
Abstract
Keywords
Background
Revascularization techniques continuously evolved during the last two decades, currently being recognized as the first-line therapy of peripheral artery disease (PAD) among vascular and endovascular operators from different disciplines worldwide. 1 However, endovascular revascularization of complex and calcified lesions remains challenging since balloon angioplasty can cause flow-limiting dissections or recoil, requiring bail-out stenting.
Especially in arterial segments, which are within mobile zones or are used as access sites, like the common femoral artery (CFA) and the popliteal artery, stenting needs to be avoided since biomechanical forces may lead to stent fracture, thrombosis, and loss of patency, possibly deteriorating PAD symptoms in the long term.2,3 In addition, stent placement in the CFA and in the popliteal artery may exclude the option for future interventions or bypass surgery. 3
We and others showed that minimal invasive atherectomy can be safely used for the treatment of calcified and complex lesions within a variety of anatomical locations extending from the groin to below-the-knee (BTK) vessels in symptomatic PAD.4,5 In addition, the ability of atherectomy to reduce dissection and barotrauma, and therefore the need for stent placement, has been confirmed in randomized controlled trials. 6
In the present study, we sought to investigate the safety and effectiveness of the Phoenix atherectomy device for the treatment of lesions in the CFA and in the popliteal segments. Procedural success and the need for bail-out stenting were systematically analyzed, whereas safety endpoints included vessel perforation and peripheral embolization. Mid-term results are presented in terms of freedom from clinically driven target lesion revascularization (CD-TLR) and clinical success during follow-up. In addition, a comparator group with drug-coated balloon (DCB) but without atherectomy treatment is provided for the popliteal artery.
Methods
Study design and ethics disclosures
Our study was conducted in a single vascular center with wide experience on endovascular procedures and minimal invasive atherectomy, and was designed as a prospective, observational registry. Ethics approval was obtained from the local ethics committee of the University of Heidelberg. In addition, the study was registered on the German Clinical Trials Register website (DRKS00016708).
Patient population and characteristics
Between July 2017 and June 2022, consecutive patients with peripheral lesions of the CFA and popliteal artery due to symptomatic PAD, requiring atherectomy-assisted endovascular revascularization, based on our internal standard operating procedures, were enrolled. 7 Typically, patients with chronic limb threatening ischemia (CLTI) were scheduled for endovascular treatment in due course, whereas a time interval of about 3 months with best medical treatment and exercise preceded the endovascular treatment in patients with lifestyle-limiting claudication.
Patients with CFA stenotic lesions (> 70% by angiographic criteria) or total occlusions were included in our trial. The presence of ipsilateral inflow lesions of the iliac arteries and of outflow lesions or occlusions of the superficial femoral artery (SFA), including Transatlantic Intersociety Consensus Classification (TASC) C and D lesions, was allowed by study protocol.
Patients with popliteal artery stenosis (> 70% by angiographic criteria) or total occlusions were included in our trial. With this subgroup, lesions extending up to 3 cm of the distal SFA and up to 1 cm of the crural arteries were allowed. However, patients with multiple lesions within the ipsilateral target limb (e.g., concomitant ipsilateral lesions in the CFA, femoral artery occlusions extending to the popliteal artery, etc.) were excluded with this patient subgroup.
With both subgroups, the inclusion of patients with contralateral CFA or popliteal artery lesions fulfilling the above-mentioned criteria was allowed. Patients with concomitant lesions of the CFA and of the popliteal artery were included in the CFA subgroup, which allowed concomitant ipsilateral femoropopliteal lesions and occlusions. In addition, only de novo lesions were considered and in-stent restenotic or occlusive lesions after stent placement were excluded.
In addition, 531 patients treated for popliteal artery stenosis or occlusion using standard balloon angioplasty, DCB, stent placement, or a combination of the prior but without atherectomy were used as a comparator group. This group of patients was previously published by the EMO-POP investigators as reported elsewhere. 8 Briefly, EMO-POP was a multicenter retrospective cohort study, performed in 15 hospitals within five countries, analyzing consecutive patients between June 2016 and June 2021, who underwent endovascular revascularization for popliteal artery stenosis or occlusions.
All patients included in our single-center study, and especially those with CFA lesions, were referred for endovascular treatment either upon clinical assessment or upon recommendation of the primary treating vascular specialists. In all cases, the possible alternative treatment option of open repair was considered and discussed, especially in patients with CFA lesions or occlusions. All patients were informed about possible advantages of the endovascular treatment, including minimally invasive treatment without general anesthesia. In addition, especially in patients who refused surgery, possible disadvantages of endovascular revascularization were mentioned with respect to the limited availability of long-term data on vessel patency are re-intervention rates compared to the standard reference technique of surgical endarterectomy. In addition, possible wound healing problems and groin infections were discussed, especially in obese patients. Patient preferences were considered in all cases and written consent to undergo endovascular treatment was signed prior to treatment, as reported previously. 5
Clinical symptoms of PAD were classified according to Rutherford categories (RC) and cardiovascular risk factors, such as hypertension, hyperlipidemia, smoking, and diabetes mellitus, and history of coronary artery disease (CAD) were recorded at time of the presentation. Laboratory data, including serum creatinine, urea, the estimated glomerular filtration rate (GFR), hemoglobin, and the highly sensitive troponin T (hs-TnT) were also evaluated at baseline.
Endovascular procedure protocol
All procedures were performed by two experienced interventional cardiologists and angiologists (JCK and GK) specifically trained for these techniques and board-certified by the German Societies of Cardiology and Angiology. In brief, all patients received a bolus of 5000 IU of heparin after placement of a 6F or a 7F sheath introducer in the contralateral femoral artery for the treatment of CFA lesions and using either a cross-over or an antegrade approach for the treatment of the popliteal artery. During interventional treatment, heparin was additionally administrated, aiming for an activated clotting time between 250 and 300 seconds, which was measured every 30 minutes after the beginning of the procedure.
The Phoenix atherectomy device (Philips, San Diego, CA) and its work principle has already been described previously.4,5,9 For the treatment of both CFA and popliteal artery lesions, we used the 1.8 mm or the 2.2 mm tracking and the 2.2 mm or the 2.4 mm deflecting devices. With the latter two device sizes, the tip of the catheter can be deflected. These deflecting properties provide a change in the direction of the catheter, thus combining rotational and directional cutting in a form of ‘hybrid’ atherectomy, which allows for more efficient debulking, especially in eccentric lesions and vessels with larger diameters. No predilation of the lesions was performed prior to the atherectomy procedure. In addition, embolic filter protection devices were not used with atherectomy procedures. After atherectomy, lesions were treated using DCB and/or scoring balloon angioplasty, based on the extent of calcification and the overall complexity of the lesions. Bail-out stenting was performed in case of extensive of flow-limiting dissections, based on our previously established internal standards. 10 Briefly, stent implantation was considered in cases of Type C or higher dissection patterns, based on the previously described dissection classification 11 and in cases of residual stenosis > 30% (recoil) after atherectomy and balloon angioplasty. If required, self-expandable or interwoven stents were deployed.
