
Abstract
Background:
Atherosclerotic cardiovascular disease is highly prevalent in patients with end-stage kidney disease (ESKD). Kidney transplant (KT) improves patient survival and cardiovascular outcomes. The impact of preexisting coronary artery disease (CAD) and peripheral artery disease (PAD) on posttransplant outcomes remains unclear.
Methods:
This is a retrospective study utilizing the United States Renal Data System. Adult diabetic dialysis patients who underwent first KT between 2006 and 2017 were included. The study population was divided into four cohorts based on presence of CAD/PAD: (1) polyvascular disease (CAD + PAD); (2) CAD without PAD; (3) PAD without CAD; (4) no CAD or PAD (reference cohort). The primary outcome was 3-year all-cause mortality. Secondary outcomes were incidence of posttransplant myocardial infarction (MI), cerebrovascular accidents (CVA), and graft failure.
Results:
The study population included 19,329 patients with 64.4% men, mean age 55.4 years, and median dialysis duration of 2.8 years. Atherosclerotic cardiovascular disease was present in 28% of patients. The median follow up was 3 years. All-cause mortality and incidence of posttransplant MI were higher with CAD and highest in patients with polyvascular disease. The cohort with polyvascular disease had twofold higher all-cause mortality (16.7%, adjusted hazard ratio (aHR) 1.5, p < 0.0001) and a fourfold higher incidence of MI (12.7%, aHR 3.3, p < 0.0001) compared to the reference cohort (8.0% and 3.1%, respectively). There was a higher incidence of posttransplant CVA in the cohort with PAD (3.4%, aHR 1.5, p = 0.01) compared to the reference cohort (2.0%). The cohorts had no difference in graft failure rates.
Conclusions:
Preexisting CAD and/or PAD result in worse posttransplant survival and cardiovascular outcomes in patients with diabetes mellitus and ESKD without a reduction in graft survival.
Keywords
Background
Patients with end-stage kidney disease (ESKD) and diabetes mellitus (DM) have a high prevalence of coronary artery disease (CAD) and peripheral artery disease (PAD), and a high incidence of cardiovascular events and related mortality.1 –4 In 2020, the prevalence of CAD and PAD in the United States was reported to be 51.5% and 49.3%, respectively, in adult patients with DM and ESKD on hemodialysis. 1 Kidney transplantation (KT) reduces the risk of adverse cardiovascular outcomes and mortality in patients with ESKD compared to those who remain on chronic dialysis.4–6 Despite the survival benefits of KT, cardiovascular disease (CVD) remains a common cause of morbidity and mortality in KT recipients with functioning allografts.7 –9 This risk is likely higher in patients with preexisting CAD. However, there are limited data on post-KT cardiovascular outcomes in KT recipients with preexisting CVD, which is mostly derived from small studies.10 –12 Further, there are no data on post-KT outcomes in patients with polyvascular disease (CAD+PAD). Understanding these associations is important as both CAD and PAD are highly prevalent in patients with ESKD and DM undergoing KT. Further, with increasing age and comorbidity burden in patients undergoing KT, the prevalence of these diseases is likely to increase in the future. We utilized the United States Renal Data System (USRDS) to study cardiovascular outcomes and mortality in dialysis-dependent patients with diabetes and preexisting CAD, PAD, or polyvascular disease who underwent successful KT.
Methods
Data source
This is a retrospective study utilizing the USRDS. The USRDS is a national database that includes information on all patients with ESKD and a representative sample of patients with non-end-stage chronic kidney disease in the United States. 1 The USRDS also maintains data on patients for up to 3 years post-KT. The USRDS is funded directly by the National Institute of Diabetes and Digestive and Kidney Disease (NIDDK). The study was reviewed and approved by the institutional review board of the University of Kansas Medical Center and is within the scope of a data user agreement between the University of Kansas and the USRDS.
Study population
We identified dialysis-dependent patients with ESKD and DM, who were 18 years or older and underwent their first KT between January 1, 2006 and January 1, 2017. We excluded patients who did not have KT hospitalization records as well as patients who did not have Medicare as primary coverage at the time of KT. In the USRDS, Medicare claims data provide a complete picture only for those patients for whom Medicare is the primary insurance payer. For patients with other healthcare insurers or for whom Medicare is a secondary payer, information is not captured for hospitalizations or other treatments paid for by an alternate insurance, potentially leading to inaccurate results. In addition, patients who directly proceeded to KT or had less than 3 months of dialysis duration prior to KT were excluded.
