
Abstract
A carotid web (CaWeb), otherwise known as a carotid bulb diaphragm, is a spur of intimal fibrous tissue extending into the carotid bulb. It is a rare, underdiagnosed cause of ischemic strokes in young people. The purpose of this narrative review was to provide an update on CaWebs, highlighting recent evolutions in their management. We undertook a comprehensive literature search on main electronic databases – MEDLINE/PubMed, Cochrane Library, Web of Science, and EMBASE – using a dedicated equation to include studies up to February 13, 2024. We also searched for the most recent guidelines about carotid disease or stroke including CaWeb management. A CaWeb is found in up to 10% of young patients, particularly young women, with severe anterior stroke due to an arterial–arterial embolism from the intra-nidus thrombus. Most patients with a CaWeb have less than 50% stenosis on duplex ultrasound, and diagnosis is mostly obtained by computed tomography angiography. When applying traditional stenosis criteria for symptomatic disease (> 50% stenosis), this highly morbid condition is easily overlooked, leading to recurrent strokes. Antithrombotic treatment is associated with a high recurrence rate of stroke after the index event. The first-line treatment of symptomatic CaWebs is increasingly based on endarterectomy or stenting. The lack of recommendations before 2021 and recent discordant guidelines make CaWeb management complex. No guidelines are available to manage patients with asymptomatic CaWebs. Results from ongoing multicenter registries will be useful in guiding management decisions.
Keywords
Introduction
A carotid web (CaWeb) has been defined as an abnormal shelf-like projection or spur of intimal fibrous tissue extending into the carotid bulb1,2 and has been identified as a rare cause of severe and recurrent ischemic stroke in young people due to an arterial–arterial embolism in the anterior and proximal intracerebral circulation. It has also been defined as an abnormal monofocal intimal wall hyperplasia of the posterolateral internal carotid bulb. 1 Anatomopathological features were firstly reported by Rainer in 1968 in a young woman with multiple ischemic strokes. 3 The arteriography showed a thin diaphragm protruding at the posterolateral carotid bulb. This anatomical entity may be underdiagnosed because it can be difficult to identify on routine imaging modalities. 4 Moreover, once the diagnosis has been made, surgical management and medical treatment are still being debated. There was no recommendation before 2021 and recent guidelines are discordant.5,6 The purpose of this narrative review was to provide an update on CaWebs, highlighting recent evolutions in their management.
Methods
To conduct this narrative review, we undertook a comprehensive literature search on the main electronic databases: PubMed (MEDLINE), Cochrane Library (Wiley), Web of Science (Clarivate), and Embase (Elsevier). The following equation was used to query PubMed, then translated to query other databases: ("carotid web*"[Tiab] OR "carotid artery web*"[Tiab] OR (CaW[Tiab] AND carotid*[Tiab]) OR "carotid diaphragm*"[Tiab] OR "cervical artery web*"[Tiab] OR "carotid bulb web*"[Tiab]). Automatic alerts were set up to check for the publication of new articles during the narrative review period, ending on February 13, 2024. We limited our searches to documents published in English or French. No date restrictions were imposed on the search, and conference abstracts were excluded. The results of the queries were deduplicated and then imported into the Rayyan software (https://www.rayyan.ai/). An initial screening was carried out on the titles and abstracts of the references by a reviewer. The second screening was based on the entire article in pdf format. Data obtained from this selection were further examined to determine their relevance to this review.
We selected systematic reviews with or without meta-analyses and original retrospective and prospective studies in order to have an overview of this rare pathology, regarding epidemiology, histology, clinical presentations, and management. We also retrieved articles of interest cited in these studies. Finally, we searched for the most recent guidelines about carotid disease or stroke including CaWeb management.
Epidemiology
CaWeb is a rare and underdiagnosed disease. Only case reports and small cohorts were reported in the literature. In a recent review conducted between 1947 and 2020, only 189 patients with symptomatic CaWebs were identified. 7 In the largest series recently reported by Brinster et al., 4 52 patients with symptomatic web were identified between 2016 and 2022 in a large, tertiary stroke center. Its prevalence in the general population is unknown and is probably lower than 1%. 8 In the systematic review by Mac Grory et al., 9 the pooled prevalence of ipsilateral CaWeb in patients under 60 years old with cryptogenic stroke was 13% (95% CI: 7–22). In the systematic review and meta-analysis by El-Masri et al., the prevalence in symptomatic patients with embolic supra-tentorial stroke of indetermined source was 9.58% (95% CI: 5.62–15.85). 10 In a French retrospective monocentric cohort including 266 patients 65 years and under with an anterior circulation cryptogenic ischemic stroke, the prevalence of ipsilateral CaWeb was 7.9% (95% CI: 4.6–11.14). 11 Compared with atherosclerotic disease, the first stroke related to a CaWeb occurs in younger patients. 9 Demographic characteristics of the population with CaWebs concerns mainly women, with a predominance of between 56.5% and 76%.4,7,10,12 There is also a predominance in patients of African descent or in Afro-Caribbean populations, varying from 58% to 91%.4,10,13–15 However, in the CAROWEB registry, an observational multicenter French registry, 47.5% of the 202 symptomatic patients were White and 20.3% were Afro-Caribbean. 12 Patients with ischemic stroke related to a CaWeb have less traditional cardiovascular risk factors. In a 2018 systematic review, 57% of patients with symptomatic CaWebs had no cardiovascular risk factors. 13 In the study by Multon et al., 14 only four among 11 (36.4%) symptomatic patients had at least one atherosclerotic risk factor. In the series by Brinster et al., 62% of patients had hypertension, 52% had hyperlipidemia, 40% had a smoking history, only 12% had diabetes mellitus, and only 28% had more than one atherosclerotic risks factor. 4 Nevertheless, a CaWeb has been particularly associated with atherosclerosis15,16 or fibromuscular dysplasia (FMD). 17
Histology
