
Abstract
Background:
There is wide variation in stress test utilization before major vascular surgery and adherence to practice guidelines is unclear. We defined rates of stress test compliance at our institution and led a quality improvement initiative to improve compliance with American Heart Association (ACC/AHA) guidelines.
Methods:
We implemented a stress testing order set in the electronic medical record at one tertiary hospital. We reviewed all patients who underwent elective, major vascular surgery in the 6 months before (Jan 1, 2022 – Jul 1, 2022) and 6 months after (Aug 1, 2022 – Jan 31, 2023) implementation. We studied stress test guideline compliance, changes in medical or surgical management, and major adverse cardiac events (MACE).
Results:
Before order set implementation, 37/122 patients (30%) underwent stress testing within the past year (29 specifically ordered preoperatively) with 66% (19/29) guideline compliance. After order set implementation, 50/173 patients (29%) underwent stress testing within the past year (41 specifically ordered preoperatively) with 80% (33/41) guideline compliance. In the pre- and postimplementation cohorts, stress testing led to a cardiovascular medication change or preoperative coronary revascularization in 24% (7/29) and 27% (11/41) of patients, and a staged surgery or less invasive anesthetic strategy in 14% (4/29) and 4.9% (2/41) of patients, respectively. All unindicated stress tests were surgeon-ordered and none led to a change in management. There was no change in MACE after order set implementation.
Conclusions:
Electronic medical record-based guidance of perioperative stress testing led to a slight decrease in overall stress testing and an increase in guideline-compliant testing. Our study highlights a need for improved preoperative cardiovascular risk assessment prior to major vascular surgery, which may eliminate unnecessary testing and more effectively guide perioperative decision-making.
Background
Major adverse cardiac events (MACE) are a significant contributor to perioperative morbidity after vascular surgery.1,2 Identification of patients at high risk for MACE has therefore been a priority in clinical practice and a focus of both prospective and retrospective studies.3–7 Specifically, nearly four million stress tests in total are performed annually in the United States with an estimated cost of over US$500 million dollars.8,9 Although the American College of Cardiology/American Heart Association (ACC/AHA) has developed a step-wise algorithm to identify patients who may benefit from preoperative stress testing and risk stratification, it currently remains unclear to what extent these govern real-world practice. 10
There have been several registry and claims-based studies that have examined stress testing paradigms in contemporary surgical practice.1,8,11–14 Despite documenting important variations in practice, these large administrative data sets remain limited in their ability to discern granular and important information surrounding testing indications, 12 and consequential changes in perioperative medical or surgical management.12,13 Furthermore, despite persistent variation in preoperative stress testing across centers having been well-reported,1,11 it remains unclear how many preoperative tests are compliant with current evidence-based guidelines. Since nonguideline-compliant tests may account for significant healthcare costs, 15 defining current guideline compliance rates may reveal an important opportunity for quality improvement.
Therefore, the objective of this study was to document stress test compliance rates with ACC/AHA guidelines, and to determine whether test results led to changes in perioperative management. To accomplish this, we implemented a preoperative cardiac risk order set in the electronic stress test ordering workflow at our institution. We hypothesized that many stress tests performed for preoperative risk stratification remain noncompliant with available guidelines and have little clinical impact in patient management. We defined ‘noncompliance’ as stress testing in patients not meeting ACC/AHA guideline criteria. We examined rates of nontesting in patients meeting guideline criteria separately. We also hypothesized that implementation of an electronic order set would improve overall stress test ordering compliance with ACC/AHA guidelines.
Methods
This study was approved by the Dartmouth-Hitchcock Institutional Review Board and a waiver for specific and individual consent was obtained. All patient data and health information were protected and de-identified prior to publication.
Data source, and inclusion and exclusion criteria
This study was comprised of all patients undergoing elective major vascular operations performed at Dartmouth-Hitchcock Medical Center between Jad January 31, 2023. Major vascular operations included were carotid endarterectomy (CEA), carotid artery stenting (CAS), open aortic aneurysm repair (OAAA), endovascular aortic aneurysm repair (EVAR), infrainguinal arterial bypass (INFRA), and suprainguinal arterial bypass (SUPRA). CAS was comprised of patients who underwent transcarotid artery revascularization or transfemoral carotid artery stenting. These six major vascular operations were combined into three groups: carotid, abdominal aortic aneurysm repair (AAA), and lower-extremity bypass (LEB). Carotid was comprised of CEA and CAS; AAA was comprised of OAAA and EVAR; and LEB was comprised of INFRA and SUPRA.
