
Abstract

Internal mammary artery (IMA) aneurysms are rare clinical entities. Immediate treatment is warranted due to the high risk of rupture which can result in hemothorax and life-threatening complications. IMA aneurysms are usually iatrogenic (typically following thoracotomy, sternotomy, insertion of a central venous catheter, or percutaneous biopsy), or associated with vasculitis, connective tissue disorders, or fibromuscular dysplasia.1,2
We describe the case of a patient presenting with two idiopathic spontaneous IMA aneurysms. She is a right-handed teacher with a background history of asthma, migraines, and obesity, who underwent laparoscopic gastric banding 10 years prior to presentation. There was no reported family history of aneurysms, dissections, sudden deaths, or early cardiovascular events to suggest heritable arteriopathy. She initially presented to the emergency department with right middle lobe bronchopneumonia. Following treatment with oral amoxicillin, repeat plain films more clearly revealed a well-defined opacity in the right upper zone, posterior to the median clavicle. Subsequent high-resolution computed tomography (CT) of the chest suggested that this lesion was related to the right IMA.
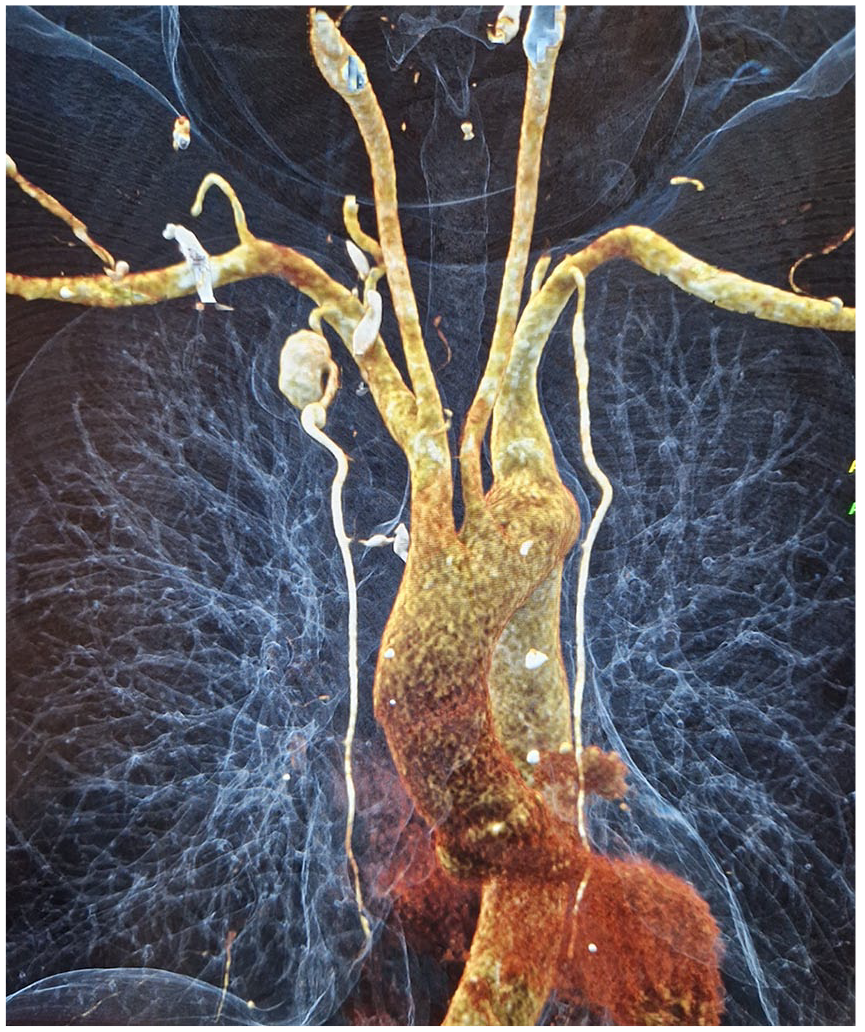
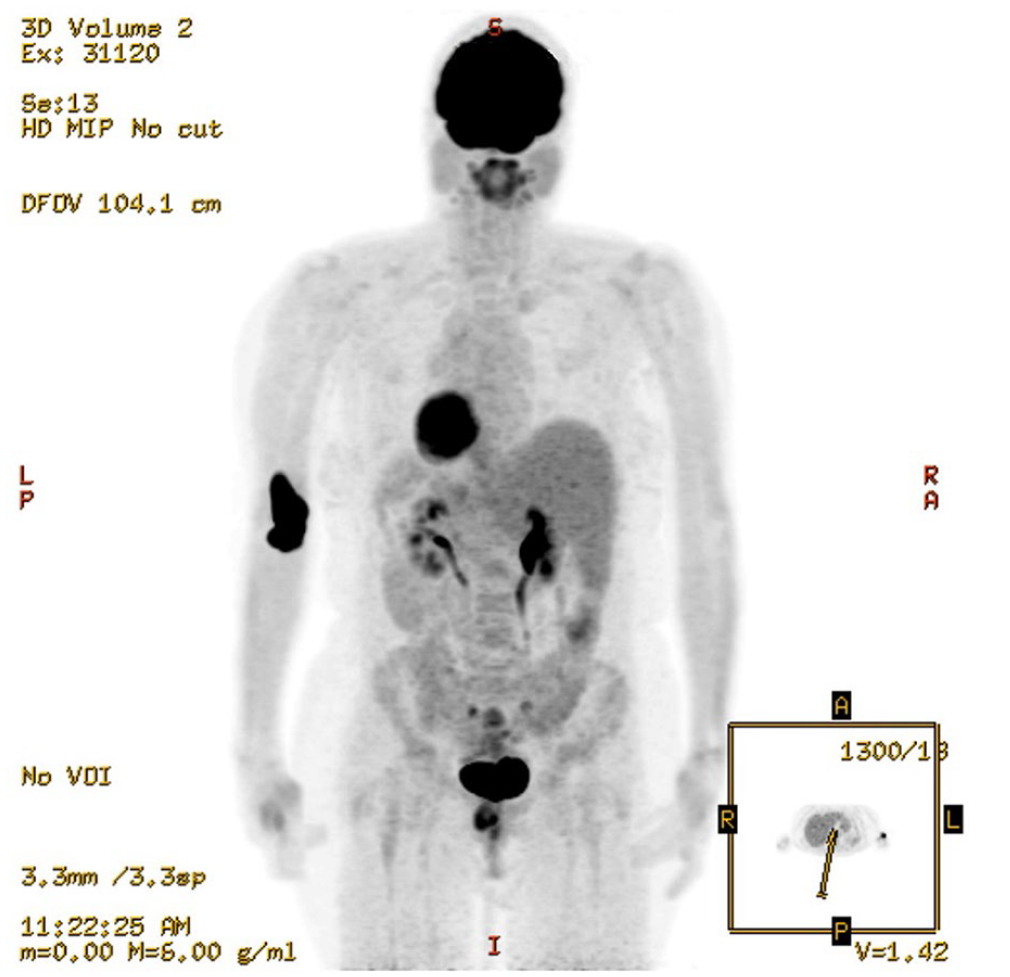
A CT angiogram of her aorta demonstrated an 18 mm aneurysm of the right IMA with a further 6 mm aneurysm distally, with no other signs of arteriopathy (Panel A, cinematic rendering of CT image showing the aneurysms). The patient remained asymptomatic. There was no history of cardiovascular disease, prior surgery, or chest trauma. She was