Upon intervention, patients without indication for oral anticoagulation received a standard dual antiplatelet therapy with aspirin (100 mg/day) and clopidogrel (75 mg/day) for a period of 4 weeks up to 3 months, followed by lifelong daily aspirin. In patients with indications for oral anticoagulation like atrial fibrillation, 250–500 mg aspirin were administrated intravenously during the procedure and patients were treated with clopidogrel (75 mg/day) and oral anticoagulants for 3 months, followed by oral anticoagulants thereafter.
On the day after the procedure, all patients received an ankle–brachial index (ABI) test and a routine duplex ultrasound to exclude proximal or distal site complications such as arteriovenous fistula and pseudoaneurysms at the puncture sites and to assess acute procedural success.
Analysis of angiographic data for the CFA and the popliteal artery
All angiograms were evaluated for assessment of lesion characteristics by either JCK or GK offline after the procedure, as follows:
Length of the lesion or occlusion for CFA and popliteal artery lesions.
Presence or absence of chronic total occlusive (CTO) lesions.
Lesion classification by Peripheral Arterial Calcium Scoring System (PACSS) criteria. 12
Presence of multilevel PAD based on the concomitant involvement of iliac and femoropopliteal arteries, requiring attention and treatment in the index limb.
CFA lesion complexity, as described previously, by anatomic localization: Type I, isolated CFA lesions; Type II, lesions in the external iliac artery (EIA) and the CFA but without involving the femoral bifurcation; Type III, CFA lesions involving the femoral bifurcation; and Type IV, lesions extending from the EIA down to the femoral bifurcation. Bifurcation lesions extending from the CFA only in the SFA, only in the deep femoral artery (DFA), and in both the SFA and the DFA were classified as Type IIIS, IIID, and IIIB, respectively, and as Type IVS, IVD, and IVB in cases of involvement of the EIA. 5
Popliteal artery lesion complexity, as described previously, by involvement of only one P1, P2, or P3, of two or of all the three subsegments of the popliteal artery. 13
Follow-up and study endpoints
Follow-up was performed at regular intervals in our outpatient centers or by the referring physicians, wherever possible. Since surveillance was affected by the COVID pandemic after March 2020 in Germany, missing clinical data were obtained via a telephone call from the patients or the referring physicians. During telephone contact, a standardized questionnaire was used to assess the patient’s clinical status, re-interventions, major adverse cardiac or limb events, and limiting symptoms, including walking distance and wound healing disorders. All these data constituted the base for the calculation of the RC during follow-up.
Safety endpoints were perforation, embolization, or access site complications requiring further interventions or open repair during the atherectomy procedure. For the assessment of peripheral embolization, full leg angiograms, including the crural and pedal arteries, were performed in all patients prior to and at the end of the endovascular procedures.
Procedural endpoints were technical success, defined as residual stenosis < 50% after atherectomy prior to any type of adjunctive treatment, 4 procedural success, defined as residual stenosis < 30% after atherectomy and adjunctive treatment, including balloon angioplasty and if required stent placement, 4 and the need for bail-out stent placement in the CFA and the popliteal artery, respectively.
Primary outcomes were clinical success, defined as the achievement of ⩾ 2 grade RC improvement during follow-up and CD-TLR during follow-up.
Statistical analysis
Analysis was performed using the commercially available software MedCalc 20.009 (MedCalc software, Mariakerke, Belgium). Continuous variables were expressed as mean ± SD if normally distributed or as median and IQR if they were not normally distributed. The Shapiro–Wilk normality test was performed to assess normality versus skewed distribution with continuous variables. Categorical variables were expressed as proportions and were compared using χ2 tests. The ANOVA test was used for comparing three or more normally distributed groups with the Scheffé test for post hoc analysis, whereas for continuous variables, which were not normally distributed, nonparametric tests (Mann–Whitney U-tests or Kruskal–Wallis tests) were performed. Pre- and postprocedural ABI values were compared to each other using paired t-tests. Kaplan–Mayer analyses were used to evaluate CD-TLR over time for patients with CFA versus popliteal artery lesions. Differences were considered statistically significant at p < 0.05. A case–control matching procedure was used between patients who underwent atherectomy from the single-center study and patients who underwent endovascular revascularization of popliteal arteries without the use of atherectomy from the EMO-POP registry, after adjustment for RC at baseline (difference of 1 RC allowed), lesion calcification by PACSS (exact match required), presence of CTO (exact match required), lesion length (maximal difference of 2.0 cm allowed), and use of DCB (use of DCB required in all cases). All tests were two-sided.
Results
Patient demographics and baseline clinical data
Between July 2017 and June 2022, 552 of 1785 patients who were referred to our department for endovascular revascularization due to symptomatic PAD underwent Phoenix-assisted atherectomy. Of 552 patients, 122 exhibited lesions in the CFA (72 patients; 73 lesions) or in the popliteal artery (50 patients; 53 lesions). Mean age was 75.0 (IQR = 67.0–82.0) years and 60 (49.2%) of the patients were women. A total of 58 (47.5%) patients had intermittent claudication (RC3), 11 (9.0%) had ischemic rest pain (RC4), and 53 (43.4%) exhibited ischemic ulcerations (RC5 [n = 51] and RC6 [n = 2]) (Table 1).
Baseline, clinical, and laboratory data.