The study population was then categorized into four cohorts based on the presence of advanced CAD and/or PAD. For study purposes, a patient was identified as having CAD if they had a history of either percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG). Patients with CAD but no prior PCI or CABG were excluded from the study. This criterion was applied with the intent to identify patients with true, established CAD and exclude patients with a possible less certain diagnosis of CAD. The ascertainment of DM, CAD, PAD, and related comorbid conditions was determined using the International Classification of Diseases, 9th and 10th (ICD-9/-10) diagnosis codes 13 from the KT hospitalization and the Center for Medicare and Medicaid Services (CMS) Form 2728 (online Supplemental Table S2).
Cohort 1 included patients with polyvascular disease (CAD + PAD). Cohort 2 included patients with CAD but no prior diagnosis of PAD. Cohort 3 included patients with PAD but no CAD. Cohort 4, which was the reference group, included patients with neither CAD nor PAD based on study inclusion criteria. Patients were followed until death, end of Medicare coverage, or December 31, 2019 (end of the 3-year maximum post-KT follow up in the USRDS for patients transplanted on the last day of the study inclusion period).
Outcomes
Our primary outcome was 3-year all-cause mortality. Our secondary outcomes were incident post-KT myocardial infarction (MI), post-KT cerebrovascular accident (CVA), and graft failure. The secondary outcome of CVA included both ischemic and hemorrhagic CVA. ICD-9/-10 diagnosis codes were used to find the outcomes of MI from any discharge diagnosis position and CVA from the primary discharge diagnosis position (online Supplemental Table S2). Graft failure was defined as retransplant or re-initiation of dialysis at least 3 months after index transplant hospitalization. The 3-month mark was selected to exclude patients requiring dialysis due to delayed graft function after index transplantation. For the assessment of primary and secondary outcomes during follow up, patients who died during the index hospitalization were excluded. We compared the incidence of outcomes in each of the cohorts 1–3 with the control group (Cohort 4).
Statistical analysis
Continuous variables, such as age, dialysis duration, Elixhauser comorbidity index, and follow-up period, were expressed as mean with SD or median with IQR. Categorical variables, such as sex, dialysis modality, and comorbidities, were expressed as frequencies with percentages. Continuous variables were compared using a two-sample t-test or Wilcoxon rank-sum test, and categorical variables were compared using Pearson’s chi-squared test. Cumulative incidence curves using the Kaplan–Meier approach were presented, and log-rank tests were used for intergroup comparison. We also performed multivariate Cox regression and reported hazard ratios after adjustment of age groups, sex, race, dialysis duration, comorbid conditions including congestive heart failure (CHF), chronic obstructive pulmonary disease, CVA/transient ischemic attack (TIA), cancer, dysrhythmia, hypertension, liver disease, and Elixhauser comorbidity index. All data extraction and analyses used SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA). Two-sided p < 0.05 was used for statistical significance.
Results
Study population
A total of 19,329 patients were included in the final study analysis after application of study inclusion and exclusion criteria (Figure 1). Table 1 shows the baseline characteristics including demographics and comorbid conditions of the overall study population as well as the patients in each cohort. Men comprised 64.4% of the study population and the overall mean age was 55.4 years. The mean duration on dialysis was 3 years, with 84.8% of the patients receiving hemodialysis. Atherosclerotic disease in at least one vascular system was present in 27.9% of patients and 4.7% had both advanced CAD and PAD.
