
Abstract
Background
Literature reviews revealed no existing research on family narratives of living with multigenerational persistent physical symptom (PPS) conditions. The current study examined the personal and family narratives of one such family, from a relational/systemic perspective.
Method
This research employed a qualitative research design, specifically using narrative methodologies to explore the experiences of a single family comprising two parents and their three children. All the children and their mother had a diagnosis of Ehlers–Danlos syndrome (EDS) but are specifically afflicted with PPS. The father is in good health. Using narrative inquiry, the family members were interviewed together and then individually. The interviews were audio-recorded, transcribed and analysed using narrative analysis in NVivo.
Findings
Overarching narratives were stories of loss and sacrifice and stories of family unity. An exploration of the family’s negotiation of roles and identities is presented in the context of stigmatised illness.
Discussion
Novel findings are presented in the context of the central role of the mother, the importance of family cohesion and the impact to family life resulting from living with stigmatised illness. Lastly, clinical implications and future research ideas are discussed.
Introduction
Medically unexplained symptoms (MUS), or the patient-preferred term, ‘persistent physical symptoms’ (PPS), is an umbrella term for a cluster of conditions commonly used in healthcare settings (Chalder et al., 2019), including chronic fatigue syndrome (CFS), irritable bowel syndrome (IBS), persistent pain, fibromyalgia and non-epileptic seizures (NES). These conditions are often stigmatised and misunderstood, partly due to uncertainty about biological aetiology (Hart, 2014). Even when told that these conditions are not ‘all in their head’, patients are often left feeling they are a nuisance or wasting medical professionals’ time (Edwards et al., 2010).
Research on this topic often focuses on individual perspectives such as the healthcare professional (HCP), the adult, the parent or the child. There is limited research on family perspectives of PPS. PPS conditions induce challenges for families so a more relational, family perspective is warranted. Research has highlighted that, within families where children have PPS, there is often evidence of unexplained illness elsewhere in the family (Garralda, 1996). However, this area is poorly understood, and family-based research is important as it has potential to shift the focus of attention from the individual to understanding the meanings of phenomena at the family level (Gilgun, 2005).
Garralda (1992) discusses the role family functioning plays within the development and maintenance of somatic symptoms in children, highlighting that familial relationships with health may relate to development of ‘somatic symptomology’ in the child(ren). Research has explored the relationship between parental unexplained illness and children’s emotional and psychosocial functioning, concluding that there is an intergenerational and interactional relationship at both parent and child level which may contribute to PPS development (Craig et al., 2002; Gilleland et al. 2009). Families often report feeling let down by medical systems and reject psychological perspectives for their children’s PPS, which may influence the way families make sense of their health experience (Kozlowska et al., 2012). Research also suggests that identity formation, specifically the uptake of stigmatised identities, can be attributed to the responses of family members and HCPs, highlighting that there may be a need for a more relational, familial approach (Sowinńska & Czachowski, 2018).
When illness is present in a family, family members often report higher levels of closeness suggesting the experience of being unwell brings families together, even when they feel misunderstood by others (Garralda, 1996; Roy, 1982). Rosland et al. (2012) review articles on the impact of family interactions and illness responses concluding outcomes are positively affected by strong family cohesion and self-reliance on the family unit. Conversely, family dysfunction has also been reported either historically or currently in families with PPS who are high users of healthcare services (Dwamena et al., 2009).
There is little research exploring the relational component to these conditions and how families make sense and live with PPS from a relational perspective. Additionally, it has been reported that the roles and family scripts that are drawn upon in the context of health and illness play an important part in the way the family interact with one another in a health context (Byng-Hall, 1988). While it is understood that PPS may be present within more than one generation of families, this has not been explored qualitatively and little is known about families’ experiences (Shraim et al., 2013).
There is limited understanding of how families with PPS may construct collective family identities and navigate different role relations in the context of PPS. Further exploring this using qualitative methodology would enrich understanding of families’ experiences of PPS, with clinical implications for how HCPs can best support them. Therefore, the aim of this research was to explore how a family with multigenerational PPS construct their identities and navigate role relationships.
Methodology
Design
This research used a single-family case study design, which allowed for an in-depth exploration of both the unique individual narrative accounts and how family narratives are co-constructed in a specific context (Crix et al., 2012; Wells, 2011). More specifically, narrative methodologies allowed exploration of how members related their understandings, within the local and broader socio-cultural context of their construction (Hunter, 2010). Service user involvement was a key aspect of the research design, supported by a consultant family (with several PPS conditions). Aspects of recruitment, consent, information sheets and interviewing were discussed and co-created with the consultant family, incorporating discussions on ethics, language and health-related logistics, for example, appropriate interview length for people experiencing PPS.
