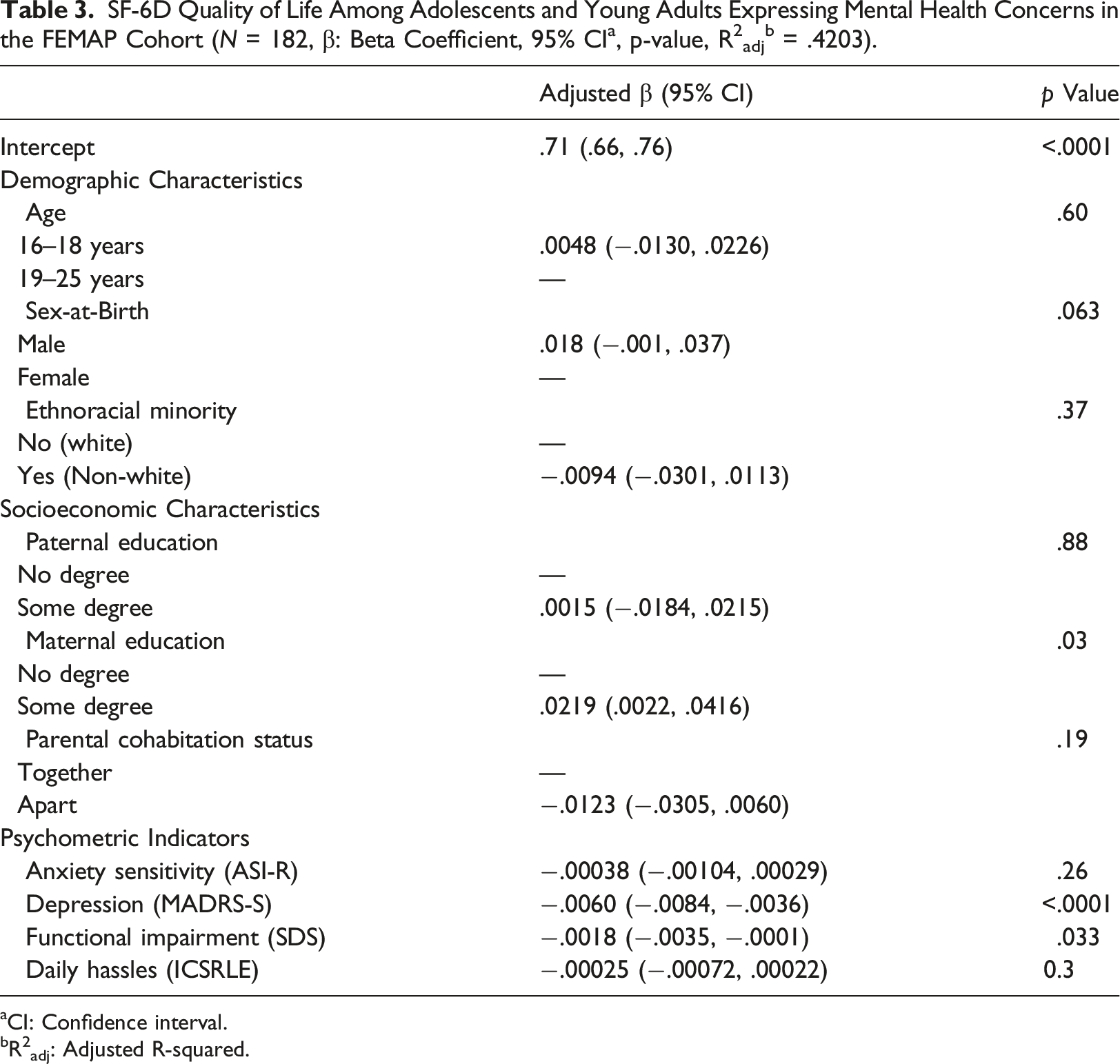
aCI: Confidence interval.
bR2adj: Adjusted R-squared.
