
Abstract
Inferior vena cava (IVC) anomalies are uncommon congenital causes of deep vein thrombosis (DVT). KILT syndrome (kidney and IVC abnormalities with leg thrombosis) has only been described as case reports in the literature. Therefore, the characteristics, evaluation, and management of patients with KILT syndrome have not yet been standardized. This study aimed to systematically review and analyze the clinical and radiographic data and treatment of previously reported cases of KILT syndrome. In this systematic review, we performed a literature search of the PubMed, Scopus, and Web of Science databases in December 2023, with no restrictions on the publication date. After duplicate extractions, 4195 articles were screened. Case reports and case series reporting on KILT syndrome were included. In addition to previously published cases, we included a new case of a previously healthy 25-year-old man with KILT syndrome in the analysis. A total of 34 cases were therefore included in this study. The majority (76.5%) were male patients with a median age of 24 years. In most patients, unprovoked bilateral iliofemoral thrombosis was diagnosed, and 64.7% had left kidney abnormalities. Our study suggests that anomalies of the IVC should be suspected in all young patients, especially male patients, with proximal, recurrent, or idiopathic DVT. If an IVC anomaly is confirmed, the kidneys should be examined to monitor and preserve healthy kidneys in cases of KILT syndrome. The data collected from all patients emphasize the requirement of long-term anticoagulation and risk factor control. Surgical measures may be effective for treating symptomatic refractory cases.
Keywords
Background
Venous thromboembolism (VTE) includes two medical conditions: deep vein thrombosis (DVT) and pulmonary embolism. 1 The estimated annual incidence of VTE among Europeans ranges from 104 to 183 per 100,000 person-years. 2 It is higher in African Americans and lower in Asians. 2 Moreover, the incidence increases markedly with age. 1
In the absence of obvious transient and persistent risk factors for VTE (unprovoked VTE), it is important to identify the underlying conditions, especially in younger patients.3,4 Inferior vena cava (IVC) anomalies are rare congenital causes of DVT, 4 with an estimated prevalence of up to 1% in a general population of patients with DVT and approximately 5% in those aged < 30 years.5,6 However, it can be assumed that their prevalence is even higher because IVC anomalies may not be seen on routine color duplex ultrasonography (CDS). 7 Hypoplasia and aplasia are the most common IVC anomalies in patients with DVT. 8 Inadequate venous return and the consequent high venous pressure and stasis in the lower limbs can cause thrombosis in such patients. 5 IVC anomalies are often isolated and may be asymptomatic or associated with other visceral abnormalities of the heart, spleen, and kidneys,9,10 including kidney and IVC abnormalities with leg thrombosis (KILT). 10
Owing to its rarity, KILT syndrome has only been described as case reports in the literature. Therefore, the evaluation and management of these patients have not yet been standardized. Therefore, this systematic review aimed to consolidate all available data regarding KILT syndrome in the literature and draw conclusions that would improve the diagnosis and further treatment of these patients.
Methods
This systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 11 The search strategy was developed by an experienced biostatistician (JML) and hematologist (MM). For this review, three databases (the PubMed, Scopus, and Web of Science) were screened in December 2023 using the following keywords: KILT syndrome OR ([inferior vena cava abnormalities OR inferior vena cava agenesis OR inferior vena cava atresia] OR [kidney abnormalities OR renal abnormalities OR kidney hypoplasia OR renal hypoplasia OR kidney agenesis OR renal agenesis OR hypoplastic kidney OR kidney dysgenesis OR renal dysgenesis] AND thrombosis). No restrictions regarding the publication date were applied. Articles written in English reporting cases or case series of KILT syndrome were included. The reference lists of the articles included in the analysis were manually searched for additional articles. Studies written in languages other than English, those with no available full text, and those involving nonhuman subjects were excluded. Two reviewers (NP and MC) independently evaluated the eligibility of all titles and abstracts, and performed full-text reviews. Disagreements were resolved by consensus (NP and MC) or arbitration (MM and MD). Two reviewers (NP and MC) independently extracted the following data: the first author’s name; year of publication; country; demographics (sex and age); and clinical (presenting symptoms, presence of thrombophilia and other predisposing factors, and comorbidities), radiographic, and therapeutic characteristics. In addition to previously published cases, we have included an unpublished case, which is presented in the following text. Informed consent was obtained from the patient for the publication of the case.