systemically well. Inflammatory markers were normal, with an erythrocyte sedimentation rate (ESR) of 6 mm/h, plasma viscosity (PV) of 1.50 mPa/s, and C-reactive protein (CRP) < 5 mg/L. Her vasculitis screen for antinuclear antibodies (ANA), antineutrophil cytoplasmic antibodies (ANCA), anti-myeloperoxidase (MPO), anti-proteinase 3 (PR3), and antiphospholipid antibodies was negative, and immunoglobulins were normal. 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET)/CT demonstrated no FDG uptake within the aneurysms, with no other evidence of active vasculitis (Panel B).
A decision was made to treat the aneurysm with coils rather than a stent graft due to the risk of trauma to vessel and stent thrombosis secondary to small caliber landing zones. The aneurysms were treated with an endovascular approach via retrograde right transradial access; a 4 French access kit (Cordis Corporation, Florida, USA) was used for catheterization (Panel C). Concerto coils (Medtronic, Minneapolis, USA) were used for embolization of the aneurysms with no on-table complications. A completion angiogram confirmed successful exclusion of the aneurysms from the circulation (Panel D).


To our knowledge, this is the first described case of a patient with multiple IMA aneurysms without clear etiology. An endovascular approach by coil embolization or stent deployment is recommended because it is low risk and avoids the risk of rupture in these rare aneurysms. 3 Our case raises the important observation that IMA aneurysms can occur in patients without a history of trauma or underlying vascular pathology.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.