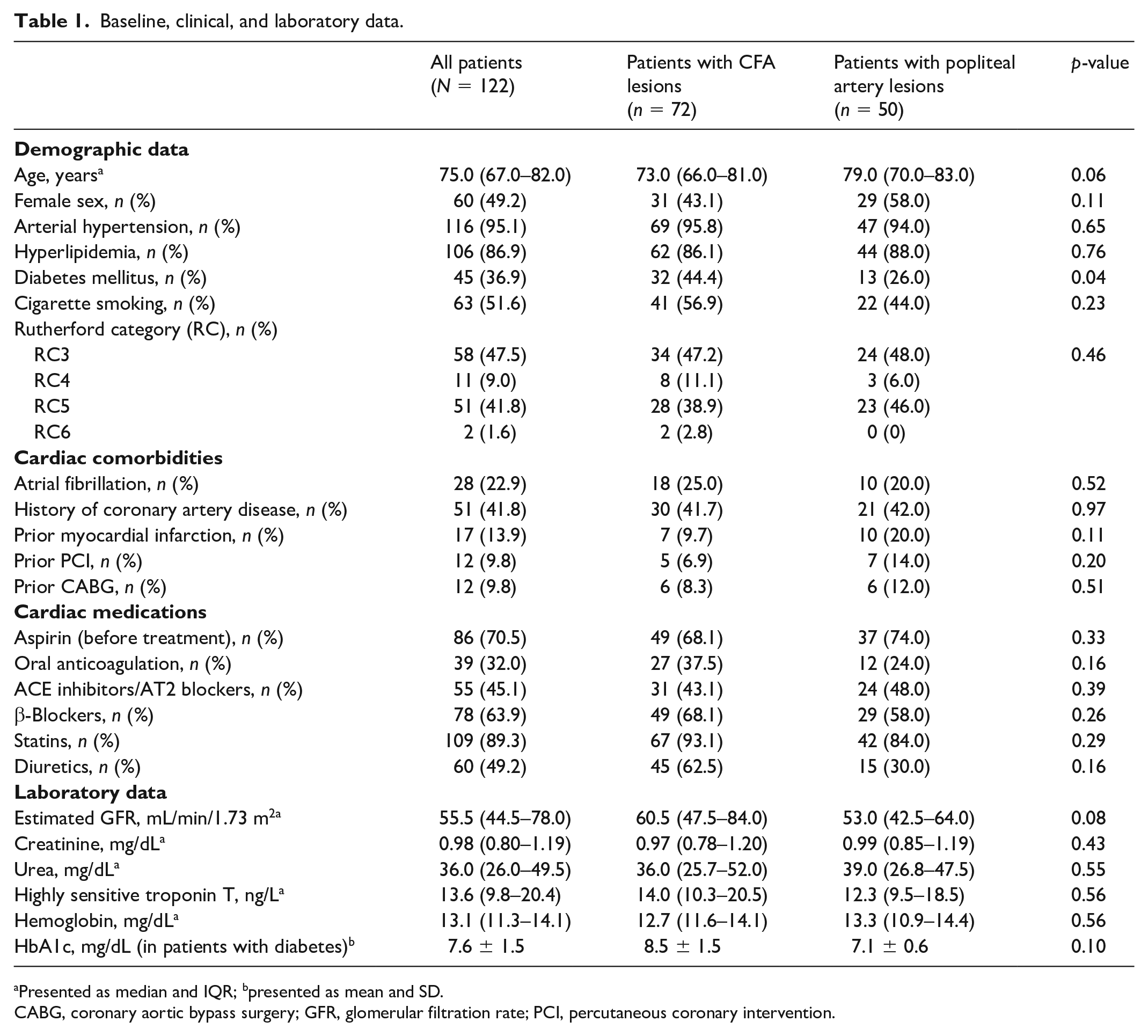
Presented as median and IQR; bpresented as mean and SD.
CABG, coronary aortic bypass surgery; GFR, glomerular filtration rate; PCI, percutaneous coronary intervention.
Lesion characteristics
Overall, 73 de novo CFA and 53 popliteal lesions were treated. CFA lesions with involvement of the femoral bifurcation were present in 41 (56.2%) cases. Inflow iliac lesions were present in 13 (17.8%) cases. With popliteal lesions, on the other hand, involvement of more than one segment was present in 28 (52.8%) cases. Median lesion length was 2.9 cm (IQR = 2.2–3.7, range 1.4–5.5 cm) with CFA and 5.5 cm (IQR = 3.5–8.5, range 1.5–13.5 cm) with popliteal artery lesions. CTO lesions were more common with popliteal versus CFA lesions (52.8% vs 12.3%, p < 0.001) (Table 2). Total lesion calcification by PACSS was high in both groups: 3.0 (IQR = 3.0–3.0). Additional complex TASC C/D femoropopliteal occlusions were present in 19 (26.0%) CFA lesions.
Lesion characteristics including lesion length, presence of chronic total occlusion, anatomical localization, and calcification.
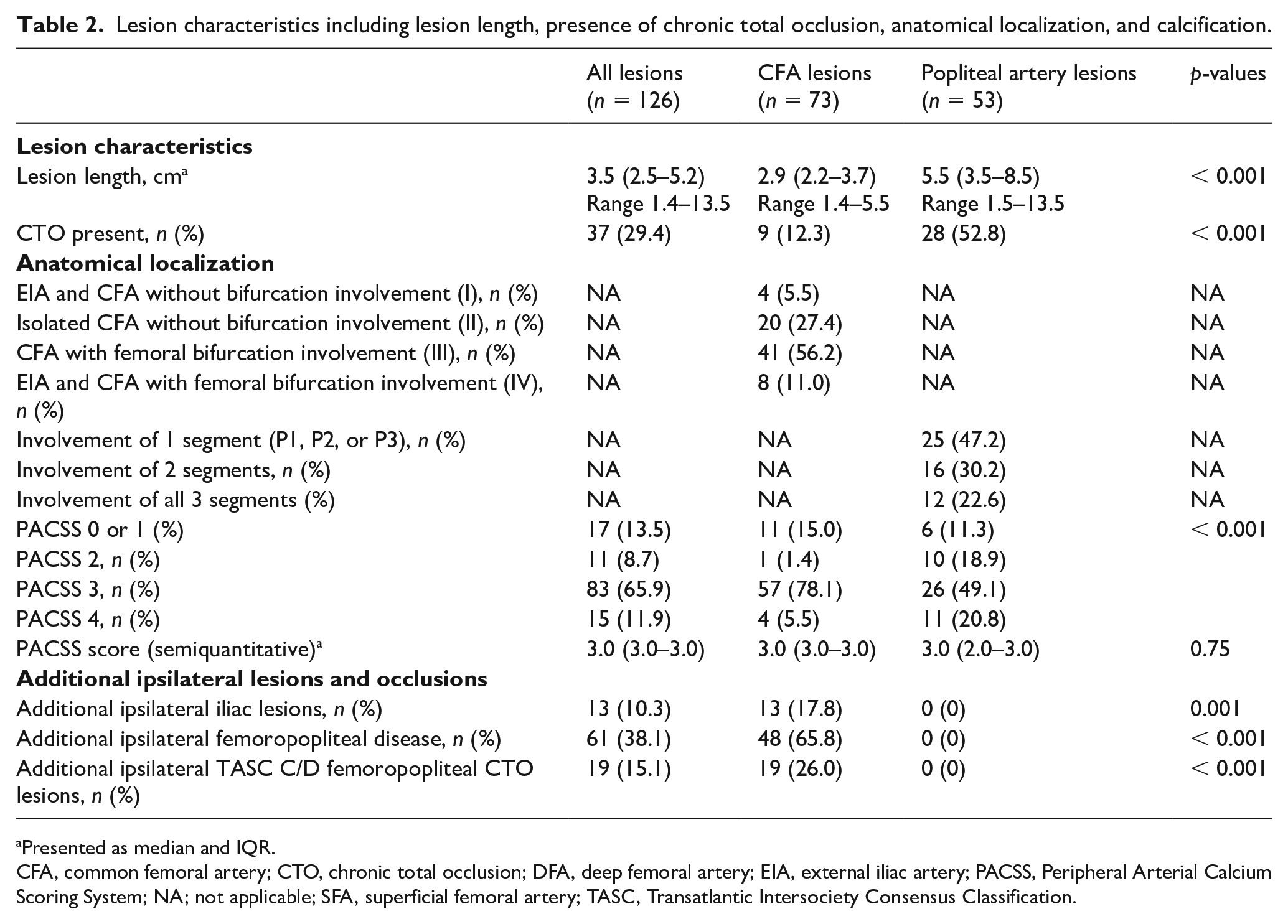
Presented as median and IQR.