CaWeb has been described as an atypical monofocal form of intimal dysplasia of the internal carotid bulb resulting in noncircumferential, diaphragmatic or spur-shaped stenosis located at the posterolateral part of the carotid bulb. This lesion has different names in the literature such as carotid bulb diaphragm, septum, web, shelf, and atypical focal carotid bulb FMD. 18 Three recent studies reported anatomopathological findings of symptomatic CaWeb lesions in, respectively, 24, 9, and 10 patients.4,19,20 All of them reported focal intimal changes including intimal hyperplasia with variable fibrosis proliferation, smooth muscle cell proliferation, myxoid degeneration, and a small amount of inflammatory and nonatheromatous cell infiltration, giving a web-like appearance. In the study by Brinster et al., eight patients among 24 had associated atherosclerotic changes or web calcifications. 4 Furthermore, due to macroscopic findings during open surgery, Brinster et al. described two different phenotypes: a ‘prism morphology corresponding to a thickened, wide-based web’ and a ‘veil morphology’ corresponding to a thin, sail-shaped web. 4 CaWeb must be distinguished from the ‘classical’ FMD, owing to its location in the posterolateral carotid bulb, the absence of typical ‘string of beads’ appearance, the anatomopathological findings, and the absence of associated renal or postbulbar carotid FMD.4,21 This anatomopathological lesion has exceptionally been described in the vertebral or subclavian arteries.22,23
Clinical presentations
Symptomatic carotid web (CaWeb)
CaWeb has been recognized as a cause of proximal anterior arterial–arterial embolic stroke. The thin membrane protrudes into the carotid bulb, creating turbulences and blood stasis in the nidus. 2 In the study by Ren et al., based on blood flow simulations with computed tomography angiography (CTA), the CaWeb caused a recirculation zone distal to the web and was associated with flow parameters closely related to thrombosis via early platelet/clot accumulation and deposition. 24 Blood flow stasis was also demonstrated on digital subtraction angiography (DSA) images by Park et al. 25 These mechanisms lead to thrombus formation in contact with the CaWeb, which can cause ischemic embolic stroke. These hypotheses are corroborated by the absence of tight stenosis created by the CaWeb, in contrast to atherosclerotic disease. In the CAROWEB registry, the degree of stenosis according to the European Carotid Surgery Trial (ECST) method was 42 ± 13%. 12 In the study by Kim et al., patients with cryptogenic stroke and CaWeb had a less than 30% degree of stenosis according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) method. 26 In the matched case–control study by Landzberg et al., 27 including 30 patients with symptomatic CaWebs and 120 controls with stroke or transient ischemic attack of other origin, patients with CaWebs had a smaller absolute number of modifiable cerebrovascular risk factors (1.7 ± 1.1 vs 2.5 ± 1.2, p = 0.002). This corroborated the proposed mechanism of local hemodynamic disturbance generated by the web causing low shear stress and stasis leading to thrombosis and artery-to-artery thromboembolism. The embolic mechanism was demonstrated in one case by recurrent thrombus formation and intracerebral migration. 28 However, diagnosis of CaWeb remains one of exclusion in the absence of other more frequent causes of stroke. In the single-center study reported by Labeyrie et al. 29 that included 466 consecutive symptomatic patients treated by thrombectomy, 12% had an embolic stroke of undetermined source. In this subgroup, ipsilateral CaWeb was more frequent than in the rest of the sample (10.7% vs 0.7%; 95% CI: 2.7–18.7, p < 0.001). The difference remained significant after adjustment for sex, age, and vascular risk factor (OR 12.5; 95% CI: 2.1–7.1, p = 0.005). Histological findings of thrombi in patients with symptomatic CaWebs included fibrin, platelets, red bloods cells, and inflammatory infiltration of leukocytes, but no signs of atheroma such as cholesterol crystals. 30 In the meta-analysis by El-Masri et al., 10 an ipsilateral CaWeb was significantly associated with cryptogenic embolic stroke compared to a group of asymptomatic patients who had CT brain and neck angiogram imaging for another indication (RR 2.74; 95% CI: 2.14–3.51). Embolic strokes related to a CaWeb lead to proximal anterior intracerebral occlusion, and more especially the middle cerebral artery territory, resulting in severe neurological damage and clinical status with a National Institute of Health Stroke Score (NIHSS) of 13.8 ± 6.6 for Coutinho in 2017 31 and a median NIHSS at admission of 8 (IQR 2–15) for Olindo in 2024. 12 In a retrospective study analyzing 51 patients with a cryptogenic ischemic stroke, 39 had an anterior circulation stroke and nine of these (23%) had an ipsilateral CaWeb. CaWeb has been associated with higher rates of proximal large intracranial arterial occlusions. 26 In the cohort study by Olindo including 92 patients, 23.9% had an unfavorable outcome with a modified Rankin Scale (mRS) at 3 or above (mRS 3 for 10.8%, mRS 4 for 8.7%, mRS 5 for 1.1, and mRS 6 for 3.3%). 32 After a transient ischemic attack, the CaWeb seems to be involved in less than 10% of cases in patients without any other risk factors for a neurovascular event. 33
Asymptomatic CaWeb
Little is known about the asymptomatic CaWeb. Around 25% of patients with a symptomatic CaWeb have a contralateral asymptomatic CaWeb.4,7 A CaWeb may also be incidentally discovered. 13 Several studies have compared the morphological appearance of CaWebs according to their symptomatic or asymptomatic characteristics.34,35 In the study by da Camara et al. 34 , who analyzed CaWeb characteristics on CTA, the mean web length and the median web volume were statistically smaller in asymptomatic CaWebs compared to symptomatic ones. In the study by Tabibian et al. based on CTA, asymptomatic CaWebs were shorter (< 3 mm), had a less acute angle relative to the carotid wall (> 90°), and occupied less than half of the bulb’s lumen. 35 In the CAROWEB registry, 12 asymptomatic mean CaWeb length was significantly shorter (2.24 ± 0.90 vs 2.82 ± 0.82, p = 0.004) and the degree of carotid bulb stenosis (measured according to the ECST method) was significantly lower (34.4 ± 11.4 vs 41.6 ± 11.8%, p = 0.009) compared to symptomatic CaWebs. 16 No patients with known asymptomatic CaWebs experienced stroke during follow-up, even without treatment.7,13,16 Therefore, according to the authors, the asymptomatic nature of the CaWeb could be related to its morphology and to a lower degree of stenosis. However, morphological changes over time in asymptomatic CaWebs have not been studied and the absence of stroke during follow-up might only be due to the small numbers of patients and to the short follow-up.
