
Abstract
Epidemiological data indicate decreased risk for development and growth of abdominal aortic aneurysm (AAA) among patients with diabetes mellitus (DM). On the other hand, DM adds to increased cardiovascular (CV) morbidity and mortality. In a nationwide observational cohort study of patients registered in the Swedish Vascular Register and the Swedish National Diabetes Register, we evaluated potential effects of DM on total mortality, CV morbidity, and the need for reintervention after elective endovascular aneurysm repair (EVAR) for AAA. We compared 748 patients with and 2630 without DM with propensity score-adjusted analysis, during a median 4.22 years of follow-up for patients with DM, and 4.05 years for those without. In adjusted analysis, diabetic patients showed higher rates of acute myocardial infarction (AMI) during follow-up (relative risk (RR) 1.44, 95% CI 1.06–1.95; p = 0.02), but lower need for reintervention (RR 0.12, CI 0.02–0.91; p = 0.04). There were no differences in total (RR 0.88, CI 0.74–1.05; p = 0.15) or CV (RR 1.58, CI 0.87–2.86; p = 0.13) mortality, or stroke (RR 0.95, CI 0.68–1.32; p = 0.75) during follow-up. In conclusion, patients with DM had higher rates of AMI and lower need for reintervention after elective EVAR than those without DM, whereas neither total nor CV mortality differed between groups. The putative protective effects of DM towards further AAA enlargement and late sac rupture may help explain the lower need for reintervention and absence of excess mortality.
Keywords
Introduction
Abdominal aortic aneurysm (AAA) may lead to rupture and death. 1 Hypertension, hyperlipidemia, and smoking are related to both AAA and atherosclerotic cardiovascular (CV) disease (CVD),2,3 whereas diabetes mellitus (DM) is a major risk factor for CVD4–8 associated with a reduced risk of incidence and expansion of AAA.9–11
AAA can be treated electively with endovascular aneurysm repair (EVAR) or open surgery. 1 Early survival gains with EVAR are followed by late survival benefits of open surgery, resulting in comparable long-term mortality.12,13 Furthermore, AAA-related death is a minor determinant of long-term survival; death from CVD is a threat of larger quantitative importance both in randomized12,13 and in follow-up studies. 14
After elective open AAA repair, patients with DM have higher rates of acute myocardial infarction (AMI) and CV events than those without DM, whereas neither total nor CV mortality differ between groups. 15 The putative effects of DM on AAA might differ after different types of intervention, however. The potentially biologically active mural thrombus and aneurysm sac is left in the body after EVAR in contrast to after open repair with thrombus removal, and might constitute a source of inflammatory mediators influencing CV morbidity. 16 EVAR patients should therefore be assessed separately from those undergoing open repair in this respect. As our knowledge on the importance of DM for mortality and CV morbidity after elective EVAR is derived from small patient materials,17–21 we explored mortality, CV morbidity, and the need for reintervention after elective EVAR in diabetic and non-diabetic patients by propensity score-adjusted analysis to evaluate the putative protective effects of DM on the aortic wall in relation and contrast to the burden caused by DM on the vascular system.4–8
Methods
Databases and procedures
Using the personal identity number unique to every Swedish inhabitant, information from nationwide population-based databases can be linked. As previously reported in detail,15,22 patients were identified by linking data from two national registries: the Swedish Vascular Register (Swedvasc) 23 and the Swedish National Diabetes Register (NDR).8,24
Swedvasc comprises data on all patients undergoing invasive vascular treatment in Sweden. Preoperative risk data are registered together with type of treatment (acute or elective, endovascular or open). Patients are followed up at 1 and 12 months after each procedure.
The NDR contains data on clinical characteristics, risk factors, diabetic complications, and treatment of the majority of Swedish diabetic patients aged over 18 in primary or specialist care.
Patients registered in Swedvasc from 2009 to 2015 after elective EVAR for AAA were identified, and those with a concomitant registration from 2009 to 2015 in the NDR (diabetic group) were compared with those without such registration (non-diabetic group).
Ethical approval
The study was approved by the ethics committee of Lund University (2016/232 and 2016/544). All patients had consented to registration in Swedvasc and the NDR.
Baseline data
Data were retrieved from the Inpatient Register (IPR) administered by the National Board of Health and Welfare (http://socialstyrelsen.se/english),25 with nationwide data for primary and secondary discharge diagnoses and lengths of hospitalization since 1987, 25 the Prescribed Drug Register (PDR) with information about prescriptions since 2005, 26 and the cancer registry 27 for information about comorbidities and drug treatment at baseline.
The IPR uses the International Classification of Diseases, 10th Revision (ICD-10). Comorbidities and drug treatment at baseline included: heart failure (HF), atrial fibrillation (AF), hypertension, coronary heart disease (CHD), and stroke. AMI was defined as I21 (ICD-10). CVD was defined as CHD and/or stroke prior to index date. We also included psychiatric disorders, dementia, cancer, and renal complications. ICD codes used in the study are listed in online supplementary Table 1.
