
Abstract
This study investigates the self-reported impact of children’s psychiatric disorders on their siblings and assesses what forms of support such children most value. We used a qualitative research design with open interviews to stimulate children between 8 and 15 years old to talk about their experiences living with a brother or sister with a psychiatric disorder. Their stories were analysed within a hermeneutic phenomenological framework in order to identify narrative themes and interpret the meaning of shared experiences. From our analysis, nine shared narrative themes emerge. Overall, siblings report feeling conflicted about adapting their lives to their brother’s or sister’s disorder and signal a need for personalized attention from parents. They also indicate that being involved in the care for their brother or sister helps them to better understand their behaviour. Finally, siblings reveal that, in their experience, formal, protocolized forms of support foreground family problems and stress. Thus, we recommend to involve children in the care process; to acknowledge their personal needs and conflicts; and to be mindful of the style of support: help offered in an informal or playful way, instead of formal and protocolized, could be a more effective way of meeting siblings’ needs.
Keywords
Introduction
Worldwide around 13.4% of all children and adolescents have psychiatric disorders (Guilherme et al., 2015) and many of them grow up with siblings. Growing up with a brother or sister with a psychiatric disorder can have important consequences for children: the sibling relationship has a major influence on personal development of brothers and sisters (Boer, 2012; Dijken, 2013) – in a negative as well as a positive sense. On the one hand, the undiagnosed siblings are at risk of also developing mental problems resulting from adversities in their social functioning, school performance or psychological well-being (Boer, 2012; Mascha & Boucher, 2006; Naylor & Prescott, 2004; Pit-Ten Cate, 2000; Verhulst, 2015). Recent research affirms an increased prevalence of psychopathology in siblings of children with mental health problems (Ma et al., 2020); in a similar vein, growing up with a brother or sister with a developmental disorder may affect siblings’ empathy skills and theory of mind ability (Eyuboglu et al., 2018). On the other hand, living with a brother or sister with a psychiatric disorder can also result in increased maturity, improved patience, and better social skills (Meadan et al., 2010; Okma et al., 2015).
It is generally agreed upon that siblings of children with a psychiatric disorder benefit from additional support (Cox et al., 2003; Moyson & Roeyers, 2012). Thankfully, several options for help have already been identified. Parents, first and foremost, play an important role for guidance and support (Boer, 2012; Okma et al., 2015). Support from other family members can further ‘buffer’ the impact of living with a child with a psychiatric disorder (Giallo & Gavidia-Payne, 2006). There is also a (limited) choice of professional help, such as support groups and training. Although there is a growing body of literature on effects of sibling support groups in a psychiatric context, these studies often focus on specific conditions (Jones et al., 2020; Tudor & Lerner, 2015). Additionally, these researchers emphasize that more research is required to best address the needs of siblings.
Existing research investigating the consequences for siblings of children with a psychiatric disorder has been mainly concerned with children with an autism spectrum disorder (Eyuboglu et al., 2018; Mascha & Boucher, 2006). More importantly, most research focuses on reports by parents and does not acknowledge the siblings’ own perspectives (Carel & Györffy, 2014; Meadan et al., 2010). An exception is the work of Moyson & Roeyers, who examined personal stories of siblings by conducting in-depth interviews in order to assess their quality of life (Moyson & Roeyers, 2012). The authors indicate that analysis of such stories can help to meet the needs of siblings.
Despite existing insights in the effects of living with a child with a psychiatric diagnosis on its siblings, then, little is known about what the personal stories of the latter indicate about their experiences, what they require, and how researchers and health-professionals can benefit from such stories. The objective of this research, therefore, is to acknowledge the perspectives of children with a brother or sister with a psychiatric disorder by focusing on their self-reported experiences and needs. Our aim is to offer a qualitative analysis of stories of children with a diagnosed brother or sisters and to trace thematic patterns that emerge in these stories. Our study is part of the Stories Database Psychiatry project (Verhalenbank Psychiatrie) of the Utrecht University Medical Centre, in which personal narratives of psychiatric patients, relatives and professionals are collected and analysed with the aim to improve patient care (Verhalenbank, n.d.). In this study, we collected narratives of siblings of children with a psychiatric disorder in order to assess the impact of having an affected brother or sister. There is growing evidence that young children are indeed able to report accurately on their experiences if given the opportunity and when using questions at their level of understanding (Moyson & Roeyers, 2012). Accordingly, the goal of our research is to explore which forms of support siblings point out to be helpful (or unhelpful) to them and why, so that forms of support might be best aligned with their needs.