Imaging diagnosis
Digital subtraction angiography (DSA)
Digital subtraction angiography (DSA)
CaWeb diagnosis is based on imaging. In older studies, the only imaging technique for CaWeb diagnosis was DSA.3,36 CaWebs were defined on DSA as a shelf-like filling defect arising from the lateral posterior side of the internal carotid bulb 37 and associated with contrast stagnation distal to the CaWeb on adapted incidences. 13 DSA is no longer the first-line imaging choice for CaWeb diagnosis. However, during thrombectomy procedures, DSA may reveal a CaWeb (Figure 1). The carotid bulb must be examined in a lateral projection. 4
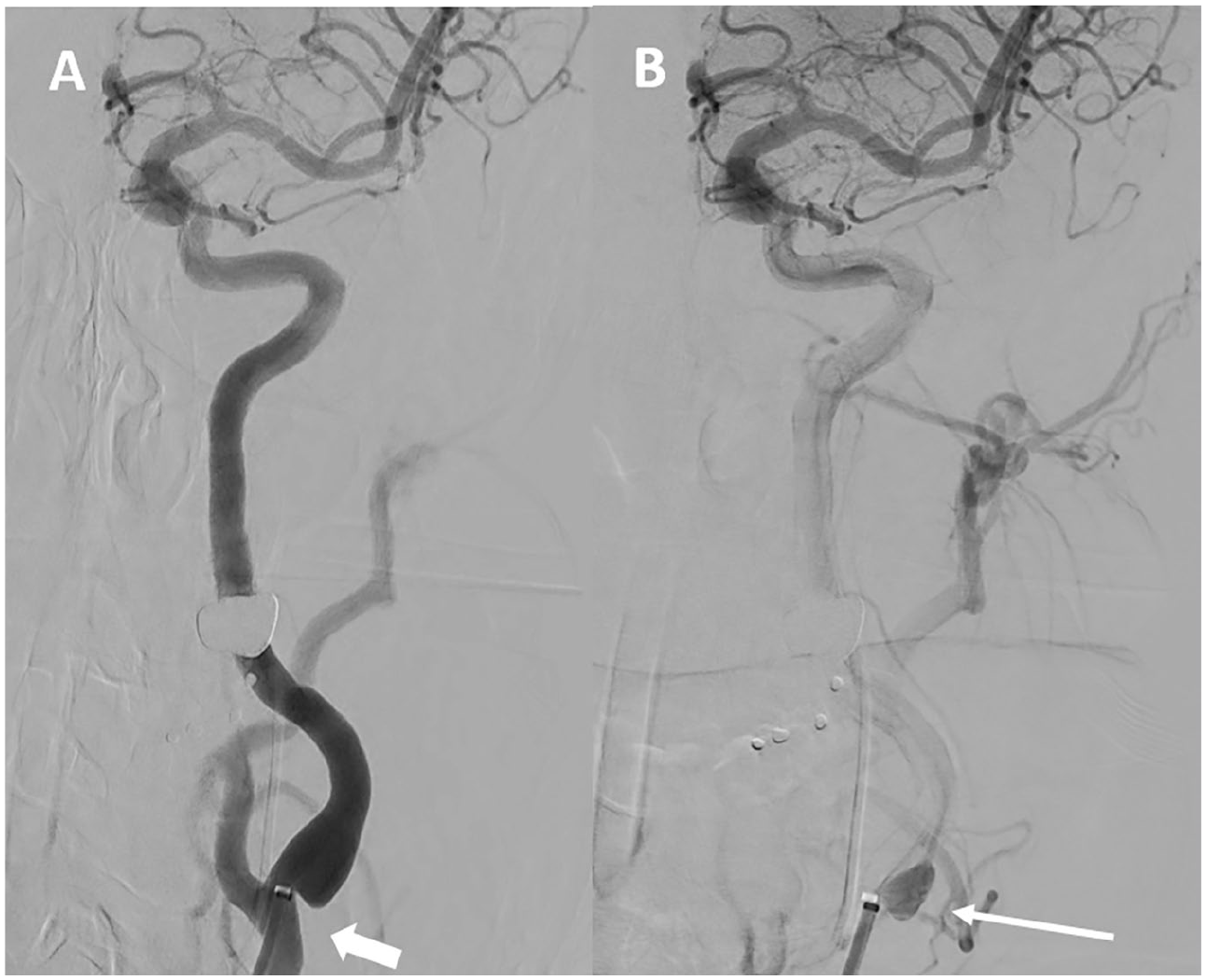
Intra-arterial angiography performed during thrombectomy.
In addition to catheter angiography, optical coherence tomography (OCT) and intravascular ultrasound (IVUS) have recently been evaluated for CaWeb diagnosis. OCT creates high-resolution images of tissues. In the retrospective study by Al-Bayati et al., intravascular OCT was evaluated in 16 patients with a suspected symptomatic CaWeb. 52 OCT confirmed the CaWeb in 12 cases and concluded atherosclerosis in four cases. Furthermore, OCT revealed microthrombi in two CaWeb cases that were misdiagnosed on both DSA and CTA. However, further studies are needed to position this invasive technique among other imaging modalities. In contrast to OCT, the performance of IVUS for diagnosing CaWeb is modest. 53
Computed tomography angiography (CTA)
The noninvasive gold standard imaging technique for CaWeb diagnosis is currently CTA.8,12,38 Diagnosis requires millimeter slices and multiplanar reconstructions. The axial section shows a focal intraluminal, thin, line-like signal or thin septum (‘burger’ sign) and the oblique sagittal section, which is the best plane, shows a spur-shaped intraluminal filling defect on the posterior wall of the carotid bulb (Figure 2).2,4,12,23,32 A recent study analyzing CTA reconstructions for CaWeb detection and feature assessment, highlights the importance of multiplanar reformatting over 3D reconstructions or maximum intensity projections as multiplanar reformatting provides images in different planes with a minimum thickness. For the authors, CTA multiplanar reformatting could also be used to differentiate CaWeb from atherosclerotic disease. 39 Furthermore, the CaWeb angioarchitecture of 22 patients retrospectively studied on CTA statistically differed between patients with (n = 11) or without (n = 11) stroke. 40 Based on the results of this pilot study, the authors concluded that web angle measurements relative to the common carotid artery and internal carotid artery might help for stroke risk assessment.