Consent, confidentiality, data management, recruitment and other ethical considerations were explored and addressed using the integrated research application system. This project received full ethical approval from the London NHS Research Ethics Committee (REC approval reference: 19/LO/1697).
Recruitment
Purposive sampling was employed to recruit a participant family, where PPS was present within both the parental and child generations. Recruitment took place at a specialist hospital in London, which supports adolescents with complex medical needs.
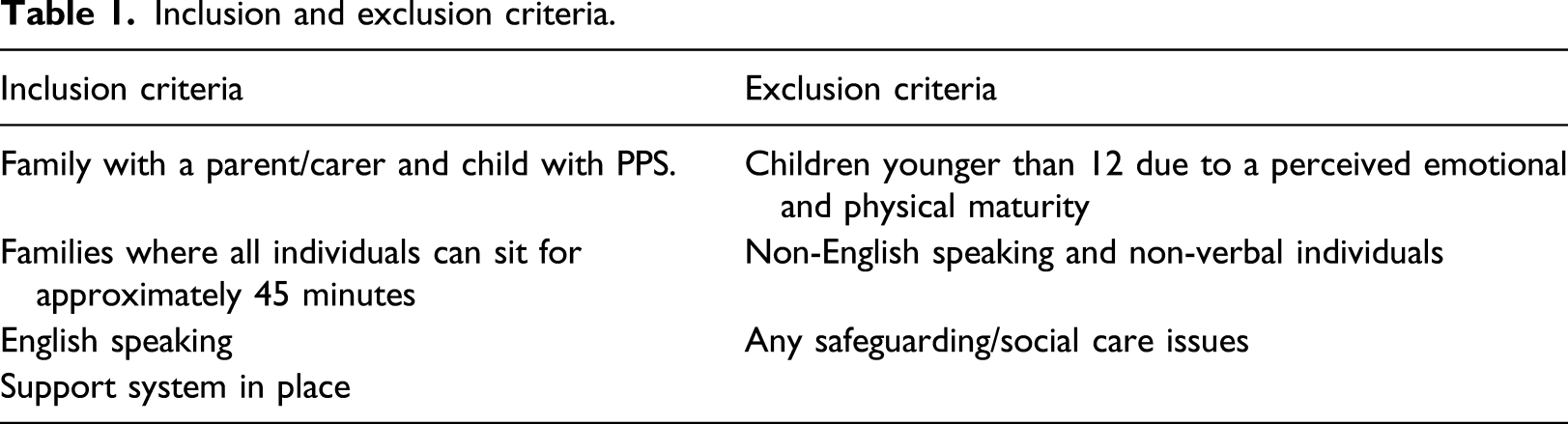
Inclusion and exclusion criteria.
Participants
The participant family were white British/Irish (see Figure 1 for family genogram). The mother and all three children have a diagnosis of Ehlers–Danlos syndrome. The