Method
Participants
We included individuals through purposive sampling, as we wanted to gain knowledge about comparable experiences related to specific psychiatric and family-related conditions. Therefore, we only included children between 8 and 16 years, with a brother or sister diagnosed with a psychiatric disorder and younger than 18 years. Participants were recruited between March 2017 and March 2018 in two ways: written invitations were sent to parents from children hospitalized in the child psychiatric day clinic of the University Medical Centre Utrecht; and information folders were presented to parents attending lectures on developmental disorders organised by the same institution in 2017.
If siblings were diagnosed with a psychiatric disorder themselves, they were excluded. The specific diagnoses of the brothers or sisters of these children were not always unproblematically comparable in themselves, as there are distinct differences between, for instance, ADHD and PDD NOS, but as our interest was with the communalities in the siblings’ experiences, we included children with brothers or sisters diagnosed along a spectrum of psychiatric disorders.
Characteristics of the children with a psychiatric disorder.
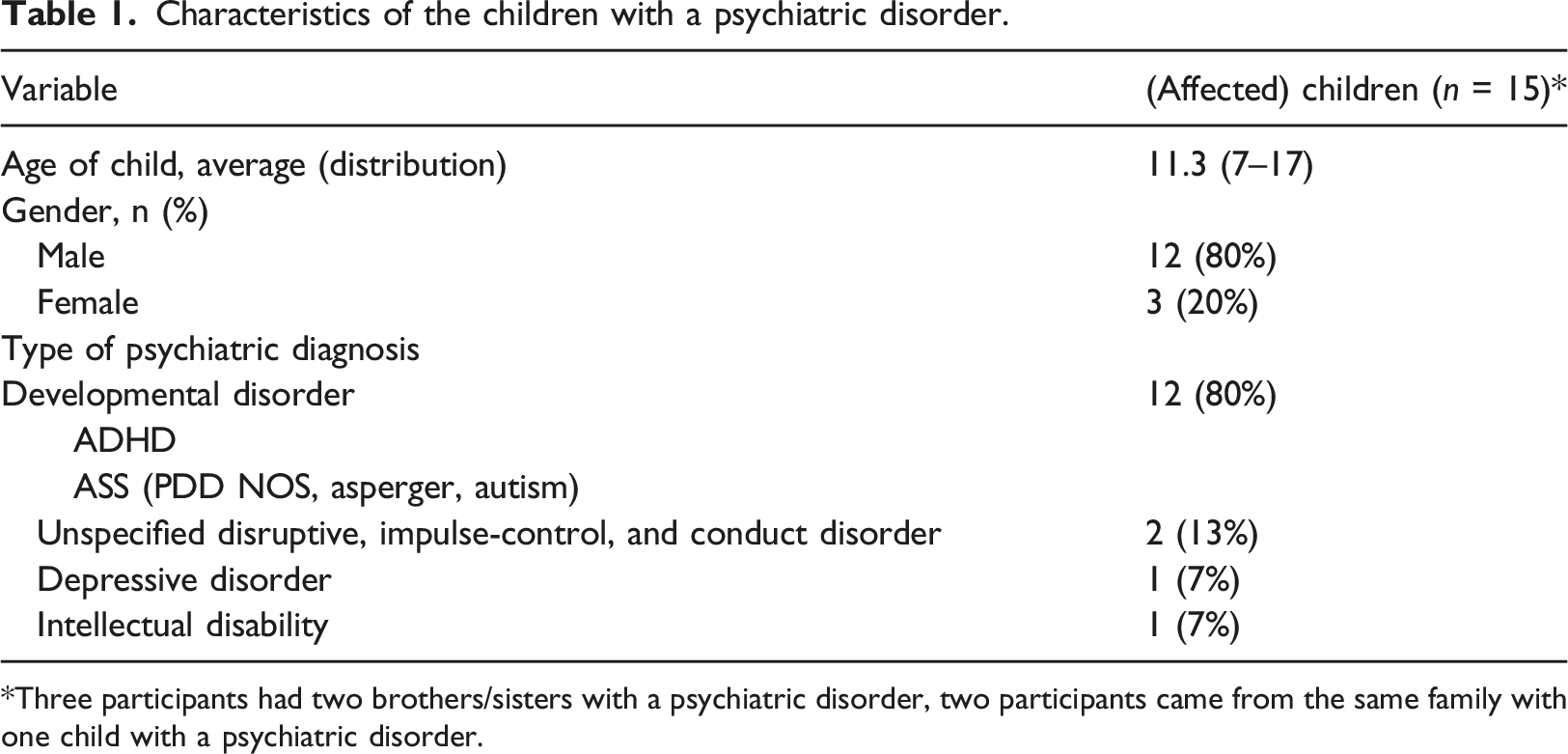
*Three participants had two brothers/sisters with a psychiatric disorder, two participants came from the same family with one child with a psychiatric disorder.
Data collection
We conducted in-depth, unstructured interviews with the participants in Dutch. We chose a qualitative research design, as described below. Several measures were taken to create a feeling of trust with the participants, as this is essential when interviewing children (Moyson & Roeyers, 2012). Siblings were given the opportunity to choose an interview location where they would feel most at ease. Furthermore, an open topic list was used, giving