
Abstract

Uterine intravenous leiomyomatosis (IVL) is a rare and often misdiagnosed condition characterized by the proliferation of benign smooth muscle cells of the uterus into the extrauterine intraluminal venous or lymphatic vessels. 1 This condition can become life-threatening if the tumor spreads to affect the inferior vena cava (IVC) or right heart chambers. 2
IVLs are surgically classified into four stages by their pattern of growth: Stage I: tumor confined within the pelvic cavity; Stage II: tumor has reached the iliac vein or IVC to the level of the renal vein; Stage III: distal extension beyond the renal vein into the right atrium/ventricles; Stage IV: expansion into the pulmonary arteries. 3 Here we discuss a patient with asymptomatic Stage IV IVL highlighting the potential for delayed diagnosis in this cohort.
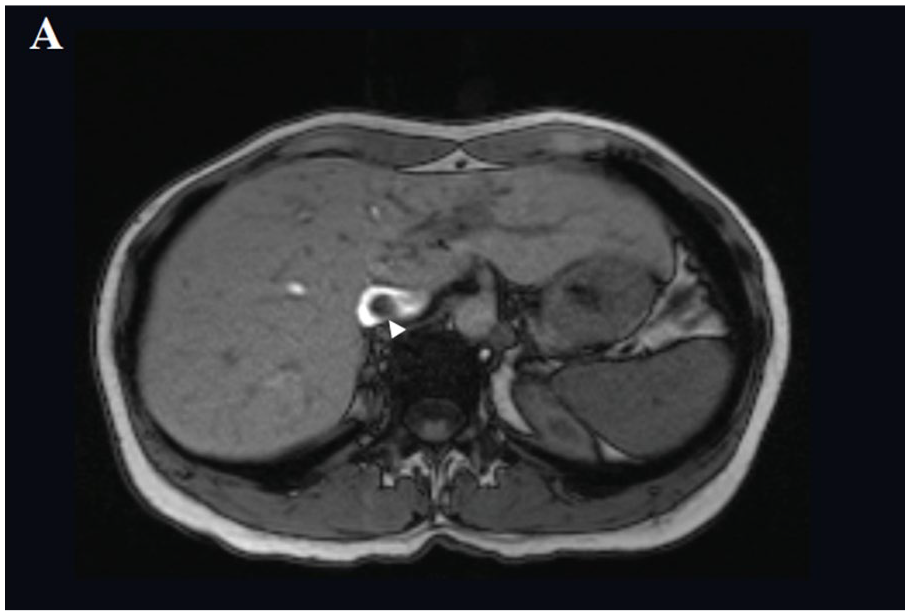
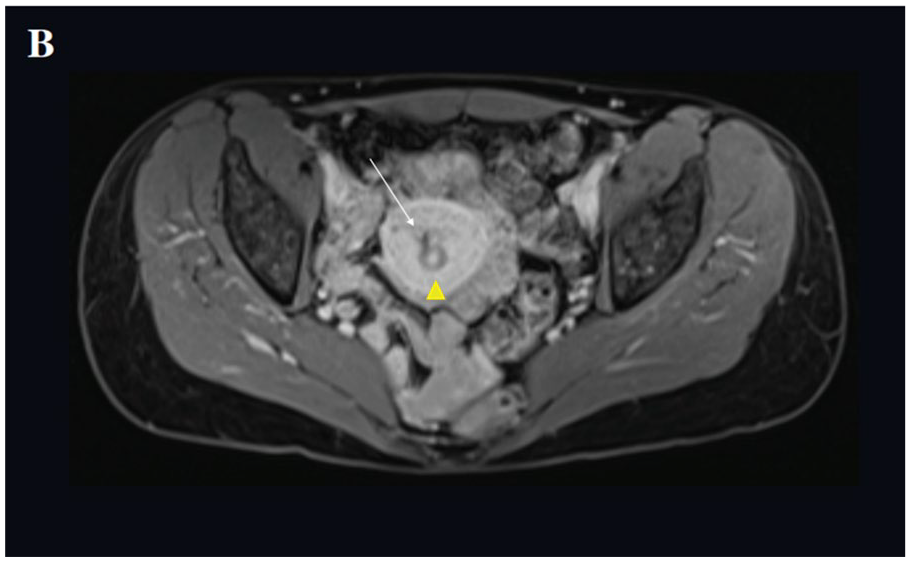
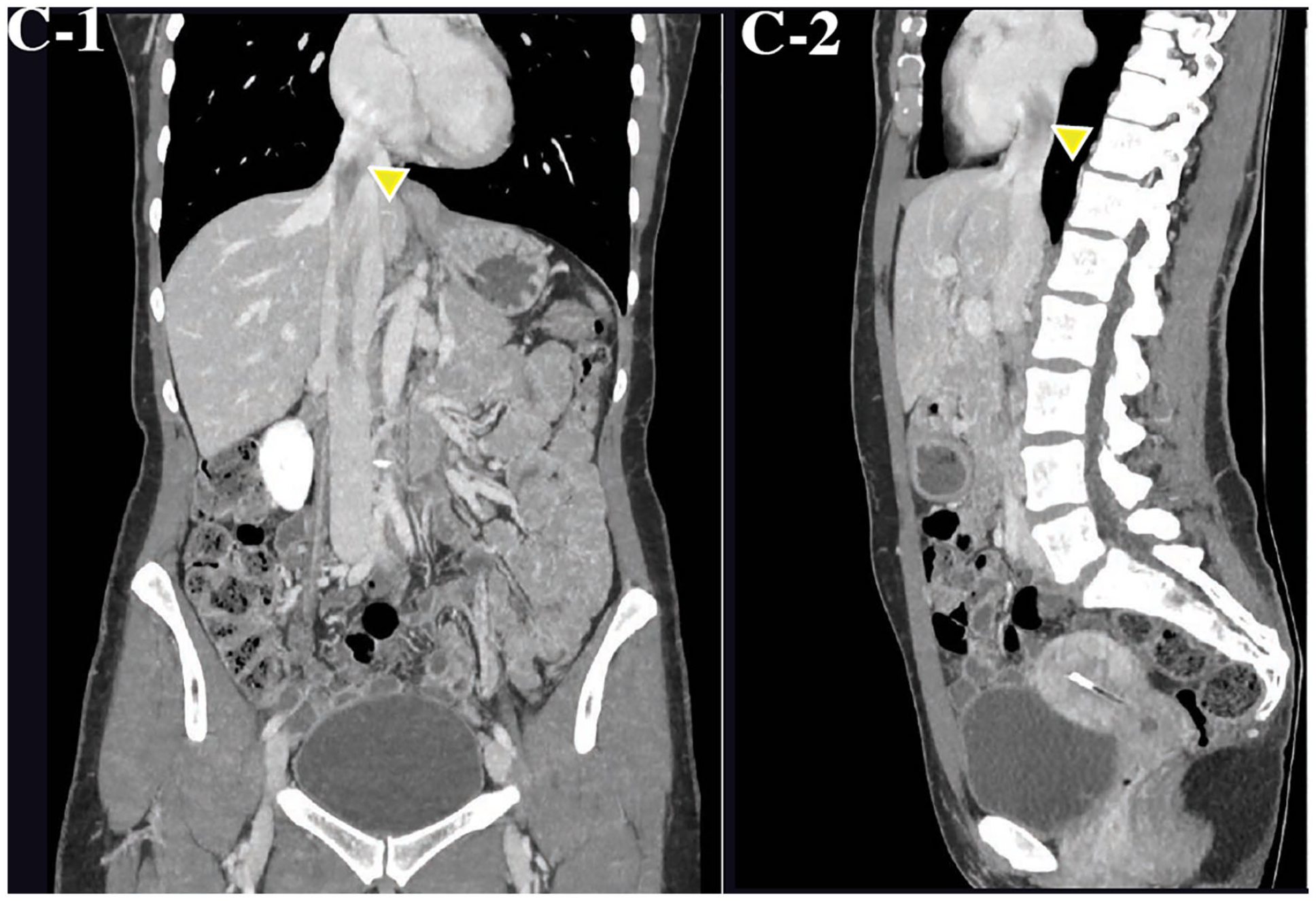
An asymptomatic 48-year-old woman was admitted for investigation and treatment of an incidental finding of a 12-cm thrombus in her IVC. Repeat magnetic resonance imaging (MRI) confirmed the nonocclusive thrombus within the hepatic IVC (Panel A: arrowhead) and right gonadal vein as well as a 13-mm fibroid (Panel B: arrowhead) next to an appropriately sited intrauterine device (Panel B: arrow). The patient was treated with therapeutic anticoagulation for 3 months, with thrombus regression of 5 cm. Despite continuation of treatment, at 6 months a repeat computed tomography venogram demonstrated thrombus extension into the right atrium (Panel C, arrowheads).
