
Abstract
Introduction:
Abdominal aortic aneurysm (AAA) is a growing public health problem, and not all patients have access to surgery when needed. This study aimed to analyze spatiotemporal variations in AAA mortality and surgical procedures in Brazilian intermediate geographic regions and explore the impact of different surgical techniques on operative mortality.
Methods:
A retrospective longitudinal study was conducted to evaluate AAA mortality from 2008 to 2020 using space–time cube (STC) analysis and the emerging hot spot analysis tool through the Getis-Ord Gi* method.
Results:
There were 34,255 deaths due to AAA, 13,075 surgeries to repair AAA, and a surgical mortality of 14.92%. STC analysis revealed an increase in AAA mortality rates (trend statistic = +1.7693, p = 0.0769) and a significant reduction in AAA surgery rates (trend statistic = −3.8436, p = 0.0001). Analysis of emerging hotspots revealed high AAA mortality rates in the South, Southeast, and Central-West, with a reduction in procedures in São Paulo and Minas Gerais States (Southeast). In the Northeast, there were extensive areas of increasing mortality rates and decreasing procedure rates (cold spots).
Conclusion:
AAA mortality increased in several regions of the country while surgery rates decreased, demonstrating the need for implementing public health policies to increase the availability of surgical procedures, particularly in less developed regions with limited access to services.
Keywords
Introduction
Abdominal aortic aneurysm (AAA) is a significant public health problem, with a prevalence of 1.7% to 3% in Brazil among individuals aged 50 and over, reaching 6.8% in patients with risk factors.1,2 Interventional treatment is indicated for aneurysms larger than 55 mm in diameter, with rapid growth or saccular features, as well as in symptomatic cases. The volume of surgery amounts to about 1100 patients per year in the Brazilian public health system and 45,000 patients per year in the United States.3–5
Few epidemiological studies have analyzed AAA mortality in Brazil. There are large regional disparities in healthcare in the country, attributed to its developing status, large territorial extension, and great heterogeneity in socioeconomic characteristics between regions.6–8 A recent national study showed an increasing trend in overall mortality from aortic aneurysms in 2000–2008, followed by a decrease in 2008–2016. The most economically developed and populated regions had a higher mortality rate, probably associated with greater access to diagnostic tests. 9
Some studies, restricted to reference centers for AAA surgery in Brazil, investigated surgical mortality rates; however, the findings do not reflect the reality of the country.10–13 Louzada et al. 3 recently published an extensive analysis of AAA surgeries performed in the Brazilian public health system, demonstrating a downward trend in the number of open and endovascular procedures in recent years. Furthermore, Brazil was found to have a significantly lower surgery rate than several other countries, and, as expected, the less economically developed regions of the country had lower surgery rates.
This study aimed to analyze spatiotemporal variations in AAA mortality and surgical procedures among individuals aged 50 years or older in different Brazilian regions and explore the impact of different surgical techniques on operative mortality from 2008 to 2020.
Methods
Study design and location
This is an ecological, descriptive, retrospective, longitudinal study based on secondary data on AAA mortality, surgical procedures, and surgical mortality in Brazil. The study was conducted according to the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14
Brazil is a country of continental extension (8,510,000 km2), comprising 5570 municipalities grouped into 134 intermediate geographic regions. These regions are based on private and public management flows and the existence of urban functions of greater complexity centralized in a hub city. Intermediate geographic regions are defined by the Brazilian Institute of Geography and Statistics (IBGE), and changes may occur when a new demographic census is conducted. 15
Data sources and study variables
The microDATASUS package of RStudio version 1.1.4 was used for data analysis. The number of deaths directly related to AAA (codes I71.3 and I71.4 of the International Classification of Diseases, 10th Revision [ICD-10]) among individuals aged 50 years or over occurring between 2008 and 2020 was obtained from the Mortality Information System of the Brazilian Ministry of Health (DATASUS).16–18 DATASUS is a reliable source of data on morbidity, healthcare access, and socioeconomic conditions; it is crucial for sanitary analyses, adapting to managers’ needs, and maintaining data reliability. The information system meticulously documents death certificates, including primary causes, contributing factors, and medical assistance. With nearly 25 years of operation, DATASUS has developed over 200 systems, strengthening the Brazilian Unified Health System (SUS) and directly assisting the Ministry of Health.