CFA, common femoral artery; CTO, chronic total occlusion; DFA, deep femoral artery; EIA, external iliac artery; PACSS, Peripheral Arterial Calcium Scoring System; NA; not applicable; SFA, superficial femoral artery; TASC, Transatlantic Intersociety Consensus Classification.
Endovascular procedures and acute outcomes
Atherectomy was performed using a 2.4-mm or 2.2-mm deflecting device in 45 (61.6%) CFA lesions and 18 (34.0%) popliteal artery lesions, respectively; whereas the 2.2 mm and 1.8 mm tracking catheters were used in 28 (38.4%) and 35 (66.0%) of the remaining cases, respectively (Table 3). Importantly, bail-out stenting rates were low both for CFA (n = 2; 2.7%) and for popliteal artery lesions (n = 3; 5.7%). Stenting was performed in all cases using interwoven stents. Adjunctive treatment was performed using scoring balloon angioplasty in 54 (42.9%) cases, whereas DCB was used in 123 (97.6%) cases. Overall technical and procedural success rates were 51.6% and 99.2%, respectively. In addition, no perforations, two pseudoaneurysms requiring manual compression, and one peripheral embolization, treated by catheter aspiration within the index interventional procedure, were observed. Procedural duration and contrast agent doses were higher with CFA compared to popliteal lesions. Baseline and postprocedural ABI values are provided in Figure 1.
Debulking strategy and procedural data, including complications.
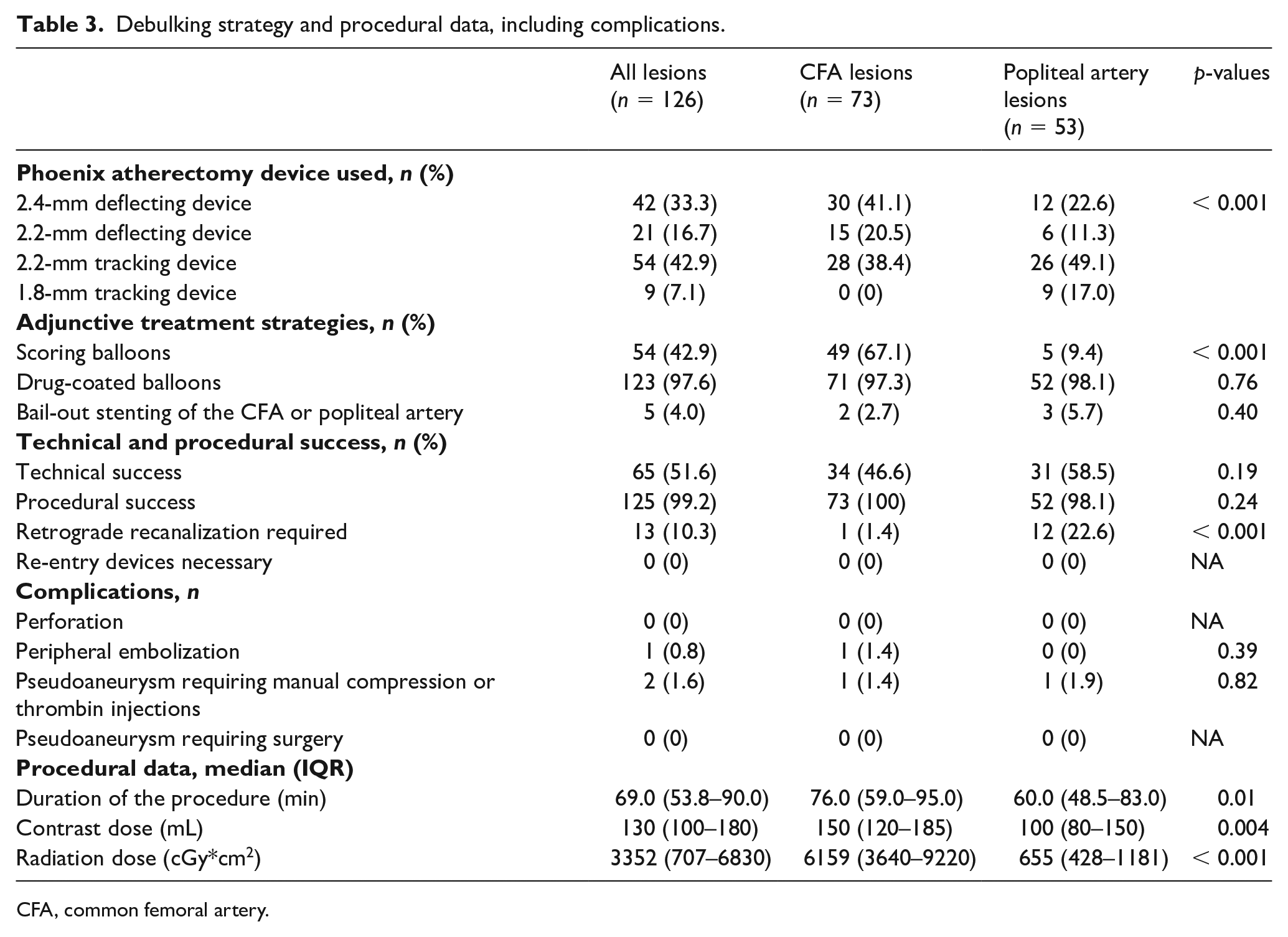
CFA, common femoral artery.