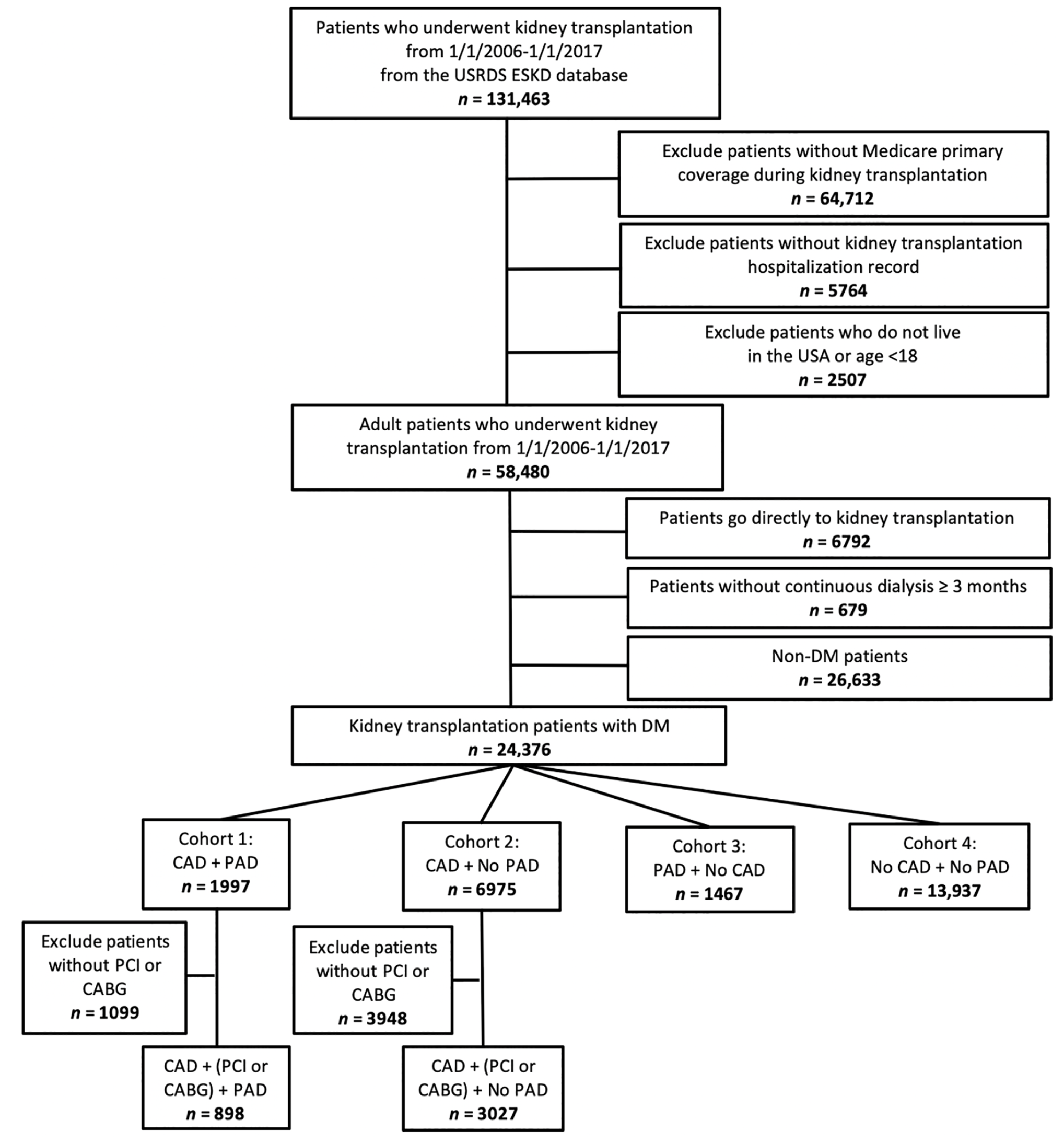
Consort diagram showing derivation of study population.
Baseline demographic characteristics and comorbid conditions of kidney transplantation patients with diabetes mellitus.
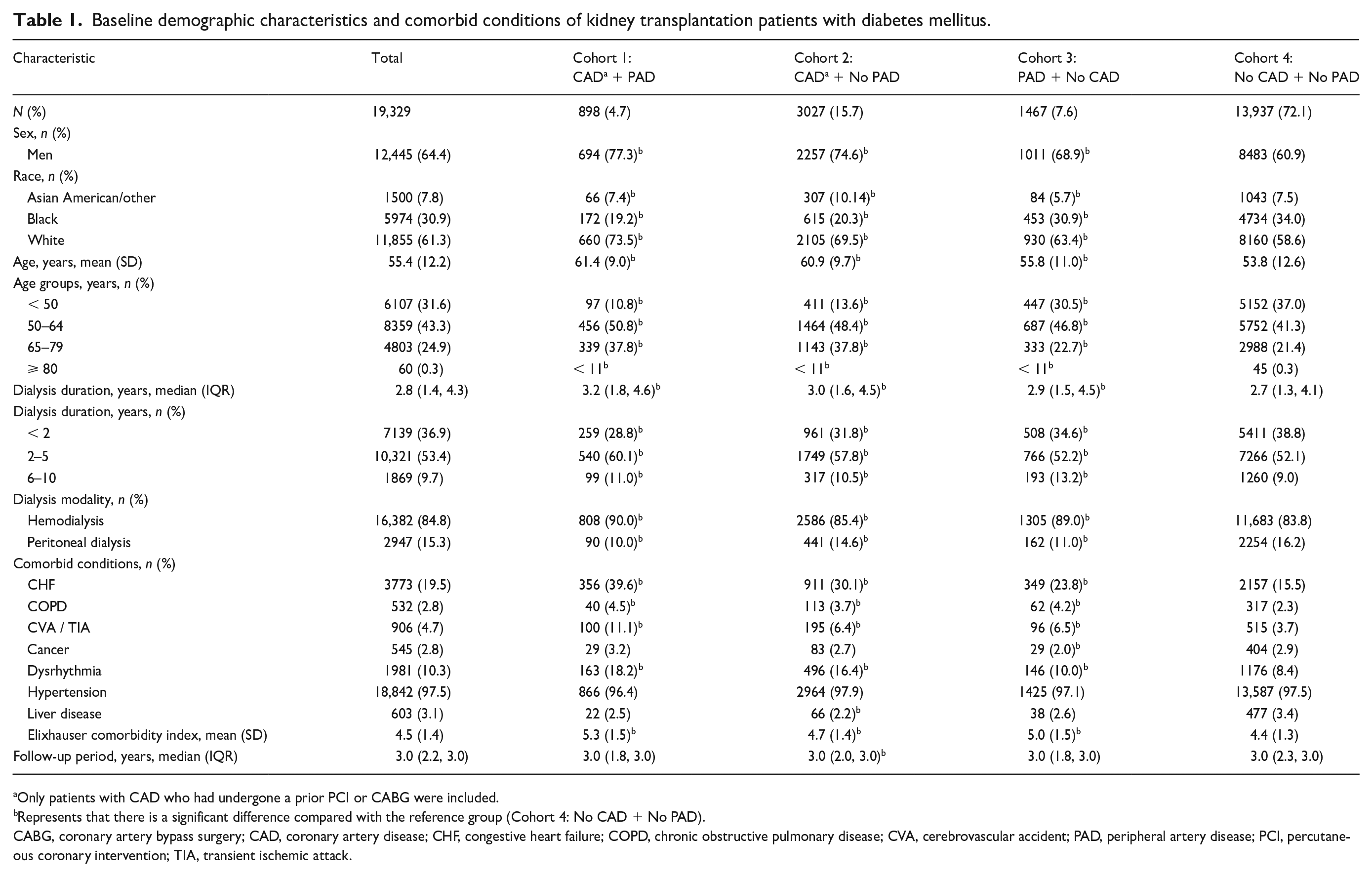
Only patients with CAD who had undergone a prior PCI or CABG were included.
Represents that there is a significant difference compared with the reference group (Cohort 4: No CAD + No PAD).
CABG, coronary artery bypass surgery; CAD, coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; TIA, transient ischemic attack.
Cohorts 1 and 2 had a higher percentage of older patients, men, and White patients. These patients also had a higher prevalence of comorbidities such as CHF, prior CVA/TIA, and dysrhythmias. The Elixhauser comorbidity index was similar in all cohorts. All four cohorts had a median follow-up period of 3 years.
Primary outcome
Table 2 and Figure 2 detail the study outcomes. The primary outcome of 3-year all-cause mortality was highest in Cohort 1 (16.7%), followed by Cohort 2 (13.8%) and Cohort 3 (12.8%), and was lowest in the reference Cohort 4 (8.0%).
Three-year outcomes and adjusted hazard ratio in kidney transplantation patients with diabetes mellitus during follow-up.