The Hospital Information System of DATASUS was used to retrieve data on patients treated in the public health system undergoing open aneurysm repair (OAR), obtained using codes 04.06.01.013-7, 04.06.02.004-3, and 04.06.02.005-1, and endovascular aneurysm repair (EVAR), using codes 04.06.04.015-0, 04.06.04.016-8, and 04.06.04.017-6.17,18 Of these procedures, only those performed on AAA were selected (codes I71.3 and I71.4) and divided into ruptured AAA (rAAA) and intact AAA (iAAA). Individuals under 50 years of age were excluded from the analysis because of the low incidence of AAA in these age groups. The database contains information on the patient’s municipality of residence, location where they were admitted and operated on, code of the main procedure, main ICD-10 code, and information on death during hospitalization.
Information on the resident population of the same age group in each municipality was obtained from IBGE and grouped according to intermediate region. The population covered by private medical assistance was accessed from the National Supplementary Health Agency (ANS).15,19
Data analysis
Raw AAA mortality rates were calculated by dividing the number of AAA deaths (including operated and nonoperated patients) by age-adjusted resident population multiplied by 100,000. Surgery rates were calculated by dividing the number of procedures performed by the age-adjusted resident population and multiplying by 100,000. Furthermore, surgical mortality rates were presented in both total values and percentages for each surgical technique, aiming to provide a comprehensive analysis.
To minimize potential instabilities in rate variability, especially when dealing with small population bases, we used the spatial empirical Bayesian estimator (SEB). SEB calculates a weighted average of the local gross rate and the region’s global rate through incorporation of the neighborhood matrix, ensuring spatial proximity between different regions during rate calculations, making rates more stable and reliable. This approach was crucial for intermediate regions, in which the combination of small rates and populations could lead to random fluctuations. 20
Space–time cube (STC) analysis was used to investigate spatiotemporal trends in mortality rates for operated and nonoperated AAA. The same technique was used to analyze the spatiotemporal trend in AAA repair procedure rates. This method aggregates data points representing event occurrences within specific time intervals and geographic areas, utilizing this information to construct a cube, in which each bin represents a unique combination of time and location. After creating the STC, we applied the emerging hot spot analysis (EHSA) tool, running a space–time implementation of the Getis-Ord Gi* on the bins of the cube. This allowed analysis of the spatiotemporal context of their neighbors to identify clusters and their intensity. In this process, a false discovery rate (FDR) correction was used for possible false positives. The FDR adjusts the critical p-value to account for the probability of encountering spurious associations. Subsequently, the time series of hot spot and cold spot clustering was assessed using the Mann–Kendall trend test, resulting in a trend z-score for each provided location.20,21 EHSA results can be visualized as behavioral trend maps, divided into 17 possible patterns. Warm/red colors traditionally indicate elevated rates, cold/blue colors represent low rates, and white is used for undefined patterns. Each hot or cold spot category is represented on the map with a specific hatch pattern, including new, consecutive, intensifying, persistent, diminishing, sporadic, oscillating, and historical spots (refer to online supplementary material for a definition of each pattern name). 22 STC analyses were performed using ArcGIS PRO software (eris). 23
The study was approved by the Research Ethics Committee at the State University of Maringá (COPEP protocol no. 5/2021). Given that secondary data were used, without identification of participants, the study was exempt from informed consent.
Results
From 2008 to 2020, there were 34,255 deaths in Brazil due to AAA or related to AAA complications among individuals over 50 years of age. The majority of deaths, amounting to 20,252 (59.12%), occurred in Southeast Brazil, which is the most developed and populous region of the country.
Among all 34,255 deaths, 19,024 patients received some kind of medical assistance. Considering that the private medicine coverage in Brazil ranged from 21.7% to 25.9% during the study period, we can infer that at least 14,895 individuals might have sought treatment in the public health system. Among patients who died without medical assistance, 67% lived in the Southeast, 70% were over 69 years of age, and 67.9% were men.
In the same period, there were 13,075 procedures for AAA repair in the public health system. We observed a predominance of surgery among individuals aged 60–79 years (76.65%). A total of 9523 (72.8%) procedures were performed to repair iAAA, of which 6014 (63.2%) corresponded to EVAR and 3509 (36.8%) to OAR. For rAAA repair, 3552 procedures were performed, of which 1595 (44.9%) were EVAR and 1957 (55.1%) OAR. The overall surgical mortality rate was 14.92%. For iAAA repair, the mortality rate was 3.02% for EVAR and 18.30% for OAR. For rAAA repair, the mortality rate was 12.28% for EVAR and 47.57% for OAR.
