
Abstract

Keywords
The Best Endovascular versus Best Surgical Therapy in Patients with Critical Limb-Threatening Ischemia (BEST-CLI) trial (ClinicalTrials.gov ID: NCT02060630) demonstrated that a surgery-first strategy reduced the risk of major adverse limb events or death compared with an endovascular-first strategy for chronic limb-threatening ischemia (CLTI) with a suitable condition for surgery (cohort 1). 1 However, the trial population was limited to patients with (1) standard surgical risk, (2) an adequate target artery for distal anastomosis of a surgical bypass, and (3) adequate quality of the great saphenous vein (GSV). Consequently, the trial population would not represent a real-world population with CLTI, especially in Japan.
This was a single-center and retrospective study. We retrospectively investigated how many patients with CLTI treated with endovascular therapy (EVT) in real-world practice met the eligibility criteria of the BEST-CLI. We included 352 consecutive patients with CLTI in whom the GSV was preoperatively assessed and who were primarily treated with EVT between January 2017 and December 2020 at our center. The dedicated duplex ultrasound technicians evaluated GSV diameter and quality using a standardized protocol that has been previously reported. 2 This study was performed in accordance with the Declaration of Helsinki and was approved by the ethics committee of Kansai Rosai Hospital (reference number: 16C036g). Standard surgical risk was defined as estimated perioperative and 2-year mortality rates of < 5% and < 50%, respectively, based on the Global Vascular Guidelines (GVG). 3 The mortality rates were estimated using the Surgical Reconstruction Versus Peripheral Intervention in Patients with Critical Limb Ischemia (SPINACH) score. 4 An adequate target tibial artery for distal anastomosis of a surgical bypass was defined as the Global Limb Anatomic Staging System (GLASS) inframalleolar descriptor of P0–1. 3 An adequate quality of GSV was defined as its diameter of ⩾ 3.0 mm. 1
Table 1 shows patient characteristics of the current study compared to the BEST-CLI trial. 1 The mean age was 72 years, 63.9% of patients were men, and the mean body mass index (BMI) was 21.7 kg/m2. Notable comorbidities included diabetes mellitus (63.1%) and hemodialysis (55.8%). Patients with standard surgical risk, inframalleolar patterns of P0–1, and an adequate quality of GSV accounted for 87.5% [95% CI, 83.6–90.8%] (308/352), 76.1% [71.3–80.5%] (268/352), and 46.3% [41.0–51.7%] (163/352), respectively. Only 32.7% [27.8–37.8%] of patients (115/352) met all three criteria (Supplemental Figure, available online).
Baseline characteristics of the current study and the BEST-CLI trial.
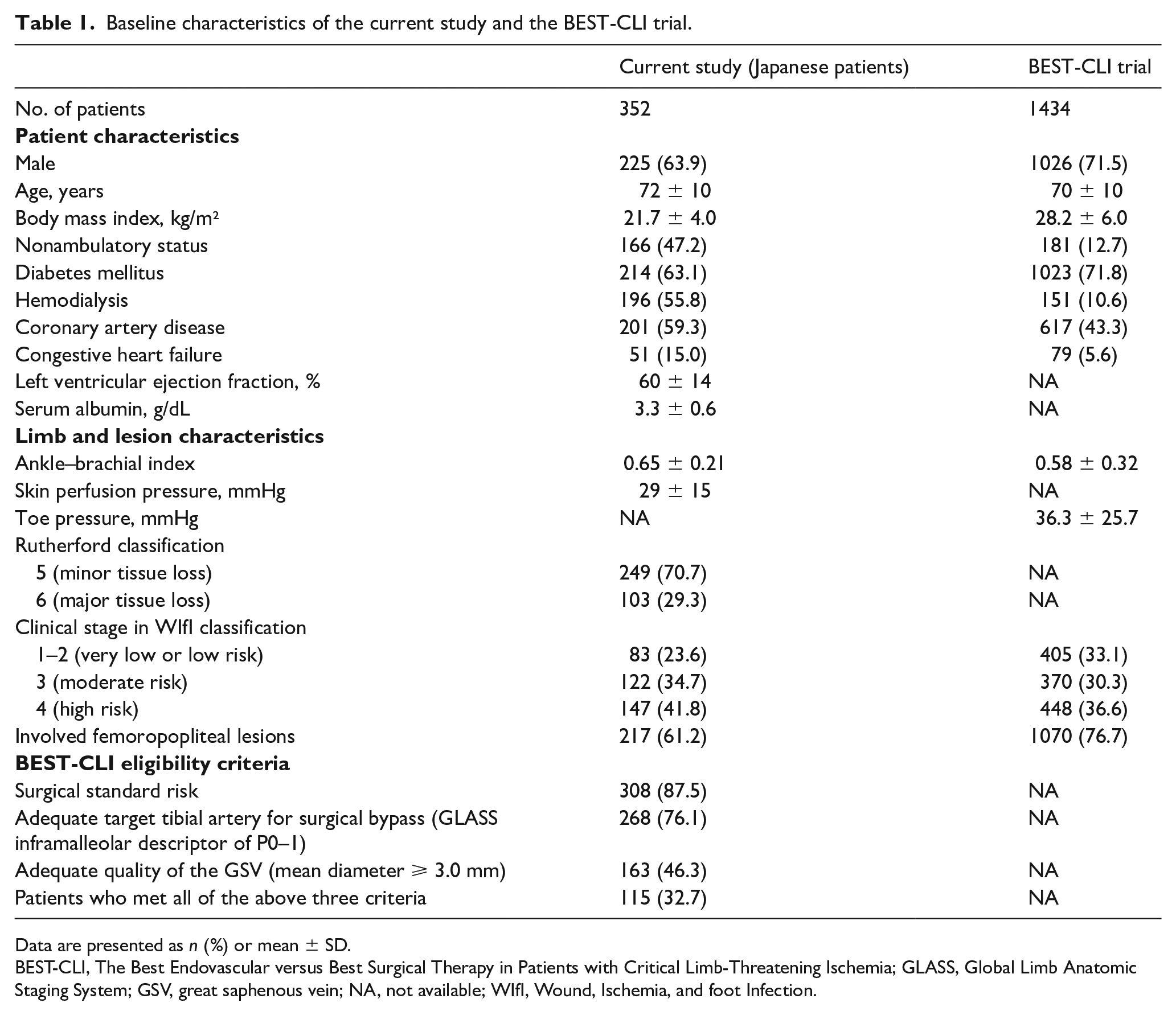
Data are presented as n (%) or mean ± SD.