The PDR defined drug treatment. Use of acetylsalicylic acid (ASA), lipid-lowering medications, and anticoagulant therapy was included. Hypertension was defined as three or more prescriptions for antihypertensive medications for 1 year prior to index operation. One prescription is equivalent to 3 months of drug use. Use of lipid-lowering drugs and ASA was defined in a similar manner.
The longitudinal integration database for health insurance and job market studies (LISA; Statistics Sweden) was used to obtain socioeconomic characteristics. Marital status was defined as single, married, divorced or widowed, and educational level as compulsory school, upper secondary school, and college or university. Native country was either Sweden or other.
Follow-up
For follow-up of mortality until 2017 we used the Cause of Death Register with information on causes and time of death, 28 administered by the National Board of Health and Welfare (http://socialstyrelsen.se/english).
Statistical analysis
Mortality, CV morbidity, and aortic reinterventions were compared between patients with and without DM by propensity score-adjusted analysis, as previously reported in detail.15,22 Propensity scores were estimated using a generalized boosted multinomial regression model with an interaction depth of three, a maximum of 10,000 trees, and a shrinkage of 0.01. The optimal number of trees was selected using a stopping rule applied to the degree of balance. Variables included in the propensity score model are listed in online supplementary Table 2. Descriptive statistics are presented as mean, SD, counts, and percentages. The degree of similarity between AAA patients with and without DM is described using standardized mean difference. Incidence rates (IR) for total and CV mortality, AMI, stroke, and aortic reinterventions are estimated as the number of events per 1000 person-years with exact 95% Poisson CIs. Cumulative total and CV mortality, AMI, stroke, and reinterventions are described in Kaplan–Meier curves transformed to estimate distribution rather than survival function. The analyses compares AAA patients with DM to AAA patients without DM using both unadjusted and inverse probability of treatment weighting (IPTW) adjusted Cox regression. As most variables