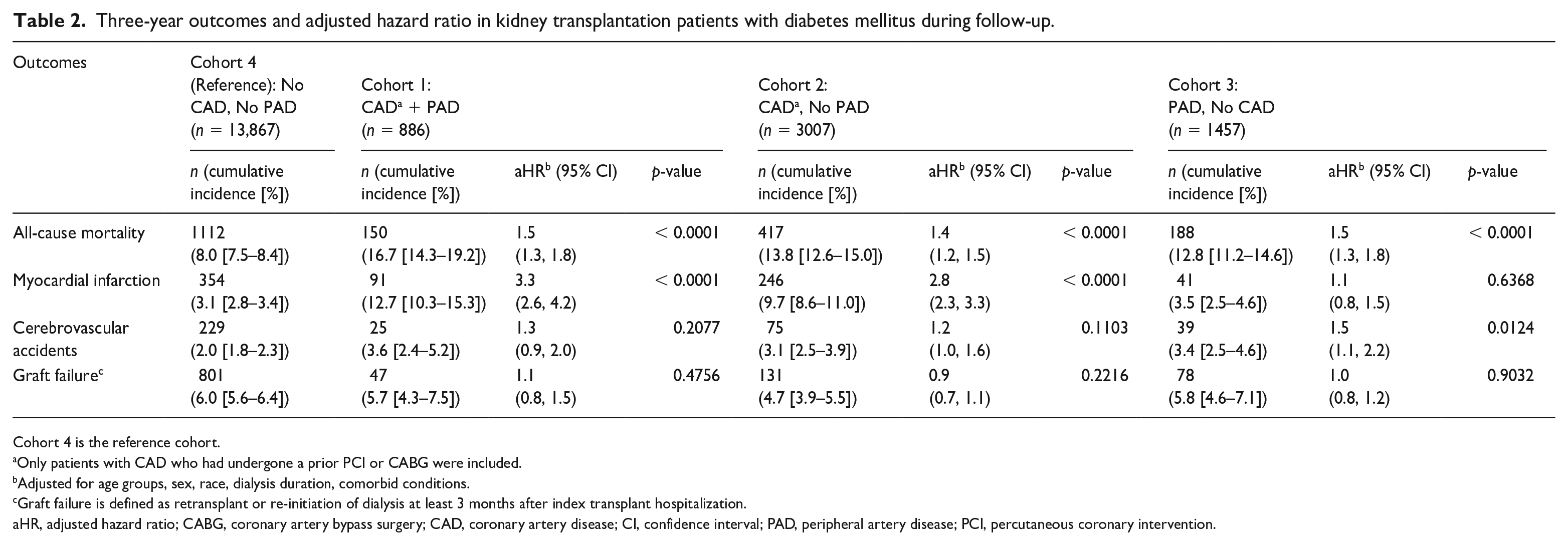
Cohort 4 is the reference cohort.
Only patients with CAD who had undergone a prior PCI or CABG were included.
Adjusted for age groups, sex, race, dialysis duration, comorbid conditions.
Graft failure is defined as retransplant or re-initiation of dialysis at least 3 months after index transplant hospitalization.
aHR, adjusted hazard ratio; CABG, coronary artery bypass surgery; CAD, coronary artery disease; CI, confidence interval; PAD, peripheral artery disease; PCI, percutaneous coronary intervention.
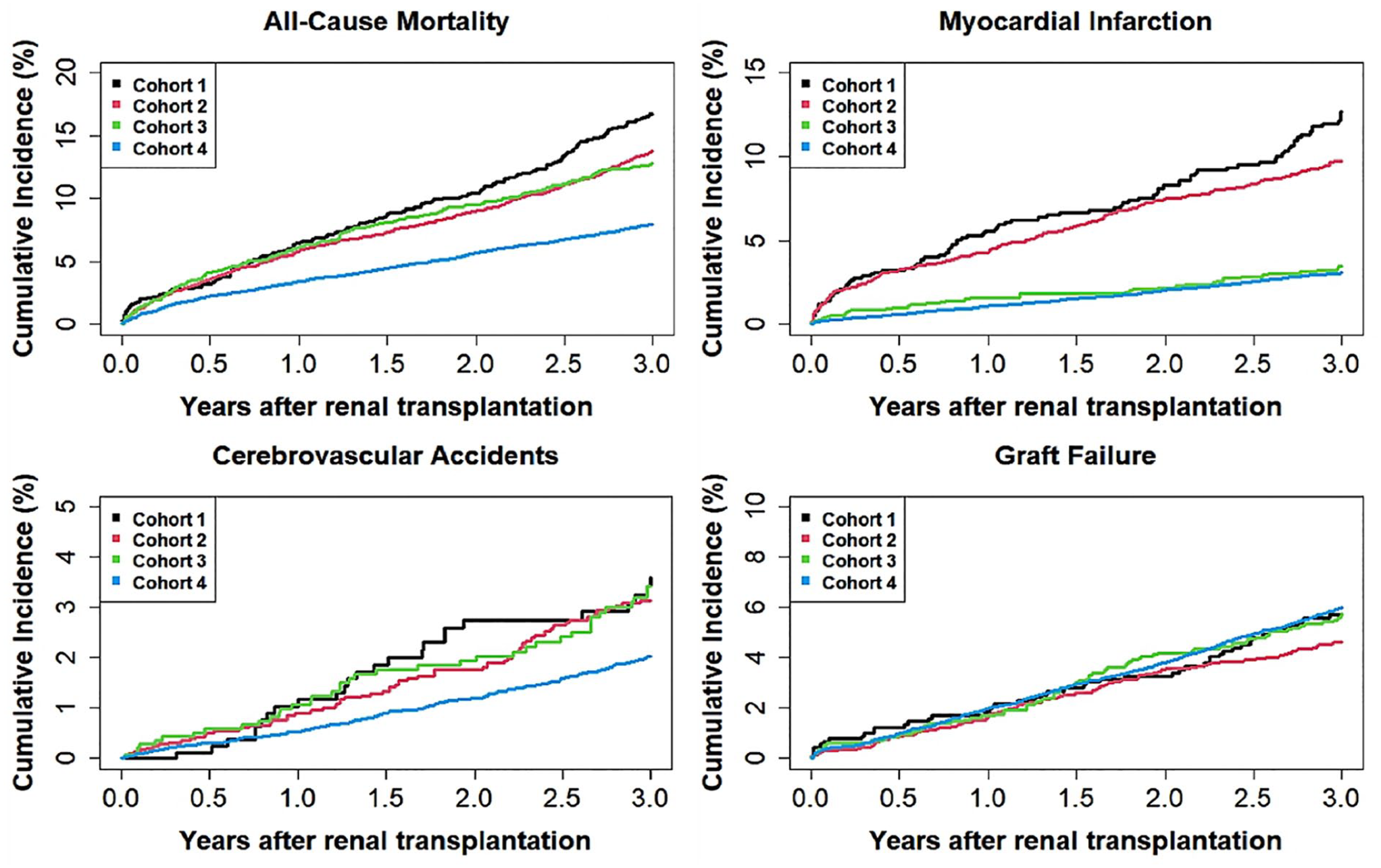
