
Abstract

Introduction
The 2024 American College of Cardiology (ACC) and American Heart Association (AHA) guidelines for the management of peripheral artery disease (PAD), which were developed in collaboration with the Society for Vascular Medicine (SVM) along with the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR), American Podiatric Medical Association (APMA), Association of Black Cardiologists (ABC), Society for Cardiovascular Angiography and Interventions (SCAI), Society for Vascular Nursing (SVN), Society for Vascular Surgery (SVS), Society of Interventional Radiology (SIR), and Vascular & Endovascular Surgery Society (VESS), introduce significant updates to clinical care, reflecting the latest evidence in pharmacotherapy, exercise interventions, hybrid revascularization strategies, multidisciplinary team-based care, and new insights into the impact of health disparities. Many SVM members participated in this document as writing committee members and peer reviewers. PAD affects more than 200 million individuals worldwide and carries significant morbidity and mortality risks, particularly from major adverse cardiovascular events (MACE) and major adverse limb events (MALE).1–3 The transition from the 2016 to 2024 guidelines highlights the evolving understanding of PAD management with focus on individualized patient care strategies that require coordinated efforts across specialties to improve outcomes.3,4 This article compares the key differences between the two guidelines, explores the evidence supporting the 2024 changes, and examines how SVM members and other healthcare providers are implementing these recommendations to deliver optimal patient care.
Dual antithrombotic therapy implementation
A major change in the 2024 guidelines is the shift toward dual antithrombotic therapy (termed ‘dual pathway inhibition’) using low-dose rivaroxaban (2.5 mg twice daily) in combination with low-dose aspirin (81 mg daily) to reduce both MACE and MALE. 3 This includes both patients with stable symptomatic PAD and individuals following lower-extremity revascularization (either surgical or endovascular). In contrast, the 2016 guidelines recommended only aspirin monotherapy or clopidogrel for most patients with PAD (Table 1).3,4 The inclusion of dual antithrombotic therapy reflects data from the COMPASS trial, which demonstrated that rivaroxaban plus aspirin reduced the risk of cardiovascular death, stroke, and myocardial infarction by 24% compared to aspirin alone while also lowering limb-related events (i.e., amputation) in patients with stable symptomatic disease. 5 After revascularization, patients should be prescribed dual pathway inhibition immediately postprocedure and longitudinally to reduce the risk of limb-related and cardiovascular events, as demonstrated by the findings of the VOYAGER PAD trial.6,7
Key differences between the 2016 and 2024 guidelines.
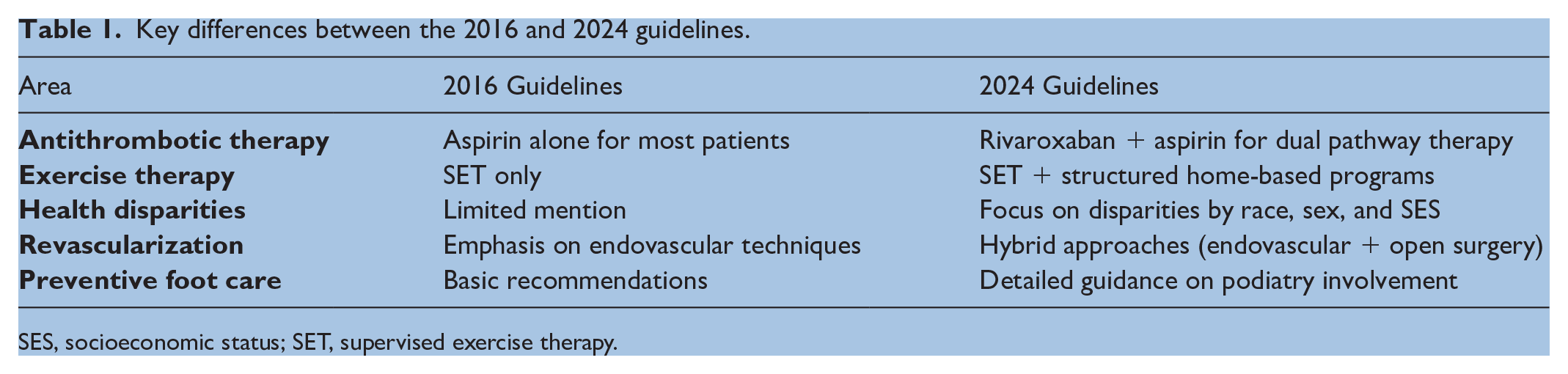
SES, socioeconomic status; SET, supervised exercise therapy.
Owing to bleeding risks associated with dual pathway inhibition, careful patient selection is emphasized with risk assessments guiding therapy to balance safety and efficacy. In practice, healthcare providers have adopted risk stratification tools, such as the HAS-BLED score, to estimate bleeding risk before initiating dual pathway inhibition. 8 Pharmacists also play a key role in promoting medication adherence and vigilance for bleeding complications, ensuring that patients understand the importance of consistent therapy and are aware of potential side effects.