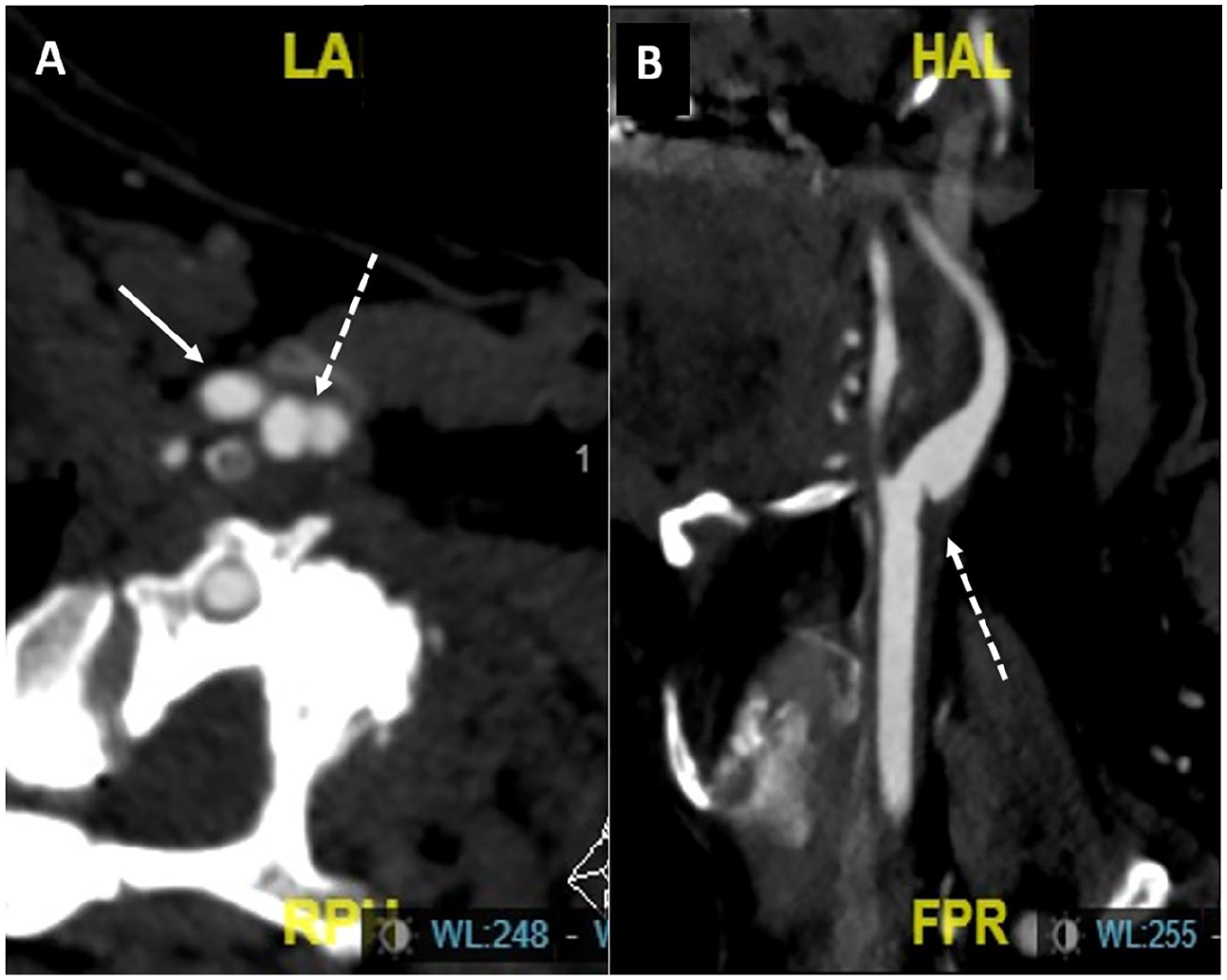
Computed tomography angiography with millimeter slices and multiplanar reformations.
Magnetic resonance imaging (MRI) and angiography (MRA)
MRI is the gold standard for diagnosing ischemic stroke. Nevertheless, at acute event, MRI focuses on cerebral damage and not on the internal carotid artery. In the study by Joux et al., the authors focused on the magnetic resonance angiography (MRA) sequences used to diagnose CaWeb. On T1-weighted sequences, the lesion was homogenous with a slight hypersignal before contrast injection and showed inner layer enhancement after gadolinium injection; on T2-weighted sequences, the lesion appeared homogenous with isosignal. 41 Other studies of CaWeb specificities with MRI have focused on morphology, composition by multicontrast fast spin-echo, and wall dynamics by cine-fast spin-echo according to cardiac phase. 42 In a recent study using 4D flow MRA reporting flow patterns in patients with a CaWeb, higher values of flow parameters linked to vascular dysfunction and thrombosis were induced by the CaWeb compared to those induced by atherosclerotic plaque or in healthy patients. 43 These sequences are not yet routinely performed. Figure 3 shows a symptomatic left CaWeb using MRA.

Magnetic resonance angiography with maximum intensity projection reformations. The white arrows show an intraluminal defect on the posterolateral wall of the left carotid bulb corresponding to the carotid web.