Cumulative incidence curves for the study outcomes in kidney transplant recipients with diabetes mellitus.
On multivariate regression analysis, the predictors of 3-year all-cause mortality were older age, being White, dialysis duration > 2 years, comorbidities including CHF, chronic obstructive pulmonary disease, prior CVA/TIA, cancer, dysrhythmias, and liver disease (Figure 3 and online Supplemental Table S1).
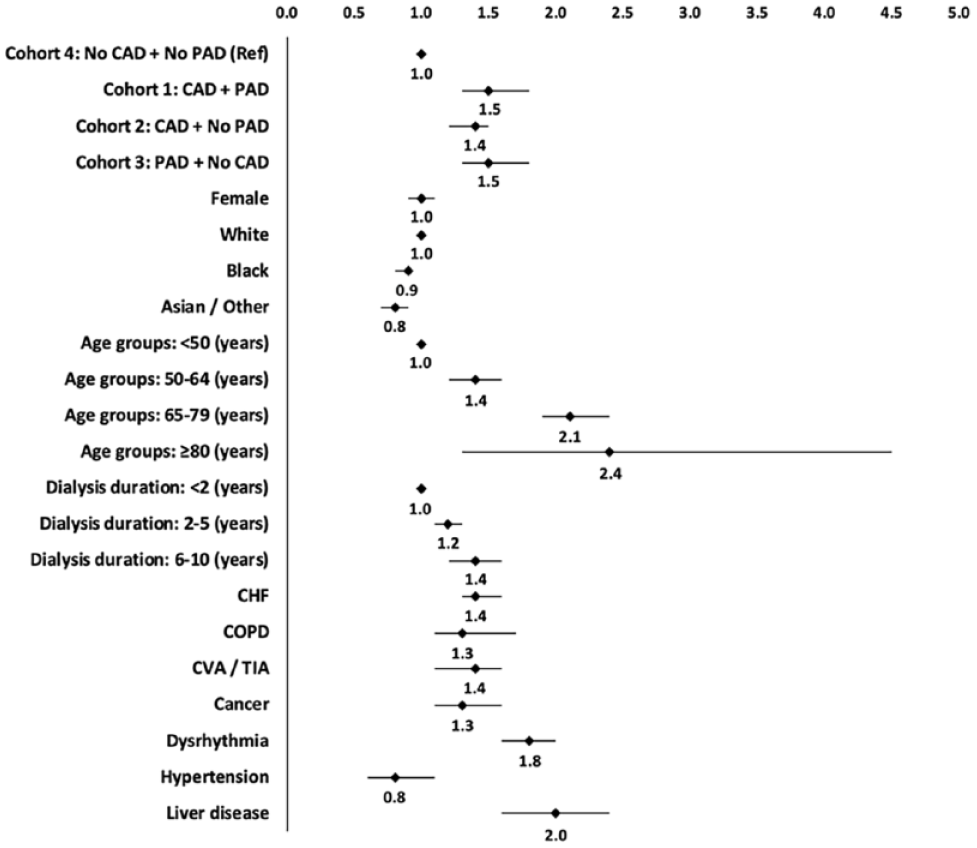
Multivariable adjusted hazard ratios with 95% CIs for impact of coronary artery disease and peripheral artery disease on 3-year all-cause mortality in kidney transplant recipients with diabetes mellitus.