family members’ information (including pseudonyms and changed ages) is summarised in Table 2. Family genogram. Participant demographics.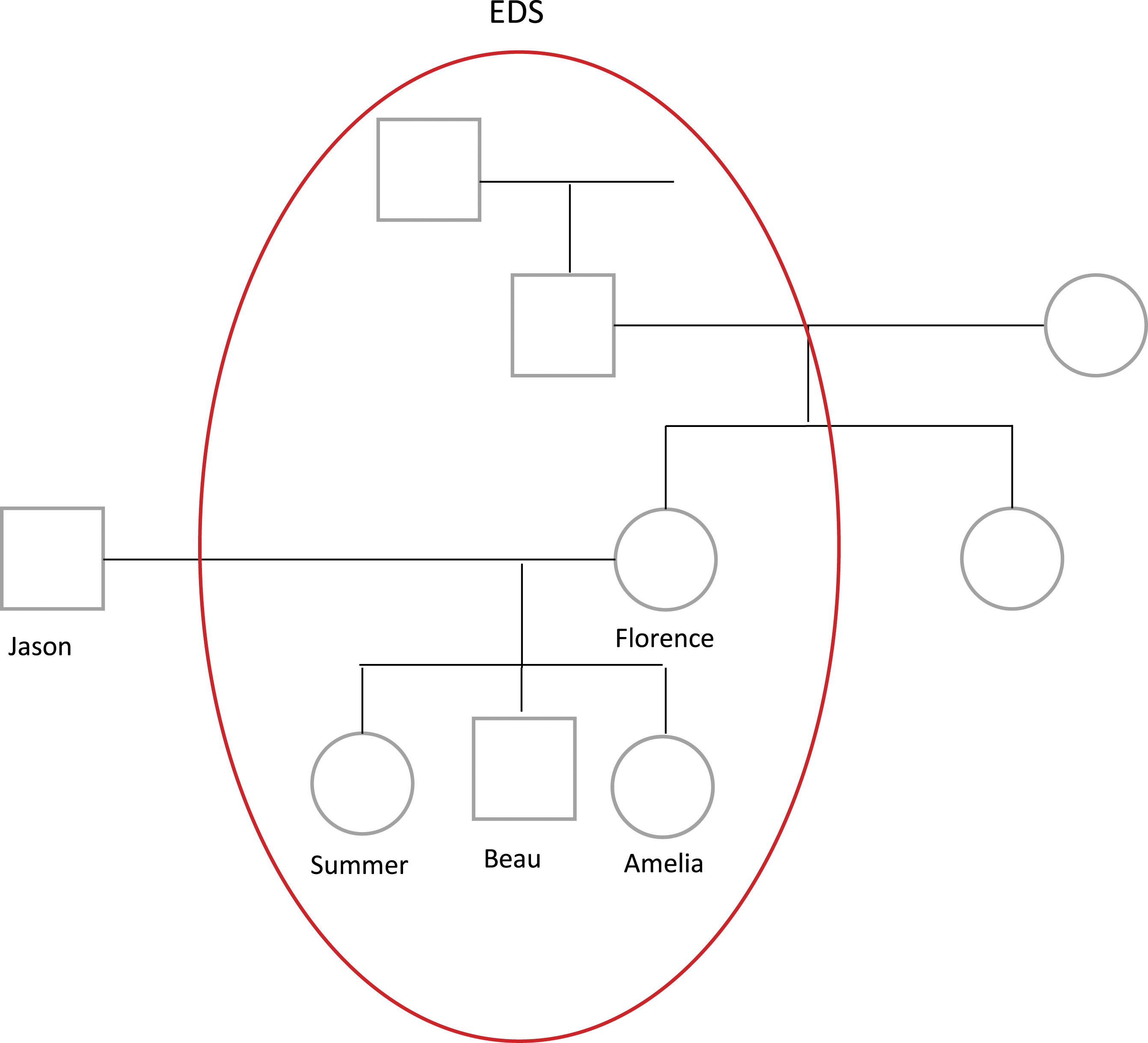
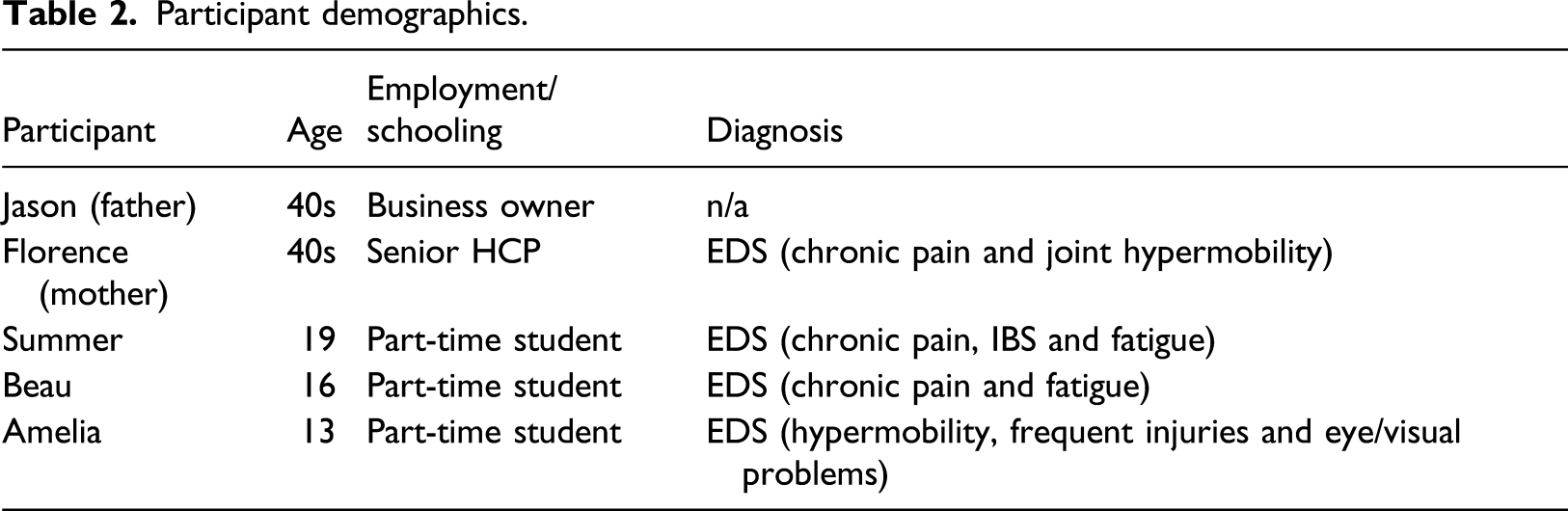
EDS is defined by NHS choices as ‘a group of rare inherited conditions that affect connective tissue’ and it falls within the spectrum of hard-to-diagnose and often misdiagnosed medical conditions (Gazit et al., 2016; NHS Choices, 2019). Hypermobile EDS, the most common classification, is characterised by joint hypermobility, fatigue, pain, digestive problems and dizziness (NHS Choices, 2019). People with EDS and PPS, experience comparable challenging journeys to diagnosis, similar stigma in response to their symptoms and similar experiences of being misunderstood (Bennett et al., 2019).
