
Abstract

Introduction
Just as vascular medicine specialists must incorporate new diagnostics, devices, and drugs into their therapeutic armamentarium to provide the best care for their patients, so too must vascular biologists rapidly assimilate new technologies to continue generating fundamental insights that may lead to transformative therapies for vascular disease. In 2006, Shinya Yamanaka published his Nobel Prize winning work, generating induced pluripotent stem cells (iPSCs) from somatic cells using retroviral vectors to overexpress the stem cell genes Oct 4, Sox2, KLF4, and c-myc (OSKM). 1 We began to generate iPSCs from human fibroblasts, and differentiated them into vascular cells. But rather than using retroviruses (which integrate OSKM into the human genome, potentially causing harmful mutations) we used message RNA (mRNA) encoding OSKM to generate iPSCs. 2 This worked well, and soon other scientists began asking us to make mRNA OSKM for them. When our group moved to Texas, we received a generous grant from the state in 2015 to generate mRNA for cancer investigators. Now, 10 years later, we have generated over 500 unique mRNA constructs for over 150 investigators in Texas and worldwide. We are developing our own mRNA constructs for cardiovascular regeneration. Because mRNA is akin to biological software, encoding any protein or antigen of interest, and because it is rapidly manufactured and less expensive than other biological drugs, it will have broad applications for pharmacotherapy, including for the treatment of vascular diseases.
The RNA revolution is coming
RNA drugs are on the way to becoming the next pillar of therapeutics, joining small molecules, recombinant proteins, and gene and cell therapies. There are over 20 RNA drugs now approved in the US, with over 130 RNA drugs in clinical trials. 3 These RNA drugs include RNA interference (RNAi) drugs that inhibit the expression of a protein, such as small interference RNA (siRNA) or antisense oligomers (ASOs); those that encode a protein such as mRNA, self-amplifying RNA (saRNA), and circular RNA (circRNA); and those that bind to, and interfere with, the action of a protein (RNA aptamers) (Figure 1). There are also RNA drugs (antagomirs) in development that interfere with the action of microRNA (miRNA), which itself suppresses the expression of multiple endogenous mRNAs. In the paragraphs that follow, I highlight key examples of how RNA technologies are leading to the transformation of vascular medicine.
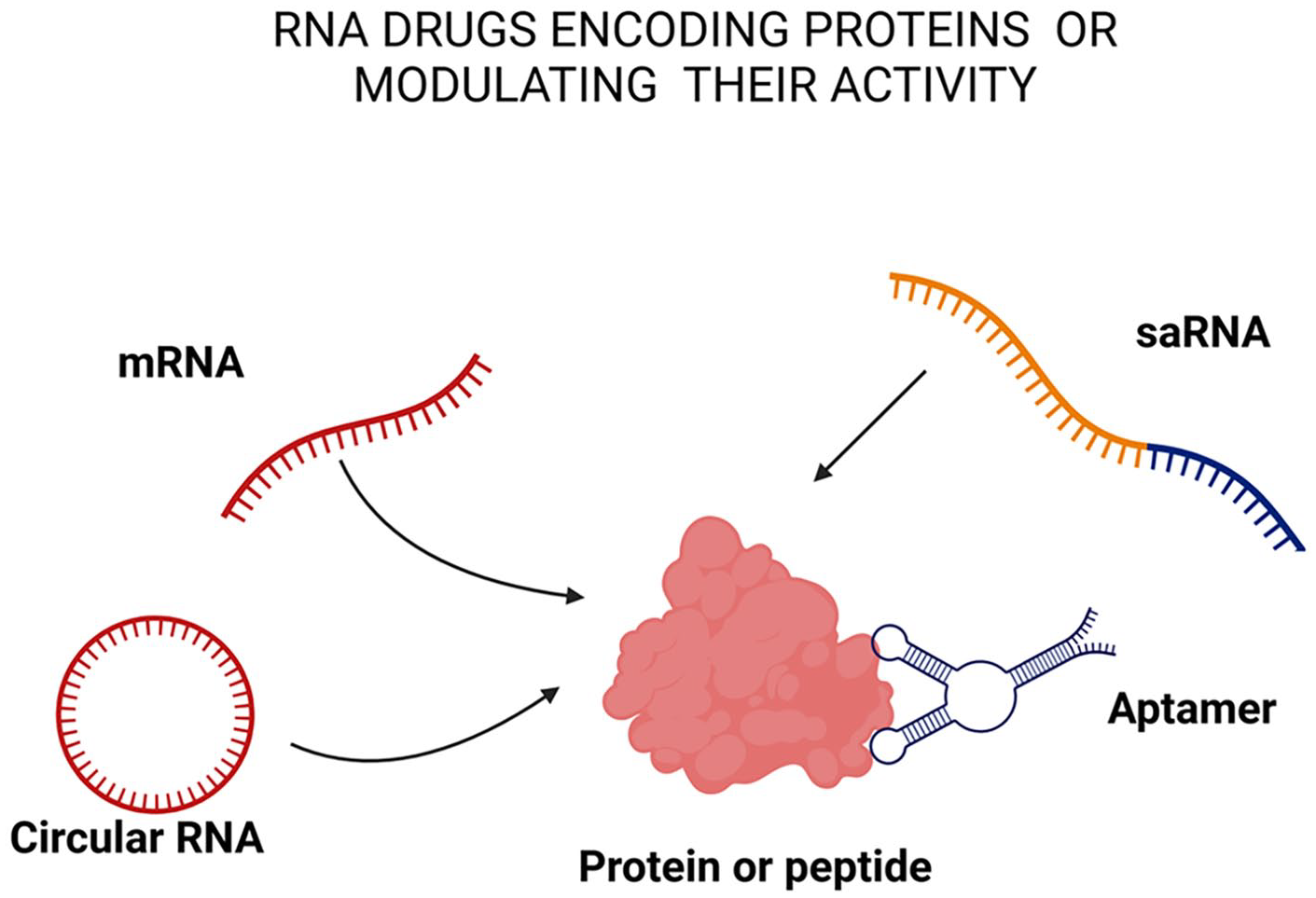
RNA drugs that encode therapeutic proteins or antigens include message RNA (mRNA), self-amplifying RNA (saRNA), and circular RNA (circRNA). These RNA drugs are translated into proteins in the cell cytoplasm. RNA aptamers have high affinity to specific sites on proteins and typically inhibit protein activity.
RNA aptamers