were derived from mandatory health data or population registries, there are virtually no missing values except for smoking, for which approximately 15% of data were missing. The model used in the estimation of the propensity score treats missing values as a separate category and attempts to balance the proportion of missing as well as non-missing values. Analyses were performed using R 3.5.1 through R studio 1.1.456 (http://cran.us.r-project.org/).
Results
Study population and demographic characteristics
Out of 7701 patients registered in Swedvasc after AAA intervention during the period 2009–2015, 5484 (71%) had undergone elective operation, of whom 3378 (62%) had been treated with EVAR. The proportion of elective AAA operations performed with EVAR were 748/1145 (65%) among diabetic patients and 2630/4339 (61%) among those without DM (p = 0.004). Among patients having undergone elective EVAR, the 748 (22%) who had been registered in the NDR due to DM were compared with the remaining 2630 (78%) patients without DM (Figure 1). Of the diabetes cases in the NDR, 98.0% were registered as type 2 DM, 1.4% as type 1, whereas the remaining 0.6% had other types of DM. Median follow-up was 4.22 years for patients with DM and 4.05 years for those without.
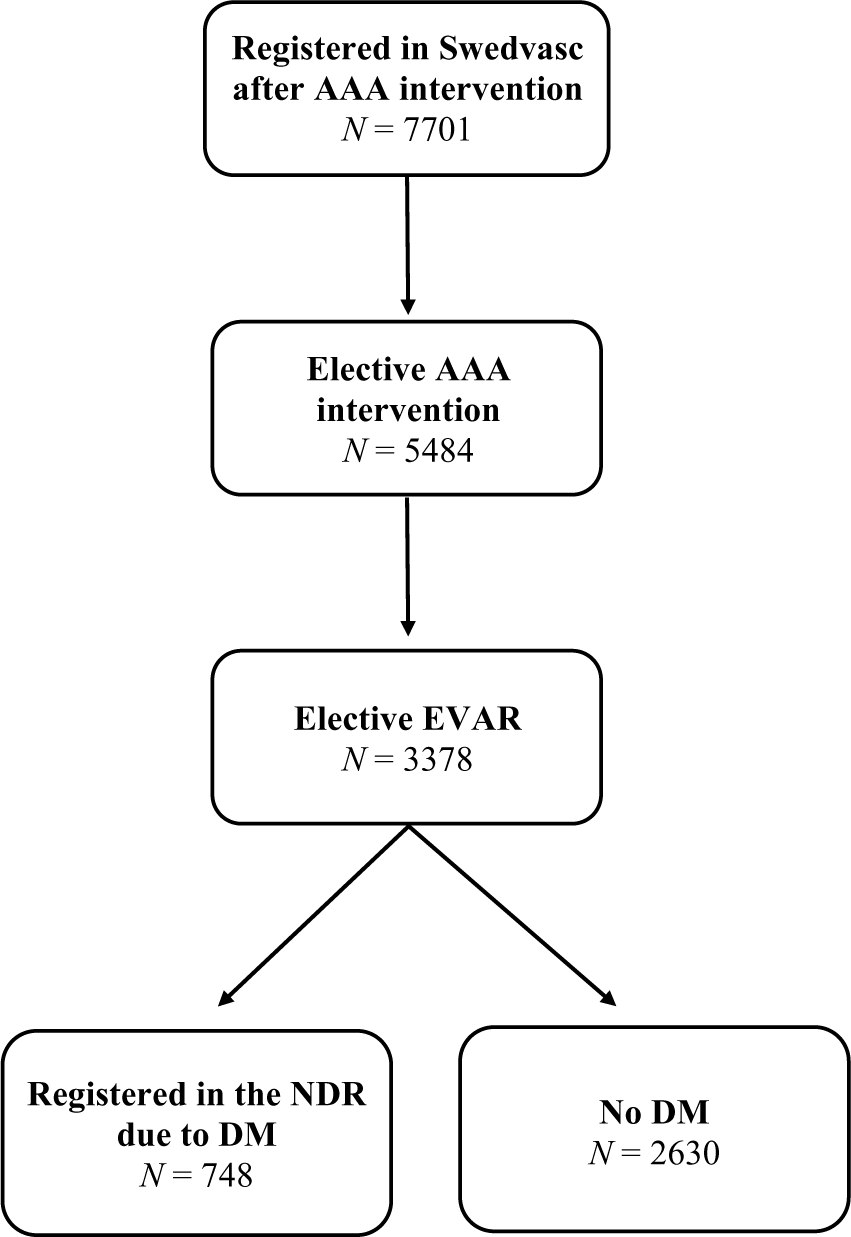
Flow chart of patients in the Swedish Vascular Register (Swedvasc) undergoing elective endovascular AAA repair (EVAR) during the period 2009–2015, with and without registration in the NDR with a diagnosis of DM.
Table 1 presents unadjusted baseline clinical and demographic characteristics. Diabetic patients were younger, less often female, and less often smokers. On the other hand, they were more likely to have a history of hypertension and CHD. Patients without diabetes, on the other hand, were more often born in Sweden, married, and had a higher educational level.
Baseline characteristics of patients with and without diabetes mellitus undergoing elective endovascular AAA repair.
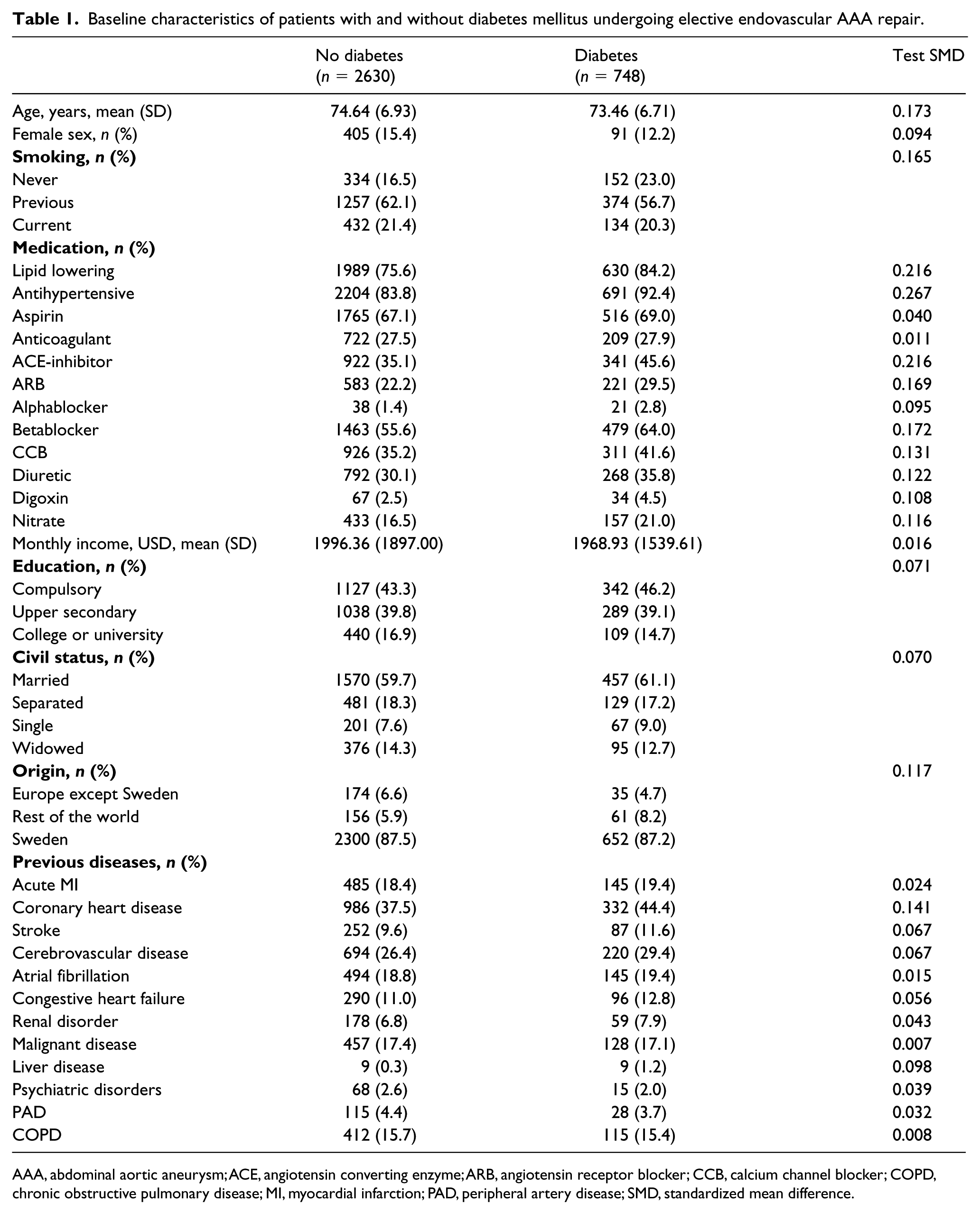
AAA, abdominal aortic aneurysm; ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; CCB, calcium channel blocker; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; PAD, peripheral artery disease; SMD, standardized mean difference.