Duplex ultrasound (DUS)
Detection of a CaWeb with DUS was first reported in 1991 by Kliewer and Carroll. 44 DUS CaWeb exploration requires a high-frequency linear array transducer and an adequate probe position to image the CaWeb due to its posterolateral location in the bulb. The optimal incidence is the longitudinal view perpendicular to the septum. 45 In B-mode, under longitudinal view, CaWeb was described as an iso or hypoechoic thin linear membrane-like lesion protruding from the posterior wall of the internal carotid bulb, just beyond the carotid bifurcation, with a wide, noncalcified implant base leading to a triangular lesion.45,46 Color Doppler ultrasound showed changes in blood flow directions and an eddy between the posterior wall and CaWeb.45,46 Pulsed Doppler analysis of the peak systolic velocity and the end-diastolic velocity shows moderate acceleration in most cases, corresponding to a degree of stenosis of less than 50% NASCET, North American Symptomatic Carotid Endarterectomy Trial. (Figure 4). DUS may also reveal hypoechoic thrombus behind the CaWeb.47,48 DUS is therefore used to identify the presence of thrombus, to monitor thrombus lysis on antithrombotic therapy, and thus define the best timing for surgery. 46 Other ultrasound modalities are works in progress, including 3D ultrasound reconstructions for anatomical analysis46,49; ultrasound microflow imaging to analyze with more sensitivity the slow flow induced by the CaWeb 45 ; or contrast-enhanced ultrasound to improve diagnostic accuracy for CaWebs in thrombosis. 50 In a systematic review including 121 patients with CaWebs having both CTA and DUS, 89 CaWeb cases were diagnosed with both techniques, whereas DUS missed diagnosis in 27 patients (22.3%) and CTA missed five patients (4.1%). 51 The accuracy rate between DUS and CTA was 73.6% (95% CI: 64.8–81.2), and the sensitivity of DUS compared to CTA was 76.7% (95% CI: 68.0–84.1).
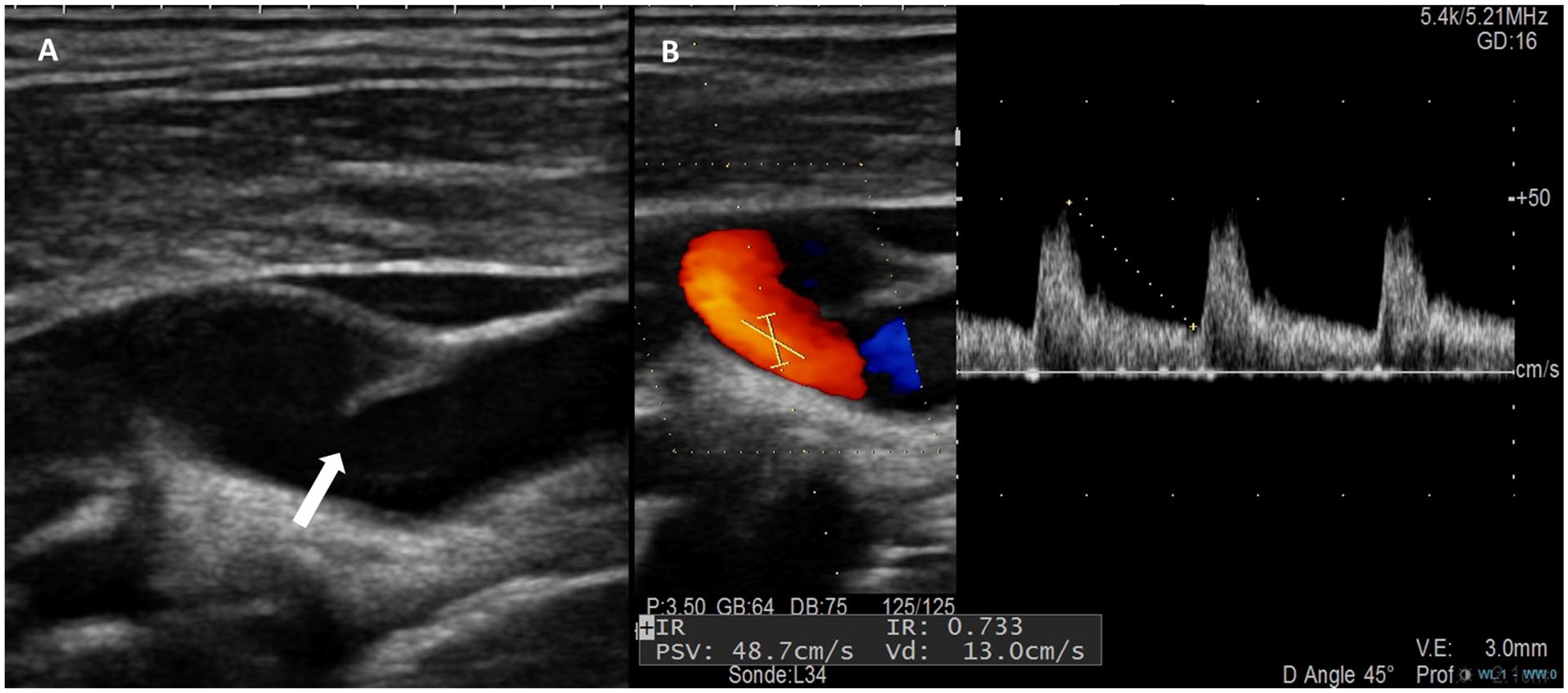
Duplex ultrasound appearance of a symptomatic left carotid web.