participants the opportunity to suggest their own topics. Interview started with open, personal questions (e.g. ‘What makes you happy?’, ‘What are your wishes?’) so that children felt at ease before talking about their relationship with their brother or sister. Interviews lasted a maximum of 60 minutes. The interviews date from 2018 as that this project was carried out in the context of (voluntary) internships and is quite time-consuming by nature. Nonetheless, it is safe to assume that the collected data is still relevant, as there have been no fundamental changes to the diagnosed condition or to the health-care context.
Data processing and analysis
Interviews were recorded and transcribed by medical students. The transcripts were analysed in a qualitative method based on hermeneutic phenomenology. Hermeneutic phenomenology is a commonly used method to interpret the meaning of interviewees’ experiences It aims at at identifying aspects of subjective experiences as well as evaluating and interpreting their meaning (Lindseth & Norberg, 2004; Manen, 2005; Ricoeur, 1976). Our assumption, then, is that an hermeneutic-phenomenological analysis of personal stories offers access to how individuals experience and evaluate life conditions. By singling out aspects of experiences as recounted in specific sections of a participant’s narrative and comparing them to related experiences in other sections of the same participant’s narrative, and subsequently to experiences as recounted by other participants, recurring and shared ‘themes’ begin to emerge. This way, the individual narrative can be analysed as offering insights into shared experiences. Previously, this method has been used to study narratives of parents with children with a psychiatric disorder (Pejlert, 2001) and to interpret experiences of siblings of children with autism and intellectual disability (Moyson & Roeyers, 2012).