We excluded minor or major amputations, dialysis access cases, venous procedures, and minor percutaneous peripheral vascular interventions (i.e., angiogram of the lower-extremity, upper-extremity, renal, or mesenteric vessels with or without percutaneous interventions such as angioplasty, stenting, or atherectomy) as these are vascular interventions associated with lower levels of procedural risk.2,16 Urgent and emergent cases were excluded, since preoperative risk stratification with stress testing might be foregone in these situations if it would not change clinical management (i.e., the decision to operate). All charts were reviewed by a single data abstractor (AP), and any questions surrounding the patients’ clinical course were resolved by adjudication by two additional reviewers (JAC, DHS) or by consultation with the operative attending surgeon.
Phases of the study
We conducted this study in two phases. First, we performed a comprehensive retrospective review of all elective major vascular operations performed at Dartmouth-Hitchcock Medical Center between January 1 and July 1, 2022, to document stress testing rates, patient clinical characteristics, and perioperative outcomes.
Next, we implemented a preoperative cardiac risk order set specific to the stress test ordering workflow within the electronic medical record (EMR) (Epic Systems, WI, USA). This was created to assess compliance rates, over the study interval, with current ACC/AHA guidelines (online Supplemental Figure 1). After order set implementation, all elective major vascular operations were studied in a prospective fashion between August 2022 and January 2023.
Electronic medical record order set
The EMR order set is comprised of three questions assessing the indication and guideline compliance of the stress test for preoperative clearance (online Supplemental Figure 2). Clinicians were still permitted to order the test irrespective of guideline compliance, though were required to enter a reason for ordering a study that was noncompliant with endorsed indications. This quality improvement effort was developed in accordance with the SQUIRE 2.0 guidelines.
Medical consultation and risk stratification
We reviewed the rates of preoperative medical consultation (i.e., cardiology, stroke neurology, or internal medicine consults) for all patients in the retrospective and prospective cohorts, as well as rates of preoperative medical optimization, preoperative invasive procedures, and perioperative cardiac events. Preoperative medical optimization was defined as a medication change made by the surgeon or consulting physician prior to the operation to the following medications: beta-blockers, angiotensin converting enzyme-inhibitors (ACE-inhibitors) or angiotensin receptor blockers (ARBs), statins, diuretics, and antiplatelet or anticoagulant agents.
Primary and secondary outcomes
For our primary outcome, we examined stress test compliance with the 2014 ACC/AHA guidelines. 10 Stress tests were deemed ‘unindicated’ if they were performed despite moderate, good, or excellent functional status; if they were ordered without documented assessment of functional status; or if they would not change management regardless of the result. To assess ‘noncompliance’, we first determined rates of stress testing in patients not meeting ACC/AHA guideline criteria. We separately assessed rates of nontesting in patients meeting guideline criteria for testing. We also compared guideline adherence before and after order set implementation. The secondary outcome was assessment of change in medical or surgical management attributable to stress testing. We defined medical change as adjustment to the patient’s cardiovascular medication regimen (e.g., increasing a beta-blocker dose) based on the stress test result. A change in surgical management was defined as selection of a less invasive or staged procedure (e.g., axillobifemoral bypass rather than open aortobifemoral bypass, or transfemoral carotid stent rather than carotid endarterectomy), or modification in anesthetic strategy (e.g., selection of neuraxial anesthesia rather than general anesthesia) attributable to the stress test result.
Next, we evaluated the time from initial vascular surgery clinic evaluation to the date of elective major vascular surgery, and compared time-to-surgery in patients who did and did not get a preoperative stress test. Lastly, we assessed whether the following additional outcomes varied with preoperative medical consultation: the rate of preoperative cardiovascular medication changes, the rate of preoperative cardiac test ordering (i.e., echocardiogram or stress testing), and perioperative major adverse cardiac events (defined as a composite of 30-day myocardial infarction, stroke, or death).
Statistical analysis
Data analysis was performed using descriptive statistics, with continuous variables reported as means with standard deviations or medians with ranges as appropriate. All categorical variables are reported as percentages. Two-sample t-tests were used to evaluate univariate associations for continuous outcomes, and the chi-squared test was used to evaluate univariate associations for dichotomous outcomes. Statistical analyses were performed using Stata 15 (College Station, TX, USA).
Results
Patient demographics and clinical characteristics
The demographic variables for the retrospective (n = 122) and prospective patient cohorts (n = 173) are presented in Table 1.
Patient demographics and clinical characteristics of retrospective (January – July 2022) and prospective (August 2022 – January 2023) cohorts according to procedure category.

Columns designated as (R) for retrospective cohort and (P) for prospective cohort.
AAA, abdominal aortic aneurysm repair; Carotid, carotid surgery; COPD, chronic obstructive pulmonary disease; LEB, lower-extremity bypass; SPECT, single-photon emission computed tomography.