Case report
We report a previously healthy 25-year-old White man who visited the emergency department with unprovoked acute left leg pain, swelling, and tingling. Moreover, left lumbar pain persisted for a couple of days. His personal and family histories were unremarkable, and he was a nonsmoker. Physical examination results were normal except for a swollen left leg. The patient was slightly overweight (body mass index 26.6 kg/m2). CDS of the left leg revealed common (up to the IVC) and external iliac, common femoral, femoral, and popliteal vein thromboses. Laboratory studies showed a normal complete blood count (hemoglobin 14.1 g/dL, white blood cells 7.6 × 109/L, and platelets 207 × 109/L), elevated D-dimer levels (10.31 mg/L) with otherwise adequate basic hemostatic tests (international normalized ratio 0.96, activated partial thromboplastin clotting time 24.1 sec, and fibrinogen level 4.6 g/L), and normal kidney and liver function tests. Therapy with low-molecular-weight heparin (LMWH) was initiated. Acquired and inherited prothrombotic disorders were excluded based on the following tests: antithrombin, protein C, and protein S levels; activated protein C resistance; prothrombin 20210 mutation; antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, and anti-β2 glycoprotein 1 antibodies [IgM and IgG]); and homocysteine levels.
Abdominal ultrasonography was performed, and a small right kidney was identified (6.2 cm). Abdominal computed tomography (CT) was performed based on ultrasound findings. The right kidney was small (68 mm), and the left kidney was compensatorily enlarged (120 mm). Two right renal arteries were also observed. In addition, an infrarenal segment of the IVC was obliterated. A bilateral pelvic/femoral venous thrombosis with multiple lumbar collaterals draining into the azygous system was seen (Figure 1). Magnetic resonance imaging (MRI) venography confirmed infrarenal IVC agenesis along with lumbar collaterals (especially the ascending lumbar vein). A previously described thrombosis was also seen (Figure 2). A functional kidney scintigraphy showed that the function of the left kidney was compensatorily increased (86%), whereas the right kidney was hypofunctional (14%). Additionally, the global glomerular filtration rate was decreased for his age: 65.6 mL/min (normally above 88 mL/min).
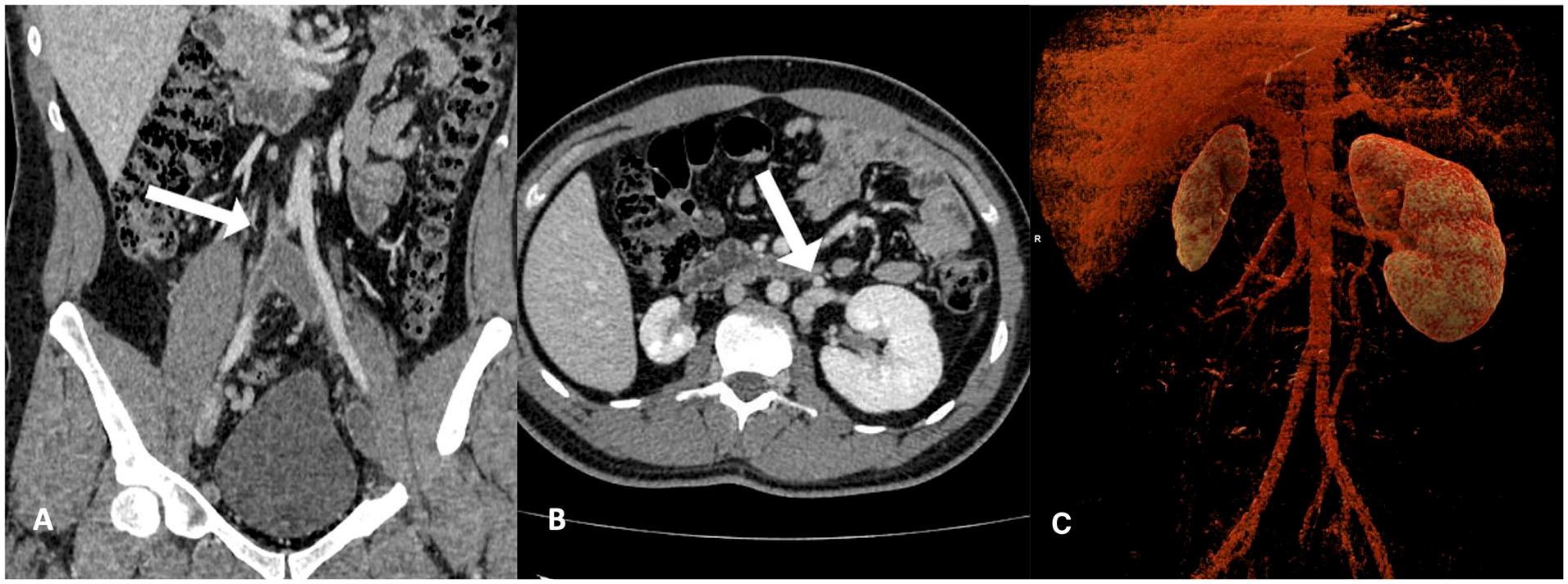
Imaging of patient with KILT syndrome.