In this model, maternal level of education, MADRS-S depression scale, and functional impairment (SDS) were significantly associated with SF-6D utility. A 10-point increase in a participant’s MADRS-S and SDS scores were associated with a .060 (95% CI 0.036-.084) and .018 (95% CI 0.001-.035) decrease in SF-6D utility, respectively. Maternal post-secondary education was associated with a .022 (95% CI 0.002-.042) increase in SF-6D utility.
Discussion
Our study of 182 AYAs seeking care for mood and/or anxiety concerns at a specialized psychiatric clinic showed significant reductions in health-related quality of life and health utility compared to population norms. In multivariable regression analysis we also found significant associations between utility measures of quality of life and maternal education, depression, and functional impairment. While past studies have considered the impact of mood and anxiety disorders on HRQOL and computed SF-6D population norms for AYAs (Hopman et al., 2009; Abdin et al., 2020; Chong et al., 2012; van den Berg, 2012), this is the first study to investigate HRQOL in a cohort of adolescents and young adults seeking help for mental health concerns, as far as we are aware.
In comparison to studies in similar age groups, our sample showed substantial deficits in the SF-6D utility. In the UK, population norms for the SF-6D utility were .843 (95% CI 0.837-.850) and .819 (95% CI 0.813-.826) for 16-19 and 20–25 year olds, respectively (van den Berg, 2012). Compared to that population, our sample had a much lower SF-6D mean of .576 (95% CI 0.565-.587). While comparison to the UK cohort is not ideal, such a large deficit in HRQOL in a cohort of AYAs who are seeking care is evidence of significant impairments and suggests the need for accessible and effective early intervention mental health care programs, including those that allow self-referral, such as that implemented at FEMAP (Osuch et al., 2019). Non-physician and self-referral did not appear to lead to overinclusion of individuals seeking help at FEMAP who did not warrant specialized psychiatric services (Osuch et al., 2019). This has implications for early intervention models of mental health care.
Our cohort of AYAs had not yet been diagnosed by FEMAP clinicians, yet our utility measures are consistent with previous research showing impaired SF-6D utility in clinical cohorts with diagnosed mood and anxiety disorders. In a UK population-based study, van den Berg (2012) found individuals with MDD to have a mean SF-6D utility of .641 (95% CI 0.633-.648) relative to a population mean of .791 (95% CI 0.789-.793). In a cohort of Singaporean adults, Abdin et al. (2020) found generalized anxiety disorder, major depressive disorder, obsessive compulsive disorder, and bipolar disorder to be associated with a decrease in SF-6D utility of .136, .097, .058, and .060, respectively. Our analysis shows that deficits are evident in younger individuals who are seeking care and who, consequently, could be at risk for substantial lifelong disability due to mental illness.
In the absence of information on household income, it is difficult to interpret our findings related to maternal education. The exact mechanism that led to a significant association between HRQOL and maternal education is unclear. Parental post-secondary education can be a marker of financial security and other economic factors, like employment and income, have been found to be associated with SF-6D utility (Chong et al., 2012; Coleman et al., 1966). A community-based longitudinal study involving the French GAZEL youth cohort found low parental income to be associated with worsening mental health (Melchior et al., 2010). Melchior et al. (2010) found that odds of psychological difficulties were higher for both families experiencing decreasing income (OR: 2.44, 95% CI 1.24-4.81) and families with persistently low income (OR: 1.83, 95% 1.10-3.06), relative to families with persistently high or intermediate income over an eight year follow-up. Our analysis revealed an association between maternal education and HRQOL, but no association between paternal education and HRQOL. Swartz et al. (2017) found maternal, not paternal, post-secondary education to buffer against amygdala activity in response to stress. Their study found that in participants whose mothers did not have post-secondary degrees, threat-related amygdala activity predicted depression and anxiety following stressful life events.2 Thus, maternal education may be independently associated with health utility through mental health resilience or may be associated through correlation with financial security.