After adjustment for age, sex, race, dialysis duration and comorbid conditions, the hazard ratio for all-cause mortality remained significantly elevated in all three cohorts compared to the reference cohort (Table 2).
Secondary outcomes
Table 2 details the secondary outcomes results. Compared to the reference cohort, the 3-year incidence of MI was four times higher in Cohort 1 (12.7% vs 3.15%) and three times higher in Cohort 2 (9.7% vs 3.15%). The incidence of MI was not different from the reference group in Cohort 3 (PAD but no CAD). These findings remained significant after adjustment for baseline differences. On multivariate regression analysis, the predictors of a higher incidence of MI at 3 years after KT were age 50–79 years, dialysis duration > 2 years, CHF, and prior CVA/TIA.
The 3-year incidence of post-KT CVA in Cohorts 1, 2, 3, and 4 was 3.6%, 3.1%, 3.4%, and 2%, respectively. After adjustment for baseline differences, this difference remained significant only in Cohort 3 (HR 1.5, 95% CI 1.1, 2.2; p = 0.012). On multivariate regression analysis, the predictors of higher incidence of CVA were age 50–79 years and prior CVA/TIA.
There was no statistically significant difference in the incidence of graft failure based on presence of CAD or PAD in the overall population of diabetic KT recipients. However, Black patients were found to have a significantly higher incidence of graft failure as compared to other races.
Discussion
The relative risk of all-cause mortality and cardiovascular events after KT in patients with diabetes and ESKD with preexisting multiterritory atherosclerotic disease is not quantified well. Our study fills this knowledge gap. In this large, nationwide study of patients with diabetes undergoing KT, we found that the presence of underlying CAD or PAD was associated with a significantly higher 3-year risk of all-cause mortality after KT. Further, the presence of polyvascular disease (CAD + PAD) resulted in an even higher risk of all-cause mortality. Patients with polyvascular disease had a fourfold higher 3-year risk of MI, and those with CAD alone had a threefold higher 3-year risk of MI than those without CAD or PAD.
KT is the optimal ESKD treatment, resulting in improved outcomes and mortality. 14 Compared to maintenance hemodialysis, long-term cardiovascular outcomes are significantly improved in patients with ESKD after KT. A study of 11,369 patients with diabetes and ESKD (enrolled in the kidney or kidney-pancreas transplant waiting list from 1994 to 1997 identified from the USRDS) found a significantly lower risk of an acute coronary syndrome in patients after KT than those who remained on maintenance dialysis. 5 Another USRDS study of 53,297 patients with ESKD who underwent KT from 1995 to 2002 showed a significant overall relative risk reduction in the incidence of acute myocardial infarction after KT compared to those on the waiting list. 6 However, these data are from all patients undergoing KT without regard to the presence of prior CAD. It is generally believed that those with underlying CAD will have a worse post-KT prognosis as many factors in the post-KT milieu predispose patients to a higher risk of CVD (such as hypertension, immunosuppression, posttransplant diabetes, etc.). 15 Further, it has been reported that patients with preexisting severe CAD are less likely to be listed for transplant due to concern for poor outcomes. 16
However, only limited information is available on outcomes after KT in patients with preexisting CAD, and this is mostly from smaller, single-center studies.10,11,17 In a study of 429 post-KT patients (only 61 with prior CAD with angina, MI, or angiographic CAD and 368 without CAD), the authors reported a significantly higher cardiovascular event rate (MI, angina, or arrhythmia) in the CAD group (31.3% vs 6.5%) and lower survival (82.8% vs 93.1%) at a mean follow up of about 3 years. 10 Similarly, in another single-center study, Felix et al. reported on 403 patients post-KT (296 had CAD with 89 having had revascularization). 11 The primary endpoint of cardiovascular mortality, acute coronary syndrome, or post-KT revascularization at the 5.6-year follow up occurred in 5% of those without CAD, 23% in those with CAD, and 26% in those with CAD and prior revascularization (HR 4.39, p = 0.002). All-cause mortality was 7%, 21%, and 24%, respectively (p = 0.07). Our large, nationwide study confirms these findings and provides real-world data regarding the higher death and MI risk in those with underlying CAD undergoing KT.
