
Abstract
Background:
The utilization and cost-effectiveness of stress testing before abdominal aortic aneurysm (AAA) repair remains insufficiently studied. We examined the variation and financial implications of stress testing, and their association with major adverse cardiovascular events (MACE).
Methods:
We studied patients who underwent elective endovascular (EVAR) or open AAA repair (OAR) at Vascular Quality Initiative centers from 2015 to 2019. We grouped centers into quintiles of preoperative stress testing frequency. We calculated the risk of postoperative MACE, a composite of in-hospital myocardial infarction, heart failure, or death, for each center-quintile. We obtained charges for stress tests locally and applied these to the cohort to estimate charges per 1000 patients.
Results:
We studied 32,459 patients (EVAR: 27,978; OAR: 4481; 283 centers). Stress test utilization varied across quintiles from 13.0% to 68.6% (median: 36.8%) before EVAR and 15.9% to 85.0% (median: 59.4%) before OAR. The risk of MACE was 1.4% after EVAR and 10.2% after OAR. There was a trend towards more common MACE after EVAR among centers with higher utilization of stress testing: 0.9% among centers in the lowest quintile, versus 1.7% in the highest quintile (p-trend = 0.068). There was no association between MACE and stress testing frequency for OAR (p-trend = 0.223). The estimated financial charges for stress testing before EVAR ranged from $125,806 per 1000 patients at 1st-quintile centers, to $665,975 at 5th-quintile centers. Charges before OAR ranged from $153,861 at 1st-quintile centers, to $825,473 at 5th-quintile centers.
Conclusion:
Stress test use before AAA repair is highly variable and associated with substantial cost, with an unclear association with postoperative MACE. This highlights the need for improved stress testing paradigms prior to surgery.
Keywords
See Commentary: Davis FM, Henke PK. Cardiac stress testing prior to abdominal aortic surgery: Widely variable utilization, costly, and of unclear benefit. Vasc Med 2022;27:477–478.
Introduction
Ischemic heart disease remains a primary cause of peri- and postoperative morbidity and mortality after major vascular surgery, with a reported prevalence between 40% and 70% among patients undergoing these procedures.1–3 Stress testing has evolved over the past three decades as a noninvasive means to stratify patients’ cardiac risk, and in doing so to optimally reduce perioperative cardiovascular events.1,4,5 Accordingly, preoperative stress testing is endorsed by the American Heart Association for patients with poor (< 4 metabolic equivalents) or unknown functional capacity or multiple cardiac risk factors if the result will alter management. 6 Not surprisingly, these recommendations are applicable to the comorbidity profiles of many patients who undergo abdominal aortic aneurysm (AAA) repair. 7 As a result, stress testing is performed in approximately half of all patients undergoing elective endovascular (EVAR) and open AAA repair in contemporary practice.8–10
However, the impact of widespread stress testing remains inadequately studied. We previously identified significant variability in stress test use across centers in New England, 10 and across the United States. 11 Furthermore, we also demonstrated that the cardiac risk profiles among patients who underwent preoperative stress testing failed to differ from patients who proceeded directly to surgery. 11 Moreover, the financial impact of such ubiquitous testing remains poorly defined.
Therefore, our objective was to further define the variation and financial impact of current widespread stress testing patterns before AAA surgery. In addition, we sought to explore whether contemporary stress testing practice patterns were associated with superior detection of postoperative adverse cardiac events. Our hypothesis was that increased stress testing would significantly increase cost without a notable reduction in adverse events. We believe that this clinical research question has substantial implications for patients, physicians, payors, and institutions alike.
Methods
Human subjects’ protection
All data used in this study were de-identified and collected from a registry designated as a Patient Safety Organization by the Agency for Healthcare Research and Quality. The study received approval from the Dartmouth-Hitchcock Institutional Review Board and a waiver for specific and individual consent was obtained. All patient data and health information were protected, and all outcomes were de-identified. No testing or procedures were performed in this study.
Data source, inclusion, and exclusion criteria
We used the Vascular Quality Initiative (VQI) registry to study a contemporary sample of patients who underwent EVAR or open AAA repair from 2015 to 2019. Data availability, applications, and information on participating centers are available at www.vqi.org. All patients in the registry over the study interval were eligible for inclusion. We excluded patients who underwent urgent or emergent procedures for symptomatic or ruptured AAAs, as well as those for whom the indication for repair was unknown and patients for whom it was unknown whether a preoperative stress test was performed.