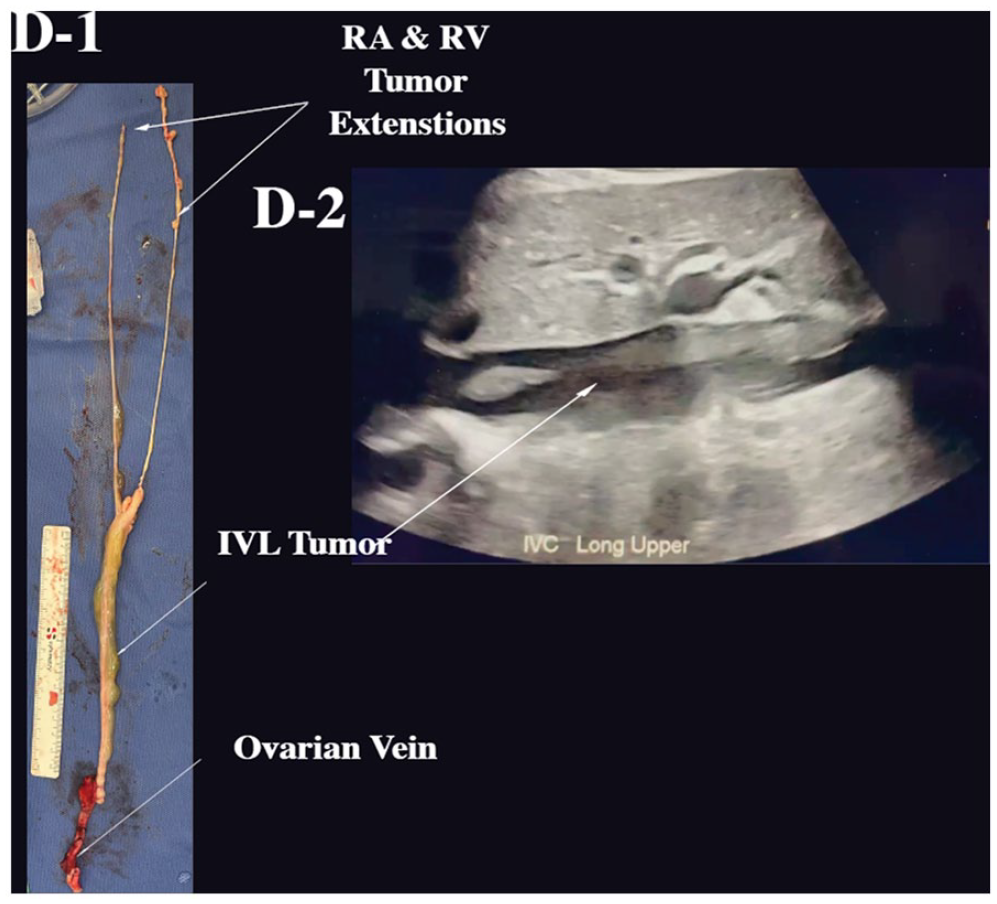
Right gonadal vein ligation and clot extraction under deep hypothermic circulatory arrest was performed and it was found intraoperatively that the thrombus had extended beyond the right atrium (RA), right ventricle (RV), and likely into the pulmonary arteries, as seen on the excised specimen and the transverse ultrasonographic still of the IVL tumor in the IVC (Panel D). Histopathology and immunochemical studies showed an angioleiomyoma with strong staining for caldesmon, SMA, desmin, and positive staining for estrogen and progesterone receptors. A total hysterectomy with bilateral salpingo-oophorectomy was performed 6 months after diagnosis. Follow up at 18 months postgonadal vein ligation showed no imaging evidence of recurrence of IVL.
Diagnosis of IVL is difficult due to its rarity and wide variety of clinical presentations. 4 The definitive treatment for IVL is through complete removal of the tumor from the blood vessels as well as total hysterectomy and oophorectomy to prevent recurrence. 5 In this case, gynecological surgery was not performed at the time of intravascular tumor excision due to the diagnostic uncertainty. Despite this, our case shows that ligation of the originating vein may be sufficient to prevent short-term recurrence of the disease.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.