The first of the RNA drugs to reach the clinic was an aptamer directed against vascular endothelial growth factor (VEGF). Pegaptanib (Macugen, Pfizer) was approved in 2004 for the treatment of the choroidal neovascularization that causes ‘wet’ age-related macular degeneration. 4 However, after the development of more effective monoclonal antibodies against VEGF, the use of pegaptanib declined. Currently, several aptamers are under development for thrombotic diseases, targeting coagulation factors such as FIXa. 5 A significant advantage is the ability to rapidly reverse the anticoagulation using an antisense aptamer that binds with high affinity to the anticoagulant aptamer. Aptamers resemble antibodies in their high affinity for a target, but they are much easier to design and manufacture, and they can be directed against any endogenous protein (e.g., receptors, enzyme, cytokine, etc.) for a wide variety of indications, including cardiovascular disease.
RNA drugs as a ‘brake’ on protein expression
The ASO and siRNA drugs generally work by binding to a target mRNA in the cell to accelerate its degradation and thereby prevent its translation into protein (Figure 2). Several of these have been approved or are in late-stage clinical trials for the treatment of hypercholesterolemia. A relevant example of such a drug is the FDA-approved siRNA inclisaran (Leqvio, Novartis). This siRNA drug binds to the mRNA encoding proprotein convertase subtilisin/kexin type 9 (PCSK9) to block its translation. 6 This reduces the expression of PCSK9, which in turn increases expression of the low-density lipoprotein receptor (LDL-R), which lowers LDL cholesterol (LDL-C). Inclisaran is approved for use in patients with atherosclerosis resistant to maximal statin therapy as well as those with heterozygous familial hypercholesterolemia.

Drugs that affect the translation of endogenous mRNA into protein typically include small interference RNA (siRNA) and antisense oligomers (ASOs). By binding to the mRNA they prevent its translation and increase its degradation. Endogenous microRNA (miRNA) binds to many endogenous mRNA constructs. Antagomirs are RNA drugs that bind to the miRNA to prevent its action.
Emerging siRNA drugs to treat vascular risk factors
Following in the path of inclisaran, there are multiple siRNA drugs under clinical investigation to treat hyperlipidemias. 7 Two of these, zerlasiran and olpasiran, each target the apolipoprotein(a) (Apo[a]) protein and thereby reduce lipoprotein(a) (Lp[a]), serum levels of which are otherwise resistant to statin therapy. Plozasiran is another siRNA in late-stage clinical trials that targets apolipoprotein C-III (APOC3) mRNA to reduce triglyceride levels in patients with severe hypertriglyceridemia. Zodasiran targets and degrades the mRNA of angiopoietin-like protein 3 (ANGPTL3) to reduce LDL-C levels in patients suffering from homozygous familial hypercholesterolemia. Designed for patients with hypertension, zilebesiran targets hepatic angiotensinogen (AGT) mRNA, to reduce the expression of angiotensin II, a major vasoconstrictor and pressor. Generally, these siRNA drugs can be administered by subcutaneous administration quarterly or twice annually, which should also improve compliance.