Once the family had consented to participation, a semi-structured group interview, followed by individual interviews, were conducted via online video calls, due to the context of the COVID-19 pandemic. The group interview was conducted using multiple devices, with Jason and Summer sat together in one room, Florence and Amelia sat together in another and Beau, alone in his bedroom. The interviews were conducted during the early months of the first wave of the COVID-19 pandemic, and confidentiality was explicitly discussed and ensured by the family and the primary researcher. Each interview lasted between 36 and 70 min, generating a total of 313 minutes of recorded material. Participants were asked open questions that facilitated story telling such as ‘can you tell me about a time when illness entered your lives?’ (sample interview schedule in supplementary material). Further questions that prompted more detailed storytelling to aid a deeper discussion were asked (Kvale, 2007; Wells, 2011). Interviews were recorded on an audio device, and field notes were written to take note of non-verbal communications. Within this methodology, it is understood that narratives told are a co-construction between interviewer and participants, located within the interview context. Recorded interviews were transcribed by the researcher as close to the interview experience as possible and texts managed using NVivo.
Analysis
Interview recordings and transcripts were subjected to narrative analysis, guided by Riessman (2008) and Wells (2011). Repeated listening, reading and note-taking focused on different levels of narratives: content, structure, performance and context (see Davies & Harré, 1990, Esin et al., 2014, Riessman, 2008 and Wells, 2011 for detail).
Each of the interviews was analysed separately by the primary researcher, a clinical psychologist, taking note of how the different storylines and themes were constructed based on the process highlighted above. Narratives and themes were compared for similarities and differences across the interviews, which allowed identification of overarching narratives. The different narratives and themes were shared with the research team to consider alternative understandings, explore researcher blind spots and ensure methodological rigour (Bailey, 1996; Tracy, 2010). The research team comprised the four co-authors of this study specifically, four female clinical psychologists all from a white, European background. Each member of the research team had different personal and professional relationship to family illness as well as bringing different ‘lenses’ dependent on their life stage, for example, being a parent or being a child to an unwell parent.
Findings
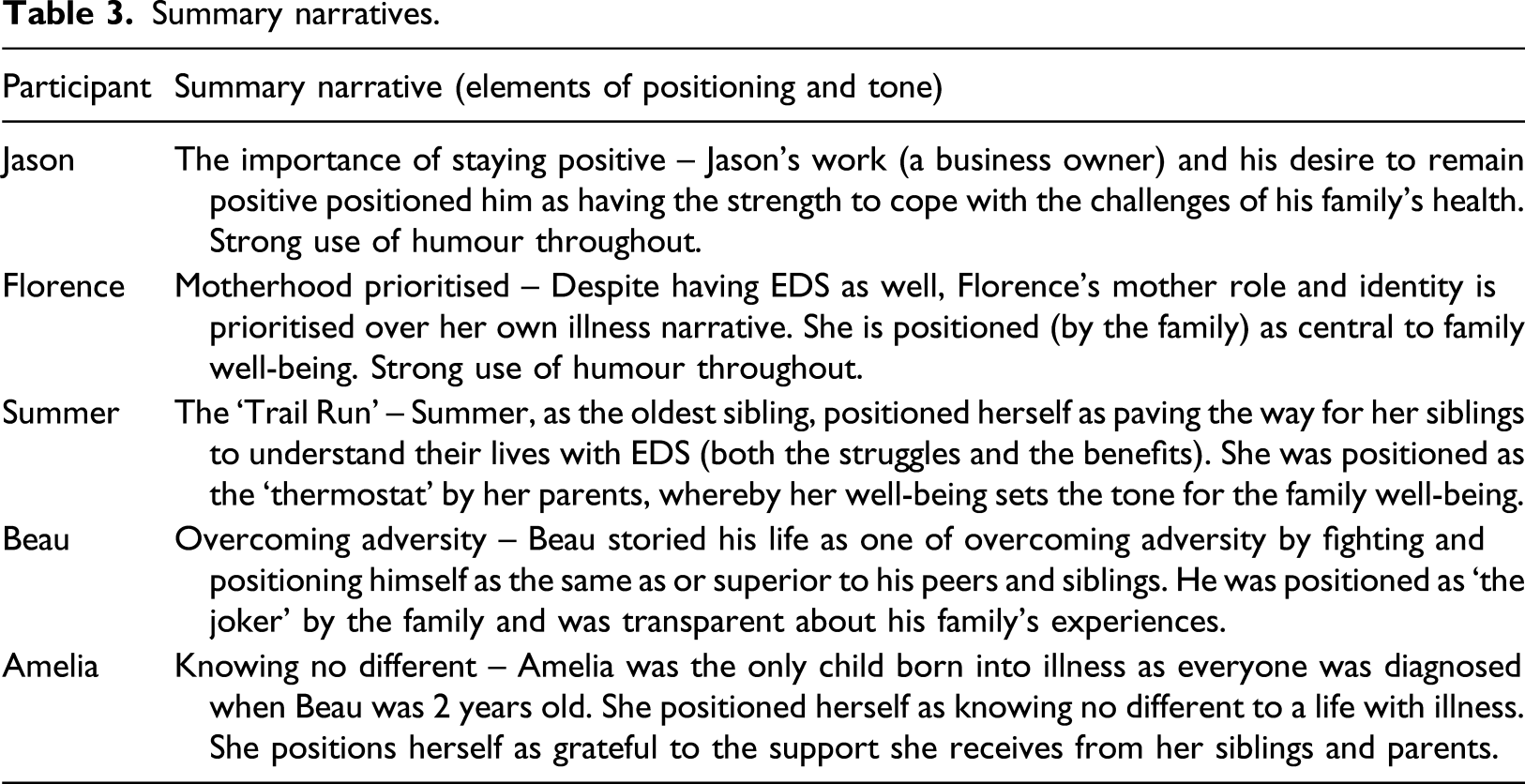
Summary narratives.