Multimodality imaging techniques
In the narrative review by Chen et al., practical recommendations positioned CTA with multiplanar reconstructions as the first-line imaging modality.8,54 MRA and DUS were considered relevant complementary imaging techniques in the presence of atypical CaWebs, and catheter angiography should be reserved for patients in whom the diagnosis of CaWeb remains uncertain despite multimodality imaging studies or for patients requiring thrombectomy or carotid stenting. Schutt et al. also underlined the importance of multiple vascular imaging modalities during stroke workup resulting in a CaWeb diagnosis rather than embolic stroke of undetermined source. 54
Pitfall in diagnostic imaging
The main pitfall in diagnosis imaging is the presence of thrombus filling the nidus. In this situation, it may be difficult to differentiate a CaWeb from small and noncalcified atheromatous plaque, especially when a plaque is present at the contralateral carotid bifurcation, even on CTA. On DUS B-mode, atheromatous plaque is frequently heterogeneous with hypo- and hyperechoic areas, and the identification of a hyperechoic septum arising from the posterolateral carotid bulb allows for CaWeb diagnosis.45,48
Therapeutic options
Optimal management of a CaWeb is not yet standardized. Though the treatment of a symptomatic CaWeb is increasingly based on surgery, the treatment of an asymptomatic CaWeb is still controversial and remains at the discretion of the medical–surgical team. The lack of recommendations and recent discordant guidelines make CaWeb management complex.5,6 Medical or surgical CaWeb management requires a multidisciplinary team consensus decision in all cases. 6
Medical treatment
Antiplatelet therapy, anticoagulant, or both, have been diversely used in the literature after the index stroke event.4,7,11–13,18,32,55 Nevertheless, many studies reported a high recurrence rate of stroke in symptomatic patients treated medically. In the systematic literature review by Zhang et al. including 158 patients, 35% (n = 47) of 135 patients with symptomatic CaWebs were treated medically, including antiplatelet therapy (91%) or anticoagulation (9%). 13 Among them, 56% (n = 25) presented with recurrent stroke during a median follow-up of 12 months. The stroke recurrence rate was 54% and 75%, respectively, in patients with antiplatelet therapy and anticoagulation. In the French cohort published by Turpinat et al., the annual stroke recurrence rate reached 11.4% (95% CI: 8.4–15.1) in patients under conservative medical therapy. 11 In the cohort study by Olindo et al., the recurrence rate after a first event was 27.3% at 5 years under medical treatment alone, ipsilateral to the symptomatic CaWeb in all cases. 32 Using data from the MR CLEAN trial (from 2010 to 2014) and MR CLEAN registry (from 2014 to 2017), Guglielmi et al. analyzed stroke recurrences in 28 among 30 patients with an ipsilateral CaWeb to the index stroke receiving medical management (23 on antiplatelet therapy and five on anticoagulant therapy). 55 The incidence of recurrent stroke within 2 years in patients with medical management was 18%: 13% in patients on antiplatelet therapy and 40% in patients on anticoagulation. In a more recent systematic literature review by Patel et al. published in 2022 including 289 symptomatic patients, 138 (48%) were treated medically. 18 The recurrence rate of stroke was 26.8% at 55 months of follow-up, without any significant difference between patients treated with antiplatelet, anticoagulant, or no antithrombotic therapy. This high recurrence rate of stroke despite medical treatment has been confirmed in the recent study by Brinster et al. including 52 symptomatic patients. 4 All 10 patients medically treated presented an ipsilateral recurrent stroke during a median follow-up of 43 months. The cause of these recurrent strokes in patients with CaWeb lesions under medical therapy is unknown. It might be related to residual thrombus, noncompliance with antithrombotic treatment, medication changes, a temporary hypercoagulability state such as dehydration, or recreational drug use 4 leading to new thrombus formation in the nidus. The delay between the index event and the recurrence was highly variable with a median time around 12 months (range 0–97 months). 13
Open surgery and carotid stenting
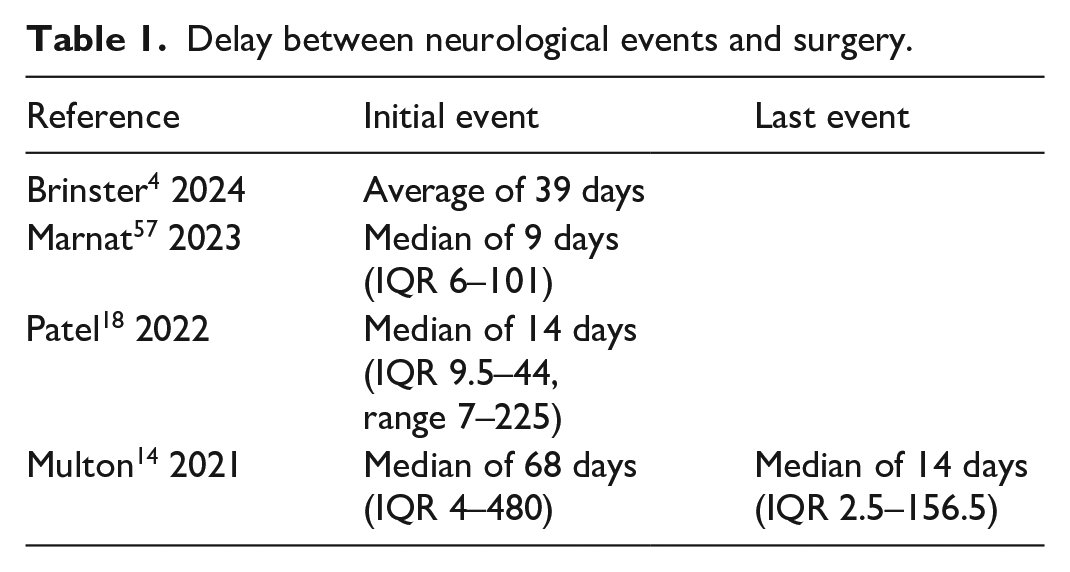