In the retrospective group, the mean age was 69 ± 10 years and 75% of patients were men. Most patients (99%) in the retrospective group were White. Patients in this group were substantially comorbid, with 31% of patients having a history of coronary revascularization, 77% having hyperlipidemia, and 89% having current or former tobacco exposure (Table 1). Notably, the patient cohort reflected complex disease with 18% of patients undergoing carotid surgery having had a history of prior carotid surgery, and 21% of patients undergoing lower-extremity bypass having had a history of prior lower-extremity bypass (suprainguinal or infrainguinal). Most patients were on a preoperative aspirin (88%) and statin (85%).
The prospective cohort had a similar clinical phenotype. The mean age was 70 ± 8.9 years and 74% of patients were men, 97% of patients were White, and 27% of patients had a history of prior coronary revascularization (Table 1).
Stress testing rates and patterns
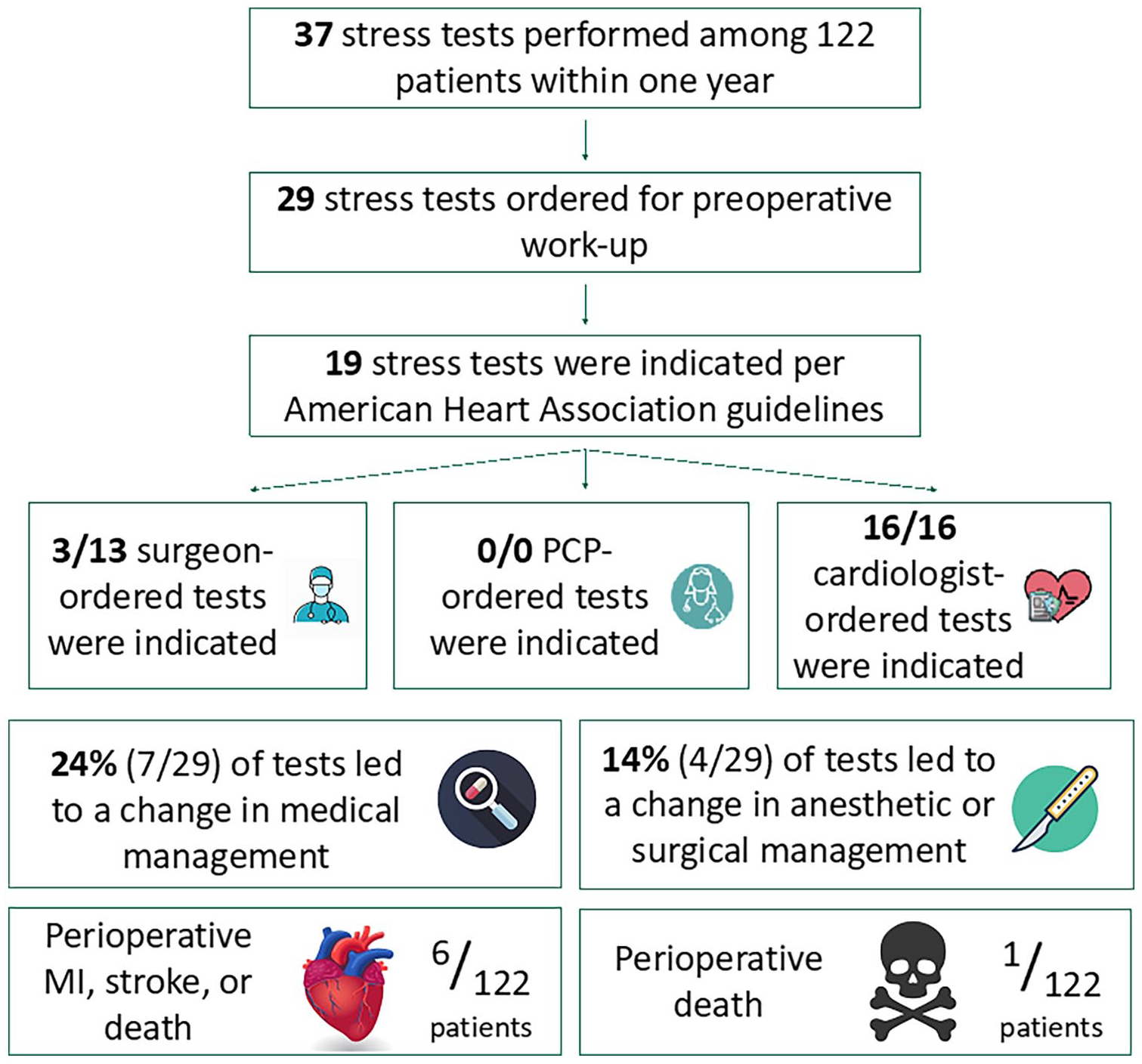
Stress testing prior to surgery was common in the retrospective cohort, with 47% (57/122) undergoing preoperative testing (online Supplemental Table 1). In this cohort, 60% of the tests were SPECT pharmacologic nuclear stress tests. Of the overall stress tests in this group, 37 (30%) were performed within 1 year of the index operation and 29 tests were ordered specifically for preoperative work-up (Figure 1). Among those stress tests that were performed in the retrospective group, 57% were negative and 2.9% were positive for ischemia (2.9% small), 34% were positive for scar (9% small, 11% moderate, 14% large), and 5.8% were positive for ischemia and scar (2.9% small, 2.9% large).