Across the interviews, two main collective narratives were primarily drawn on: ‘They can’t have that type of a life’ – Stories of Loss and Sacrifice; and ‘The bond between us, it doesn’t really falter’ – Stories of Family Unity.
Story 1: ‘They can’t have that type of a life’ – Stories of Loss and Sacrifice
Each family member draws on the idea of loss and sacrifice in different ways. This story is most frequently drawn upon by the parents where they appear to lament what their children and family life might have been without illness.
Jason began by highlighting the ‘reality’ of his situation is never far away when he states: ‘for our kids(.) it’s °kind of tough° (.) knowing that they °can’t have F: ‘you know Summer was
This narrative is also reflected when Beau draws on the story of loss, specifically focussing on his sadness for his parents’ experience because he and his siblings are unwell when he says: B: ‘you really want them to (.) have the same
Beau continued to draw on stories of a loss of opportunity through illness and appears to speak on behalf of his family, when questioned about what happens when illness enters their lives. He responds with: B: ‘I mean (.) I guess we didn’t really get to do everything that we normally would do (.) so like it has sort of stunted the (.) opportunities that we might have had (.) if we were more
Summer reflected on her own experiences of loss. In response to Beau citing that things had improved for him over time, she drew on counternarratives of things getting harder as she got older. She said: S: ‘especially during this UCAS period (.) […] it was like every- was around like “well I can put DofE (.) I’ve been charity working” this sort of stuff (.) […] I don’t have anything to °write down° (.) I think for me (.) I noticed that there is more difference between me and my peers (.) I think as I’ve got on (.) I’ve struggled more’.
While loss and sacrifice has been explored in this family’s narratives, they also narrate stories of family unity which is discussed next.
Story 2: ‘The bond between us, it doesn’t really falter’ – Stories of Family Unity
Throughout all the interviews, the family members frequently drew on narratives of family unity; a finding that speaks against prevalent discourses of ‘family dysfunction’ and PPS (Dwamena et al., 2009).
Beau initially draws on this narrative early in his individual interview when he explained the importance of coming together as a family at challenging times. When asked how his family copes when faced with a future of worsening health (e.g. when he saw wheelchair bound children with EDS), he prioritised family closeness to feel safe ahead of an uncertain future: B: ‘we went back up to the hotel room and we just sat around […] it was almost like having that (.) family moment’.