Outcome analysis
Incidences of the different end points during follow-up are shown in Table 2 and Figures 2–4. Total mortality per 1000 person-years was 60.3 (95% CI 52.2–69.4) in patients with DM and 70.7 (CI 65.8–75.9) in those without. The number of aortic reinterventions per 1000 person-years was 0.3 (CI 0.0–1.7) in patients with DM and 1.2 (CI 0.6–2.0) in those without. Unadjusted proportions of patients with different events are shown in online supplementary Table 3. The proportions of patients dying during the 5-year follow-up were 0.409 (CI 0.368–0.448) in the diabetic group and 0.295 (CI 0.274–0.314) in the group without DM.
Events of total and CV mortality, AMI, stroke, and aortic reintervention during follow-up of patients with and without diabetes mellitus after elective endovascular AAA repair.
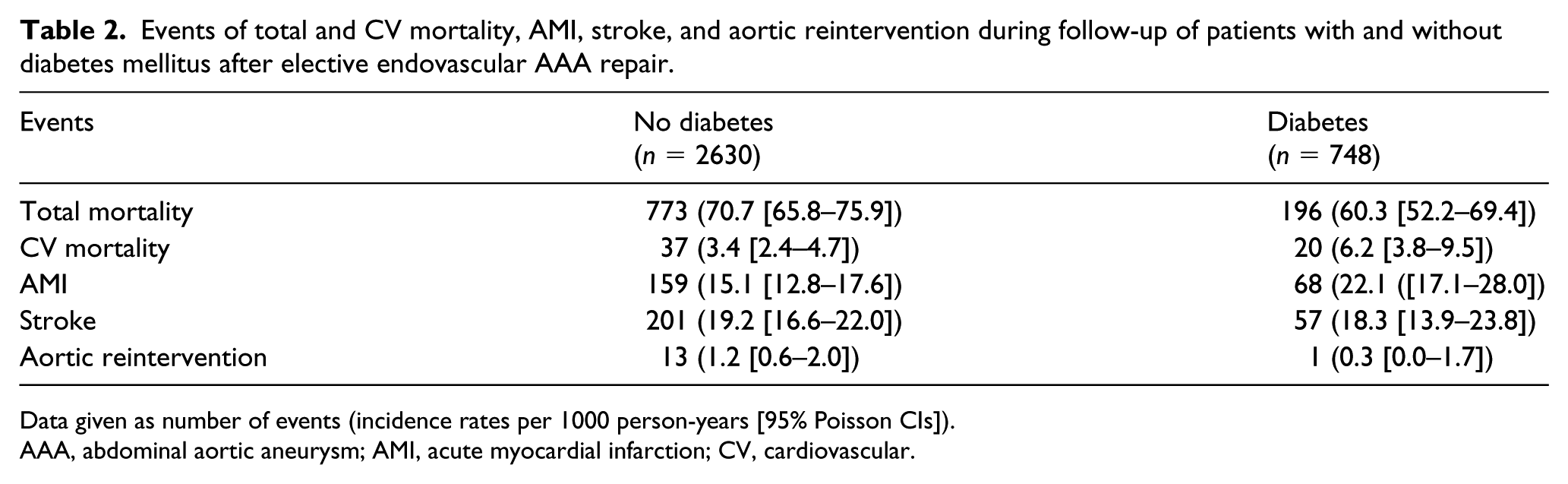
Data given as number of events (incidence rates per 1000 person-years [95% Poisson CIs]).
AAA, abdominal aortic aneurysm; AMI, acute myocardial infarction; CV, cardiovascular.