STC analysis revealed an increase in the overall AAA mortality rate in Brazil (trend statistic = +1.7693, p = 0.0769) and a significant reduction in AAA repair rates (trend statistic = −3.8436, p = 0.0001). The South, Southeast, and Central-West had the highest mortality rates (4.9–8.2), with extensive areas that maintained these high rates throughout the analysis period (persistent hot spot). An area in the Central-West had high mortality rates, which increased even more over the years, from 5.7 to 9.2 (intensifying hot spot) (online supplementary material). Part of the South and a small area of the Central-West showed a small increase in mortality in the last years, from 4.8 to 6.6 (sporadic hot spot). In other areas of high mortality, a downward trend was observed, from 9.6 to 5.2, mainly in the regions of the largest cities in the Southeast and part of the South (diminishing hot spot and historical hot spot). The North and Northeast had the lowest mortality rates. In some areas, these rates increased from 2.3 to 4.2, mainly in the Northeast (diminishing cold spot). The areas identified as sporadic cold spots exhibited a decrease in mortality only in the last years of the analysis (3.1 to 5.2) (Figure 1A).
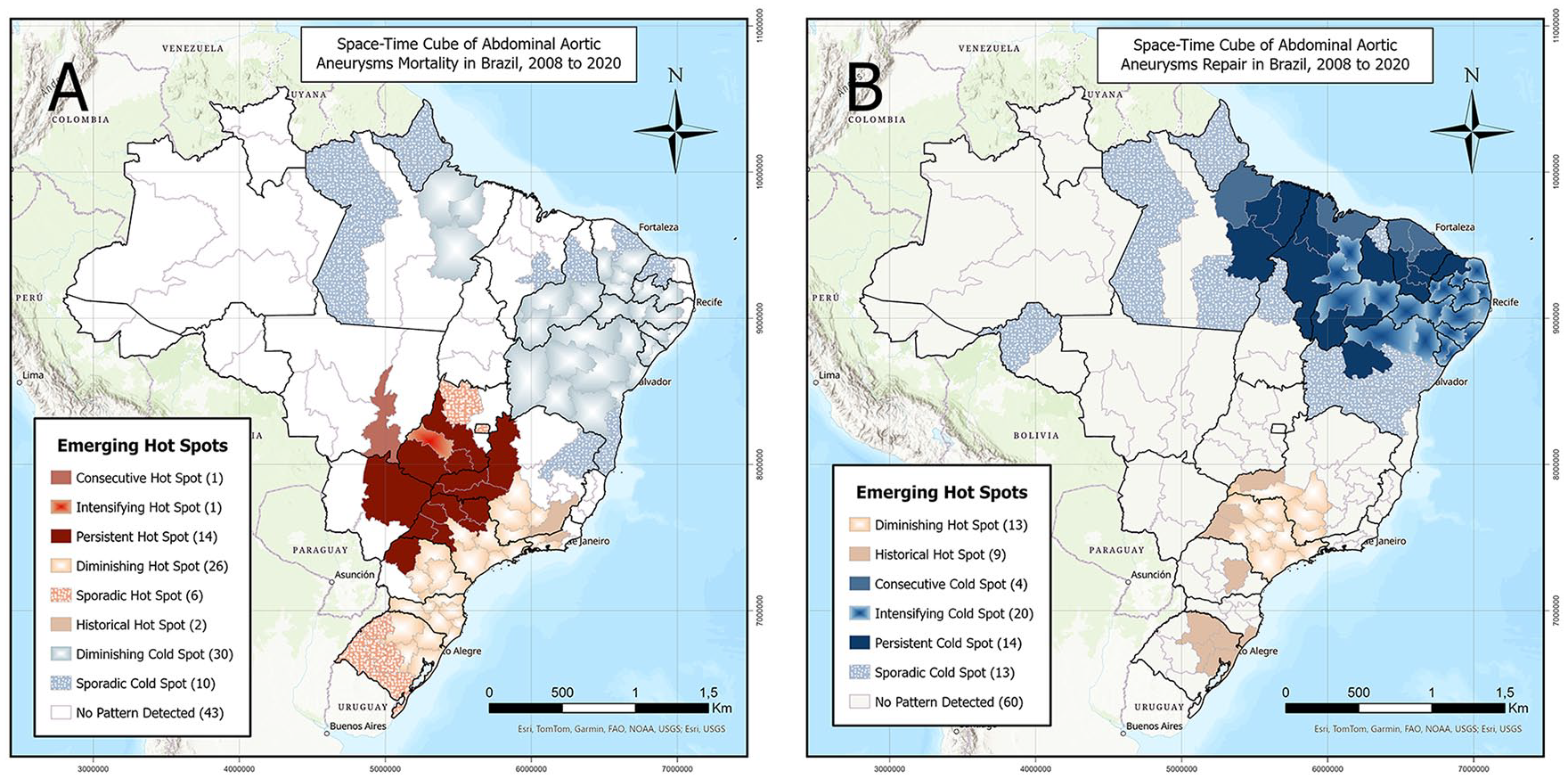
Space–time cube analysis demonstrating spatiotemporal variations in