Primary exposure
Our primary exposure of interest in this study was stress testing. The VQI captures data on preoperative stress testing and classifies the result as: not performed, normal, myocardial ischemia, myocardial scar, or myocardial scar with ischemia.
Rates of stress test utilization
We calculated the percent of patients who underwent preoperative stress testing prior to EVAR and open AAA repair at each center over the study period. We determined the proportion of stress tests that were positive for ischemia, scar, or both, for each center. We then grouped centers into quintiles according to the center-level percent of patients who underwent preoperative stress testing.
Primary outcomes
Our primary outcomes were threefold. First, we determined variation in preoperative stress test use across VQI centers. Second, we examined estimated financial charges as a proxy for procedure-associated costs attributable to preoperative stress testing per 1000 patients. Third, we studied postoperative (in-hospital) major adverse cardiovascular events (MACE). We defined MACE as a composite of in-hospital myocardial infarction (defined as clinical symptoms with ischemic electrocardiographic changes or troponin elevation); in-hospital heart failure exacerbation; or in-hospital all-cause mortality.
Estimating the cost impact of stress testing
To estimate the cost impact of preoperative stress testing, we ascertained the stress test type-specific charges associated with stress testing at Dartmouth-Hitchcock Medical Center (DHMC), an academic tertiary care center in New Hampshire. We first determined the types of stress tests (e.g., electrocardiographic stress testing, stress echocardiography, and nuclear stress testing), and the relative proportions of those tests that patients underwent for calendar year 2019. In 2019, there were 3662 stress tests performed. These represented 1212 (33.1%) electrocardiographic stress tests, 1797 (49.1%) stress echocardiograms, and 653 (17.8%) nuclear stress tests. The local charges for these tests were $416 per electrocardiographic stress test, $1163 per stress echocardiogram, and $1475 per nuclear stress test. The number of patients who underwent each of these stress tests at DHMC in 2019 was determined and a weighted average was performed to estimate the mean charge per patient. We then multiplied this weighted average by the percent of stress testing performed for centers in each respective quintile. We used this to estimate the expected charges for stress testing per 1000 patients treated at centers that utilized stress testing at that quintile’s respective frequency.
Statistical analysis
Continuous variables are reported as means with SDs or medians with IQRs as appropriate, and categorical variables are reported as percentages. We calculated the percent of patients at each VQI center who underwent a preoperative stress test, and the percent of those tests that were positive. Next, we grouped centers according to their respective quintile of preoperative stress testing frequency. We next calculated the cost of stress testing for each quintile using the weighted average of stress testing performed as noted in the methodologic section above. We then calculated the percent of patients that experienced a MACE in each quintile and compared the quintiles with a test of trend. Finally, we performed a subanalysis to determine whether patients who underwent surgery despite a positive preoperative stress test had a higher likelihood of MACE than patients who had a negative stress test or those who were not tested. To do this we created a logistic regression model where the exposure was a positive preoperative stress test, and the outcome was MACE. We adjusted for all covariates in Table 1. We repeated this for both the EVAR and open AAA cohorts. The number of patients meeting inclusion for each step of the analysis is found in Figure 1. Patients with missing stress test information (EVAR n = 47, open AAA repair n = 5) were excluded from cost and variation calculations. Patients with missing data on baseline characteristics (EVAR n = 747, open AAA repair n = 149) were excluded from the regression models. All patients had information on MACE. Baseline characteristics were calculated out of the known, nonmissing values for each variable. Statistical analyses were performed using Stata Statistical Software, Release 15 (StataCorp LP, College Station, TX, USA).
Demographics of patients undergoing stress tests prior to endovascular and open abdominal aortic aneurysm repair in Vascular Quality Initiative (VQI) participating centers between 2015 and 2019.
