
Abstract
Background:
Non-Hispanic Black and Hispanic patients with symptomatic PAD may receive different treatments than White patients with symptomatic PAD. The delivery of guideline-directed medical treatment may be a modifiable upstream driver of race and ethnicity-related disparities in outcomes such as limb amputation. The purpose of our study was to investigate the prescription of preoperative antiplatelets and statins in producing disparities in the risk of amputation following revascularization for symptomatic peripheral artery disease (PAD).
Methods:
We used data from the Vascular Quality Initiative, a vascular procedure-based registry in the United States (2011–2018). We estimated the probability of preoperative antiplatelet and statin prescriptions and 1-year incidence of amputation. We then estimated the amputation risk difference between race/ethnicity groups that could be eliminated under a hypothetical intervention.
Results:
Across 100,579 revascularizations, the 1-year amputation risk was 2.5% (2.4%, 2.6%) in White patients, 5.3% (4.9%, 5.6%) in Black patients, and 5.3% (4.7%, 5.9%) in Hispanic patients. Black (57.5%) and Hispanic patients (58.7%) were only slightly less likely than White patients (60.9%) to receive antiplatelet and statin therapy. However, the effect of antiplatelets and statins was greater in Black and Hispanic patients such that, had all patients received these medications, the estimated risk difference comparing Black to White patients would have reduced by 8.9% (–2.9%, 21.9%) and the risk difference comparing Hispanic to White patients would have been reduced by 17.6% (–0.7%, 38.6%).
Conclusion:
Even though guideline-directed care appeared evenly distributed by race/ethnicity, increasing access to such care may decrease health care disparities in major limb amputation.
Keywords
Background
Peripheral artery disease (PAD) is a common atherosclerotic disorder that reduces blood flow to the lower extremities, leading to muscle pain, ischemic wounds that do not heal, and eventual tissue death. 1 Globally, more than 236 million people have PAD, with a disproportionate number living in low and middle income countries.2,3 Among the 8.5–12 million people estimated to have PAD in the United States, 4 the highest burden and worst prognosis following a PAD diagnosis are consistently observed in historically disadvantaged groups such as Black and Hispanic populations.5,6
Black people in the United States have a higher prevalence and incidence of PAD, 7 receive less preventive treatment, 8 and have worse limb-based outcomes 9 compared to White people. In addition, White patients with PAD are more likely than Black patients to have a revascularization (i.e., a limb-sparing procedure) attempt for their PAD rather than an amputation (i.e., limb-removing procedure). 10 Black patients with symptomatic PAD are four to five times more likely than White patients to undergo a PAD-related limb amputation.11,12 Though the incidence of PAD in Hispanic versus non-Hispanic White people may be similar,5,13 Hispanic people with PAD are under-prescribed cardiovascular medications 14 and have a higher incidence of chronic limb-threatening ischemia (CLTI; end-stage PAD) when hospitalized. 6 Hispanic patients are also more likely to receive a limb amputation compared to non-Hispanic White patients.15,16
Little is known about the uptake of PAD guidelines, particularly in diverse populations. We do know that when PAD guidelines are followed, outcomes for patients with PAD are improved.17 –19 As one potential explanation of the poor limb outcomes observed in Black and Hispanic patients, we hypothesized that guideline-directed preoperative management may be differentially administered across race/ethnicity groups and that differentially applied care may increase harm to already disadvantaged race/ethnicity groups.
Herein, we focused on one component of guideline-directed preoperative care for patients undergoing revascularization for PAD: the prescription of antiplatelets and statins prior to a revascularization procedure. We describe the prevalence of prescriptions of antiplatelets and statins; estimate the effect of prescribing antiplatelets and statins on subsequent risk of amputation stratified by race/ethnicity; and estimate the proportion of race/ethnicity-related disparities in major limb amputation following vascular intervention for PAD that could be eliminated through universal provision of preoperative antiplatelets and statins.
Methods
Database
The Society for Vascular Surgery (SVS) Patient Safety Organization established the Vascular Quality Initiative (VQI), a vascular procedure-based registry to document and improve the quality of care delivered to patients with vascular diseases. 20 A map of participating sites is included in the supplemental files (online supplementary Figure S1). During our study period, 5215 physicians at 536 health care centers were participating at centers including academic medical centers, teaching hospitals, community hospitals, and private practices.