The South and Southeast were the regions with the largest number of surgical procedures. However, only a few small areas maintained high surgery rates, close to 6.0 (persistent hot spot). Most of São Paulo State and southern Minas Gerais State showed a decrease in procedure rates, from 6.3 to 1.6 (diminishing hot spot). The North and Northeast had the lowest surgery rates. Some areas of the Northeast maintained low surgery rates (about 0.1) throughout the analysis period (persistent cold spot). Extensive areas of the Northeast had low surgery rates, which reduced over the years (from 1.3 to 0.2) (intensifying cold spot). The other areas identified as sporadic cold spots and historical cold spots showed a decrease in surgery rates (from 1.3 to 0.5) at the end of the analyzed period (Figure 1B).
Figure 2 illustrates the Pearson correlations for z-scores derived from the Mann–Kendall trend test applied to Getis-Ord Gi* results for mortality and procedure rates across different regions. The Northeast was the only region with a statistically significant negative correlation (R = −0.65, p < 0.001), a pattern also perceptible in EHSA maps. The other regions had positive correlations; however, only the Southeast and Central-West had significant values, with R = 0.56 (p < 0.001) and R = 0.57 (p = 0.0279), respectively. Figure 3 illustrates the annual fluctuations in AAA mortality and surgery rates across various regions of the country, notably highlighting a discernible decline in mortality rates during the onset of the COVID-19 pandemic in 2020.
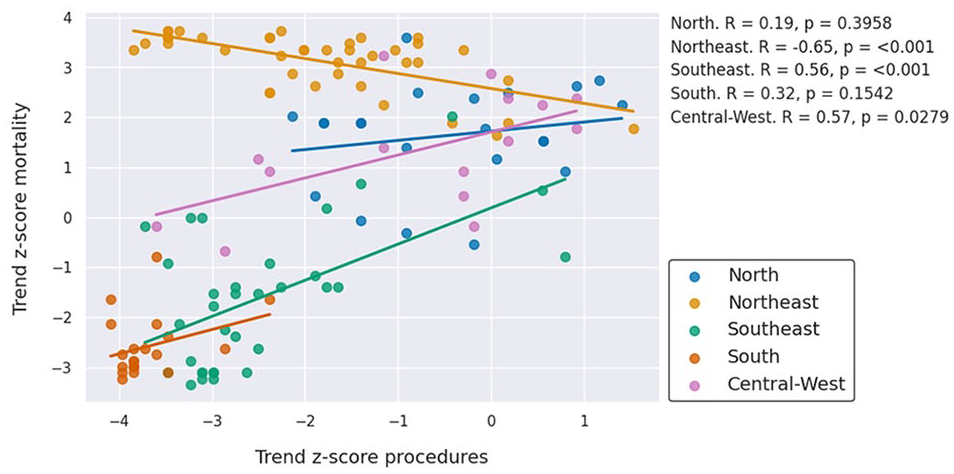
Correlation between Mann–Kendall trend test z-scores for mortality and procedures rates by region.