Amelia appears to strengthen the narrative of family unity when she talks about how people with PPS are often misunderstood. Feeling understood by your family is noted to be beneficial in the context of feeling misunderstood by others (Årestedt et al., 2014). She explained: A: ‘it’s also quite nice to know that you’ve always got some people that understand what you’re going through’.
Summer, however, appears to offer a counternarrative in her individual interview when she describes her struggle with the lack of escape from illness (‘it can be quite difficult when all three of us (.) you know (.) we’re all coping with the same thing’). This counternarrative was not expressed by anyone else in the family.
Across the interviews, it was discussed how Summer struggled the most with social relationships, which would lead her to isolate herself in her room. In response to this, Beau explained that when Summer is feeling well: ‘it’s almost like the whole morale of the house is up (.) you know (.) we’re all having fun (.) m-we’re all enjoying ourselves’.
When Jason, the only well member of the family is asked about his experiences of his whole family being unwell, he continues to strengthen the family unity narrative when he demonstrates that despite illness, they have each other and that is most important: J: ‘our life’s good in a lot of ways (.) we’re all very well connected (.) that’s the most important thing […] as long as we have that (.) we can get through most of this’.
This reliance on each other to be unified is further explored by Jason in the group interview when speaking about the consequences of either external pressures or illness flare ups on the family: K: […] is there anyone that perhaps has more flare ups or more kind of becomes more unwell than others in the family? J: ‘[…] once somebody’s down (.) it’s very easy to drag everybody down (.) so it’s important that you know that when it does happen (.) we try to stay close in as much as we possibly can’.
He both strengthens and resists the narrative of family unity, when he speaks about the how they can lift one another up or drag each other down. This is seen in the literature which proposes when a family faces ‘extrafamilial’ pressures, strong familial interpersonal skills help the family cope (Pardeck, 1989).
The family were also challenged in the group interview to think about if the closeness would be present if illness was not part of their lives, and when Summer began to respond with: S: ‘I don't know (.) because when you think about it (.) you know (.) if we were out socialising more–’.
Jason interrupts her and speaks with expertise to offer a counter narrative when he says: J: ‘I-I-I think I can I can probably answer that a little bit better because from my own point of view’.
He draws on his experiences growing up with a sister he describes as ‘mentally handicapped’ which resulted in ‘the bond in my family’s really strong’. He has a foundation of closeness which he would want in his family, illness or not. His interruption of Summer may have been his way of strengthening his counternarrative protecting the image of family closeness that may not be there if they were healthy. If Summer had finished that sentence, it might have challenged an aspect of his strongly held family identity.
How do families construct their identities?
Throughout these stories, the concept of ‘the ill person’ unsurprisingly recurs, with different individuals taking up different positions in relation to this. Florence, Beau and Summer, all reject traditional ‘illness identities’ in different ways, with Florence appearing to favour a more ‘can-do’ identity, Beau privileging identities based on strength and Summer favouring identities focused on maturation. In contrast, Amelia’s talk makes less explicit resistance to traditional notions of illness identity. It may be significant that her family members’ stories regularly position Amelia as different, in that she was ‘born into’ illness, to a family who were already familiar with the hereditary and expected nature of EDS symptoms.
Additionally, throughout the interviews, traditional gender identities appear to come through with Jason’s role as the breadwinner and provider for the family. Beau, being the only male child, also prioritises his male identity, through comparing himself to his peers and focussing on training and exercise. Florence, who also works, uses her talk to construct strong gendered identities and roles relating to women in the home, for example, raising the children. F: ‘there’s more that goes on in our household than (.) in other households (.) a lot of work in keeping our f- our children (.) afloat (.) it’s a good job I don't have to work full time’.
Florence’s identity as a mother often triumphs above her illness identities, signifying that her illness comes second to her children’s (Vallido et al., 2010).
Additionally, the children frequently rejected their child identities. Parents of chronically unwell children report a loss of the child identity in the context of illness (Smith et al., 2013). Amelia appears to reject her child identities when she describes her experiences of interacting with doctors and not understanding when they ask her questions about her condition. A: ‘I never really understood because the doctors would asked me questions and I was only like three or four (.) but my mother was answering them as well (.) but then the doctor would always be like “so what do you think about that?” I didn't really understand it cos, I didn't really know what like fatigue or things meant’.
These experiences may be mirrored by her siblings and would demonstrate the need to detach themselves from their child identity to feel more comfortable around doctors and appear more knowledgeable about their condition.
All identities presented were co-constructed through the researcher–participant interaction within the specific interview context.