Patients with PAD and ESKD are also at a high risk of mortality and adverse cardiovascular events. Patients with PAD also derive a mortality benefit after KT. 18 In an analysis from the USRDS database (2004–2009), Brar et al. assessed the impact of underlying PAD on post-KT mortality. 19 They found a significantly higher mortality rate in those with PAD than those without (6.2% vs 3.0%). The mean follow-up duration was not specified. Our study confirms these findings and reports a higher incidence of mortality and CVA in these patients.
Polyvascular disease is highly prevalent in patients with DM and chronic kidney disease. It is associated with an even worse prognosis than those with CAD or PAD alone.3,20 There is no information in the literature that we could find that reports on outcomes after KT in these patients. In this study, we found that these patients have the worst outcomes in terms of mortality and MI after KT, even when compared to patients with advanced CAD or preexisting PAD and with a fourfold higher risk of MI when compared to those without CAD and PAD.
Our study reports similar graft survival (as defined by a return to dialysis or re-transplantation after 3 months of KT) in all groups without an impact of underlying CAD, PAD, or polyvascular disease. Although we did not find any prior studies that assessed graft survival in those with underlying CAD or polyvascular disease, there are prior studies that assessed graft survival in patients with underlying PAD. 19 In a USRDS study (2004–2009), Brar et al. reported a significantly higher incidence of graft failure in those with PAD than those without PAD (12.8% vs 6.3% at 3 years). This is discrepant from our findings, where we found no significant difference. This may be related to the definition of PAD as they only included those with symptomatic PAD as identified on the transplant candidate registration form rather than using ICD codes, such as in our study. Further, they included any return to dialysis in their definition of graft loss and may have inadvertently included patients who may have been on transient post-KT dialysis. Our study findings of similar graft failure rates in all patient cohorts are reassuring in this regard.
Study limitations
Our study results should be interpreted with an understanding of the limitations of an observational, administrative database study. Even though the USRDS data have been extensively reported and validated, it is subject to coding errors and unmeasured confounders. To reduce the likelihood of including patients who may have been erroneously coded as CAD, we included only patients with a history of coronary revascularization. Thus, these study results do not apply to patients who may have CAD but have not had prior revascularization procedures. Similarly, the diagnosis of PAD was identified through ICD codes, and information regarding ankle–brachial indices (ABIs) or symptomatology is unavailable. In addition, our study sample was limited to patients with primary Medicare coverage and the findings of this study may not be generalizable to the overall population. Since this is an administrative database study, it will benefit from external validation of these findings. However, it would likely need a large registry of patients with ESKD where information on PAD-specific tests such as ABIs or arterial duplex exam is available, including post-KT follow-up information of outcomes.
Given the paucity of current information from well-conducted clinical trials on the subject, our study provides clinically useful information for clinicians taking care of KT candidates and KT recipients with preexisting CVD.
Conclusions
This study found a significantly higher post-KT 3-year all-cause mortality in those with underlying CAD, PAD, or polyvascular disease (CAD + PAD), with polyvascular disease having worse outcomes than those without CAD or PAD. The risk of MI was several-folds higher in those with preexisting CAD or polyvascular disease. The risk of CVA was higher in those with PAD than in those without PAD.
The findings of this study are important for clinicians caring for patients with ESKD and underscore the significance of pre- and post-KT planning, prognosis assessment, and patient education. Our study also identifies these patients as a high-risk group who can benefit from the optimization of atherosclerotic risk factors before and after KT. Furthermore, these results provide strong support for the involvement of KT recipients in cardiovascular research, enhancing our comprehension of CVD management and impact on outcomes within this distinctive population. In addition, these outcomes advocate for the adoption of a multidisciplinary approach involving a collaborative ‘cardio-nephrology’ care team. Such an approach would mitigate care fragmentation, allowing for prioritized CVD screening and treatment among patients with high-risk CVD. These strategies collectively contribute to mitigating the impact of CVD among KT recipients, ultimately optimizing both long-term patient well-being and KT outcomes, all while maintaining cost-effectiveness.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231205574 – Supplemental material for Impact of preexisting coronary artery and peripheral artery disease on outcomes in diabetic patients after kidney transplant
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231205574 for Impact of preexisting coronary artery and peripheral artery disease on outcomes in diabetic patients after kidney transplant by Sania Jiwani, Wan-Chi Chan, Monil Majmundar, Kunal N Patel, Harsh Mehta, Aditya Sharma, Gaurav Parmar, Mark Wiley, Peter Tadros, Eric Hockstad, Sri G Yarlagadda, Aditi Gupta and Kamal Gupta in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the US government.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.