Dynamic contrast-enhanced MRI studies (T1-weighted) in the coronal plane using the maximum intensity projection (MIP) method show absence of the IVC (top-left arrow) and extensive lumbar collaterals draining into the azygous system (thick arrows) in patient (same as Fig. 1) with KILT syndrome.
After 1 month of LMWH therapy, the patient was switched to rivaroxaban. CDS of the lower extremities after 3 months showed partial recanalization, whereas the recanalization was complete after 1 year. One year after the KILT diagnosis, the patient felt well and experienced no adverse events from anticoagulation therapy (online supplemental figure). However, the patient reported a palpable vein in the abdominal wall (Figure 3). A control MRI of the abdomen and pelvis was performed and the results were compared with those of the previous MRI: collaterals were developed in the front abdominal wall and pelvic region. Complete recanalization of the iliac veins was observed. However, the collateral vessels of the right obturatory vein were thrombosed.
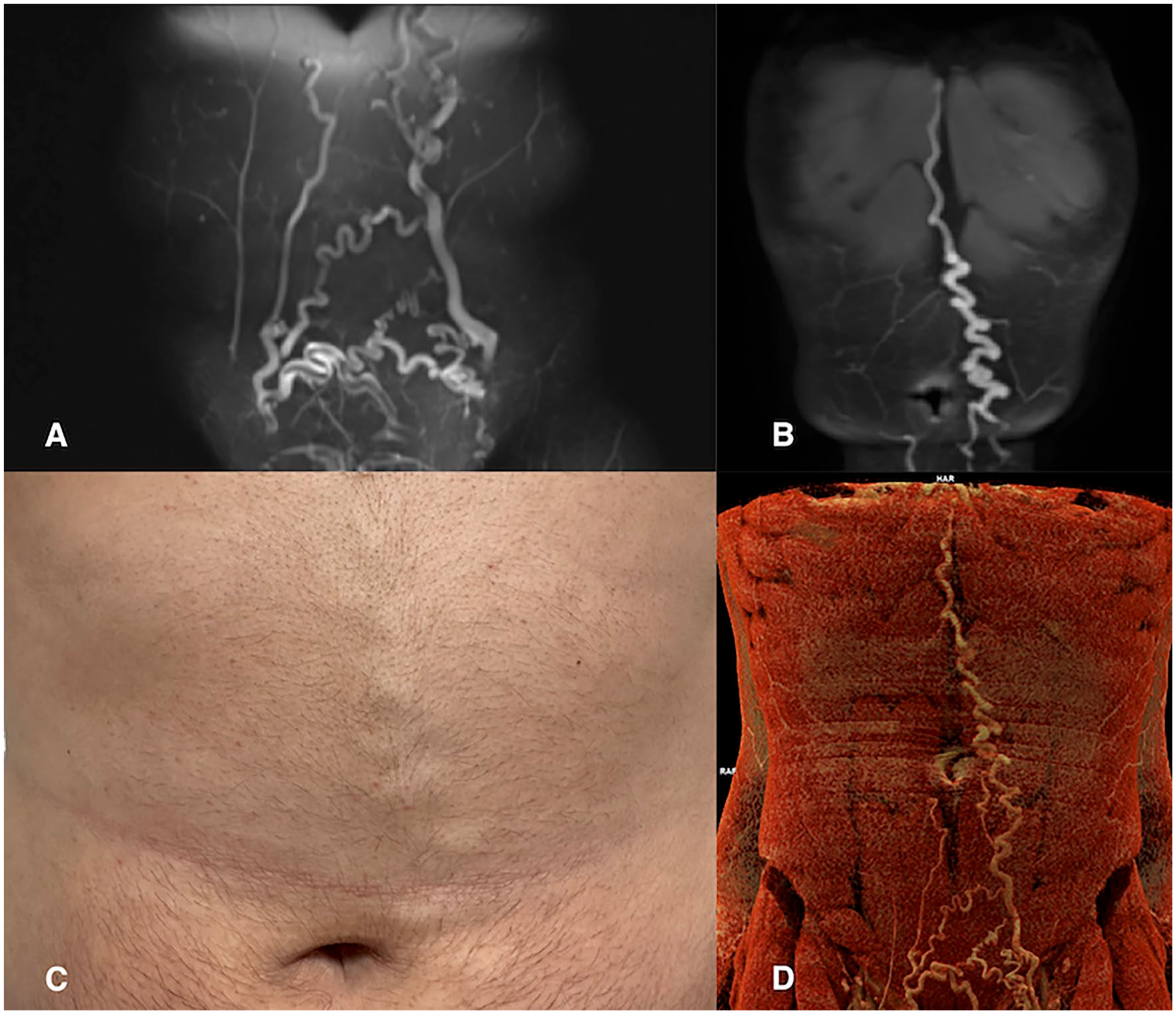
Abdominal wall venous collateral circulation in a patient with KILT syndrome (same patient as Figs. 1 and 2). (A and B) Dynamic contrast-enhanced MRI studies (T1w) in the coronal plane using the maximum-intensity projection (MIP) method; (C) Photography of the front abdominal wall; (D) CT venography with cinematic voume rendering technology.
Results
Using the search criteria, 4859 articles were identified (Figure 4). After removing duplicates, 4195 titles and abstracts were screened. In the next step, 4101 abstracts and titles were excluded because they were written in a language other than English and were not reported as human subjects or cases/case series of KILT syndrome. Nine full articles could not be accessed (conference papers with only abstracts available or locked unavailable papers). After reading 85 full articles, 52 case reports were excluded because they did not report patients with KILT syndrome and one paper was excluded because it was not a case report (correspondence without an abstract). Finally, 32 papers were included in the systematic review, with 33 patients (one article reported two patients with KILT syndrome, and the others were single case reports).
