
Abstract

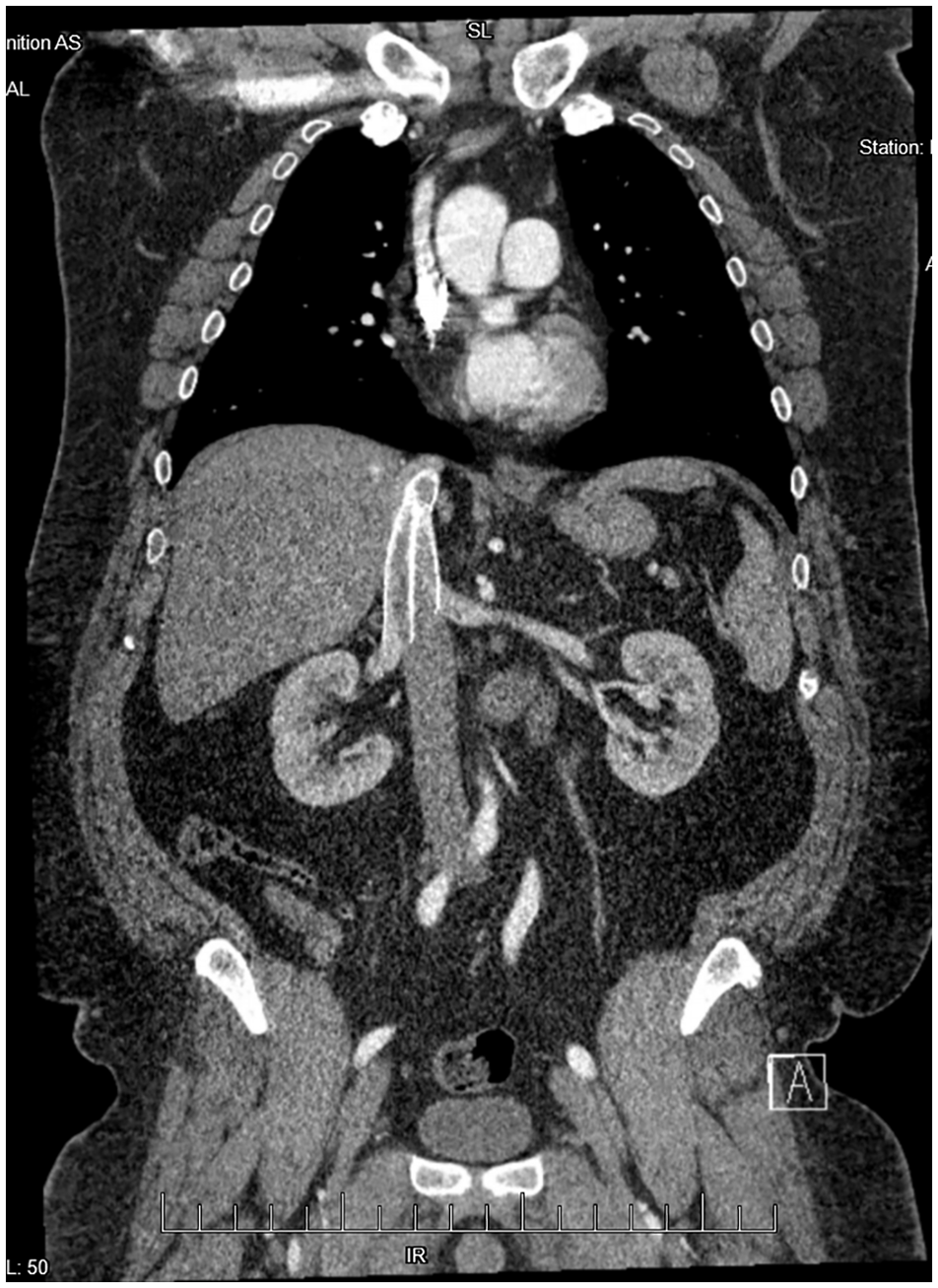
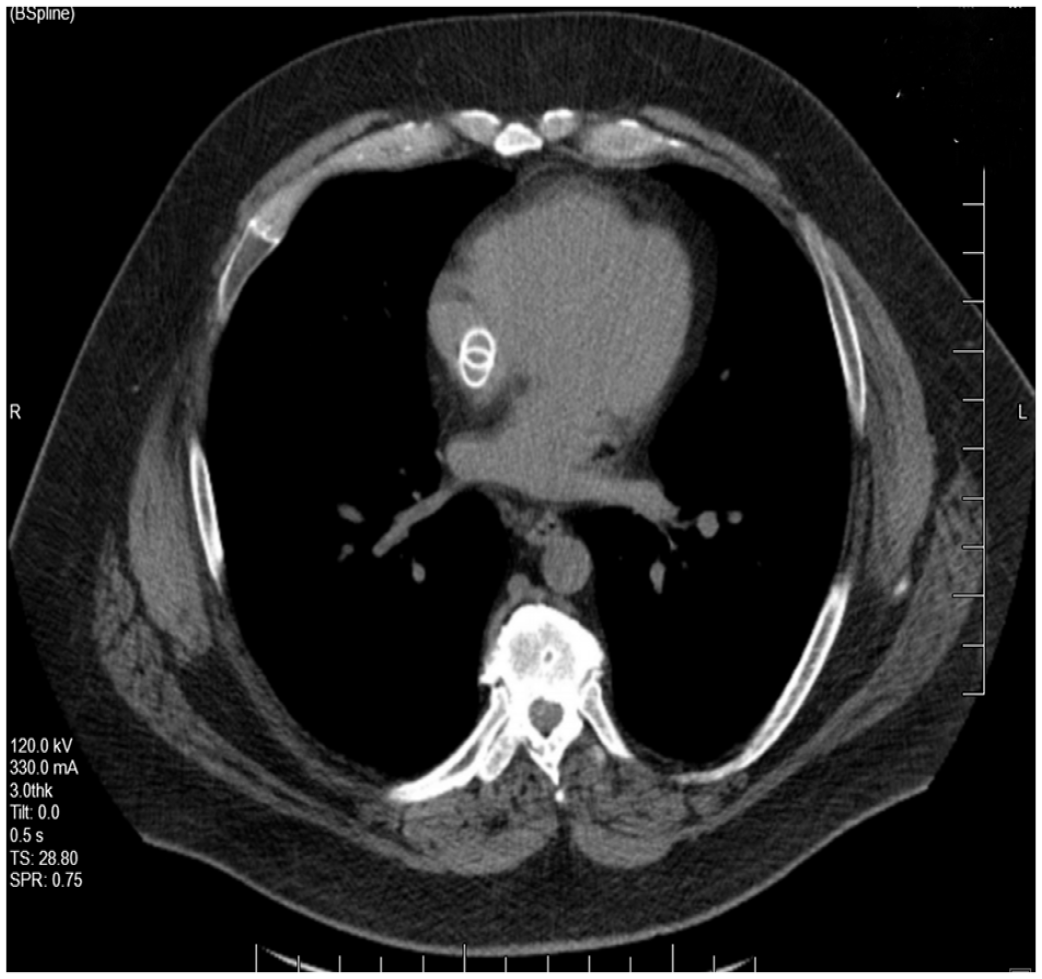
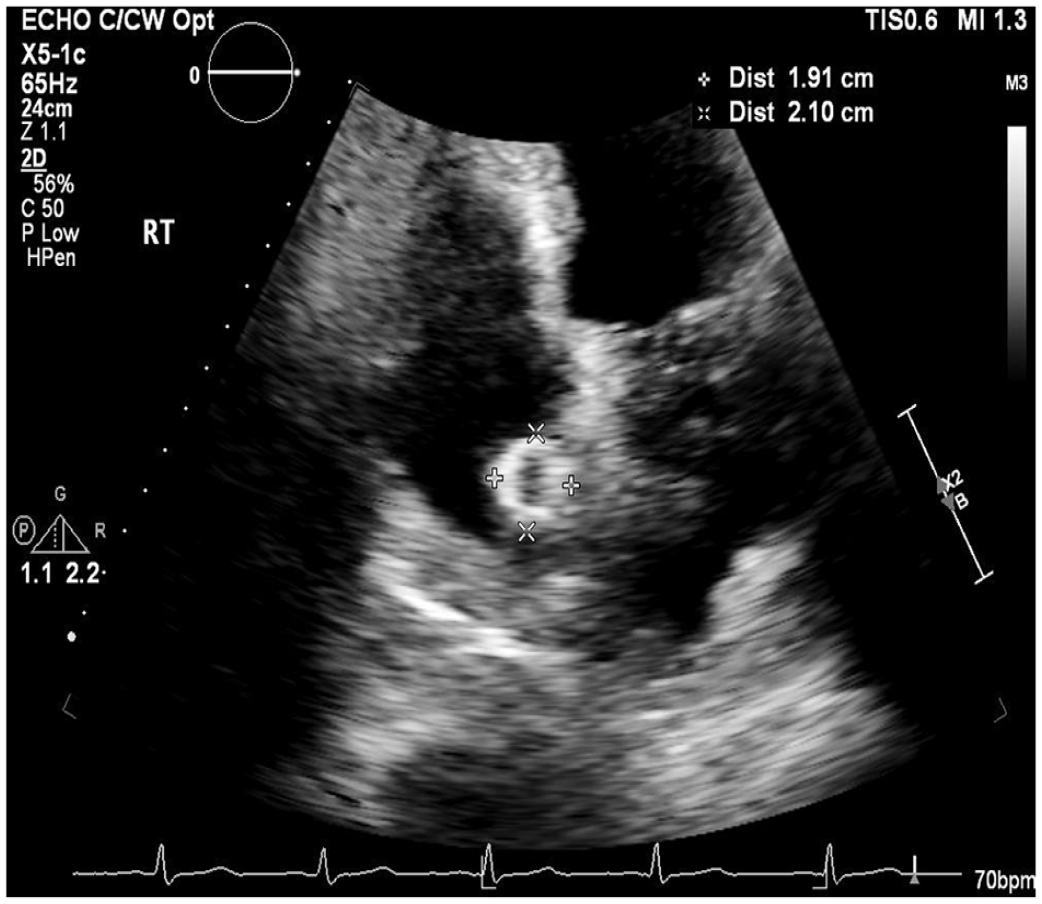
A 44-year-old man presented with bilateral leg edema with venous stasis ulcers at an outside facility 3 years prior to this presentation to us. At that time he underwent intravascular ultrasound-guided stenting of bilateral common and external iliac veins with a total of four 16-mm diameter venous (VICI®; Boston Scientific, Marlborough, MA, USA) stents (two on each side). He did well with complete healing of leg wounds and resolution of edema. At the current presentation, he had an abdominal X-ray and a noncontrast computed tomography (CT) scan to assess for a suspected ureteral stone that resulted in the incidental finding of migrated stents. Subsequent imaging with CT of chest abdomen and pelvis (Panels A, B, and C), as well as a transthoracic echocardiogram (Panel D and Video [online supplemental material]), showed migration of all four stents. Two stents had migrated into the right atrium and two into the suprarenal inferior vena cava. The double ring appearance seen in Panel C was likely caused by motion artifact due to non-gated CT. There was no evidence of stent thrombosis or soft tissue penetration. The echocardiogram was otherwise unremarkable without evidence of structural or functional abnormality. The patient was asymptomatic, and a rhythm monitor was normal.

A recent review compiled reports of 54 cases of venous stent migration. 1 Of those, 48% were from iliac veins. Stents less than < 14 mm diameter and length < 60 mm were more likely to migrate. A US Food and Drug Administration Manufacturer and User Facility Device Experience (MAUDE) database study found VICI stents to have 28 events of migration (48% of all device issues reported). 2 Optimal management of migrated stents is unclear and may depend on symptoms, location, and interval from implant. Stents have been reported to migrate to the right ventricle and pulmonary artery and may result in arrythmia, perforation, or valve disfunction. 3 In most cases, endovascular treatment has been shown to be successful, with a few requiring an open surgical approach. 1
Most migrated stents are discovered within a few months of placement. Sayed et al. only found one case of implant migration after 1 year of implant. 1
After a multidisciplinary team discussion, including with the patient, it was decided to pursue conservative management using anticoagulation with close clinical and imaging follow up for the time being. There was concern that since the stents were placed over 3 years ago, retrieval may result in tissue injury.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.