Stress testing patterns in the retrospective cohort (n = 122; January – July 2022).
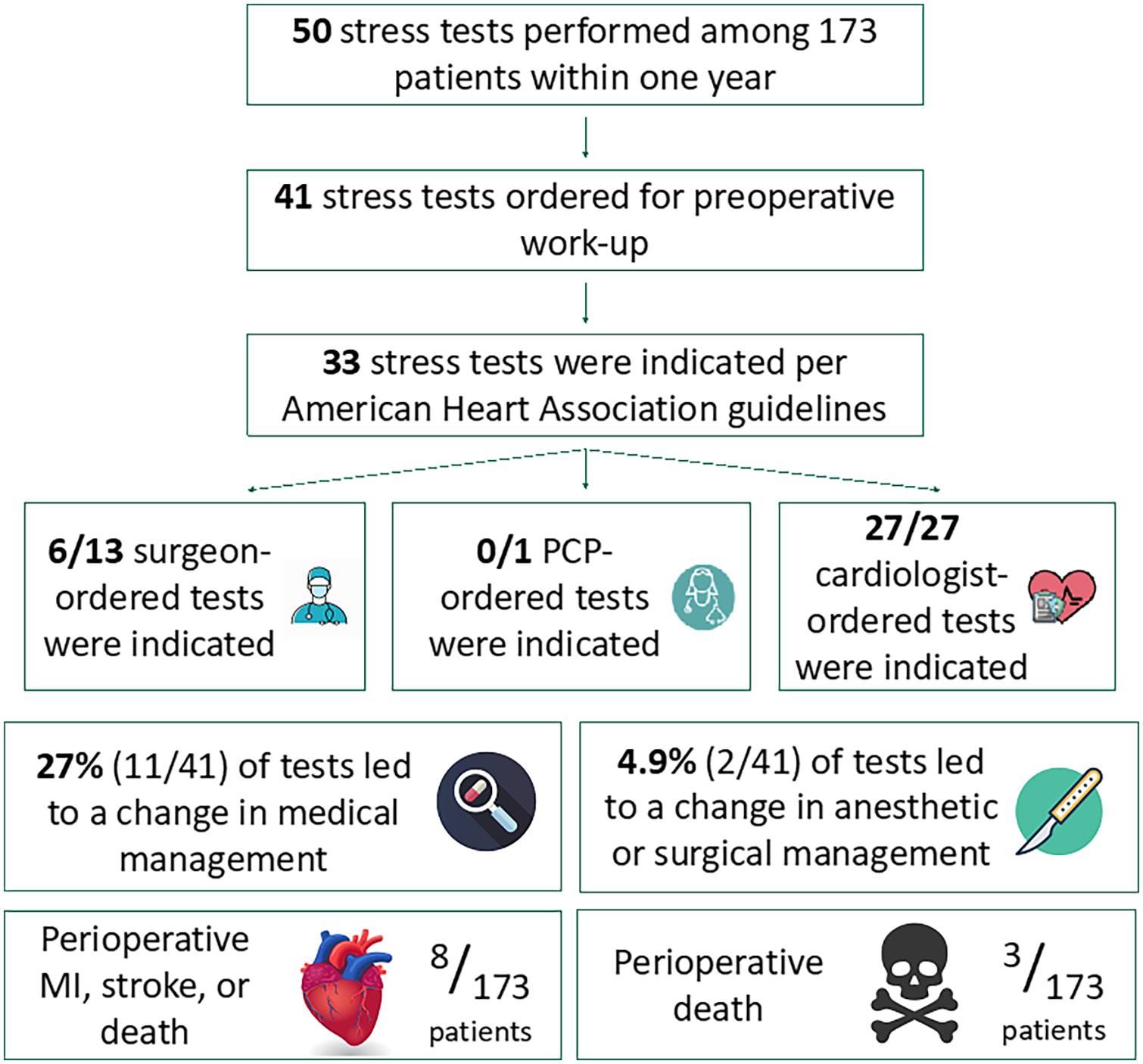
In the prospective cohort, 93 stress tests were performed at any time among the 173 patients, again with 63% of these tests being SPECT pharmacologic stress tests (online Supplemental Table 2). Fifty stress tests (29%) in this group were performed within 1 year of the index operation and 41 tests were ordered specifically for preoperative work-up (Figure 2). Of performed stress tests, 56% were negative, 10% were positive for ischemia (2% small, 6% moderate, 2% large), 20% were positive for scar (8% small, 7% moderate, 5% large), and 14% were positive for ischemia and scar (2% small, 9% moderate, 3% large).