Our analysis consisted of three phases. First, an initial or ‘naïve’ reading of the transcripts resulted in a preliminary understanding of the overall narrative. Secondly, recurring structures were identified and coded. The text of the transcript was subsequently divided into ‘meaning units’ – text parts revolving around specific experiences. By comparing the (individual) ‘sub-themes’ in the meaning units amongst the different interviews, overarching, shared ‘main themes’ could be identified. Thirdly, all meaning units, subthemes and main themes where continuously validated against the background of the results of the previous analytic phases. This resulted in a circular process (see Figure 1) that ensured that the findings of each stage of the analysis aligned with the previous stages. After a first full analysis, the text was read by a second assessor. All analyses and codes were discussed amongst the research group members. Data collection and analysis.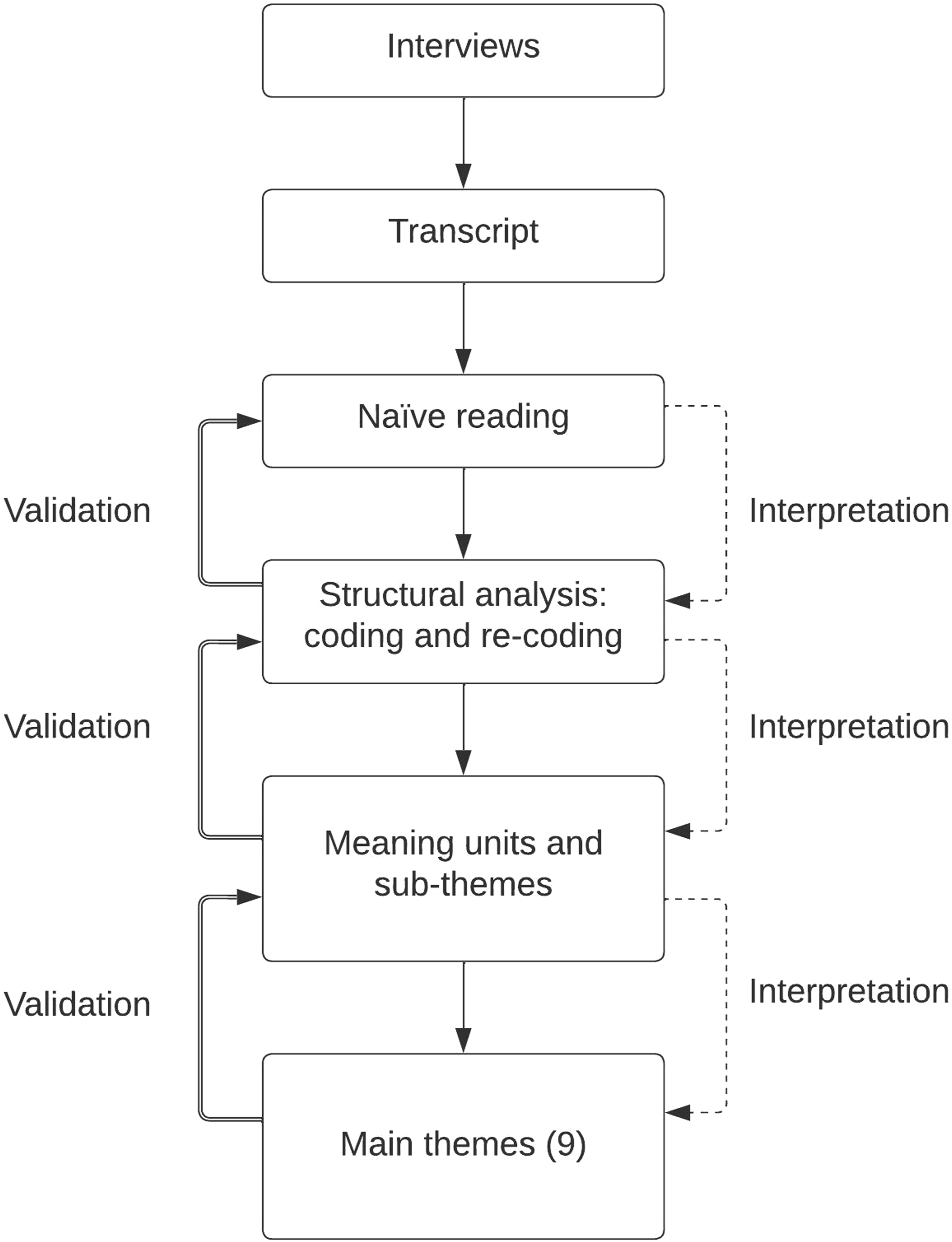
Interpretation and results
The naïve reading resulted in a general understanding of the overall structure and content of the narrative. In most stories, siblings mentioned the difficulties in living together with their brother or sister with a psychiatric disorder, emphasizing their struggles to deal with conflicts and unpredictable behaviour. They mentioned positive experiences too, as well as coping mechanisms, but the emphasis was on difficulties and challenges. Notably, the stories expressed feelings of ambivalence: the siblings expressed their appreciation of growing up together, but also indicated that this required continuous adjustment, as they felt that they needed to prioritize their brother or sister’s needs. The overall message of their stories was that siblings require attention and support from loves ones or relatives and do not necessarily value professional help.