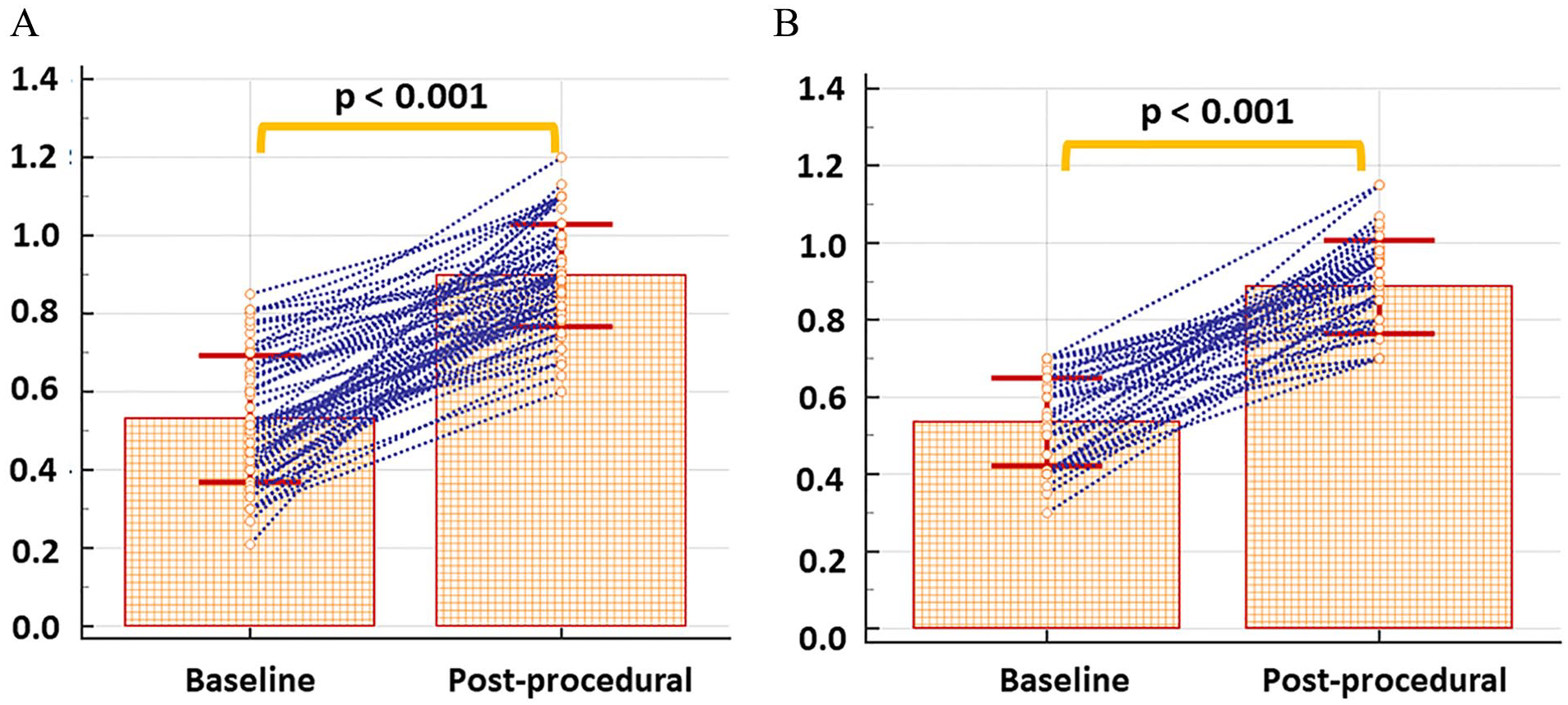
Pre- and postprocedural ABI values with
Clinically driven target lesion revascularization (CD-TLR) and clinical success
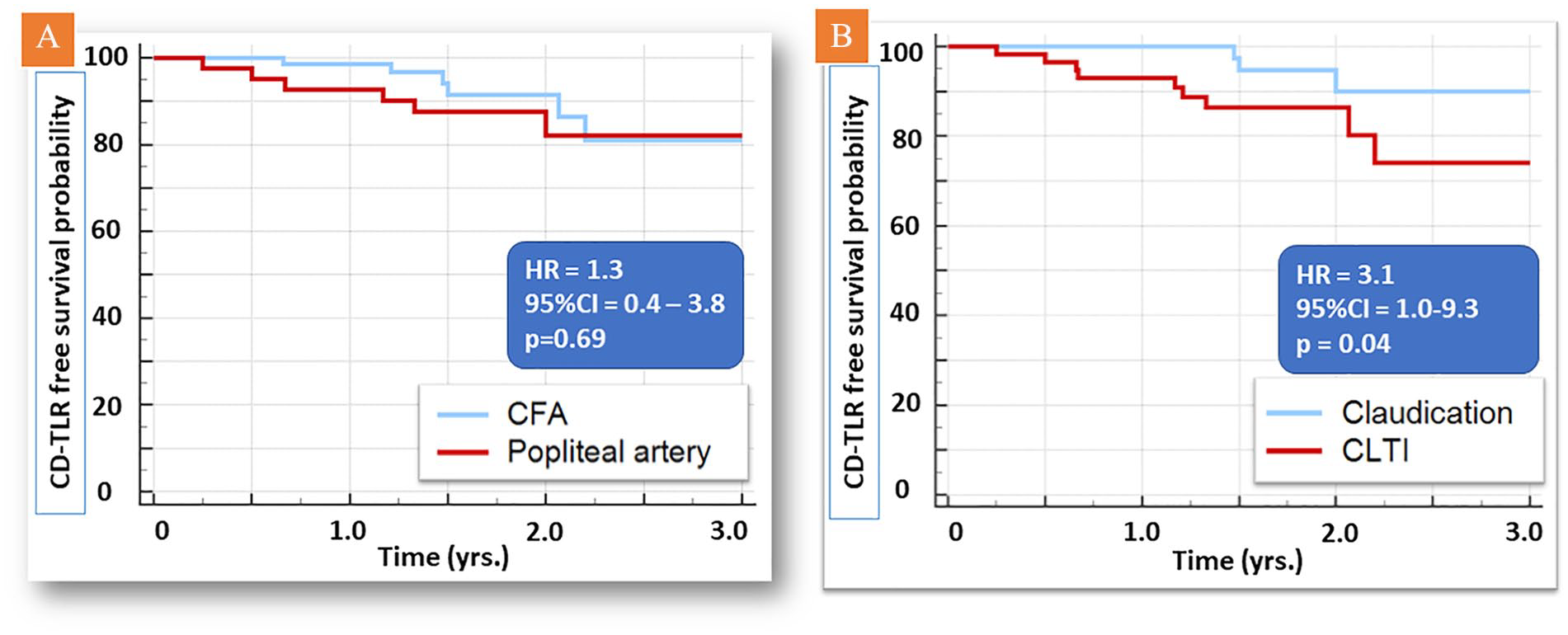
Clinical follow-up was available in 113 out of 122 (92.6%) patients during 1.50 years (IQR = 1.17–2.2 years). During the follow-up period, 22 (19.5%) patients died. None of the deaths was device or procedure related. CD-TLR was performed during follow-up in 13 (11.5%) patients, including seven (9.2%) and six (14.6%) cases, respectively, in patients who had been treated in the CFA and popliteal artery during the index procedure (Figure 2A). Higher CD-TLR rates were noted in patients with CLTI versus claudication (hazard ratio [HR] = 3.1; 95% CI = 1.0–9.3, p = 0.04; Figure 2B). All re-interventions were performed endovascularly, including 10 atherectomy-assisted re-interventions, two re-angioplasty and DCB, and in one re-angioplasty and stenting. During follow-up, the mean RC decreased from 4.0 (IQR = 3.0–5.0) to 2.0 (IQR = 1.0–3.0) (p < 0.001) (Table 4). Clinical success was noted in 93 (85.3%) patients, including 62 (91.2%) with CFA and 31 (75.6%) with popliteal artery lesions (Table 4; Figure 3). Eleven planned minor amputations (9.7%) and no major amputations occurred.