Stress testing patterns in the prospective cohort (n = 173; August 2022 to January 2023).
Guideline compliance and management change with stress testing
Twenty-nine stress tests in the retrospective cohort were ordered specifically for preoperative work-up. The stress test compliance rate with the ACC/AHA guideline prior to order set implementation was 66% (19/29). In this group, 24% (7/29) of preoperative stress tests led to a change in medical management with beta-blocker initiation or cardiac catheterization whereas 14% (4/29) of tests led to a change in surgical or anesthetic management with staged surgery or modified anesthetic strategy (Figure 1).
Compliance increased to 80% (33/41) after order set implementation (Figure 2). After order set implementation, 27% (11/41) of tests led to a change in medical management whereas 4.9% (2/41) of tests led to a change in surgical or anesthetic management. Importantly, none of the 18 unindicated stress tests across both cohorts led to a change in medical, surgical, or anesthetic management.
Patterns and outcomes of patients not undergoing stress testing
Among all patients with a history of coronary artery disease (CAD) in both cohorts, 66% (78/118) did not undergo stress testing. In comparison, 78% (138/177) of patients without a history of CAD did not undergo preoperative stress testing across both cohorts. Of 163 patients across both cohorts without a history of CAD who had a functional status assessment available, 78% (127/163) did not undergo stress testing. Only two of these 163 patients without a history of CAD who had a functional status assessment available experienced a MACE event over the study period.
We identified eight patients in the retrospective cohort and seven in the prospective cohort who met guideline criteria for preoperative stress testing but were not tested. Four of the 15 patients who met guideline criteria but were not stress tested had a MACE event.
Surgical delays with and without stress testing
Among patients who did not undergo a preoperative stress test, the median time from initial vascular surgery clinic evaluation to the date of elective major vascular surgery was 22 days (IQR: 7–57 days) prior to order set implementation. Similarly, after order set implementation, the median time from clinic evaluation to the date of elective surgery was 30 days (IQR: 9–50 days).
Among patients who underwent a preoperative stress test, the median time from initial vascular surgery clinic evaluation to the date of elective major vascular surgery was 55 days (IQR: 29–103 days) prior to order set implementation. In contrast, after order set implementation, the median time from clinic evaluation to the date of elective surgery was 21 days (IQR: 10–69 days).
Stress testing by specialty and setting, and trends in compliance
Prior to order set implementation, 23% (3/13) of vascular surgeons were compliant with the ACC/AHA guidelines, compared to 100% compliance (16/16) among cardiologist-ordered stress tests (Figure 1).
After order set implementation, the rate of vascular surgeon-ordered, guideline-compliant stress tests doubled to 46% (6/13). The rate of guideline-compliant cardiologist-ordered tests remained at 100% (27/27) even after order set implementation (Figure 2). The rate of cardiology-ordered stress testing increased from 55% (16/29) in the retrospective cohort to 65% (26/40) in the prospective cohort. There was a corresponding decrease of 27% in surgeon-ordered stress testing over time, from 45% (13/29) in the retrospective cohort to 33% (13/41) in the prospective cohort.
Lastly, of the 87 stress tests performed within 1 year of surgery across both cohorts, 25% (22/87) were ordered in the inpatient setting and 75% (65/87) were ordered in the outpatient setting. Stress testing in the inpatient versus outpatient setting was not statistically associated with preoperative medication optimization or MACE (p > 0.05).
Major adverse cardiac events and stress testing
Among the 122 patients in the retrospective cohort, six patients experienced the composite outcome of perioperative myocardial infarction, stroke, and death within 30 days (online Supplemental Table 3). Of these six patients, none had a preoperative stress test performed and four had preoperative medical management changes made. There was one perioperative death in this group, due to complications of decompensated systolic heart failure.
After order set implementation, the rate of MACE remained low: eight patients experienced the composite outcome of perioperative myocardial infarction, stroke, and death within 30 days (online Supplemental Table 4). Fifty percent of the MACE events in the prospective group occurred in those who did not have a preoperative stress test, and six patients had preoperative medical management changes made. There were three perioperative deaths in the prospective cohort: two deaths were due to noncardiac etiologies, and one was due to complications of biventricular heart failure. There was no statistical association between order set implementation and 30-day MACE (p = 0.91).
Lastly, five patients in the retrospective group and seven patients in the prospective group experienced 30-day postoperative heart failure. Two patients in the retrospective group and four patients in the prospective group experienced 30-day postoperative arrhythmia.