Role Relationships
The familial, collective response to illness is dictated by how the family’s roles and relationships change within this family system. Amelia describes how each of the family members navigate the sick role:
A: ‘if we’re feeling well (.) if one of us is like feeling well (.) or we’re all feeling a bit ill but we’re all okay […] one person’s like really well (.) and we all kind of just feel well (.) so it kind of makes everyone happy (.) and then if we’re ill (.) we all kind of feel a bit like (.) ill really’.
Despite it being apparent that illness is ever present within this family’s life, each of the unwell family members navigate the sick role in different ways. It appears that when the children are ill, the parents move into the role of keeping the mood light. With this, Florence describes Jason as their ‘whistling Rufus’ and brings his ‘happy soul’ to the family to keep the tone light. He reported in his interview that he does things ‘to keep a nice joyful (.) air around the place’.
It appeared evident from all the interviews, the most challenging time for this family was when Florence had her hip replacements, meaning that the ‘mother role’ was temporarily left vacant. It was swiftly filled between the children with them all commenting: S: ‘I did the washing and stuff like that↑ but it was like we tried to keep (.) doing stuff that Mum would do’. A: ‘I would make sure that the dinner was done and I make sure that the- (.) […] I was kind of charge the kitchen (.) my brother would do the bins and the hoovering (.) my sister would make sure the house is B: ‘we all had to sort of erm work together to kind of fill the hole when Mum wasn't there’.
Summer storied that she negotiates several roles; she is the ‘trial run’ and the one that keeps an even temperature in the family. It appeared that Summer felt pressured to be a certain way for her siblings: S: ‘I think Beau and Amelia very much erm (.) look up to me because I’m obviously the oldest sibling (.) it’s kind of the way things normally go (.) so I think they look at what I’ve:: done (.) and they try and do bett::er::’.
In the group interview Florence suggested that Summer was ‘a thermostat’ for the whole family. This is built on by Beau when he explains: B: ‘when Summer’s doing good (.) it’s almost like there’s a uplift to the whole family […] Summer’s almost like the catalyst to the right reactions’.
This pressure for Summer to be well to maintain whole family well-being is mirrored in Amelia’s role. Summer described her in the group interview as ‘the happiness pill (.) the vitamin’. She appears to take on a rescuer role of keeping the family healthy. However, Florence commented on the consequences of this role: F: ‘when her symptoms get too much there is a complete change in her when °she is very dark° and (.)
Discussion
This research focused on understanding, through the application of narrative methodologies, how a family with PPS in multiple generations constructed and negotiated various identities and relationships. The findings are discussed in the context of existing literature and the research questions. Lastly, methodological strengths and limitations, as well as clinical implications and future indications, are considered.
Overview
The analysis explored the wider narratives that emerged from the interviews and then focused on how family members co-constructed their multiple identities and navigated changing roles in the context of illness. The findings were co-created through the interaction between the primary researcher and the participants and presented through the lens and context of the researcher. Participants’ positionings of themselves and the researcher also influenced co-constructions of narratives, identities, roles and relationships.
The wider narratives presented across the interviews drew on ideas of loss and sacrifice and family unity. The greatest loss that people with PPS experience appeared to be the loss of social relationships and other social factors external to the family system (Winger et al., 2013). In keeping with previous research (Dirkzwager & Verhaak, 2007; Winger et al., 2013) in which people with PPS report significantly greater social isolation and loneliness compared to their healthy counterparts, the stories of these family members highlight loss and sacrifice, particularly regarding lost opportunities and social relationships.
Family unity was discussed by all family members. This was ever present in their narratives, appearing with little researcher prompting and observed through non-verbal communication. The overarching sense was that their family unity and cohesion was a strong protective factor from further distress. In the researcher–participant interactions, co-constructions of family unity flowed across interviews. The family discussed the times they felt most overwhelmed was when they faced external pressures or when something unexpected happened. Research has shown that family cohesion may be disrupted when family rituals are unsettled (Fiese et al., 2002; Santos et al., 2015). While this family draws heavily on their family unity in shared accounts, research has shown the family members of people with PPS report how their lives, roles and relationships are negatively impacted by the unwell person and their illness (Ashe et al., 2017; Liedberg & Henriksson, 2002). The wider evidence base has documented the challenging reciprocal relationship between PPS and family dysfunction (Dwamena et al., 2009; Edwards et al., 2010). However, this was not case for this family and the findings fit with research undertaken by Garralda (1996), Rosland et al. (2012) and Roy (1982).
The identities prioritised in these stories were illness identities, the rejection of ‘child’ identities and the juggle between a parent, a patient and professional identities. The rejection of the ‘child’ identities is commonly found in children who are chronically unwell. An explanation for this may be due to spending much of their time communicating with adults (in hospitals), they are treated like and can feel like an adult (Kirkpatrick Johnson & Mollborn, 2009; Smith et al., 2013).