Emerging ASO drugs to treat vascular risk factors
The ASO drugs have been developed against many of the same targets for dyslipidemia. 7 Mipomersen was the first ASO be approved by the US FDA for patients with homozygous familial hypercholesterolemia (HoFH). It reduced LDL-C by targeting the mRNA encoding apolipoprotein B-100 (ApoB-100). However, reports of hepatic steatosis associated with mipomersen led the FDA to withdraw its approval. Pelacarsen is an investigational ASO in phase 3 clinical trials, which is designed to target Apo(a) mRNA, thereby reducing Lp(a) levels. Another investigational ASO is CIVI008, which differs from the other RNA interference (RNAi) strategies in that it is orally administered. This ASO targets the mRNA of PCSK9 in hepatocytes, thereby reducing the production of the PCSK9 protein, increasing the expression of LDL-R, and thereby reducing blood levels of LDL-C.
Stepping on the accelerator with mRNA
As opposed to ASOs and siRNA, which act as a brake on the expression of a protein, mRNA encodes a therapeutic protein or antigen. The importance of this new category of pharmacotherapy was strikingly manifested when mRNA vaccines against SARS-CoV-2 provided an effective solution to the COVID-19 pandemic. At no time in the history of medicine has a drug (vaccine) been developed so quickly, been administered to so many people (5 billion doses to date), with such safety and efficacy.8,9 Within a week of determining the sequence of SARS-CoV-2 in January 2020, the nucleotide sequence for the vaccine was generated. The mRNA vaccine was rapidly synthesized, tested in animals, and by April 2020 was in clinical trials. By the end of 2020, large clinical trials had documented the safety and efficacy of the vaccine, global vaccination campaigns were initiated, and millions of lives were saved. Truly, mRNA had won the day.
The rapid development of RNA drugs is partly due to RNA being a form of biological software. For mRNA, one can simply write the code for an antigenic peptide or a therapeutic protein into the DNA template that is used for the mRNA synthesis. This is a much more direct process than typical drug discovery of therapeutic small molecules which requires high throughput assays and large chemical libraries to screen for hits; orthogonal assays to confirm hits; medicinal chemistry to improve pharmacokinetics; and a complex preclinical testing roadmap to understand absorption, distribution, metabolism, excretion, as well as the off-target effects of the novel small molecule. The mRNA therapeutics also have significant advantages over recombinant proteins, as each mRNA transcript can generate tens to hundreds of the therapeutic protein. Furthermore, it is far simpler to let the cell read the mRNA code to generate the therapeutic protein, fold it properly, and provide the selective and appropriate posttranslational modifications than to manufacture a recombinant protein with the proper conformation and modifications. Furthermore, the manufacturing processes for RNA therapeutics are generally much less costly than that for gene therapies, which are typically delivered by a viral vector. With respect to cell therapies, an exciting development is to improve or generate cell therapies using mRNA to make modifications in a simpler and safer fashion than using viral vectors. In one transformative application, chimeric antigen receptor (CAR)-T cells were generated in vivo using lipid nanoparticles targeting T cells and carrying the mRNA for the CAR. 10 The first proof-of-concept for this approach was successful in targeting activated myofibroblasts in a preclinical model of cardiac fibrosis. 10
By comparison to gene therapy, RNA approaches are safer because there is no risk of genomic integration of the RNA, unless the RNA is specifically designed to do so. However, it is possible to perform genome editing with mRNA. Indeed, Verve Therapeutics has two ongoing clinical trials of a base editing strategy using mRNA. In one case, the guide RNA is directed against PCSK9; in the other trial, the guide RNA is directed against ANGPTL3.11,12 Early data from their clinical trials is promising, with substantial reductions in LDL-C. In addition, because the mRNA is more transient than a viral vector, it may have fewer off-target edits.
To conclude, there are almost limitless possibilities for the application of RNA drugs for the management of vascular disease. Initially, most of these agents will be directed against vascular risk factors, but broader applications are inevitable. RNA is biological software, and the code for vascular health is being written.
Footnotes
Acknowledgements
The author acknowledges the assistance of Ms Renee Kamin who helped to refine the illustrations.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Cooke is the inventor on patents broadly related to the use of mRNA technology for therapeutic cellular reprogramming and rejuvenation, assigned to Stanford University or Houston Methodist Hospital, some of which are licensed to ChromeX Therapeutics, in which Dr Cooke holds equity.
Funding
This work was supported in part by federal grants (R01 HL148338, R01 HL157790; NASA Contract #80ARC023CA002) and funding from the Joseph C ‘Rusty’ Walter and Carole Walter Looke Presidential Distinguished Chair.