Patterns of preoperative medical consultation and risk stratification
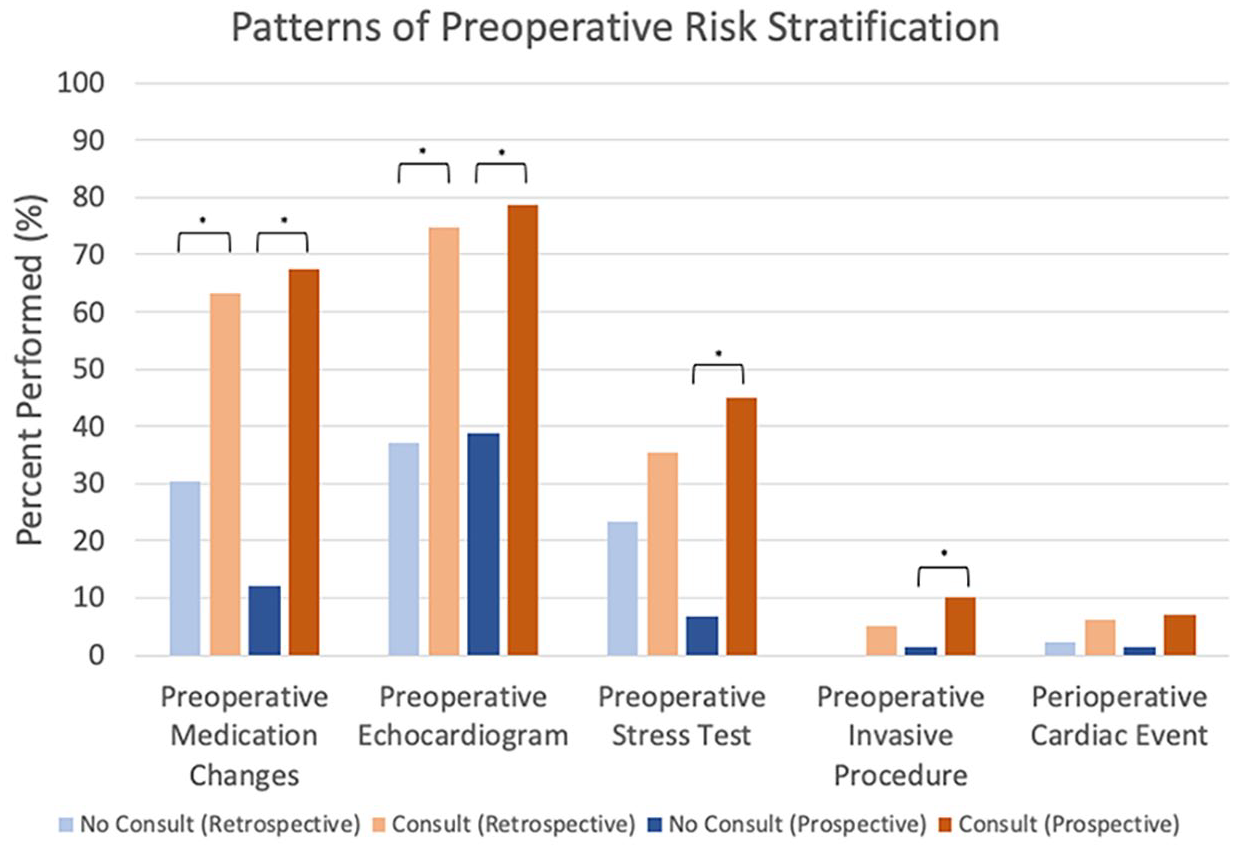
The rates of preoperative risk stratification across the retrospective and prospective cohorts are summarized in Figure 3. Both pre- and postorder set implementation and preoperative medical consultation by a primary care provider, cardiologist, or stroke neurologist (prior to carotid surgery) led to statistically significant increases in: preoperative cardiovascular medication adjustment in the retrospective (p < 0.001) and prospective (p < 0.001) cohorts, preoperative echocardiogram ordering in the retrospective (p < 0.001) and prospective (p < 0.001) cohorts, preoperative stress test ordering in the prospective cohort (p < 0.001), and preoperative invasive procedures in the prospective cohort (p = 0.0177). Risk stratification by consult subspecialty is presented in online Supplemental Tables 5 and 6.
Rates of preoperative medical consultation and risk stratification before and after electronic medical record order set implementation.
However, preoperative medication adjustment was not statistically associated with a reduction in perioperative 30-day major adverse cardiovascular events in the retrospective (p = 0.45) or prospective groups (p = 0.064). There was a decrease in preoperative medication adjustments made by vascular surgeons after order set implementation, from 30% to 12%, but a slight increase in medication adjustment by medical consultants (63% in the retrospective group, 67% in the prospective group) across all six procedures.