Structured exercise therapy and home-based programs
The 2024 PAD guidelines introduce a broadened focus on structured exercise therapy (SET), expanding on the 2016 recommendation for supervised exercise alone.3,4 Recognizing that many patients have difficulty accessing facility-based programs, the 2024 update addresses practical barriers such as transportation and mobility issues to recommend structured home and community-based exercise programs supported by virtual coaching and remote monitoring. Data from recent trials confirm that both supervised and structured home-based programs yield improvements in walking distance, functional status, and quality of life, ensuring that patients who cannot attend in-person programs still receive therapeutic benefits.9–11
To implement these changes, clinics can provide wearable activity trackers, virtual coaching, remote monitoring, and individualized walking plans for patients to follow at home. In some models, exercise physiologists and advanced practice providers (APPs) conduct weekly virtual check-ins to monitor progress and offer guidance. Hybrid models are also being adopted, where patients initially engage in supervised programs and later transition to home-based exercise. During follow-up visits, providers review patient progress and adjust exercise plans as needed to ensure optimal outcomes. The addition of such programs to the guidelines reflects advances in digital health and supports patient adherence to prescribed walking regimens with a focus on improving walking performance and reducing claudication symptoms. Though the guidelines now recommend such programs, current payor coverage and reimbursement models will need to evolve to support broad implementation of these effective programs in clinical practice.
Addressing health disparities through screening and outreach
Another pivotal update in the 2024 PAD guidelines is the heightened focus on addressing racial, sex, and socioeconomic disparities, acknowledging that PAD disproportionately impacts certain populations, resulting in higher rates of amputation and worse cardiovascular outcomes. 3 This focus reflects the growing awareness that systemic inequities affect both the diagnosis and treatment of PAD, and that addressing these disparities is essential for improving population health outcomes.
Hybrid revascularization techniques for advanced PAD
The 2024 guidelines highlight advancements in revascularization techniques, which combine
In clinical settings, multispecialty teams collaborate to tailor treatment strategies and provide seamless preoperative and postoperative care to determine the best treatment approach for each patient. Postoperative care includes close coordination among vascular teams, wound care specialists, and podiatrists, among other specialists, to ensure proper wound healing and prevent further ischemic events. Hospitals are also participating in national vascular registries to document outcomes and refine best practices.
Preventive foot care as a central strategy
The 2024 PAD guidelines emphasize preventive foot care as a critical component of PAD management, especially for patients with diabetes and CLTI. This underscores the need for early intervention to reduce amputation risk. 3
Collaboration among podiatrists, vascular specialists, and wound care teams ensures that patients with nonhealing ulcers receive timely interventions to prevent amputations. Additionally, nurses and APPs are actively involved in patient education, teaching individuals and caregivers how to perform daily foot inspections, to maintain proper hygiene, and to select appropriate footwear to minimize injury risk.
Conclusion
The 2024 ACC/AHA PAD guidelines represent a significant evolution in the management of PAD, through dual antithrombotic therapy, expanded exercise programs, hybrid revascularization techniques, preventive foot care, and emphasizing multidisciplinary collaboration. 3 These changes address practice gaps identified in the 2016 guidelines and place a greater emphasis on health disparities in PAD to encourage equitable access to care. Healthcare providers can implement these updates by integrating community-based screening programs for patients at increased risk of PAD, virtual exercise coaching, multidisciplinary care teams, and advanced wound management protocols. With these strategies in place, clinicians can work toward reducing amputation rates, improving cardiovascular outcomes, and enhancing the quality of life for patients with PAD. The 2024 guidelines represent a significant step forward in ensuring that all patients receive comprehensive, evidence-based care tailored to their individual needs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
SVM Announcements: 2024 Giving Tuesday update
The Giving Tuesday donations that were received in 2023 covered registration to attend the 2024 Vascular Scientific Sessions for 21 students and trainees, distributed in conjunction with the Alan T Hirsch Travel Award program. The 2024 Giving Tuesday donations will once again support students and trainees to attend the 2025 Vascular Scientific Sessions.
Thank you to the 2024 SVM Giving Tuesday donors: Syed Ahsan, Fahad Alkhalfan, Herbert Aronow, John (Jerry) Bartholomew, Joshua Beckman, G. Jay Bishop, Marc Bonaca, Teresa Carman, Andrew Dicks, Robert Eberhardt, Eri Fukaya, Heather Gornik, Kamal Gupta, Stanislav Henkin, Deborah Honacek, Daniella Kadian-Dodov, Yogendra Kanthi, Hratch Karamanoukian, Esther S.H. Kim, Ann Marie Kupinski, Wenzhu Li, Elizabeth Ratchford, Eric Secemsky, Aditya Sharma, Alexandra Solomon, David Song, Danielle Vlazny, John Waites, Mitchell Weinberg, and Bryan Wells.