Open surgery or carotid angioplasty stenting have been proposed for the treatment of symptomatic CaWebs without clear recommendations and no randomized clinical trial to compare both strategies. There are only case reports and short series. Surgical treatment concerns more than half of symptomatic patients.12,18 The indication for surgery seems to depend on the patient’s clinical characteristics and the CaWeb lesion. In a previous CAROWEB report, symptomatic patients treated by surgery were younger (45.9 ± 9.7 vs 50.4 ± 9.5 years, p = 0.02), had more severe CaWeb stenosis (43 ± 13% vs 34 ± 14%, p = 0.002), and were more likely to have vessel occlusion (82.6 vs 46.7%, p = 0.005). 32 In the more recent CAROWEB report, after multivariate analysis, surgery was significantly associated with a lower NIHSS score and ipsilateral chronic cerebral infarction. 12 Time to revascularization between ischemic events and CaWeb surgery are reported in Table 1 with no established recommendations.4,14,18,56,57 The origin of a CaWeb ischemic stroke is the migration of the thrombus formed in the nidus. The important point to consider in the preoperative period is the presence of residual thrombus in the web pocket that determines the operative risk. For this reason, a morphologic exam just before surgery seems to be indicated and duplex ultrasound can provide this information. The objective of surgery is to eliminate the pocket, not to treat a stenosis. Different approaches of open surgery have been described in the literature.14,18,58 In the review by Patel et al., 26 patients had open surgery. The most used technique was internal carotid artery resection followed by end-to-end anastomosis (54%), resection with direct arteriotomy closure (23%), or patch angioplasty (23%). 18 In the study by Multon et al., 13 patients had open surgery: 11 with internal carotid resection anastomosis and two with patch enlargement. 14 Stenting is currently the most commonly proposed procedure in symptomatic patients,12,57,59 occurring in more than half of patients according to the series and reaching 73% compared to surgery excision (27%) in 12 Some authors also reported stenting during an intracerebral thrombectomy procedure.4,37 Guidelines for carotid artery stenting recommends dual antiplatelet therapy before stenting or a high dose of antiplatelet therapy the day of the procedure to avoid acute thrombosis, followed by treatment continuation for several weeks or months. Antiplatelet treatment at the acute phase of stroke, required by stenting, might increase the risk of intracerebral hemorrhage. In the series of 23 carotid artery stenting procedures performed during the same procedure as intracerebral thrombectomy, Brinster et al. did not report hemorrhagic strokes. 4 These reassuring results need to be confirmed. After stenting, dual antiplatelet therapy for 3 months followed by long-term single therapy were prescribed,56,57,59 which can be restrictive for young patients. Results after open surgery or stenting are reported in Table 2. Whatever the surgical technique, no permanent or severe complications have been reported, during the procedure or follow-up. In the systematic review by Zhang et al., no stroke recurrence was recorded, neither at the early phase nor during follow-up, with a follow-up period reaching 12 years. 13 Only one case of 10% restenosis was described at 4-month follow-up by Wojcik et al. without neurological symptoms or new stenting. 37 There is currently no recommendation to choose between open surgery or stenting. With the experience of 27 endarterectomies for CaWeb lesions, Brinster et al. made a description of two distinct CaWeb phenotypes during carotid endarterectomy with interesting surgical implications. 4 The endarterectomy plane seemed to be easier with the thin, sail-shaped phenotype and the isolated resection of the diaphragm was possible for this type. For the thickened, wide-based phenotype, the intimal resection should be more extensive. For this second phenotype, carotid artery stenting could be preferred. To make this choice, distinguishing the two phenotypes is required on preoperative morphological exams. For the moment, this distinction has only been possible macroscopically when the carotid artery was opened.
Delay between neurological events and surgery.
Symptomatic CaWeb: Results after open surgery or stenting.
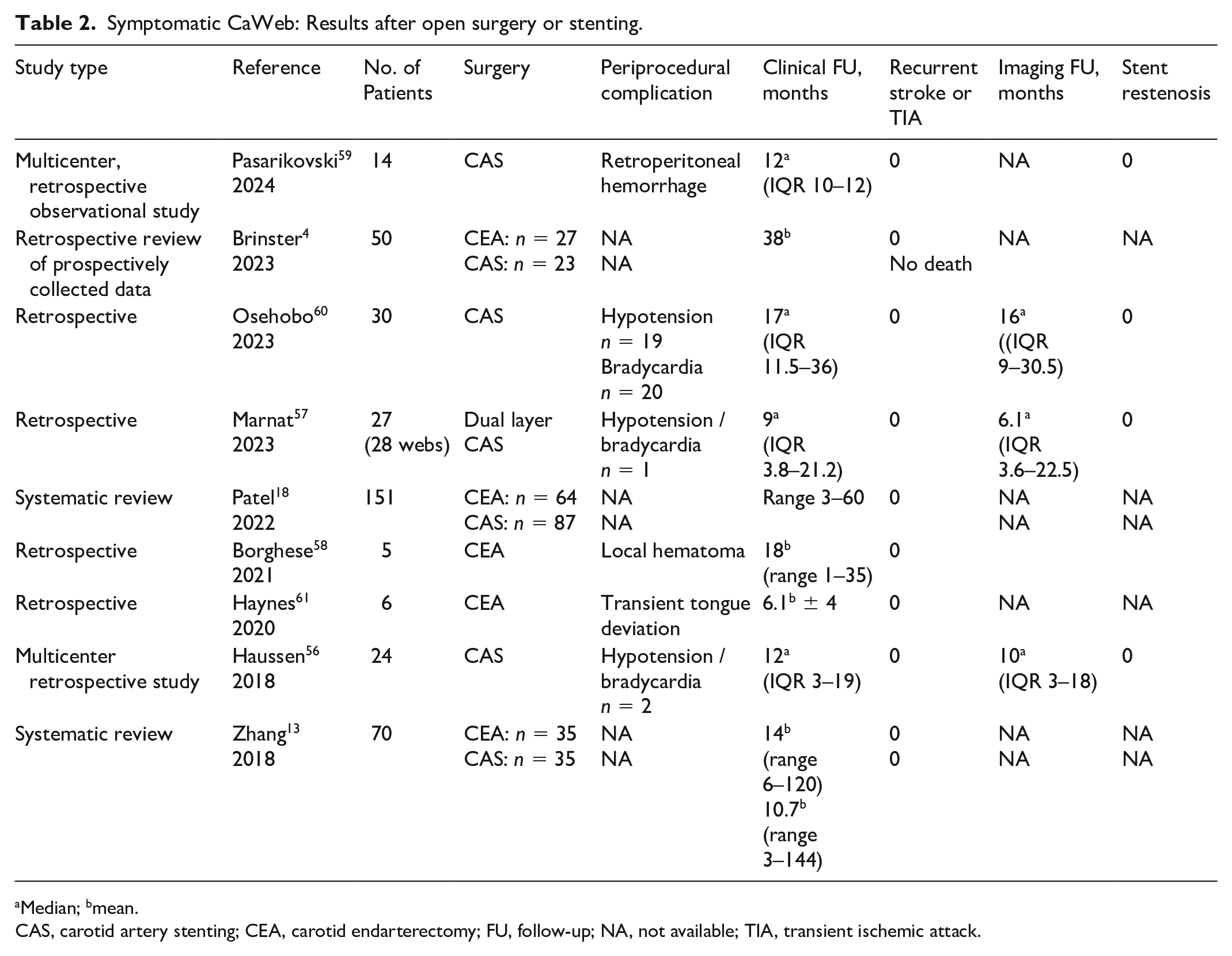
Median; bmean.
CAS, carotid artery stenting; CEA, carotid endarterectomy; FU, follow-up; NA, not available; TIA, transient ischemic attack.