The first structural analysis focused on narrative categories (e.g. metaphors, common stop words, protagonists and temporal perspectives) (Peljert, 2001). The siblings and their brother or sister were the stories’ protagonists. Co-actors were parents or other family members. The temporal perspective was mostly the present. The future tense was mostly used to describe hopes and wishes for a positive sibling relationship. Occasionally, siblings talked about the past to describe the development of their relation with their affected brother or sister. Most participants preferred the use of first-person, but some switched to second-person when discussing difficult situations or expressing wishes and desires. Participants used vague expressions such as ‘or so’ and ‘etcetera’ when describing disrupting behaviour, their parents’ approach to it or their own feelings related to it. Some younger participants gave evading answers or did not reply to specific questions, mainly when talking about their own (negative) feelings or experiences directly related to their brother or sister: ‘Do you find it difficult to talk about R.?’... ‘Yes, I think that is kind of difficult... [Silence]... Uhm, I am not very used to it yet.’ (E.,8 years old)
In the second structured analysis all transcripts were coded with meaning units that captured recurring experiences. This resulted in sub-themes that capture returning and shared stories about events (e.g. ‘Disrupting behaviour’), emotional impact (e.g. ‘Processing difficult feelings’), or impact (‘Influence on everyday choices’).
Main themes and sub-themes.
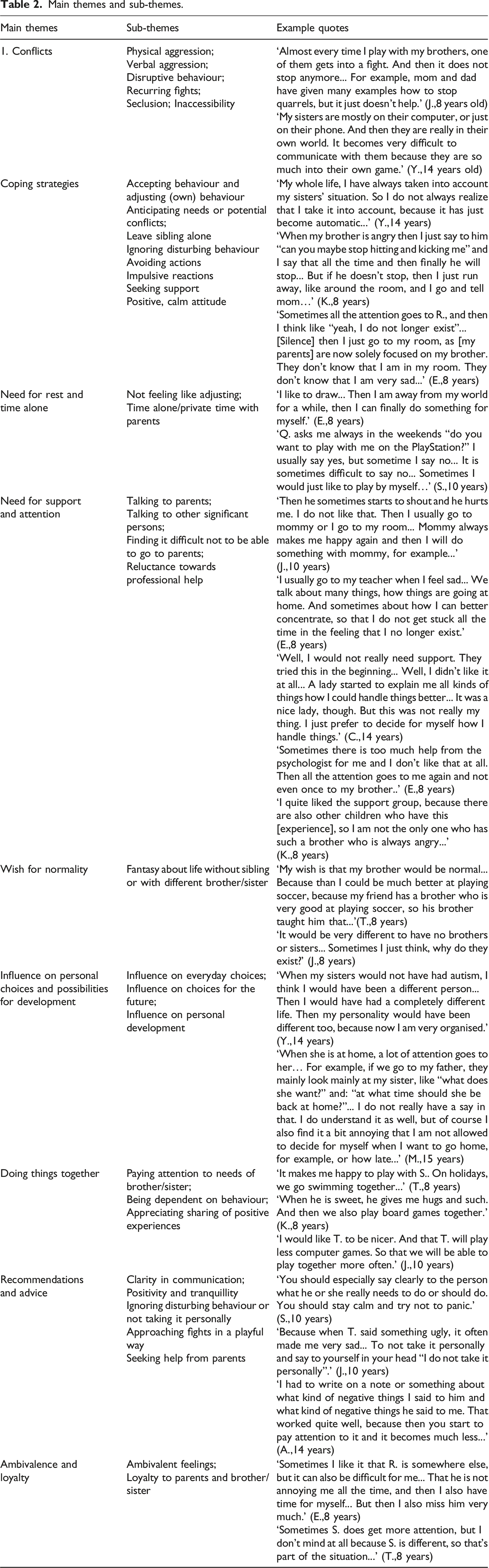
In sum, we found sub-themes that could be clustered into nine main themes related to experiences of ‘Conflict’ (e.g. ‘Physical aggression’), descriptions of ‘Coping strategies’ (e.g. ‘Leave sibling alone’), indications of a ‘Need for rest and time alone’ as well as a ‘Need for support and attention’ (e.g. ‘Talking to parents’), expressions of a ‘Wish for normality’ (‘Fantasy about life without sibling or with unaffected brother or sister’), descriptions of the ‘Influence on personal choices’ (e.g. ‘Influence on everyday choices’), indications of the importance of ‘Doing things together’ (e.g. ‘Appreciating sharing of positive experiences’) and the children’s own ‘Recommendations and advice’ (e.g. ‘Clarity in communication’).