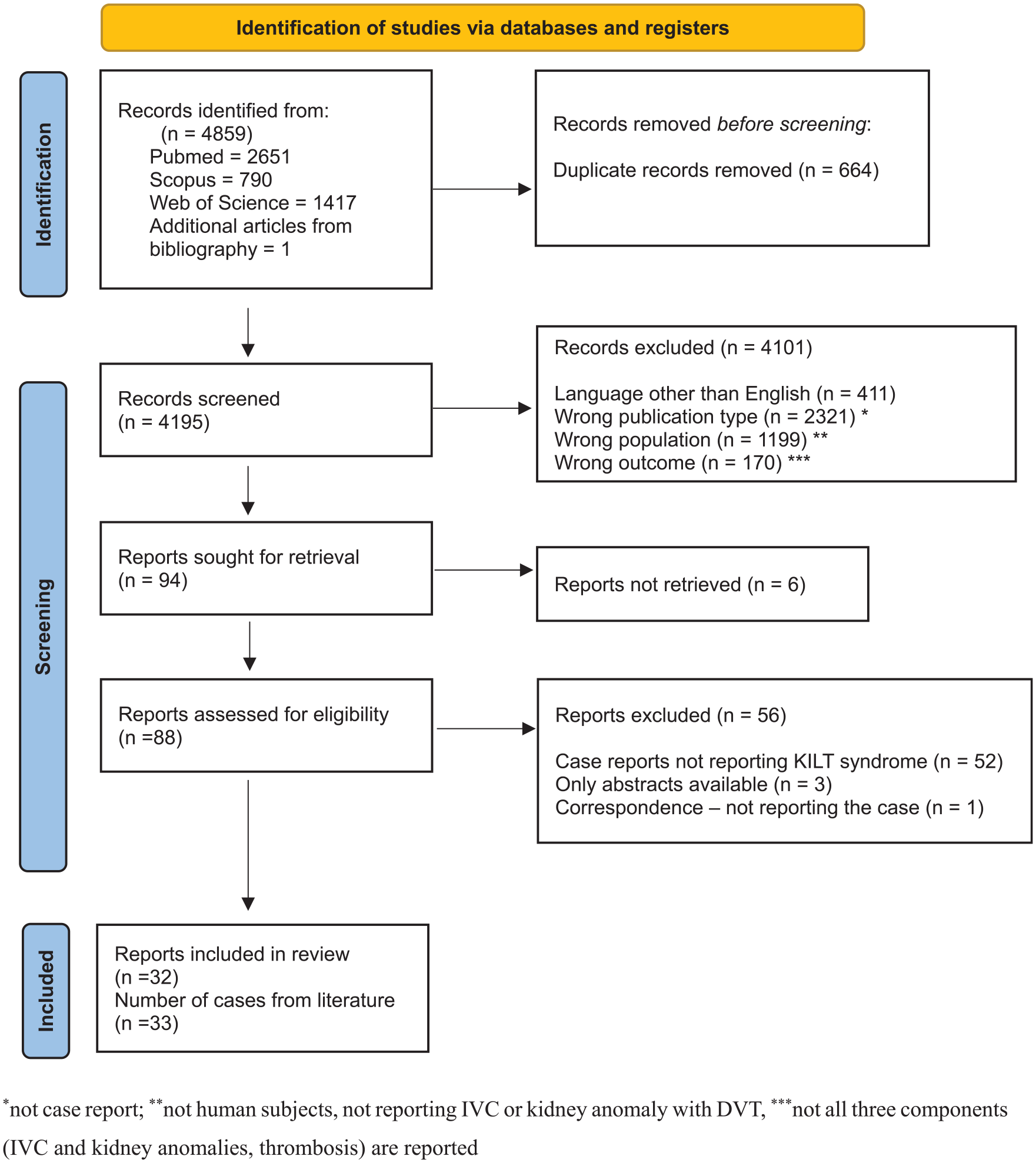
PRISMA flowchart of article selection.
The characteristics of the 32 publications (33 patients) included in the systematic review and our case are presented in the online supplemental table. All articles were published between 1998 and 2023. Sixteen articles were from Europe (four from the United Kingdom,5,10,12,13 three from Italy,14–16 three from Spain,17–19 and one each from Belgium, 20 the Netherlands, 21 Switzerland, 22 Romania, 23 Slovakia, 24 and Poland 25 ), nine from North America (eight from the USA26–33 and one from Canada 34 ), six from Asia (two from China35,36 and one each from Japan, 37 Iran, 38 Jordan, 39 and the United Arab Emirates 40 ), and one from Australia. 41
The majority (76.5%) were male patients. The median age was 24 years (range: 11 to late 60s). Pediatric cases (< 18 years) comprised 35.3%. Most of the patients presented with thrombosis-related symptoms (leg swelling and pain), but almost 20% of the patients presented with abdominal or lumbar pain which was caused by the collateral venous system (e.g., azygos and lumbar). In half of the patients, predisposing conditions (acquired or inherited thrombophilia, smoking, and oral contraceptive pill consumption) or provoking factors (physical strain, surgery, hospitalization, and systemic inflammation) were reported. Surgery was performed in four patients,15,20,23,38 signs of systemic inflammation with elevated C-reactive protein levels were noted in four,20,25,32,37 one patient used contraceptive pills and experienced excessive physical strain before thrombosis, 20 and one was obese and his father experienced an unprovoked pulmonary embolism. 33 Three patients were smokers,22,30,39 four had elevated homocysteine levels,14,16,19,24 two were heterozygous factor (F) V Leiden carriers,28,39 two had mildly elevated FVIII,16,34 and one had decreased antithrombin levels. 