Guidelines
Guidelines concerning CaWebs were first proposed by the American Heart Association/American Stroke Association (AHA/ASA) 5 in 2021 and then by the European Society for Vascular Surgery (ESVS) 6 in 2023. These guidelines only focused on symptomatic CaWebs. In the 2021 AHA/ASA guidelines, the experts proposed as first-line treatment antiplatelet therapy to prevent recurrent ischemic stroke or transient ischemic attack with a class of recommendation (COR) 1 (strong), and a level of evidence (LOE) B-NR, based on nonrandomized studies. Carotid stenting or endarterectomy might be considered in patients refractory to medical management with a COR 2b (weak) and a LOE C-LD reflecting limited data. 5 The 2023 ESVS guidelines stipulated that medical treatment such as antiplatelet therapy or anticoagulation were insufficient to prevent recurrent events and that carotid endarterectomy or carotid artery stenting might be considered to prevent recurrent stroke in patients with no other cause of neurological event, with a Class IIb and Level C. 6 None of these guidelines have made any recommendation regarding the optimal medical management of asymptomatic patients with a CaWeb or patients with bilateral CaWebs with one being asymptomatic, nor the optimal medical management between the index stroke and endarterectomy or stenting.5,6
Conclusion
Key points concerning CaWeb are summarized in Table 3. CaWeb is a rare but serious nidus-like lesion of the carotid bulb potentially leading to recurrent ischemic strokes in young patients due to an arterial–arterial embolism in the anterior and proximal intracerebral circulation. This lesion should be investigated in all cases of cryptogenic stroke in young people in the absence of cardiovascular risk factors and especially in women and patients of African descent or in Afro-Caribbean populations. Diagnostic imaging for CaWeb is based on CTA with millimeter slices and multiplanar reconstructions. Medical treatment alone is ineffective in preventing recurrent strokes. Carotid stenting or open surgery must be considered as first-line treatment and, in the absence of guidelines or randomized trials, the choice is surgical team-dependent. There is still a lack of guidelines concerning the delay and the medical treatment between stroke and surgery. No guidelines are available to manage patients with asymptomatic CaWebs. Results from ongoing multicenter registries will be useful in guiding management decisions.
Carotid webs (CaWebs): Key points.
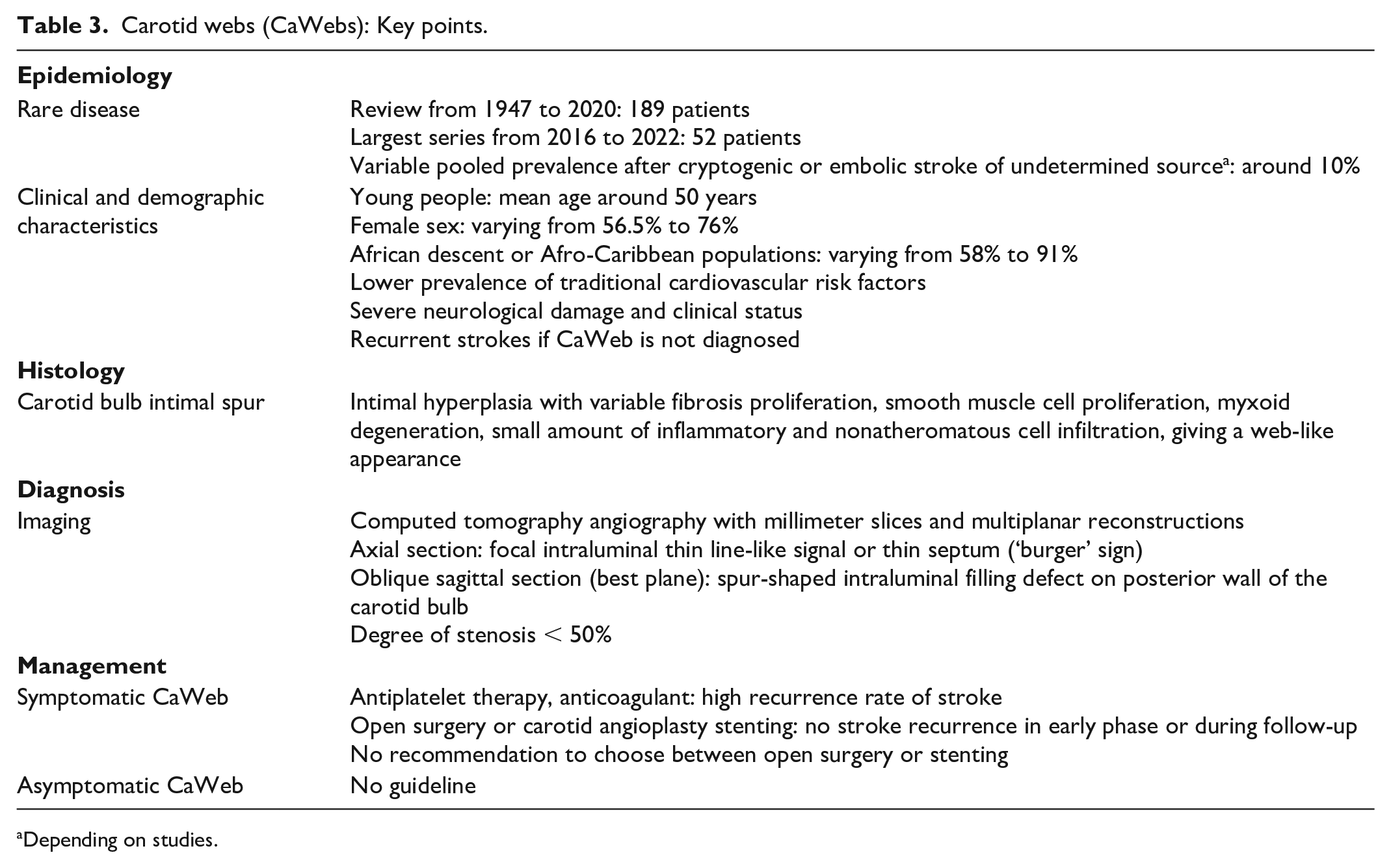
Depending on studies.
Footnotes
Acknowledgements
The authors thank Caroline Giroudon, librarian from the Central Documentation Department of the Hospices Civils de Lyon, for her wise remarks and help in developing the literature search strategy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.