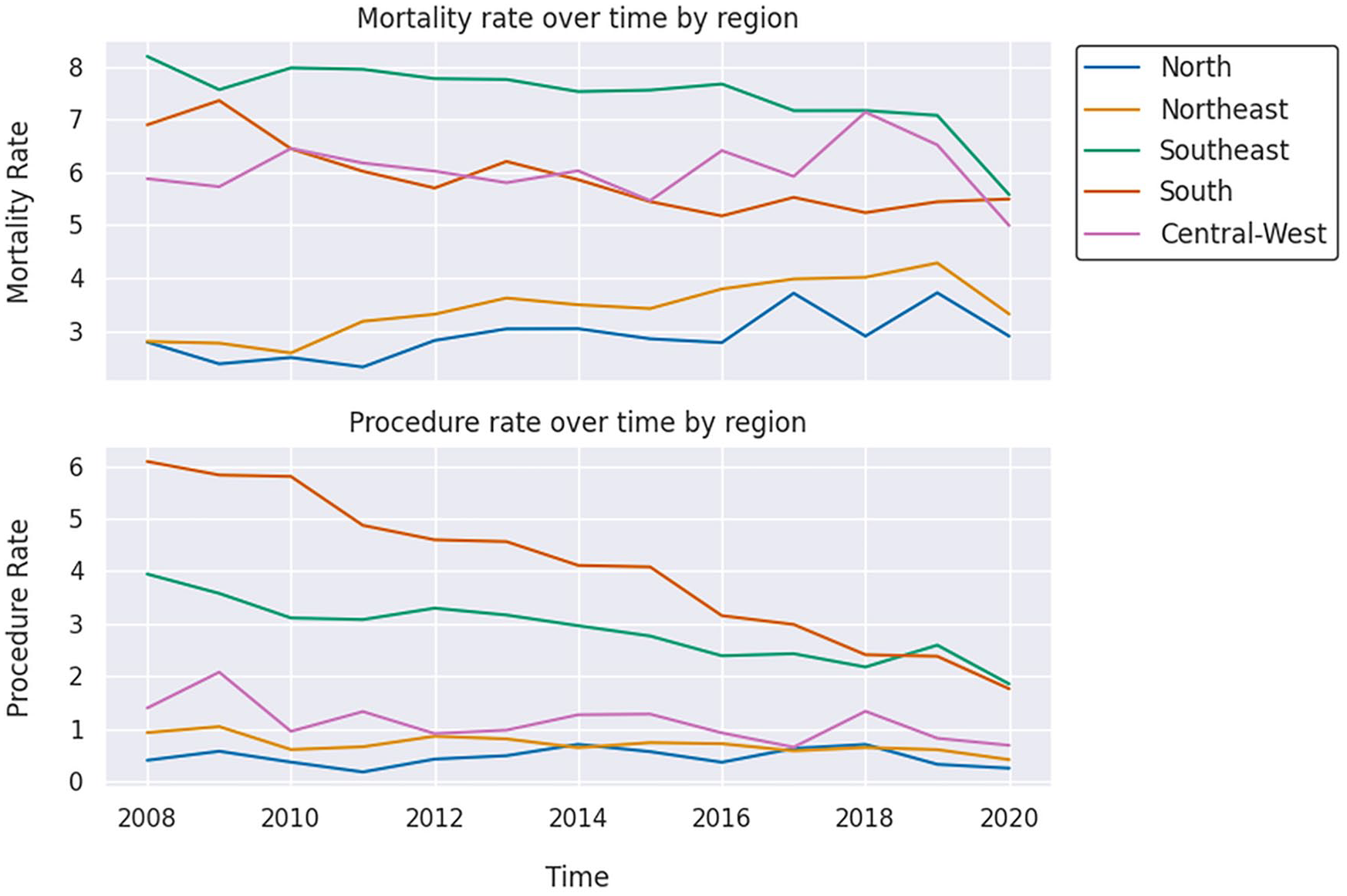
Abdominal aortic aneurysm mortality rate and repair procedure rate over time by region.
Discussion
This study observed a high mortality rate for AAA across Brazil, with a progressive increase that was not accompanied by an increase in surgery rate. Furthermore, mortality from EVAR tended to be lower than mortality from OAR, highlighting a possible disparity between these procedures.
We identified a decline in surgery rates over the years examined. In more advanced regions, there was a large reduction in surgery rate concomitant with a small decrease in the mortality rate. Conversely, in less developed regions and with historically low surgery rates, we noted a decline in procedures along with an increase in AAA mortality. Considering that, during the analyzed period, there were 34,255 deaths from AAA and only 19,024 of these cases received medical assistance, we conclude that there is a great deficit in diagnosis and procedures in Brazil. This finding underscores the impact of challenges in accessing treatment centers on mortality outcomes. Similar observations were reported by Louzada et al., 3 highlighting the need to improve early diagnosis, easily achievable through abdominal ultrasound, and increase the availability of surgical procedures, especially in less developed regions.