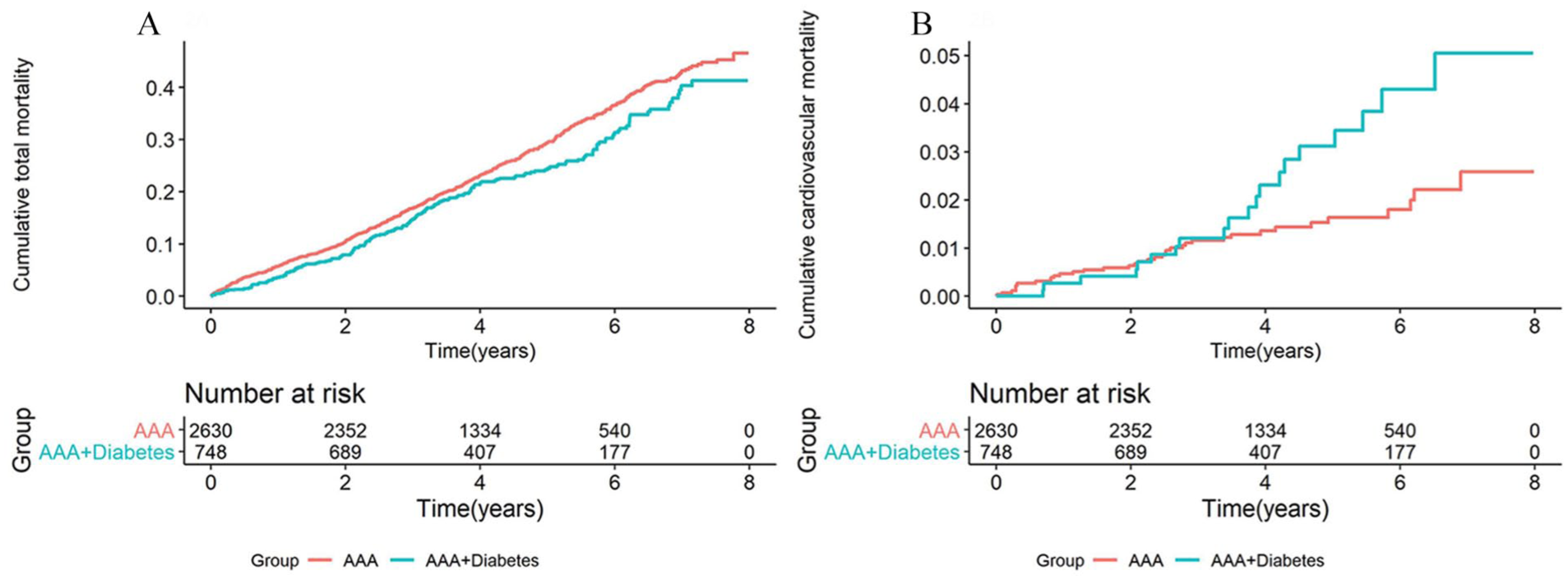
Crude Kaplan–Meier curve showing the cumulative total (A) and CV (B) mortality after elective endovascular AAA repair in patients with and without diabetes.
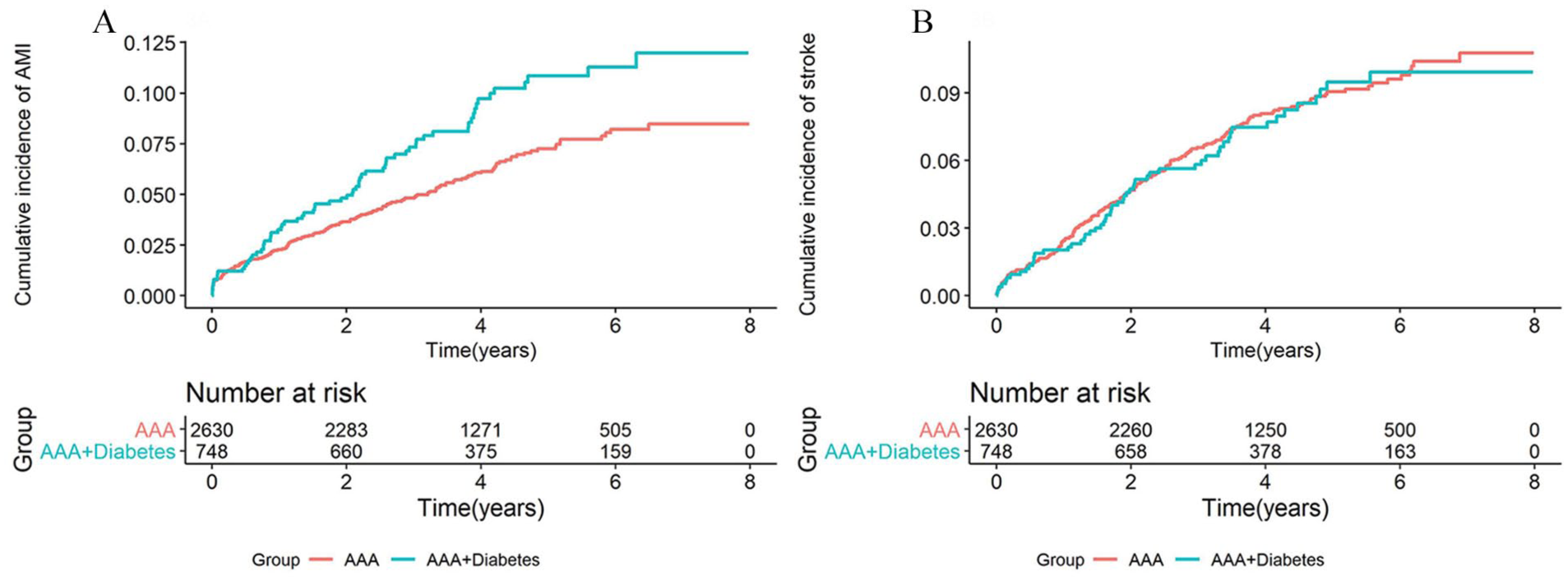
Crude Kaplan–Meier curve showing the cumulative incidence of AMI (A) and stroke (B) after elective endovascular AAA repair in patients with and without diabetes.