Strengths and limitations
Our study has several strengths. We analyzed data from a cohort of adolescents and young adults seeking mental health care for the most common mental health concerns and in the early stage of their illness. We collected detailed demographic and socioeconomic information in addition to symptom severity scores and validated psychometric indicators. This allowed us to build a model that not only considered indicators of mental health but also assessed possible contributions of demographic and socioeconomic factors to HRQOL. In building our regression model, we were attentive to model validation and fit, assessing floor and ceiling effects, and ensuring model assumptions were not violated. Very few cohort studies have reported on this age group. As far as we are aware, this is the first study to demonstrate seriously impaired HRQOL in a population of early stage psychiatric treatment-seeking AYAs with mood and/or anxiety concerns and to identify key contributing factors to HRQOL in this group.
This study also has several noteworthy limitations. Our cohort is composed of AYAs who exhibit treatment-seeking behaviors. As a result, we are unable to make statements about AYAs who have not sought treatment for their mental health concerns. However, the population of AYAs seeking care is clinically relevant with significant implications for health services planning. The cross-sectional design of the study precludes us from inferring causality as we can only observe associations among factors. We were also limited in the factors that could be included in our model as we did not capture information on all relevant social determinants. While this study was consistent with past literature in analyzing sex as a covariate associated with HRQOL, we were unable to investigate the association between HRQOL and gender explicitly, since those data were not collected. The modifications to the ICSRLE also precluded us from exploring any association between sexual activity and HRQOL.
Our cohort was composed of a moderate number of individuals who did not identify as white. However, we were limited in our ability to analyze the association between ethnoracial minority status and contribution to HRQOL. Despite having 14 individuals who identified as “Mixed”, we decided against analyzing them as a single group. Each of the other ethnoracial categories had fewer than ten individuals. Missing data imputation was based on the assumption that missingness was completely at random. This assumption may not have been valid because all of the individuals with missing parental education were from families where the parents were apart. These individuals may have been unaware of the level of education of the other parent. In addition, parental marital status and level of education are imperfect proxies for parental income, a measure that we did not have. We were unable to find Canadian normative data for the SF-6D utility in this age group, which limits our ability to compare the HRQOL of our sample to the Canadian general population.
By dichotomizing age, we are leaving potentially important information out of our linear regression model. This was done to allow comparison of our findings to population norms in the existing literature, which are reported by age group. Nevertheless, age was analyzed both as a dichotomous and continuous variable (not reported). When age was treated as a continuous variable, there was no statistically significant association with SF6D utility in the multivariable model.
Conclusion
Our findings suggest that adolescents and young adults seeking psychiatric care for mood and anxiety concerns, prior to extensive psychiatric treatment, have considerably impaired health-related quality of life. The findings underscore the importance of reaching adolescents and young adults with mental health concerns with targeted early intervention. They also illustrate that allowing self-referral does not lead to overinclusion of individuals not in need of care. Intervening early has the potential to significantly reduce years lived with low quality of life or disability, which would provide overall benefit to society and reduction in lifetime burden of patients within the health care and social welfare systems in particular. Further studies that monitor changes in quality of life over time and, most importantly, response to treatment can better inform optimal care for mental illness amongst adolescents and young adults.
Supplemental Material
Supplemental Material - Health-related quality of life among adolescents and young adults with mood and anxiety concerns
Supplemental Material for Health-related quality of life among adolescents and young adults with mood and anxiety concerns by Ayman A Kazi, Elizabeth A Osuch, Michae Wammes and Ava John-Baptiste in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgments
All authors extend their gratitude towards the staff at FEMAP without whom this project would not be possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the London Health Sciences Centre, Schulich School of Medicine and Dentistry, University of Western Ontario, Lawson Health Research Institute, St. Joseph’s Health Care, Canadian Depression Research and Intervention Network (CDRIN), London Health Sciences Foundation and the Innovation Fund of the Alternate Funding Plan of the Academic Health Sciences Centres of Ontario (INN13-008).
Data availability statement
The data in this article are unavailable due to a lack of informed consent from study participants.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.