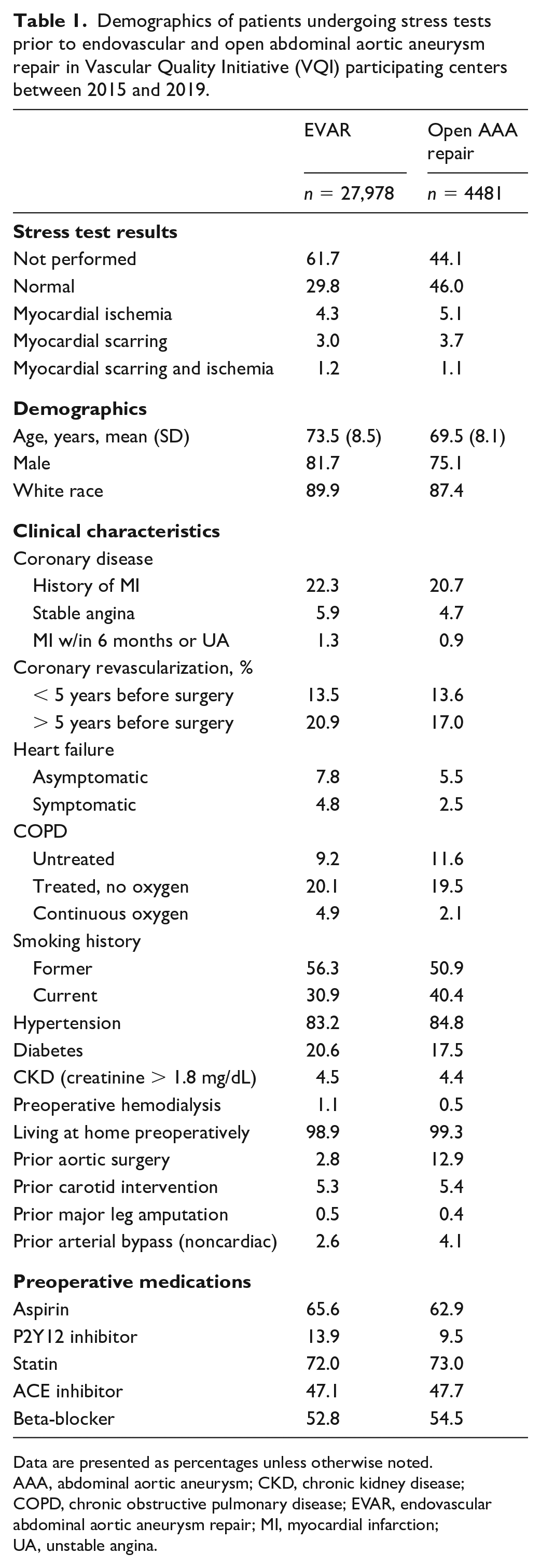
Data are presented as percentages unless otherwise noted.
AAA, abdominal aortic aneurysm; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; EVAR, endovascular abdominal aortic aneurysm repair; MI, myocardial infarction; UA, unstable angina.
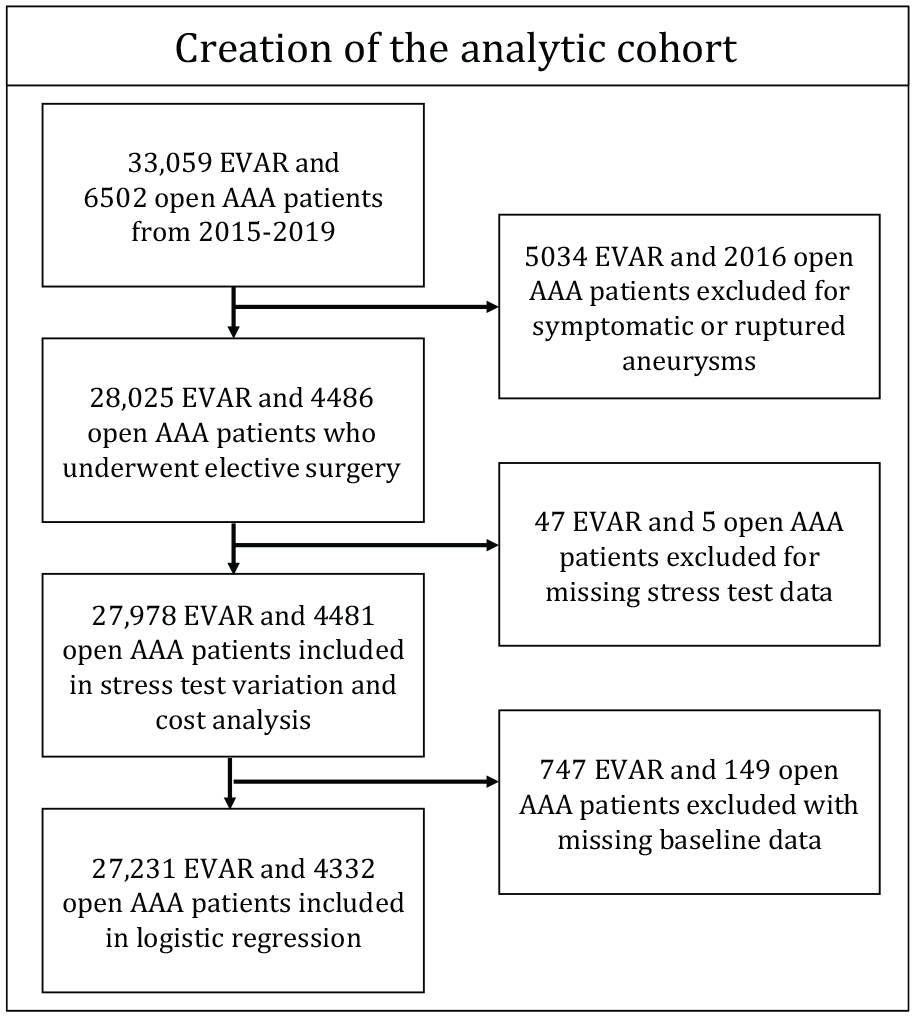
Flow diagram describing the creation of the cohort of patients for analysis.