BEST-CLI, The Best Endovascular versus Best Surgical Therapy in Patients with Critical Limb-Threatening Ischemia; GLASS, Global Limb Anatomic Staging System; GSV, great saphenous vein; NA, not available; WIfI, Wound, Ischemia, and foot Infection.
Only a small proportion of patients who met the main criteria of the BEST-CLI trial cohort 1 would reflect the clinical features of Japanese patients with CLTI. This study differs significantly from the BEST-CLI trial, where most participants were White, as our study included Asian patients. Baseline characteristics of Japanese patients with CLTI are mainly attributable to a higher prevalence of patients on hemodialysis, with nonambulatory status, and a low BMI. A previous study reported that renal insufficiency is independently associated with a distal distribution pattern of symptomatic lower-limb atherosclerosis and commonly with diffuse, severely calcified lesions along infrapopliteal arteries, 5 leading to a higher prevalence of GLASS P2. Additionally, our previous study reported that both a low BMI and nonambulatory status are correlated with a smaller diameter GSV. 2 Consequently, these would be attributed to the lower proportion of patients who meet the criteria of the BEST-CLI trial. Similar to this study, the results of the BEST-CLI trial may not be applicable to patients with CLTI who have a distinct ethnic and regional background from the randomized clinical trial.
When we additionally investigated the proportion of GVG-based bypass-preferred conditions defined as GLASS stage III and Wound, Ischemia, and foot Infection (WIfI) clinical stage 3–4 3 in our study population, the proportion was found to be only 8.8% [6.1%–12.3%] (31/352). The endovascular-first strategy would be a reasonable option if it does not damage the distal anastomosis of future surgical bypass. Although the results of the BEST-CLI trial report a high level of evidence, the results would not always be applicable in clinical practice. Further investigation is needed to determine whether and how the results of the BEST-CLI trial could apply to the Japanese population.
This study has several limitations. First, this was a retrospective single-center study. Second, the presence of an adequate target artery for surgical bypass was not evaluated based on a surgeon’s discretion. However, it has been reported that GLASS inframalleolar P2 was associated with poor clinical outcomes after bypass surgery in Japanese patients 6 ; P0–1 would be a practical indicator for the presence of an adequate target artery for surgical bypass. Third, this study did not enroll all patients with CLTI in the study period. During the study period, 659 patients with CLTI underwent primarily EVT. Out of these patients, 352 who had available data on the diameter of the GSV were selected for retrospective analysis. However, it is worth noting that the BEST-CLI trial itself may have introduced biases as it was not conducted on consecutive patients at participating facilities. Fourth, we included patients with CLTI with tissue loss, and excluded those with only rest pain. Fifth, the length of the GSV was not assessed in the current study. Finally, we were unable to perform statistical comparisons with the BEST-CLI trial, which constitutes a limitation of our study.
In conclusion, only a small proportion of Japanese patients with CLTI in clinical practice met the main criteria of the BEST-CLI trial cohort 1.
Supplemental Material
sj-tif-1-vmj-10.1177_1358863X231205229 – Supplemental material for Japanese real-world population with chronic limb-threatening ischemia who meet the criteria of the BEST-CLI trial
Supplemental material, sj-tif-1-vmj-10.1177_1358863X231205229 for Japanese real-world population with chronic limb-threatening ischemia who meet the criteria of the BEST-CLI trial by Yosuke Hata, Osamu Iida, Shin Okamoto, Takayuki Ishihara, Takuya Tsujimura, Naoko Higashino, Taku Toyoshima, Sho Nakao, Mitsuyoshi Takahara and Toshiaki Mano in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.