Follow-up data and clinical success.
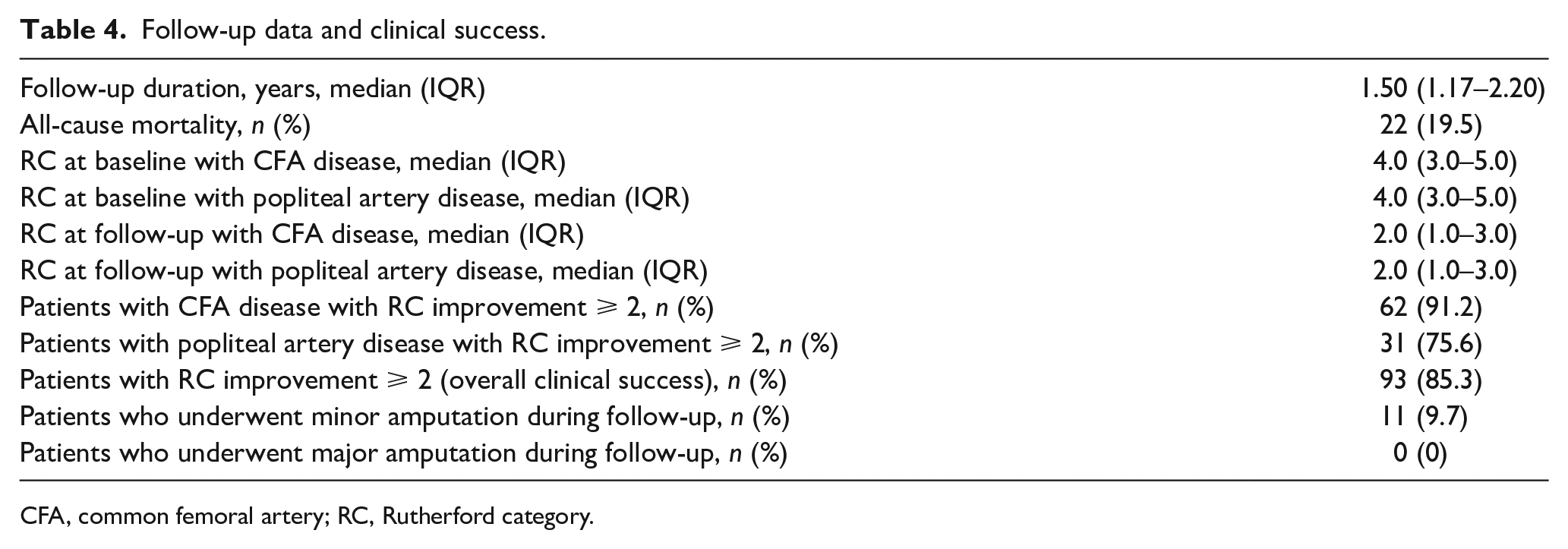
CFA, common femoral artery; RC, Rutherford category.
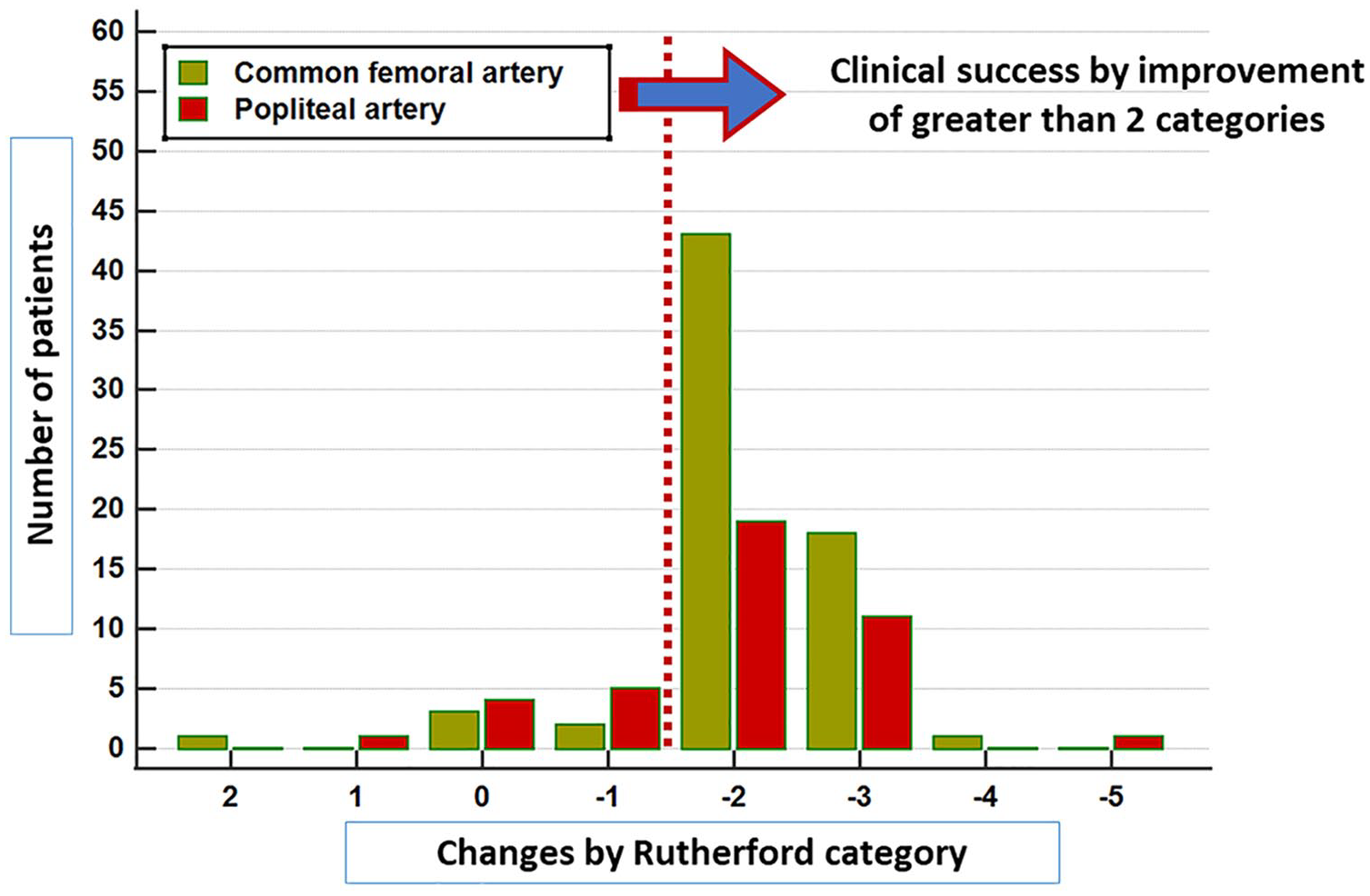
Changes in Rutherford categories in patients undergoing atherectomy and drug-coated balloon treatment. Clinical success was noted in 93 (85.3%) patients.