24 The majority of patients (64.7%) had left kidney abnormalities, four had arterial hypertension,19,24,27,36 and one had chronic kidney disease. 12 Bilateral thromboses were registered in 55.9%, whereas in 26.5% it was localized on the right side. In almost all cases, the findings involved iliofemoral thrombosis. The majority of patients (76.5%) were treated with unfractionated heparin or LMWH, followed by vitamin K antagonists (VKA). Five patients, including the one reported here, received direct oral anticoagulants (DOAC; rivaroxaban,29,35 apixaban, 13 and dabigatran 14 ). Additionally, in one patient, rivaroxaban and apixaban were tried after VKA failure (persistent symptoms, recurrence, and stent thrombosis), but without any success; therefore, the patient was treated with clopidogrel and enoxaparin. 22 Owing to persistence of symptoms during medical treatment (8.8%), invasive procedures (thrombectomy, balloon angioplasty, or stent placement) were performed in three patients.16,22,28 Direct thrombolysis, mechanical thrombectomy, and balloon angioplasty were performed as the first-line therapy in three patients, followed by long-term anticoagulation.29,33,40 Thrombosis was recurrent in nine patients (26.5% cases). In three patients, anticoagulation had already been stopped at the time of recurrence (after recurrence, long-term therapy was indicated in two patients,13,30 and anticoagulation was not possible because of intracranial bleeding in others 26 ); for three patients, there were no data on anticoagulation treatment at the time of thrombosis.17,19,20 Three patients – one on VKA, 22 one on LMWH with antithrombin concentrate, 24 and one on rivaroxaban – were still receiving treatment when recurrence was diagnosed. Medical therapy was stopped without any signs of recurrence only in one patient; however, the follow-up period was only 6 months after drug cessation. 41 Summarized patient characteristics are shown in Table 1.