Together, these themes indicate the narrative shared by the siblings: how they experience living with an affected brother or sister, what needs they have, and in which ways these needs can be best addressed. In all stories siblings mentioned conflicts, often involving verbal or physical aggression. These confrontations cause negative emotions. Siblings show a remarkable level of reflection on how to avoid or solve conflicts. They attempt to adjust themselves in behavioural, cognitive and emotional ways. Siblings are able to reflect on coping strategies: these include seeking support from parents, ignoring the difficult behaviour, or adjusting their behaviour (see Table 2).
Siblings express a need for time alone and private activities with their parents. They acknowledged attempts to treat all children equally, but find that their parents are not always successful in doing so. However, they realize and accept that their brother or sister simply needs more care. Since they feel loyal to their family members, they are willing to adjust.
To be able to talk about their problems and emotions is very important for siblings in order to feel supported. They prefer to talk to their parents, but also accept support from other significant persons. Interestingly, they generally do not indicate a specific need for professional help, such as a parent mentor or psychologist: they would rather play than have a formal conversation. Additionally, they mention having had positive experiences with sibling support groups, in which help is offered in a playful way, for instance through a game. Advice that they would offer other siblings is to maintain a patient and calm attitude, to communicate clearly or to ignore disrupting behaviour (see Table 2).
Sometimes, siblings fantasize about what their live would be like without their brother or sister. They then come to reflect on how their brother or sister influences their lives, both in positive and negative ways. Overall, the stories demonstrate a certain longing for ‘normality', for a way of living that does not foreground that their family situation is ‘different’ and problematic.
Discussion
In this study, we found that siblings of children with a psychiatric disorder were able to describe and evaluate their experiences: they showed a high level of reflection on the impact of living together with an affected brother or sister.
The interviews created a safe space for detailed exploration of the siblings’ experiences. From their stories, nine main themes emerged. Some of the themes are confirmed by previous research: these include the need for private time and sharing or exchanging experiences with others (Moyson & Roeyers, 2012).
Additionally, the narratives revealed that living with an affected brother or sister has a profound impact on siblings. They experience ambivalent feelings towards their brother or sister and find themselves in an emotional conflict. They love their brother or sister, but they struggle with their disruptive behaviour. Simultaneously, they feel guilty about having feelings of frustration and anger. The narratives indicate that this emotional conflict often results in strategic adaptation of behaviour to maintain stability and avoid stress. Consequently, as described in previous research (Cox et al., 2003; Ross & Cuskelly, 2006), the siblings develop a variety of coping strategies. Paradoxically, the need for a ‘normal’ and uncomplicated family life requires ‘artificial’ adaptation from the siblings and intense reflection on the interaction with their brother or sister.
Being used to adapting to their brother or sister, and pleasing their parents, the siblings often ignore their own needs, which can lead to negative emotions. Unfortunately, in choosing family activities, the wishes of the affected child tend to be prioritized. Consequently, siblings miss private time and undivided attention (Hastings, 2014).