Comparison to the EMO-POP registry for popliteal artery lesions
Baseline and lesion characteristics of our single-center study and nondebulking cases from the EMO-POP registry are shown in the online supplementary Table 1A. After case–control matching of 50 patients of our single-center study and 531 patients from the EMO-POP registry, 40 patients from the single-center cohort who underwent atherectomy and DCB were compared to a matched comparator group of 40 patients from the EMO-POP registry who underwent DCB angioplasty without atherectomy. Baseline and lesion characteristics of the matched cohorts are provided in online supplementary Table 1B. Patients treated with the combination of atherectomy and DCB exhibited significantly higher freedom from CD-TLR during follow-up compared to a DCB only strategy (HR = 3.1; 95% CI = 1.1–8.5, p = 0.03) (Figure 4).
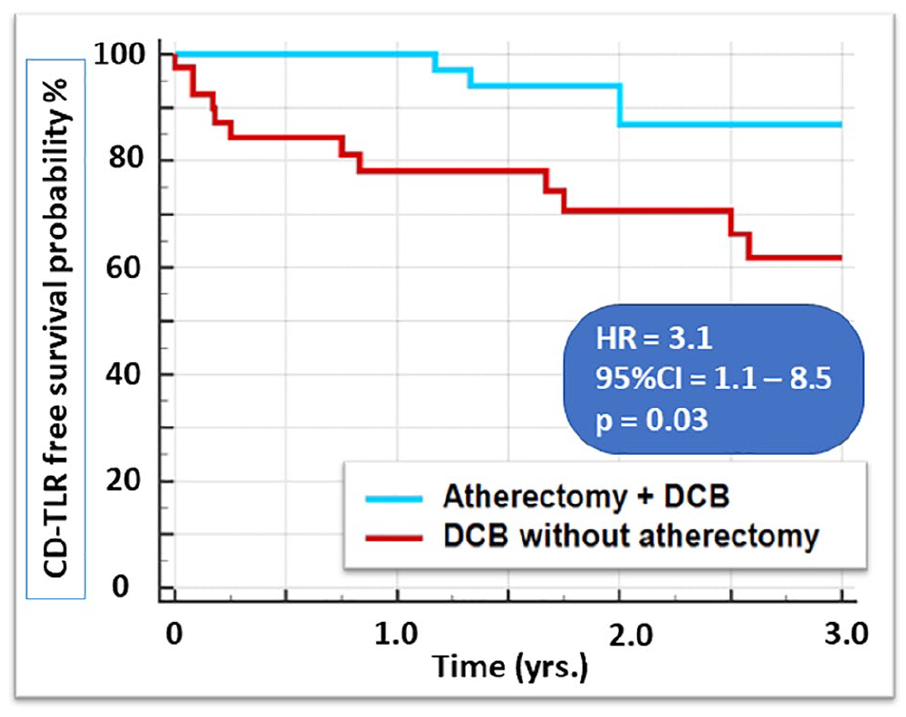
Using case–control matching, 40 patients from the single-center study were compared to a matched comparator group of 40 patients from the EMO-POP registry. Patients treated with the combination of atherectomy and DCB exhibited significantly higher freedom from CD-TLR during follow-up compared to a DCB only strategy.
Patient cases
Three representative cases of patients who underwent Phoenix atherectomy of the groin and the popliteal artery and CD-TLR, respectively, are provided in Supplemental Figures 1–3.
Discussion
Our study demonstrates that rotational or hybrid atherectomy using the Phoenix device can be used safely for the endovascular treatment of calcified and complex lesions in the CFA and popliteal artery with low complication rates, including no perforations and a single (0.8%) peripheral embolization. In addition, low rates of bail-out stenting were observed both with the CFA (2.7%) and with the popliteal artery (5.7%), considering the high overall complexity and calcification of the treated lesions. Good procedural and clinical success rates are provided by this treatment option with clinically acceptable TLR rates of 11.5% during 1.5 years of median follow-up. In all 13 cases requiring re-intervention due to CD-TLR, endovascular treatment was successfully performed. In addition, relatively high clinical success rates were observed. Finally, using case–control matching for RC at baseline and lesion characteristics, an atherectomy plus DCB strategy demonstrated higher freedom from CD-TLR compared to a DCB only strategy in the popliteal artery.
Previous studies in the CFA
Endovascular treatment has become the standardized approach and first choice for most peripheral lesions.1,14 In addition, recent studies have reported on the efficacy and long-term safety of endovascular atherectomy procedures in large patient cohorts. 15 Even in the CFA region, which has been so far considered as a surgical zone, 16 an increasing amount of evidence suggests that minimal invasive percutaneous therapy might be a valuable alternative in frail and older patients,5,17 or in obese patients, who may be more prone to perioperative complications such as wound healing. 18 So far, a direct comparison between surgical endarterectomy and endovascular treatment has been provided only in the TECCO trial. 19 This study, revealed that mid-term patency and freedom from TLR were comparable between endarterectomy and stent placement of the CFA even in anatomically complex CFA lesions, whereas morbidity and mortality were higher in patients undergoing open repair. 19 However, especially in complex lesions, including the CFA birfurcation, a trend for higher TLR rates has been reported previously. 20 In addition, since the CFA is a segment with mobile components and is vastly used as an access site for peripheral, coronary, and structural heart interventions, a no-stent strategy may be preferable for this vessel segment. Furthermore, where there are repeated endovascular failures in the groin, endarterectomy may be cumbersome in cases of one or more implated stents in this region. Traditional balloon angioplasty, on the other hand, previously showed unacceptably high restenosis rates of 28% at a 1-year follow-up. 21 In addition, the recent large-scale CAULIFLOWER study pointed to the inferior performance of nondebulking endovascular revascularization versus open repair, especially with calcified CFA disease, 22 so that advanced endovascular revascularization options become necessary with the treatment of this vessel segment. In respect to the choice between endovascular techniques and open repair, the multicenter randomized PESTO-AFC trial (NCT02517827) aims at this comparison and first results are expected during the next years.