Discussion
In this study, we found that use of an EMR-based stress test ordering tool doubled surgeon compliance (from 23% to 46%) with ACC/AHA testing practice guidelines. Moreover, 31% of stress tests were associated with a change in clinical (i.e., medical, surgical, or anesthetic) management across the entire study period. Somewhat surprisingly, none of the noncompliant tests led to changes in clinical management. Despite this improvement in stress test use, there was no observed change in documented MACE events after order set implementation and the majority of patients who suffered MACE did not get a stress test. These findings indicate that an EMR tool can potentially improve stress test guideline compliance, which may serve as a significant opportunity for quality improvement.
Previous registry-based studies have been unable to determine the impact of stress testing on clinical management and operative decision-making, as the indication for testing and other important variables are not routinely available in procedural registries or administrative datasets.12,13 This single-center study allowed us to address these persistent limitations and demonstrate that roughly 25% of preoperative stress tests led to a change in medical management (i.e., medication change or cardiac catheterization), and 5–14% of tests led to a modification in surgical or anesthetic strategy. Review of individual patient records revealed that the majority of the ‘medical management’ changes were medication adjustments (six of seven in the retrospective group, and seven of 11 in the prospective group), with only 14% of stress tests culminating in cardiac catheterization. Medical management most often entailed the addition of a beta-blocker consistent with prior evidence for beta-blocker efficacy in patients undergoing major vascular surgery with myocardial ischemia on preoperative testing. 17
Importantly, preoperative stress testing was not associated with a decrease in postoperative MACE. This is consistent with our prior published work,1,11 and supports the notion that stress tests are not independent or singularly sufficient for the prevention of MACE. A large fraction of patients who experienced MACE did not have a preoperative stress test (100% in the retrospective group and 50% in the prospective group). Additionally, four of the 15 MACE events across both cohorts occurred in patients who were not stress tested but met guideline criteria on retrospective review—in other words, stress testing was under-used in these cases. On the other hand, MACE events in patients who were not stress tested but did not meet guideline criteria suggest that current stress test guidelines are unable to optimally identify all patients at high risk of progression to MACE. Stress tests are likely best used as a component of a preoperative risk stratification paradigm rather than as an isolated litmus test for ruling-in or ruling-out potential major adverse cardiac events in the postoperative period.
Implementation of the electronic medical record order set led to changes in compliance and testing trends over the course of this year-long study. First, the overall rate of stress testing—including tests performed prior to preoperative evaluation—decreased slightly after order set implementation (30% to 29%). There was also a significant increase in vascular surgeon compliance with the ACC/AHA guidelines from 23% to 46%, as well as an increase in overall provider compliance from 66% to 80%. This change persisted, although surgeons were able to order nonguideline-compliant tests with a written rationale. Additionally, incorporation of the ACC/AHA guideline into the stress test ordering workflow appeared to shift ordering patterns from vascular surgeons to cardiologists, with a corresponding decrease in surgeon-ordered tests and concurrent increase in medical consultant-ordered tests. This increase in preoperative medical consultation after order set implementation may have been driven by the consultants’ greater familiarity with current risk stratification protocols. Thus, it appears that increased guideline compliance through preoperative medical consultation has the potential to significantly reduce unnecessary testing and its associated direct costs. 15
The median delay from initial clinic evaluation to elective surgery in patients who were preoperatively stress tested, compared to nonstress tested patients, decreased after order set implementation. This was observed despite more preoperative medical consultation in the prospective cohort, which may be expected to delay surgery in some patients. However, the decrease from a 33-day delay preimplementation to no significant delay postimplementation is based on a small sample size and future studies are needed to evaluate the effect of stress testing on surgical delays.
Though increased medical consultation was not necessarily associated with management change in this study—as has been reported previously18,19—it does appear to be associated with improvement in real-world guideline compliance. Therefore, cardiologists and medical consultants may be better stewards of stress testing prior to elective surgery to reduce cost. It is also notable that medication optimization was performed significantly more frequently with preoperative medical consultation. Patients with minimal antecedent contact with the healthcare system were able to have important medication adjustments, as well as have long-term outpatient cardiologist care established. These medications such as beta-blockers, antiplatelet medications, and ACE inhibitors in indicated patients have been shown to improve long-term morbidity and mortality. 20 Despite these impacts, increased medical consultation was not associated with decreased perioperative MACE, which may be due, in part, to the greater comorbidity profiles among those being referred for preoperative medical risk stratification.