Results
Patients
We studied 27,978 patients who underwent EVAR and 4481 patients who underwent open AAA repair across 283 VQI centers (Table 1). The mean age was 73.5 (± 8.5) years for EVAR, and 69.5 (± 8.1) years for open AAA repair. Most patients were male (EVAR: 81.7%, open AAA repair: 75.1%) and of White race (EVAR: 89.9%, open AAA repair: 87.4%). Overall, a preoperative stress test was obtained in 38.3% of patients who underwent EVAR, and in 55.9% of patients who underwent open AAA repair. The preoperative stress test demonstrated myocardial ischemia, scar, or scar and ischemia in 8.5% of patients who underwent EVAR, and in 9.9% of patients who underwent open AAA repair. Comorbidities were common in these cohorts: 29.5% of EVAR and 26.3% of open AAA repair patients had a history of coronary artery disease, and 87.2% of EVAR and 91.3% of open AAA repair patients had a history of current or prior tobacco use.
Variation in stress testing
Substantial variation was noted in the frequency of stress testing prior to AAA repair across VQI centers (Figure 2). The median rate of stress testing prior to EVAR was 36.8% across centers, and ranged from 13.0% at the lowest observed (1st) quintile centers, to 68.6% at the greatest observed (5th) quintile centers. Although stress testing was obtained with some regularity, there was still significant variation in observed testing prior to open AAA repair: the median preoperative use was 59.4% and ranged from 15.9% at 1st-quintile centers to 85.0% at 5th-quintile centers (Figure 3).
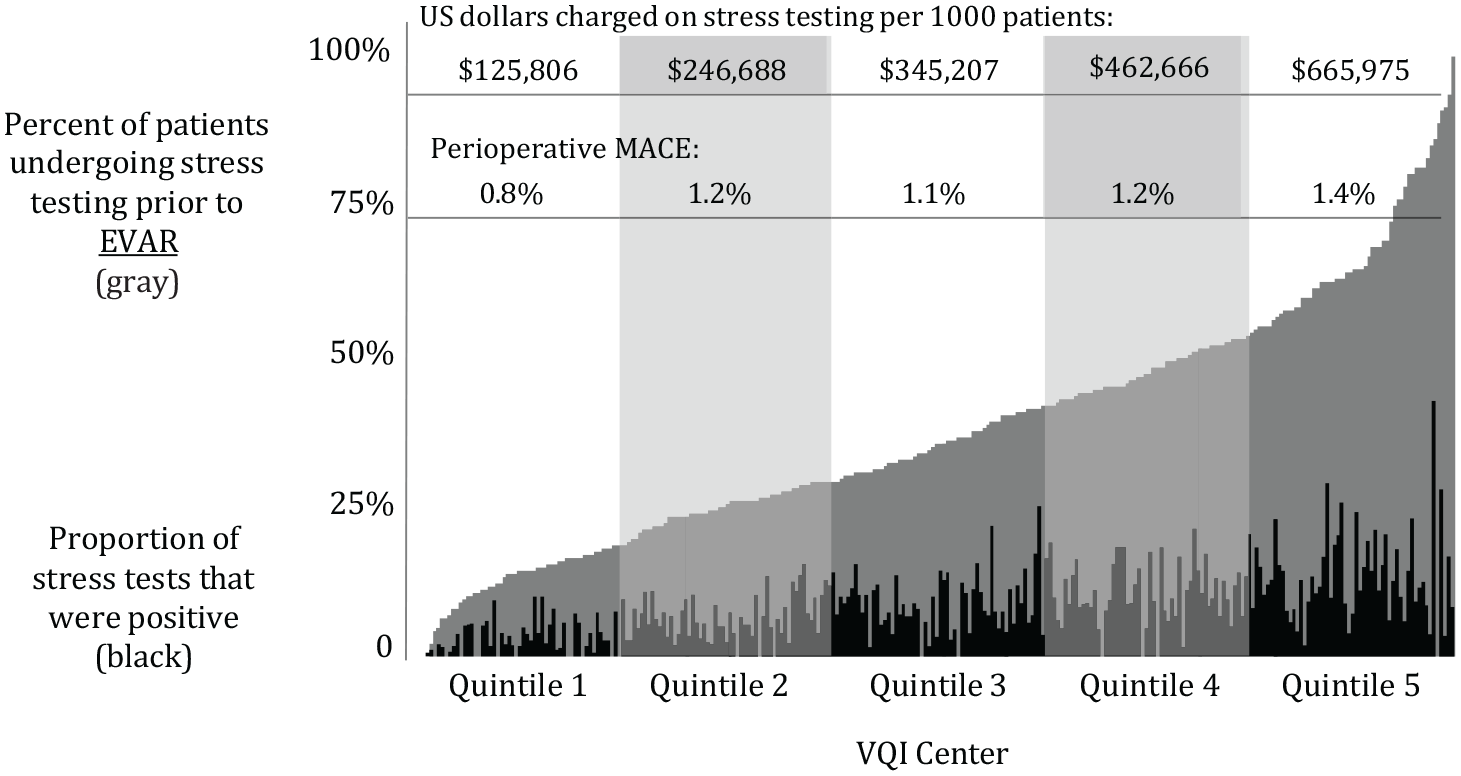
Percent of patients who underwent a stress test prior to EVAR, the proportion of tests that were positive, and estimated charges per 1000 patients, by quintile.
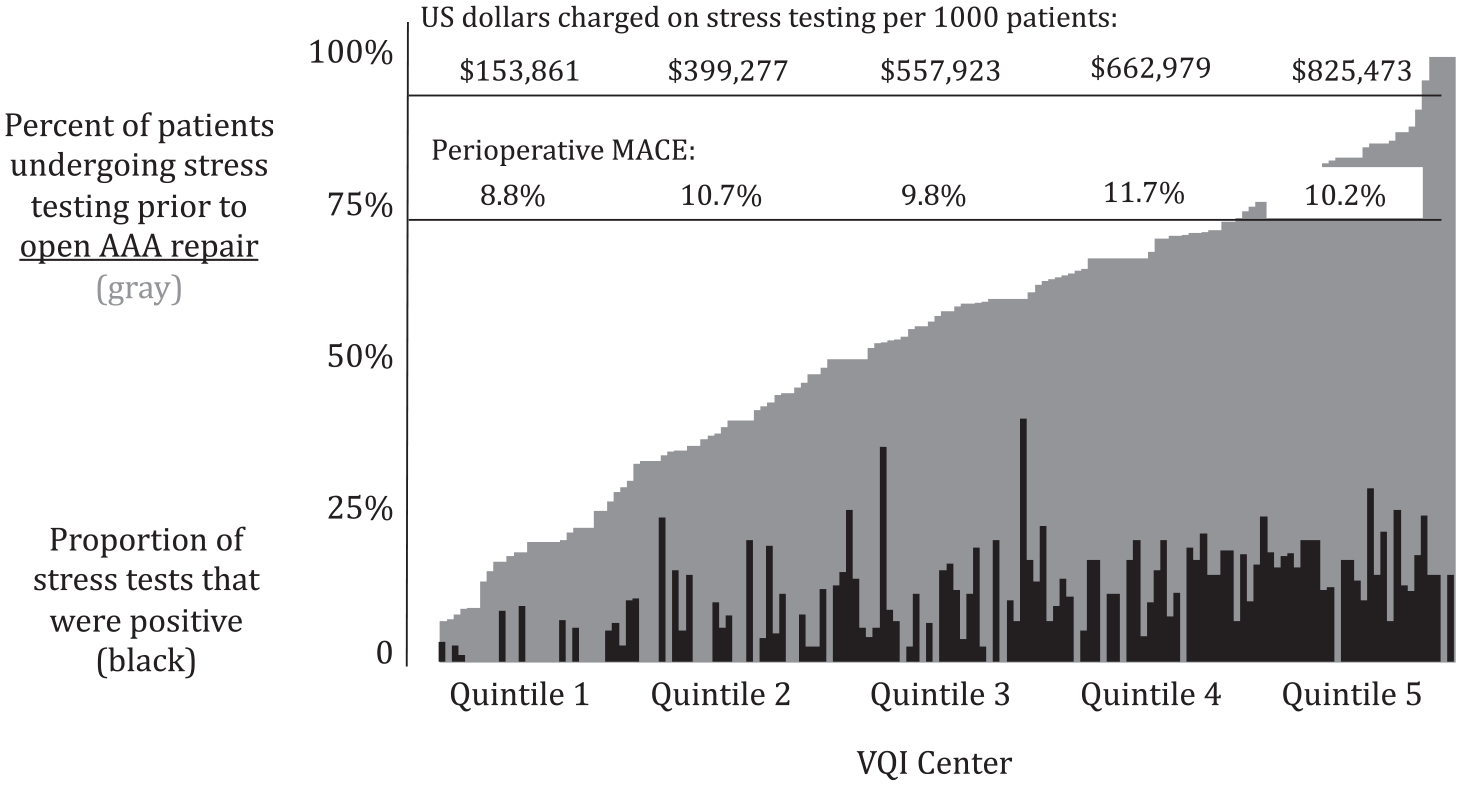
Percent of patients who underwent a stress test prior to open AAA repair, the proportion of tests that were positive, and estimated charges per 1000 patients, by quintile.