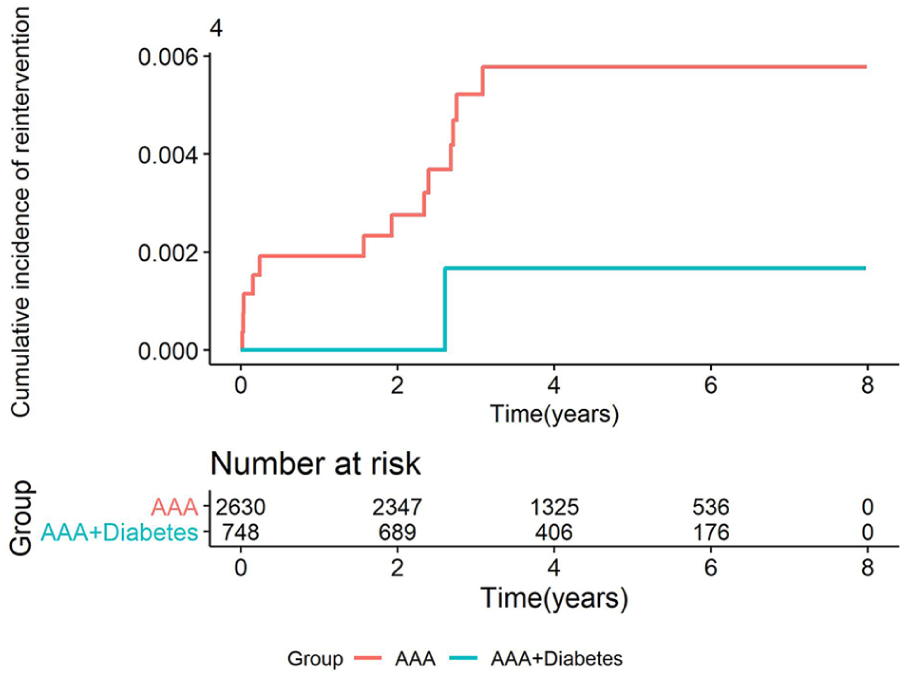
Crude Kaplan–Meier curve showing the cumulative incidence of aortic reintervention after elective endovascular AAA repair in patients with and without diabetes.
In IPTW-adjusted Cox regression (Table 3), diabetic patients showed higher rates of AMI (relative risk (RR) 1.44, CI 1.06–1.95; p = 0.02), but a lower need for reintervention (RR 0.12, CI 0.02–0.91; p = 0.04) than patients without DM. There were no differences in total (RR 0.88, CI 0.74–1.05; p = 0.15) or CV (RR 1.58, CI 0.87–2.86; p = 0.13) mortality, or stroke (RR 0.95, CI 0.68–1.32; p = 0.75) between groups.
Unadjusted and adjusted analysis of RR for total and CV mortality, AMI, stroke, and aortic reintervention for patients with diabetes mellitus compared to patients without during 5 years of follow-up after elective endovascular AAA repair.
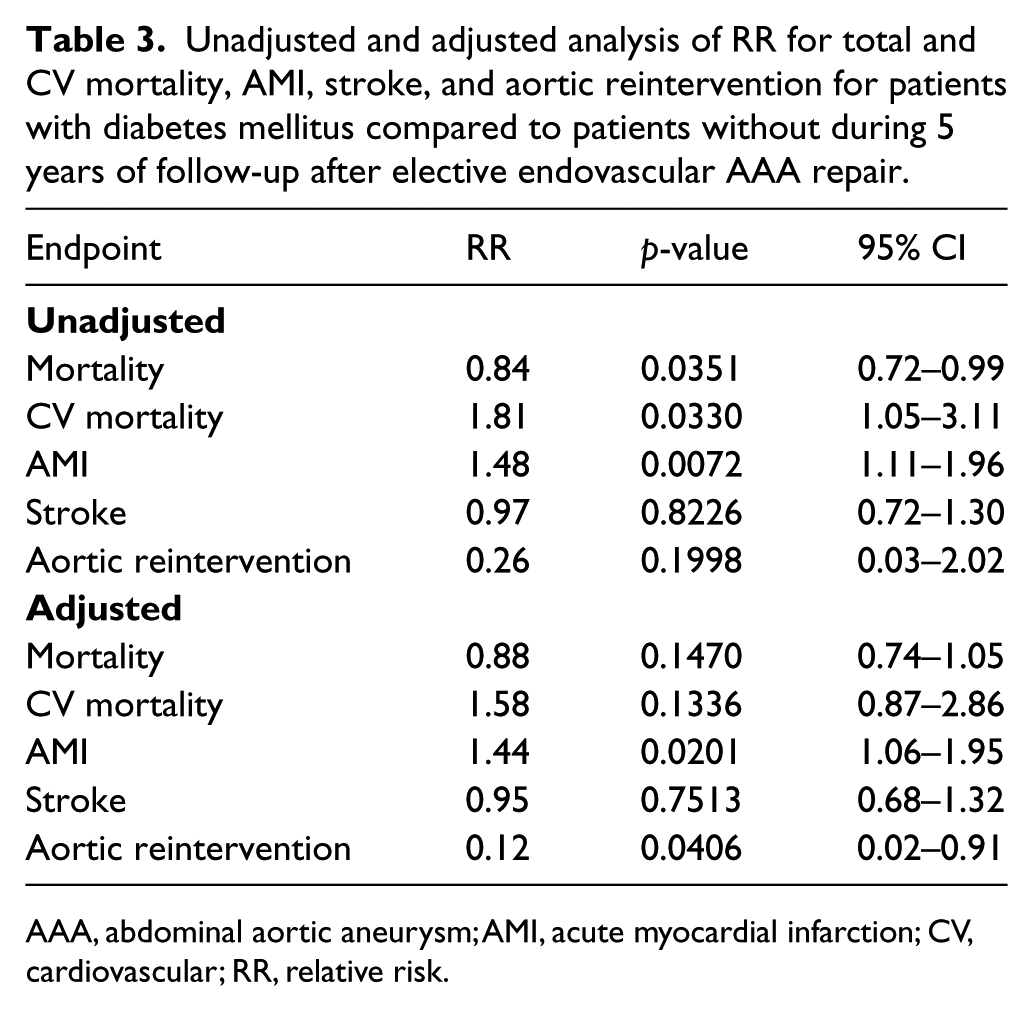
AAA, abdominal aortic aneurysm; AMI, acute myocardial infarction; CV, cardiovascular; RR, relative risk.
In the diabetic group, disease duration or HbA1c level were not related to total or CV mortality, AMI, or stroke (online supplementary Table 4).
Discussion
The adjusted analysis in this nationwide observational study showed that patients with DM had a significantly increased risk of AMI, but had a lower need for aortic reintervention after elective EVAR for AAA compared to patients without DM. On the other hand, neither total, nor CV mortality differed between groups after adjustment for baseline differences.
In a recent meta-analysis of 12 studies, including 82,306 patients undergoing elective EVAR, all-cause mortality was associated to several factors such as age, sex, aneurysm diameter, smoking, heart failure, and coronary, peripheral and cerebral vascular disease, as well as chronic pulmonary and renal disease. 17 As expected, patients with and without DM in our study differed concerning several of these relevant important background variables, such as smoking, concomitant disease, and medication. When evaluating the observed differences between groups in our study, such as an expected4–8 increased risk for AMI and a lower need for aortic reintervention in the diabetic group, it is therefore important that adjustment for these important differences at baseline had been performed. We therefore speculate that the putative protective effects of DM upon AAA development and expansion9–11,29–32 might perhaps help explain that neither total nor CV mortality was increased in the diabetic group by counteracting the negative effects of DM on the vascular system, but the study does not allow us to draw any conclusions concerning potential underlying mechanisms.
The decreased risk for aortic reintervention in the DM group is also interesting, albeit the total number of reintervention cases in our cohort was low. As mortality did not differ between groups, the lower need for reintervention can hardly be explained by an excess of CV or other deaths in the diabetic group.