Previous studies in the popliteal artery segment
Recent randomized controlled trials pointed to improved patency rates of drug eluting stents (DES) versus bare metal stents and DCB in femoropopliteal lesions.23,24 However, real-world studies pointed out that failures of DES in femoropopliteal segments result in more complicated lesion characteristics and occlusion extension to more distal segments beyond the point of patency loss. 3 This extension of the primary lesion or occlusion to more distal vessel segments may be associated with poorer limb outcomes, compared to DCB treatment failures. 3 This is particularly important for lesions located in the popliteal artery because extension of the occlusion to the P3 segment may exclude options for future bypass surgery. 3 Since biomechanical forces of external compression, torsion, and elongation occur with locomotion of the popliteal artery, stent placement may be associated with higher rates of thrombosis, fractures, in-stent restenosis (ISR), and occlusions. Therefore, DCB angioplasty with optional stent implantation is currently preferentially recommended, especially for distal SFA and popliteal artery lesions. 25
Recently, the multicenter EMO-POP registry reported on contemporary endovascular treatment options in patients referred for endovascular revascularization due to symptomatic popliteal artery lesions and occlusion in 651 patients. Patients were treated with various techniques, including plain old balloon angioplasty (POBA) (44%), DCB (15%), primary stenting (25%), and directional (14%) or rotational atherectomy (3%) partially combined with DCB. Hereby, both rotational and directional atherectomy combined with DCB performed better than POBA. In addition, rotational atherectomy exhibited higher patency rates compared to all other treatment strategies. However, rotational atherectomy was performed in a small group of patients, and a direct comparison between atherectomy and DCB versus a DCB only strategy could not be provided. 8
Current findings
We and others previously reported on the use of atherectomy combined with DCB angioplasty in the CFA and in femoropopliteal segments.4,5,9,13,17,26 –28 These studies showed a relatively low rate of bail-out stenting of the CFA after lesion preparation with atherectomy, even in strongly calcified lesions and in bifurcation lesions of the CFA/SFA and the DFA. In addition, previous studies demonstrated promising results with lower stent rates of the popliteal arteries after the use of lesion preparation techniques such as atherectomy or intravascular lithotripsy (IVL) compared to balloon angioplasty.29,30 Notably, atherectomy represents a lesion preparation strategy, which is then followed by definitive lesion treatment with balloon angioplasty, DCB and, if required, bail-out stenting, and not a stand-alone technique. In the present single-center study, we report on our experience of the use of rotational and hybrid assisted endovascular treatment of CFA and popliteal artery lesions (i.e., lesions located in two mobile vessel segments). The value of lesion preparation could be confirmed in the present analysis, aiding a ‘leave nothing behind’ strategy, combining plaque removal followed by DCB angioplasty since the rate of stent placement was lower than in previous observations. 5 In addition, low complication rates were observed in terms of perforation and distal embolization, all of which could be managed during the intervention, without affecting procedural success. Notably, no embolic filter protection devices were used with the procedures. In addition, higher procedural times, contrast agent doses, and radiation exposure were noted with CFA compared to popliteal lesions, which was attributed to higher lesion length and complexity and to concomitant iliac and femoropopliteal lesions requiring additional treatment. Patients with popliteal artery lesions were, on the other hand, a priori selected to extend up to 3 cm to the distal SFA or 1 cm to the crural arteries, by study protocol, so that despite the higher rate of CTOs, recanalization could be achieved faster and with less contrast administration. This process in the selection of the popliteal artery lesions needs to be considered when interpreting our results, which may not be applicable for more complex and longer femoropopliteal occlusions.
Using case–control matching from patients in the EMO-POP trial for RC and lesion characteristics, an atherectomy plus DCB strategy demonstrated higher freedom from CD-TLR, compared to a DCB in the popliteal artery. This underlines the use of lesion preparation strategies in mobile segments, resulting in low stent placement rates and higher freedom from CD-TLR, compared to a DCB only strategy.
Study limitations
Several limitations need to be acknowledged with our single-center observational study. First, our trial represents an observational study. A comparator arm is provided for the popliteal artery but not for the CFA, which is a limitation. In addition, a historical cohort was used after case matching for the popliteal artery and randomization was not performed, which is warranted in future studies. Furthermore, no comparisons with other atherectomy devices or by open repair are available. The size of the Phoenix catheter device, as well as the decision regarding the type of adjunctive treatment, was not defined a priori but was left at the discretion of the endovascular specialist in charge of the procedure. This might have influenced the results of the study and therefore needs to be considered. The same applies for adjunctive treatments such as DCB and especially bail-out stenting, which despite the TECCO trial is still controversially discussed in the mobile CFA segment since it represents a permanent challenge for future punctures, interventions, and/or open repair if ultimately required, in the groin area. Although a semiquantitative score was applied for the assessment of CFA and popliteal vessel lesion complexity, calcification was graded visually and not quantified (e.g., by intravascular ultrasound or computed tomography), and the evaluation of the anatomical location was not core-lab adjudicated. In addition, the walking distance for the assessment of RC was patient reported and not objectively measured. Furthermore, subgroup analysis for the influence of the CFA lesion complexity, including grade of calcification and bifurcation involvement on CD-TLR rates, was not regarded as meaningful and was therefore not reported in our study due to the small number of patients who underwent CD-TLR during follow-up, and this needs to be addressed in future multicenter studies with longer follow-up duration.
Conclusions
This study shows that hybrid atherectomy represents a safe and effective option, contributing to clinically acceptable clinically driven target lesion revascularization (CD-TLR) and clinical success rates for the endovascular revascularization of moderate to severely calcified lesions in CFA and popliteal artery segments with low rates of bail-out stenting in patients with symptomatic PAD. An atherectomy-assisted DCB strategy in the popliteal artery resulted in higher freedom from CD-TLR compared to a DCB only treatment strategy.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X241231943 – Supplemental material for Safety and effectiveness of the Phoenix atherectomy device for endovascular treatment of common femoral and popliteal arteries: Results of the EN-MOBILE trial
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X241231943 for Safety and effectiveness of the Phoenix atherectomy device for endovascular treatment of common femoral and popliteal arteries: Results of the EN-MOBILE trial by Christoph Schöfthaler, Nicola Troisi, Giovanni Torsello, Amila Jehn, Michael Lichtenberg, Jan C Karcher, Konstantinos Stavroulakis, Mario D’Oria, Athanasios Saratzis, Hany Zayed, Martin Andrassy and Grigorios Korosoglou in Vascular Medicine
Footnotes
Acknowledgements
We thank all the members of the EMO-POP registry collaborative group: Denise Özdemir-van Brunschot, Teresa Martín González, Thomas Denisselle, Giacomo Isernia, Stefano Michelagnoli, Antonio Nicola Giordano, Konstantinos P Donas, Apostolos G Pitoulias, Stavros Spiliopoulos, Massimiliano Martelli, Alberto Maria Settembrini, Emmanuel Katsogridakis, and Raffaella Berchiolli.
Data availability statement
Data included in this manuscript will be made available upon request to the corresponding author.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
GRN Hospital Weinheim (Grigorios Korosoglou) received an institutional research grant from Philips for this study.
Supplementary material
The supplementary material is available online with the article..
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.