Summarized patient characteristics (N = 34).
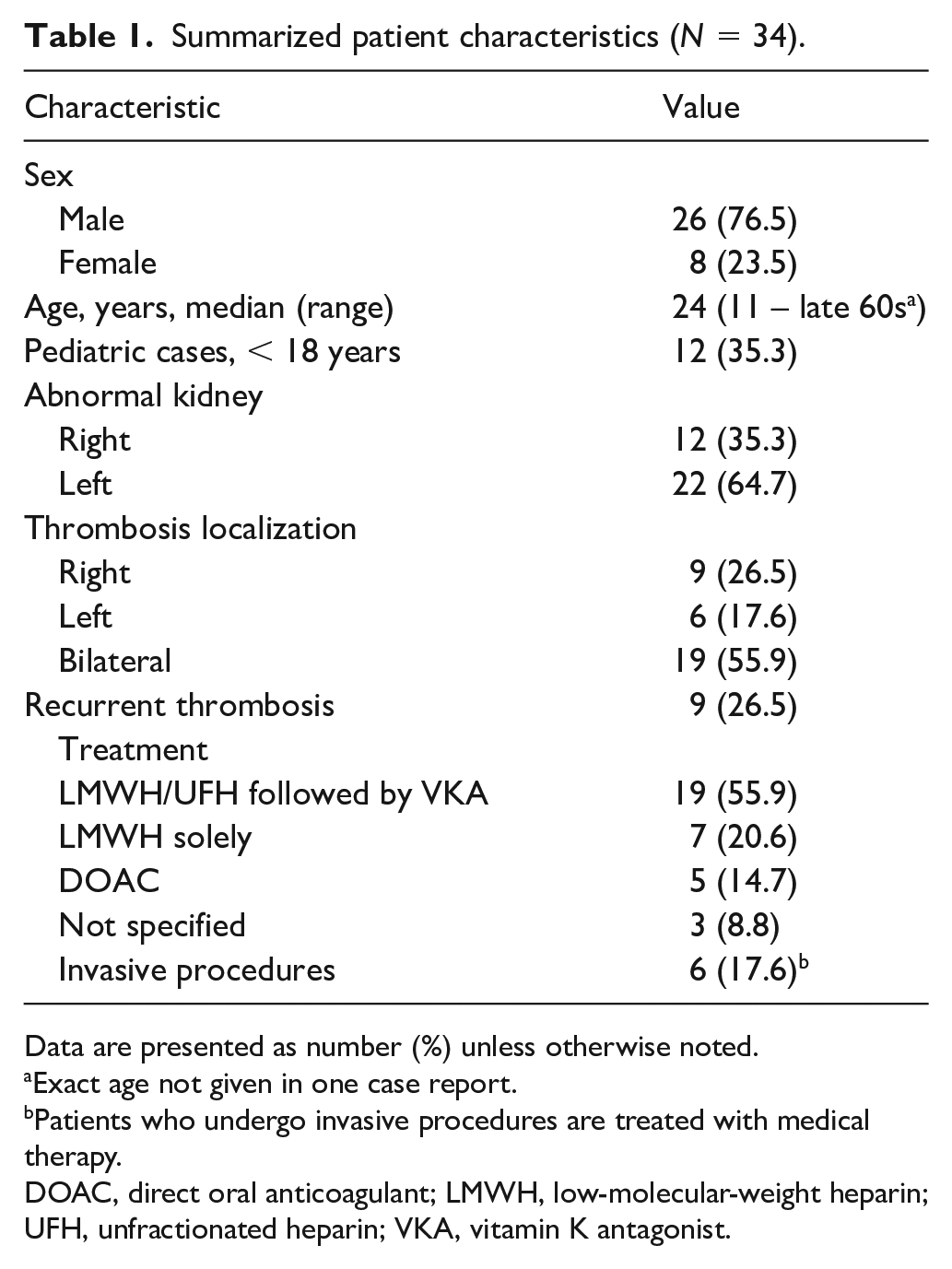
Data are presented as number (%) unless otherwise noted.