Finally, this research leads us to formulate four recommendations to better meet siblings’ needs. First, it is important to stimulate siblings to talk about their feelings. It is well-known that when children have an understanding of their family situation, they will be more effective in processing their experiences and expressing their needs (Boer, 2012). However, we found that siblings were often not used to talk about feelings. They struggled with describing challenging situations and negative emotions related to their affected brother or sister. Talking about these experiences can cause stress or anxiety (Moyson & Roeyers, 2012). Additionally, they are used to deprioritize themselves (Okma et al., 2015). They come to ignore their own emotions, with a risk of developing mental problems (Garley & Johnson, 1994). Our advice to offer a listening ear to siblings of children with a psychiatric disorder, then, applies in the first place to the parents and relatives. In addition, health care professionals as well as other people involved should give siblings opportunities to talk about their feelings and should acknowledge their needs.
Second, we recommend to involve siblings in their brother or sister’s treatment and offer them relevant psychoeducation. Previous research has shown that siblings find it easier to accept the disorder of their brother or sister if they have a better understanding of it (Garley & Johnson, 1994; Moyson & Roeyers, 2012). When siblings know how to deal with the situation, they tend to experience a better quality of life. Simple tips on how to respond to disrupting behaviour can already contribute to a less frustrating and more effective way of communicating. It is also important to undertake joined activities, as these have a positive effect on the brother-sister relationship (Boer, 2012; Moyson & Roeyers, 2012).
Third, it is important to offer close, dedicated support from parents or caregivers. Even though other significant persons are mentioned (e.g. extended family members, friends), siblings point out that they prefer talking to their parents and having one-on-one activities with them. Research shows that open communication between parents and children is an important preventive factor for the development of psychological problems in siblings (Moyson & Roeyers, 2012; Pit-Ten Cate, 2000), while insufficient availability of parents can lead to negative emotions (e.g. feelings of not being important enough) in children. Understandable, many parents experience difficulties adequately dividing the attention between their children (Delfos, 2009; Okma et al., 2015), but we found that some parents of the interviewed sibling admitted to underestimating the impact of the family situation on their non-diagnosed children. Thus, it is crucial that parents do not to underestimate the importance of being available for siblings.
Fourth, we suggest to be careful with respect to offering professional – that is, formerly ‘marked’ as professional – help, since this can be counterproductive when siblings experience too much attention and feel that their problem gets too ‘loaded’. Interviewed siblings did mention positive experiences with support groups focussing on sharing or exchanging expression through playful activities. Realizing that the problems they face are not unique, the siblings experience recognition, shared awareness and acknowledgement of their feelings (Evans et al., 2001; Naylor & Prescott, 2004; Okma et al., 2015). In general, it is important to give children the opportunity to play with each other and offer help in an informal way. This way, they can learn how to better process and appreciate their personal experiences (Moyson & Roeyers, 2012; Naylor & Prescott, 2004).
Limitations of the study
The number of participants in this study was relatively small (n = 13) and in the affected siblings there was a variety of diagnoses. However, siblings’ responses to questions related to support needs were highly comparable. Additionally, some researchers argue that in smaller, preliminary, explorative studies, saturation – the point at which no new themes are observed in the data – can be achieved with eight to 10 participants (van Geelen et al., 2013). Another limitation was that participants signed up through their parents: some parents refused to allow their child to participate, resulting in possible selection bias. Additionally, we mainly talked to siblings of children with a developmental disorder or behaviour disorder so we missed other diagnosis like psychotic disorders or depression. Furthermore, there was a relatively wide age range of siblings (8–15 years) and the sample size was too small to compare the different age groups. Finally, all participants were recruited in the region of Utrecht, which could cause bias as the mental health system might be organized differently in other regions.
Future research
The results invite follow-up research on the facilitation of support for siblings of children with a psychiatric disorder, as well on the role of family members and of professionals in the healthcare sector and social care. Since siblings’ support need may be interrelated with the characteristics of the disorder of their brother or sister, future research could focus on children with other disorders than those included here or in other research, e.g. depression or anxiety disorder. Additionally, children’s needs may be influenced by their developmental stage, cultural factors and socio-economic environment: all these are factors of interest for future research. Finally, the results of this study, in line with extant research literature, point out the possibly increased efficacy of professional help when offered in an informal or playful manner. Despite these hopeful results, more research is needed to ensure such interventions will be sufficiently valid and reliable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.