The present results differ partly from those in our previous analysis of diabetic patients after elective open repair, 15 in whom AMI rates were higher but reinterventions too few to be reported. Compared to those undergoing open AAA repair, EVAR patients are more susceptible to late aneurysm-related complications due to progress of aortic degeneration and dilatation resulting in late aneurysm sac rupture, device failures, or endoleaks 12 necessitating reintervention. Such complications were not assessed in this study, but might perhaps arise less often in patients with DM; in a large cohort of 1479 patients, DM was shown to be associated with a decrease in aneurysm sac enlargement and a lower need for reintervention after EVAR. 33 However, in a recent meta-analysis of 24 studies with 14,754 patients, no association between DM and sac shrinkage after EVAR was found. 34
In the EVAR trial 112,13 comparing EVAR with open aneurysm repair in elective AAA patients, survival was > 70% 4 years after EVAR (i.e. comparably higher than in our study), probably reflecting the recruitment of patients with fewer comorbidities than commonly occurring in clinical practice into a clinical trial. Of the 12 studies included in the previously mentioned meta-analysis on elective EVAR, 17 only four18–21 assessed the importance of DM for long-term mortality, and one of these 21 reported significantly increased mortality in patients with an HbA1c > 6.5%. However, it is important to note that Hjellestad included only 66 patients in the analysis, 21 whereas on the other hand, follow-up was extended to 71 months. In another meta-analysis on mortality after elective AAA repair, including both EVAR and open surgery, 35 the picture was slightly different, however. The pooled hazard ratio for mortality conferred by DM among 44,211 patients in 14 different studies was reported at 1.34 (95% CI 1.2–1.49). Patients having undergone open repair were included in many of these studies, however, and as comorbidities such as DM might well influence the choice of interventional method, the results cannot be directly compared to ours. The proportion of patients undergoing EVAR among those operated on electively for AAA was higher in the diabetic group than among those without diabetes, indicating selection mechanisms also in our population. This highlights the importance of evaluating patients treated with different methods separately when assessing the potential effects of DM on results and prognosis after elective AAA surgery. As mortality and morbidity after acute AAA surgery are a completely different issue, we refrain from direct comparison with our results in such patients showing reduced mortality in patients with diabetes. 22
In our study, the well-established increased risk for CV morbidity and mortality in patients with diabetes4–8 was reflected only in an increased rate of AMI during follow-up. Cardioprotective medication is recommended in all patients with AAA, 1 but the proportions of patients using statin and antihypertensive drugs in our study were higher in the diabetic group, which might have led to better risk factor control. ACE inhibitors have been suggested to slow progression of AAA, but no such effects could be demonstrated in a randomized setting. 36 When discussing potential effects of pharmacological treatment on our results, however, it has to be remembered that differences in lipid and blood pressure-lowering drugs were adjusted for, whereas we could not adjust for antidiabetic drug use as it differed between groups by definition. The potential effects of antidiabetic therapy upon our outcomes therefore cannot be separated from the effects of the diabetic disease itself.