Exact age not given in one case report.
Patients who undergo invasive procedures are treated with medical therapy.
DOAC, direct oral anticoagulant; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin; VKA, vitamin K antagonist.
Discussion
In 2002, KILT syndrome was first defined by Van Veen et al. 10 Twenty years later, we attempted to gather information on this syndrome. We collected data of 34 cases of KILT syndrome, including the one reported here. To the best of our knowledge, this is the highest number of reported cases of KILT syndrome to date.
The IVC is a major venous blood system, 42 which is mainly formed between the sixth and eighth weeks of gestation by growth, regression, and interconnection between the posterior cardinal, subcardinal, and supracardinal veins (Figure 5).43,44 The suprarenal IVC is formed by the right subcardinal vein, the renal segment is formed by the right and left subcardinal veins, and the infrarenal segment from the right supracardinal vein.9,43 Anomalous IVC anatomy may result from abnormal persistence or regression of these fetal venous structures. 44 The etiology of the absence of the IVC remains controversial. From one point of view, this could be the consequence of perinatal thrombosis and subsequent fibrosis, 45 and from the other, it could be the consequence of some disturbed embryological processes (e.g., maldevelopment of the right supracardinal vein). 46 Acquired IVC obstruction often implies the lack of one IVC segment and could be associated with certain provoking factors, such as cardiac catheterization during infancy, and the congenital absence of the IVC could be associated with other congenital malformations (e.g., asplenia). However, both are associated with a higher risk of thrombosis in later life.9,47 It can be assumed that both mechanisms are involved in the KILT syndrome. Simultaneous kidney anomalies can be explained by perinatal renal vein thrombosis or insufficient blood supply owing to vascular abnormalities. 48 However, Duicu et al. reported KILT syndrome in siblings, suggesting a genetic background. 23
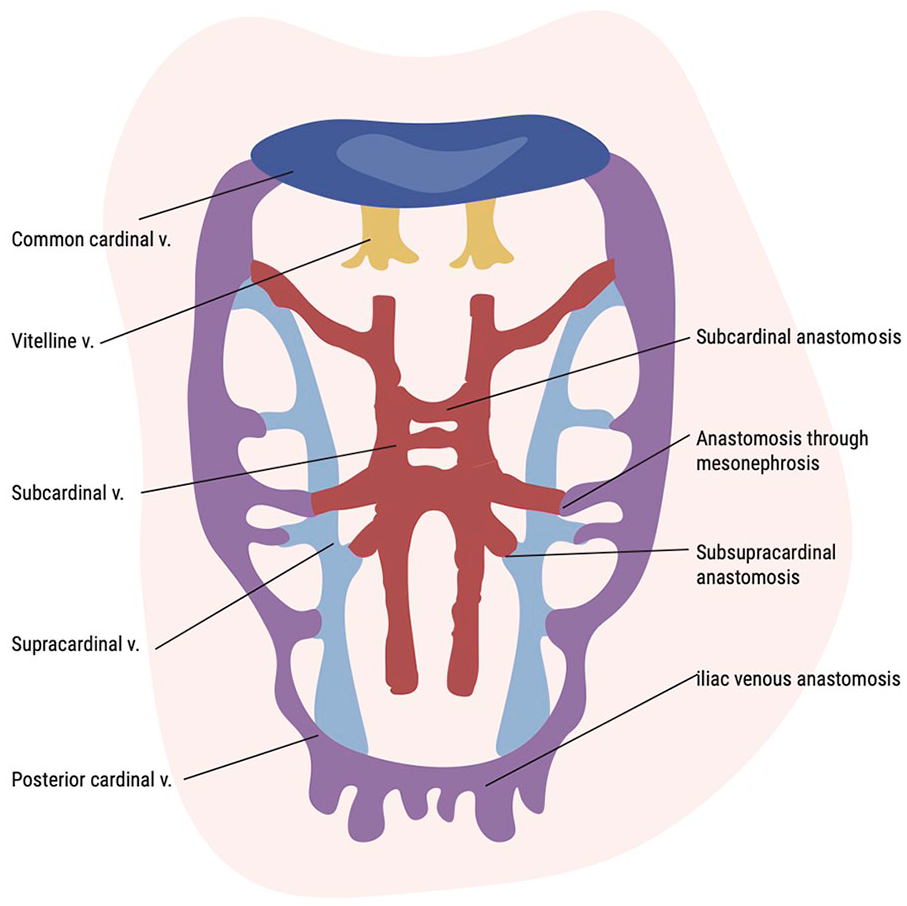
Embryonic structures involved in IVC formation.