Adverse cardiac events
The unadjusted risk of MACE was 1.4% for EVAR and 10.2% for open AAA repair (Table 2). All adverse events including myocardial infarction, heart failure, and death were higher for open AAA repair than for EVAR. The risk of postoperative mortality was 0.5% for EVAR and 3.5% for open AAA repair. The risk of postoperative myocardial infarction was 0.6% for EVAR and 4.8% for open AAA repair.
Postoperative major adverse cardiovascular events after endovascular and open aortic aneurysm repair at Vascular Quality Initiative participating centers between 2015 and 2019.
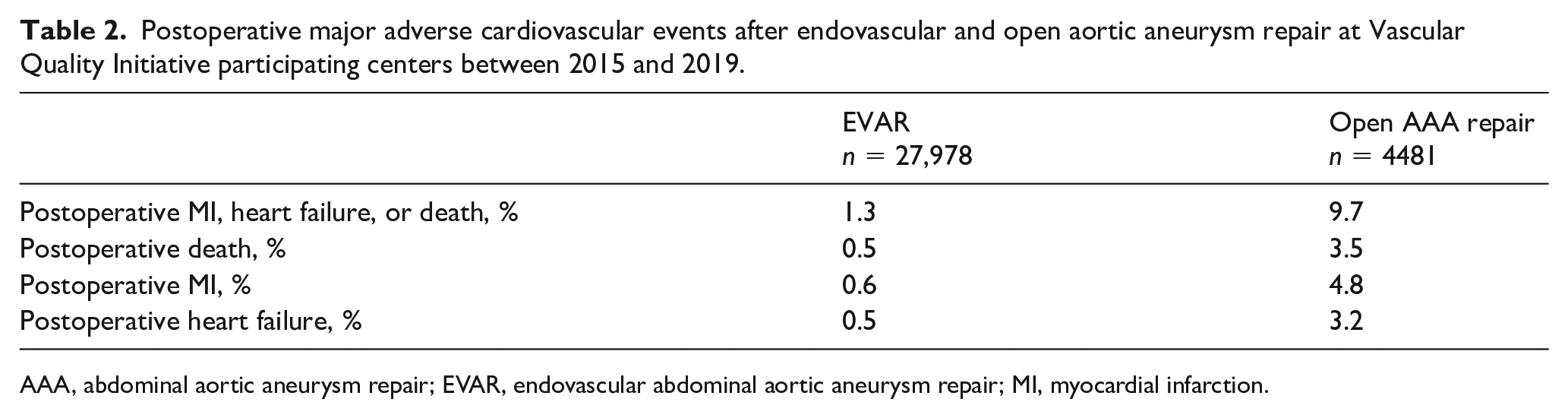
AAA, abdominal aortic aneurysm repair; EVAR, endovascular abdominal aortic aneurysm repair; MI, myocardial infarction.
Cost and MACE across the quintiles of stress testing
Next, centers were grouped into quintiles based on their documented rates of stress testing prior to AAA repair. The cost of stress testing increased substantially over the quintiles for both EVAR and open AAA repair. The estimated amount charged for stress testing prior to EVAR per 1000 patients at centers in the lowest quintile was $125,806. This increased in a stepwise fashion across the quintiles to $665,975 at centers in the highest quintile (Figure 2). The financial impact was even higher for open AAA repair. The estimated amount charged for stress testing prior to open AAA repair was $153,861 per 1000 patients for centers in the lowest quintile and increased to $825,473 accordingly among centers in the highest quintile (Figure 3).