In elective cases, patients can be transferred to referral services. However, due to the country’s vast territory and administrative state divisions, many patients lack access to large centers. Some regions are located thousands of kilometers away from capitals or high-volume centers, posing challenges for patients and their families in terms of transportation and accommodation during treatment. In emergency situations, the circumstances become even more dire, with patients facing reduced chances of survival due to the vast distances between rural and metropolitan areas.
The negative correlation observed in the Northeast (Figure 2) suggests how difficulty in accessing surgical treatment can increase mortality in regions of low development. The implementation of a screening program in the Northeast could lead to an increase in diagnosis and a subsequent increase in elective surgical repairs, reversing the negative correlation observed and serving as a model for the rest of the country.
Several studies conducted in highly developed countries demonstrated a mortality rate of 1.2% to 1.4% in the first 30 days after EVAR compared with 3.1% to 4.5% after OAR; differences between mortality rates became negligible only at long-term follow-up.24,25 Our study identified a larger difference in hospital mortality between EVAR and OAR (3.02% vs 18.30%). Multicentric prospective studies in Brazil are needed to obtain robust data for comparison of the mortality rates of procedures in the long term. The data used in this study represent the most comprehensive information currently available.
We believe that the elevated mortality rates and discrepancies between techniques stem from limitations in hospital infrastructure, particularly in nonmetropolitan municipalities. These findings could serve as an incentive for the internalization of hemodynamic services and the training of vascular surgeons, which could reduce mortality from AAA and other cardiovascular diseases. 7 We also recognize that EVAR cases may involve anatomically simpler aneurysms, whereas only the most severe cases are subjected to OAR. Nevertheless, the analysis performed here should not be disregarded, as it encompasses a substantial number of surgeries, and the database used is currently the best available in Brazil. We did not include procedures performed by the private health sector because of the lack of consolidated and unified databases in the country. Furthermore, most of the Brazilian population is served by the public health system.
Study limitations
On the basis of our results, healthcare managers can devise strategies primarily aimed at regions with high mortality rates and low procedure rates. However, some limitations persist, as other factors need to be considered before implementing an intervention, such as distance to treatment centers. Less developed regions might have performed fewer surgeries because of the great distance to treatment centers. The determination of the cause of death in rural areas is more challenging due to limited access to equipment and specialized professionals capable of conducting specific procedures. Furthermore, there is considerable underreporting of mortality data, as many patients in these regions pass away without a specific diagnosis.
It was not possible to associate mortality with individual characteristics, given that analyses were based on intermediate regions. Therefore, complementary research is needed to understand the role of AAA procedures and mortality rates in middle-income countries. Secondary data are susceptible to underreporting. However, the data quality of the Mortality Information System obtained from the website of the Ministry of Health has increased its reliability.
Conclusions
In less developed regions of Brazil, we observed an increase in AAA mortality rates accompanied by a decrease in AAA surgery rates. Given Brazil’s vast territory, many patients face challenges in accessing specialized surgical treatment at referral services. It is imperative for health managers to consider enhancing hospital infrastructure in regions distant from major urban centers. Vital to this effort is the promotion of training programs for vascular surgeons willing to practice in these underserved areas. Though medical residency programs are increasing in Brazil, the implementation of incentive policies becomes crucial to encourage these emerging professionals to establish their practices in rural regions. The culmination of these initiatives holds the potential to significantly enhance the populace’s accessibility to surgical treatment for AAA.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241253732 – Supplemental material for Geographical disparities in access to surgical treatment and mortality rates from abdominal aortic aneurysms in Brazil: A retrospective longitudinal study
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241253732 for Geographical disparities in access to surgical treatment and mortality rates from abdominal aortic aneurysms in Brazil: A retrospective longitudinal study by Rogério do Lago Franco, Pedro Henrique Iora, Miyoko Massago, Matheus Henrique Arruda Beltrame, Ualid Saleh Hatoum, Vinicius Giacomin, Isadora Martins Borba, Sérgio Quilici Belczak, Catherine Ann Staton, Amanda de Carvalho Dutra and Luciano de Andrade in Vascular Medicine
Footnotes
Acknowledgements
See commentary by Brown et al. Solving the Rubik’s cube of AAA mortality in Brazil using space-time cube analysis. Vasc Med 2024; 29: 532-533. 26
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All data are publicly available online from the Brazilian Ministry of Health, National Supplementary Health Agency, and Brazilian Institute of Geography and Statistics.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.