Based on our review, the typical patient was a young man in his 20s without any strong predisposing conditions or risk factors. Kidney function screening is usually normal, although some patients have slightly elevated creatinine levels.12,22,25 However, renal function tests (technetium-99m with dimercaptosuccinic acid scan) showed that the affected kidney had severely decreased function (< 15%),23,27,34,35 suggesting that the use of potentially nephrotoxic substances should be restricted in order to preserve the function of the unaffected kidney. In patients with KILT, the initial symptoms are usually related to DVT, and patients are asymptomatic in the early period of life. Bilateral extensive iliofemoral thromboses were diagnosed in most of the patients in this study. Moreover, the collateral venous systems were well developed in all patients, causing lumbar pain, appearance of abdominal masses, or visible veins of the abdominal wall. In one patient, venous ulcerations were diagnosed at a very young age. 12 In young patients with venous ulceration and chronic venous insufficiency, IVC agenesis and KILT syndrome should be considered since it has been shown that up to 31% of patients with IVC agenesia could have venous ulceration. 49 In patients with KILT, ultrasound was not sufficiently accurate to make a diagnosis. Patients required CT or MRI when the distal IVC could not be visualized via CDS or an IVC anomaly was suspected because of their young age, and a diagnosis was made.
In most reported cases of IVC agenesis associated with DVT, including patients with KILT syndrome, long-term conservative treatment with heparin followed by VKA was the treatment of choice. In most cases, this approach leads to symptom relief and blood vessel recanalization.7,46 Although less frequently reported, cases that were successfully treated with long-term DOAC have also been reported.14,29,35,50 However, no studies have compared the two approaches. Progression or rethrombosis in patients on therapy with both VKA and DOAC has also been reported.15,22 For such patients, invasive procedures such as thrombolysis or thrombectomy, as well as switching to another drug class, could be viable options. Although IVC reconstruction is possible, it is only performed in cases where other treatment modalities failed.16,50 Thrombolysis or thrombectomy can be performed to prevent chronic symptoms, such as residual pain, tenderness, and swelling. It has been shown that patients with IVC anomalies and thrombosis treated with thrombolysis are less likely to develop postthrombotic syndrome or thrombosis recurrence. 51 This fact should be considered, especially because the association between hypoplasia and aplasia of the IVC and DVT is most frequent among young patients with DVT. 8 Such patients have compromised venous outflow and are likely to develop postthrombotic signs and symptoms at a younger age.
Most reported patients with KILT were tested for inherited and acquired thrombophilia despite having defined thrombophilic conditions. One patient who was an FV Leiden carrier and one with decreased antithrombin levels had progressive thrombosis despite adequate anticoagulation, suggesting that such patients require more frequent monitoring.24,28 Additionally, factors such as smoking and oral contraception should be avoided in all patients.
Conclusion
Underlying conditions should be actively investigated in young patients with thrombosis. IVC anomalies should be included in the diagnostic algorithm for such patients, especially young male patients with bilateral lower-limb DVT. If IVC anomalies are proven, kidney anomalies and KILT syndrome should be considered. Based on available data, extended anticoagulation is a common practice for treating KILT syndrome; however, clinical evidence and/or data are limited. As this is a rare condition, the development of a multicenter registry could include more patients, which would allow for the development of more concrete recommendations.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241240427 – Supplemental material for Deep venous thrombosis in patients with atresia of the inferior vena cava and right kidney hypoplasia (KILT syndrome): Systematic review of the literature
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241240427 for Deep venous thrombosis in patients with atresia of the inferior vena cava and right kidney hypoplasia (KILT syndrome): Systematic review of the literature by Nikola Pantic, Mirjana Cvetkovic, Jelena Milin-Lazovic, Jelica Vukmirovic, Aleksandar Pavlovic, Marijana Virijevic, Zlatko Pravdic, Sofija Kozarac, Nikica Sabljic, Nada Suvajdzic-Vukovic, Marko Dragas and Mirjana Mitrovic in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.