Data on weight, length, and body mass index were not available, but on the other hand, obesity does not increase the odds of major adverse outcomes in patients undergoing EVAR. 37
The prognosis after elective EVAR was not related to duration of DM in the diabetic group. The duration of hyperglycemia might be of relevance for putative protective effects of DM upon AAA.9–11,29–32 When glycemic control was related to aortic diameter at subsequent ultrasound screening for AAA 30 years later, 38 no relationships were found, neither do 65-year-old men with newly detected DM have increased aortic diameter or AAA prevalence. 39 Nevertheless, the reduced risk of AAA in DM is related to diabetes duration, with decreasing odds ratios from 0.50 after 3–5 years to 0.37 after 12 years. 40 With increasing disease duration in the DM group during prolonged follow-up, more reliable differences in mortality, morbidity, and complications might therefore appear.
Neither did we find any relationship between the prognosis after elective EVAR and HbA1c among diabetic patients. Potential positive effects of DM on the risk of AAA have been suggested to be enhanced if glycemic control is poor,10,40 but, in contrast, HbA1c is clearly related to an adverse prognosis concerning atherosclerosis. 41
We have not analyzed the anatomical features of the AAA, the type of anesthesia, or whether the proportions of different types of aortic endografts implanted were the same in the two groups. Neither do we have any data on compliance with the instructions for use of the different grafts. This is a limitation of our study as different graft types might be associated with differences in long-term prognosis, 42 but randomized, direct, long-term comparisons are lacking.
Our nationwide, valid 43 registry data on the performed endovascular intervention, the diagnosis of diabetes, comorbidities, and outcomes, on the other hand, lends strength to our results. As Swedvasc has been validated concerning index interventions, 43 but not concerning reinterventions however, the need for reintervention in our study might be underestimated. As it is hard to conduct a randomized clinical trial to answer the current question, longitudinal, observational studies of large unselected materials are relevant.
Conclusion
This nationwide, observational, longitudinal follow-up suggests that patients with DM have higher rates of AMI, but a lower need for aortic reintervention during 4 years of follow-up after elective EVAR than those without DM, whereas neither total nor CV mortality differ between groups. Putative protective effects of DM on AAA complications may partly explain these findings. Future research is needed to separate the potential such effects of the diabetic state in itself from the effects of antidiabetic medication.
Supplemental Material
10.1177_1358863X19870243_Supplementary_tables – Supplemental material for Survival, cardiovascular morbidity, and reinterventions after elective endovascular aortic aneurysm repair in patients with and without diabetes: A nationwide propensity-adjusted analysis
Supplemental material, 10.1177_1358863X19870243_Supplementary_tables for Survival, cardiovascular morbidity, and reinterventions after elective endovascular aortic aneurysm repair in patients with and without diabetes: A nationwide propensity-adjusted analysis by Soumia Taimour, Tarik Avdic, Stefan Franzén, Moncef Zarrouk, Stefan Acosta, Peter Nilsson, Mervete Miftaraj, Björn Eliasson, Ann-Marie Svensson and Anders Gottsäter in Vascular Medicine
Footnotes
Acknowledgements
The authors thank the steering groups of the Swedvasc and NDR registries and the patients enlisted in the registries for making this study possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by grants from the Ernhold Lundström Foundation, Research Funds at Skåne University Hospital and at Region Skåne, the Hulda Ahlmroth Foundation, the Swedish Government under the LUA/ALF agreement and from the NDR (Swedish National Diabetes Register), Gothenburg, Sweden. Swedvasc and the NDR are funded by the Swedish Association of Local Authorities and Regions (SKL). The funders did not have any role in study design, analysis, interpretation or writing.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.