The risk of MACE varied across the quintiles of preoperative stress test use for patients who underwent EVAR. Specifically, in the lowest quintile of stress testing the risk of MACE was 0.8%, and in the highest quintile of testing the risk of MACE was 1.4%, whereas the middle three quintiles had a risk of MACE that ranged from 1.1% to 1.2% (p-trend = 0.068; Figure 2). There was no statistically significant difference in MACE across the quintiles for open AAA repair. The percent of patients suffering an event after open AAA repair ranged from 8.8% to 11.7% across the quintiles (p-trend = 0.223; Figure 3).
Subanalysis of patients with a positive preoperative stress test
Patients who had a positive stress test had a higher likelihood of MACE than patients who had a negative stress test, or no stress test at all. Patients with a positive stress test who underwent EVAR had a 2.4% risk of MACE, versus 1.0% for those with a negative stress test, and 1.3% for those who did not undergo stress testing (p < 0.001). The adjusted odds ratio of MACE after EVAR among patients with a positive stress test versus all others was 1.54 (95% CI: 1.13–2.09). Similarly, patients who underwent open AAA repair despite a positive stress test had a risk of MACE of 15.9%, versus 9.4% for those with a negative stress test, and 8.6% for those who were not tested. The adjusted odds ratio of MACE after open AAA repair among patients with a positive stress test versus all others was 1.42 (95% CI: 1.05–1.92).
Discussion
In this study of nearly 27,000 patients who underwent EVAR and 4500 patients who underwent open AAA repair, we determined that the frequency of associated preoperative stress testing varied seven- and tenfold across centers, respectively. Increased stress testing was associated with substantially greater costs, with centers in the highest quintile of stress testing spending an estimated four- to fivefold greater amount than centers in the lowest quintile. The link between preoperative stress testing patterns and postoperative MACE was more difficult to define. Patients with a positive stress test undergoing EVAR or open AAA repair were more likely to experience postoperative MACE. However, centers that performed stress tests more frequently did not see a reduction in MACE. This important observation highlights that stress testing can be used to predict adverse events, but careful patient selection of whom should undergo a stress test is paramount to controlling cost. We would furthermore hypothesize that similar findings may be extrapolated across other large magnitude surgical procedures, thus amplifying the observed findings associated with preoperative stress testing noted herein.
Stress testing remains a commonly used risk stratification modality prior to major vascular surgery in current practice, but its benefit remains disputed among asymptomatic patients. Although small randomized trials have studied preoperative stress testing prior to noncardiac surgery, there remains no level 1 evidence to definitively support the utility of stress testing in the reduction of perioperative mortality.12,13 Despite this, some retrospective and small prospective studies have demonstrated lower rates of perioperative mortality among select patients undergoing stress testing with or without coronary revascularization prior to aortic surgery,14–16 suggesting that careful patient selection is critical in order to best identify patients who will derive benefit from preoperative cardiac testing.
A primary aim of this study was to elucidate the financial implications of widespread stress testing in patients undergoing AAA repair. Since test associated charges and overall institutional costs are not readily available across centers nationally, we ascertained local institutional costs, and extrapolated these test-associated charges across centers in the VQI. Our mean charges attributable to stress testing calculated in this study were comparable to previously reported cost estimates in the literature,17–19 and thus we felt that amortizing local costs across institutions was a reasonable proxy for test-associated charges elsewhere. Our results demonstrated that the cost of stress testing varied approximately fivefold between low-utilization and high-utilization centers and the cost impact was as high as $600,000 per 1000 patients in the EVAR group and $800,000 per 1000 patients in the open AAA repair group.