Even after order set implementation, providers were permitted to order stress tests determined to be unindicated per the current ACC/AHA guideline. These providers were required to enter a rationale in the stress test ordering workflow. Eight stress tests over the prospective study period from August 2022 to January 2023 were unindicated: seven of these patients were at risk for coronary artery disease but were able to achieve 4 metabolic equivalents of activity, and one was determined not to be at high risk for coronary disease. Sample reasons provided included ‘surgeon requested’ and ‘significant coronary history status post a three-vessel CABG’, or ‘disagreement with the guideline’. These responses suggest that unindicated testing in this study was driven primarily by surgeon request and the belief that coronary disease burden despite moderate functional status requires further risk stratification, which is contrary to the current guideline. This identifies a need for future educational efforts targeted towards surgeons, focused on the evidence backing the ACC/AHA guidelines.
Heart failure accounted for more perioperative cardiac events in this study than myocardial infarction (five patients vs five patients in the retrospective cohort, and six patients vs three patients in the prospective cohort, respectively). It is important to note that MACE has been defined variably in prior literature and some groups have previously included heart failure and arrhythmia in the composite endpoint. 21 However, the ACC/AHA algorithm does not consider a clinically significant history of heart failure in ‘CAD risk’, and may not adequately predict risk for common complications like heart failure exacerbation. The Revised Cardiac Risk Index and the American College of Surgeons NSQIP Surgical Risk Calculator improve on these limitations by including conditions such as congestive heart failure, recent ascites or sepsis, and acute renal failure in the assessment of cardiac risk. 22 Our study suggests that though the 2014 ACC/AHA guideline has its role in preoperative risk stratification, other risk indices assessing non-CAD factors should be applied in conjunction to effectively guide perioperative medical decision making.
Study limitations
There are several limitations to this work. First, patients who never underwent surgery based on a high-risk stress test result were not captured in this study. These patients may have proceeded to undergo medical management alone, which is arguably a unique endpoint of stress testing. This work was able to elucidate which patients went on to undergo staged or less invasive surgery, and future work will aim to study the cohort of patients undergoing stress testing whose surgery was deferred. Second, the six operations studied herein exclude cases such as branched-fenestrated endovascular aortic repair, which are large-magnitude operations prior to which stress testing is often performed. Third, the studied patient population is homogeneous, with over 95% of patients being White and 75% being men, thereby limiting its generalizability to other populations. Future studies with a larger and more diverse sample could expand on this work by exploring differences in preoperative referral and testing rates by race and sex. Fourth, provider stress testing patterns and types of stress tests ordered in this study are institution-specific—a different mix of stress electrocardiogram, echocardiogram, nuclear stress testing, and stress cardiac MRI may have yielded different results. Fifth, as discussed above, routine use of the Revised Cardiac Risk Index or the NSQIP Surgical Risk Calculator would have more comprehensively assessed non-CAD factors and may have led to higher rates of preoperative medical and cardiac optimization. Lastly, this is a retrospective cohort study with its usual limitations and contains a small total sample size of approximately 300 patients at a single institution. Despite the small number of patients, we were able to glean important trends in stress testing and likely changes in practice patterns with order set implementation.
Conclusions
There remains a significant dearth of information regarding provider- and institution-level stress testing practice patterns, and the rates of guideline compliance with the most recent ACC/AHA guidelines. We demonstrate that approximately one-quarter of current preoperative stress tests, obtained at a tertiary care medical center, led to a change in medical management, and 5–10% led to a change in surgical or anesthetic management. No unindicated stress tests prompted a change in clinical management, calling their ultimate clinical utility into question. Moreover, as all unindicated stress tests were vascular surgeon-ordered, even after a quality improvement initiative, there is a need for educational efforts targeted toward this group to improve guideline compliance.
Implementation of a stress test order set led to a significant shift from surgeon-ordered tests to medical consultant-prompted testing. This change in practice also corresponded with an increase in both surgeon guideline compliance and overall testing compliance. More frequent preoperative medical consultation did not lead to a reduction in MACE, but it was associated with more consistent medication optimization and likelihood for testing compliance. Our findings demonstrate a need for improved preoperative cardiovascular risk assessment prior to major vascular surgery, including a more comprehensive assessment of non-CAD factors. This has the potential to streamline care, eliminate unnecessary costly testing, and help optimize patient selection paradigms prior to vascular surgery.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241247537 – Supplemental material for Most preoperative stress tests fail to comply with practice guideline indications and do not reduce cardiac events
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241247537 for Most preoperative stress tests fail to comply with practice guideline indications and do not reduce cardiac events by Aravind S Ponukumati, Jesse A Columbo, Stanislav Henkin, Jocelyn M Beach, Bjoern D Suckow, Philip P Goodney, Salvatore T Scali and David H Stone in Vascular Medicine
Footnotes
Acknowledgements
This study was presented in the Poster Competition at the 2023 Vascular Annual Meeting on June 16, 2023 (National Harbor, MD, USA).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding was obtained from the 2022 Vascular Study Group of New England (VSGNE) Quality Improvement Program (QIP).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.