Årestedt et al. (2014) found that for families living with chronic illness, there is a daily negotiation of roles and sharing of responsibilities in a way that may not occur in families without ill health. For this family, this focused particularly on the dynamism of the mother role. The role of the mother has been established in the literature but often from a relatively pejorative stance with mother blaming or highlighting the role that maternal overprotection plays in subsequent PPS in the child (Fisher & Chalder, 2003). The novel finding from this research was the way the mother role was centralised for this family and how this was negotiated amongst the family members when Florence’s illness worsened. Florence’s story positions her as prioritising her children’s health needs over her own, which has been seen by Vallido et al. (2010) as they discuss how unwell mothers’ prioritisation of their mother role comes at a cost to their own health.
Overall, while there are some findings in this study that were in line with the current research, several novel findings are also presented relating to the experiences of a family with multigenerational PPS. The novel findings explored by this research are the centralised role of the mother, the importance of family cohesion as well as the impact to family life resulting from living with stigmatised illness.
Strengths and limitations of the research
Anderson (2010) suggests that some of the strengths of qualitative research are that issues can be researched in depth, draw on human experience and permit an iterative process to knowledge conception. The main strength of this research is that it provided an opportunity to explore an under-researched area, specifically with PPS conditions and even less researched with EDS. This study provided an opportunity for the family to discuss their unique life events in the context of their illness and puts forward a novel perspective of the narratives of a family where PPS is in multiple generations.
However, it is important to reflect on the limitations that are inherent in research. This research initially focused on PPS diagnoses and the uncertainty associated with the unique experiences of these family members. However, the participant family had a family history with a diagnosis of EDS. While EDS is a rare diagnosis which may be misunderstood by the medical profession (Bennett et al., 2019), it is nevertheless a diagnosis – in contrast to the experience of other PPS sufferers living with the uncertainty of any form of diagnosis, and the additional challenges that this can bring. Nonetheless, the narratives constructed by these family members largely resonate with findings from individuals with other PPS conditions. With a single-family case study design, it is not possible to remove the stories of this family from their specific context and their own individual differences, and their experiences may not sufficiently resonate with other family’s with PPS. For this reason, it would be useful to explore the same research aims with a larger participant pool.
Clinical Implications
The relationship between how family members juggle their symptoms, roles and identities in the context of misunderstood illness has been discussed. While it is important to prioritise the dynamic relationship between all these factors, in current NHS frameworks, therapeutic and medical interventions are often offered from an individualistic perspective. Both the negotiation of illness identities and the dynamism of relationships in the context of illness have been documented within this research. For this reason, along with the intergenerational component, clinicians should start to conceptualise people with PPS’s healthcare from a more relational/systemic perspective. Clinicians may be interested in exploring relationships and communication patterns currently and historically, both within and between the family systems and the wider context, along with the protective factors and strength connected to family cohesion and closeness. This may signify the need for an MDT perspective (inclusive of school involvement) when it comes to working with children and families. This may create more room for psychological and systemic interventions to support families as they negotiate multigenerational physical symptoms.
Future Research
As with all ideographic research, generalisability is theoretical (i.e. to allow consideration of resonances with other families living with PPS), and differences – such as cultural and socio-economic contexts – should be explored in future research (Evangelidou et al., 2020). Similarly, alternative family structures (e.g. single-parent, same-sex or adoptive families) would be an important focus, as would the presence of PPS where no additional diagnosis had been made. Lastly, drawing on gendered ideas mentioned above, it may be of interest for future researchers to explore these ideas when the father, opposed to the mother, is afflicted with stigmatised illness.
Final Conclusions
This research set out to explore how families constructed their identities and made sense of their role relationships when both parent and child were unwell with PPS. This research employed narrative methodologies to understand the unique narratives of a single family in which four out of five members were diagnosed with EDS, specifically afflicted by PPS. The analysis showed how the family drew on a multitude of narratives and wider discourses to co-construct their stories, giving insight into the navigation of roles within the family, and their relationships with illness identities, parent and child identities and gendered identities. Lastly, clinical implications and further research ideas have been discussed.
Supplemental Material
sj-pdf-1-ccp-10.1177_13591045211033188 – Supplemental Material for Family narratives of lives with persistent physical symptom conditions
Supplemental Material, sj-pdf-1-ccp-10.1177_13591045211033188 for Family narratives of lives with persistent physical symptom conditions by Kimberley Friedner, Wendy Solomons, Halina Flannery and Jenna Harrington in Clinical Child Psychology and Psychiatry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.