Interestingly, we did note a trend towards an increase in MACE in conjunction with increased preoperative stress testing among patients undergoing EVAR. There are several possible explanations for this. First, it may indicate that stress tests in this population are being used more frequently for high-risk patients, and that despite a negative or normal stress test, patients remain at high risk for MACE. However, we have previously demonstrated that the risk profile of patients who underwent a preoperative stress test is remarkably similar to patients who were not tested, which calls into question this potential explanation. 1 Second, it could represent patients who were initially considered for open AAA repair, that were ultimately deemed too high risk and then offered EVAR. However, we have again previously demonstrated that centers performing more stress tests do not simultaneously have more patients who are offered EVAR based on the results of the associated stress tests, which may make this explanation less likely. Third, the observed higher rate of MACE in high stress testing quintiles in this study could be attributable to an increase in vigilant postoperative testing for myocardial injury. It is reasonable to assume that centers that test more frequently preoperatively, may also be more likely to test more frequently postoperatively. Our prior results demonstrating that 1-year mortality is no different with increased stress testing despite increases in observed MACE may be explained by an increased frequency of postoperative testing at high-utilization centers. 11
Finally, it is possible that current stress testing practice patterns are ineffective and not guideline compliant. This observed trend towards an increase in MACE among EVAR patients may be in part due to false reassurance reported with negative stress testing in noncardiac surgery, where prior reports have documented an increased risk of adverse cardiovascular events despite negative stress testing.10,20 It has been documented that even with an estimated 80% sensitivity and specificity of stress testing, at least 20% of patients may have a false-negative result, which may lead to further invasive procedures and potential major complications with noncardiac surgery.19,21 In addition, the above sensitivity and specificity estimates only apply to the detection of obstructive coronary artery disease (i.e., lesions greater than approximately 70% stenosis). However, patients with nonobstructive coronary lesions remain at two to four times higher risk of myocardial infarction than healthy patients.22,23 These patients with nonobstructive coronary disease may not be appropriately captured by routine stress testing and may account for a significant portion of high-risk patients undergoing EVAR. These hypotheses may explain why approximately half of the composite MACE was attributable to postoperative MI in both the EVAR and open AAA groups despite widespread use of stress testing in this study.
Our findings highlight important areas for future work. Reasons for such widespread variation in preoperative stress test use remains unknown. Since the stress testing in the VQI registry is performed at the discretion of the clinician, we cannot know the reasons for such testing. Prospectively studying stress test practice patterns, guideline compliance, and the reason for these tests is an area of active work. In addition, it remains unknown how or if obtaining these stress tests led to a change in preoperative management, which could have led to changes in preoperative medications, an invasive cardiovascular evaluation, or a change to the operative plan (e.g., EVAR instead of open AAA repair). To study this, a prospective study is likely required. In addition, we found relatively low rates of medical therapy for patients undergoing aneurysm repair. Statin use was used in approximately 75% of patients, and beta-blockers in just over half. Given the known baseline cardiovascular risk in this patient population, targeted improvements in preoperative medical management seem justified. Finally, the American Heart Association and American College of Cardiology have published statements in whom to consider preoperative stress testing, but data upon which these guidelines are based are dated and relatively low quality, with no level 1 evidence to support stress test use. 6 Therefore, defining in whom and how preoperative stress testing should be used remains an important topic for investigation. However, regardless of these remaining gaps in knowledge, our findings of wide variation with substantial associated costs highlight the critical need for more research in this area.
Study limitations
This study has limitations. Specific charges data are not captured by the VQI registry. Since these data are also not publicly available, we estimated them using charges data from our institution. We designed this to provide a conservative measure of the costs associated with stress testing prior to AAA repair, realizing that this may underestimate the actual charges. Our institution is in the lowest quartile of cost for AAA care nationally, and therefore our costs are likely lower than many other institutions.24,25 In addition, 33% of stress tests performed at our institution in 2019 were electrocardiographic (exercise) stress testing. Most patients who undergo AAA repair undergo stress echocardiography or nuclear stress testing rather than an exercise stress test. Therefore, our estimates herein again likely provide a conservative measurement of the charges associated with stress testing. Our mean estimated cost per stress test per patient is on the same order of magnitude as costs reported in the published literature.17–19 Therefore, our conservative measures of the costs associated with widespread testing may underestimate the actual costs in contemporary practice, further highlighting the need for appropriate patient selection for stress testing prior to AAA surgery. Some patients may have undergone stress testing that was in the recent past but not considered part of the immediate preoperative workup, which would not be captured in this analysis. The external validity of this study to other populations is limited by the predominance of male and white patients in the VQI, which may fail to accurately depict more nuanced outcome disparities.
Conclusions
This study highlights that the contemporary utilization of preoperative stress testing prior to EVAR and open AAA repair vary substantially among centers in the United States. Moreover, more frequent stress testing was associated with a substantial increase in cost, though had an unclear association with MACE. The estimated charges associated with observed testing patterns were in excess of $600,000–800,000 per 1000 patients prior to AAA repair in high-utilization centers. These findings would indicate a substantial cost with an unclear clinical benefit. Accordingly, these findings highlight the need for improved and standardized stress testing paradigms prior to AAA surgery.