A detailed description of the VQI registry has been previously published. 20 Briefly, trained data abstractors or clinicians input all data from each center into one of 14 major vascular procedure registries. Each registry contains information on patient demographic traits, comorbid conditions, imaging studies, medication usage, periprocedural details, and in-hospital and 30-day outcomes. Patients also complete a 1-year follow-up visit for any procedure covered by the VQI and outcome data are included in the registry.
Study sample
This study used data from adult (⩾ 18 years old) patients in the VQI registry who underwent a revascularization procedure from 2011 to 2018. We restricted our analysis to revascularization procedures indicated due to chronic PAD, including claudication (pain while walking) or CLTI (inadequate blood and oxygen supply resulting in ischemic pain at rest or tissue loss). The registries also capture patients treated for acute ischemia (15%), a different clinical etiology that is excluded from our analysis. The institutional review board of Clemson University determined the study met criteria for exemption because only deidentified data were used.
The unit of analysis for this study was an affected revascularized leg; individual patients could contribute two legs to this analysis. We included only the first procedure for the right and left legs of each patient. Patients of race-ethnicity other than non-Hispanic Black, non-Hispanic White, and Hispanic were also excluded. Hispanic ethnicity was defined as a person of Cuban, Mexican, Puerto Rican, South or Central American, or other Spanish culture or origin, regardless of race.
Outcome
The primary outcome was all-cause major amputation, defined as an amputation that occurred either below the knee or above the knee but excluding minor amputations of toes or trans-metatarsal or midfoot.
Guideline care measures
The major organizations that govern vascular care recommend that patients with PAD receive antiplatelet therapy and statin medications for secondary prevention and cardiovascular risk reduction. 21 Patients who took aspirin, or drugs that include aspirin, within 36 hours prior to surgery were classified as following antiplatelet therapy recommendations. Patients who received any of the HMG-CoA reductase inhibitors used to reduce cholesterol and stabilize atherosclerotic plaque within 36 hours prior to surgery were classified as following the recommendations for statin medications.
Demographics and comorbidities
All demographics and comorbidities were abstracted from the medical record at each participating center. Demographics included race, ethnicity, sex, and age at time of procedure (modeled as a quadratic). Insurance status was determined by the primary payer of the procedure and classified as uninsured (none, self-pay) or insured (Medicare, Medicaid, Commercial, Military/VA, non-US insurance). Smoking history was categorized as never or ever. Diabetes mellitus was defined as absent or present (whether controlled or uncontrolled). Chronic obstructive pulmonary disease (COPD) was categorized as absent, present and requires medication, or present and requires home oxygen. Hypertension was defined as documented history of blood pressure ⩾ 140 mmHg/90 mmHg on at least three occasions. Obesity was defined as having a body mass index ⩾ 30 kg/m2. Coronary artery disease was classified as present if there was any history of myocardial infarction, stable angina, or unstable angina. Congestive heart failure was defined according to the New York Heart Association Classification system 22 and classified as present if patients were asymptomatic with a positive history or symptomatic regardless of severity. Dialysis-dependence was defined as current use of hemo- or peritoneal dialysis. We categorized disease severity (indication for revascularization) as claudication or CLTI. Revascularization was classified as either (1) infrainguinal peripheral vascular intervention (PVI) including percutaneous catheter-based revascularization or (2) infrainguinal bypass.
Statistical analysis
We first compared the distribution of demographic characteristics and comorbidities of patients in our study sample across race/ethnicity groups. We then compared the crude probability of having a preoperative antiplatelet, a preoperative statin, and both antiplatelets and a statin, across race/ethnicity groups, in the entire sample and stratified by the indication for revascularization (CLTI or claudication).
We followed patients/limbs from revascularization until the first occurrence of major amputation, death (a competing event), or administrative censoring at 1 year. We report results based on the 30-day and 1-year cumulative incidence of major amputation, estimated using the Aalen–Johansen estimator. 23 For all analyses, we accounted for possible selection bias as a result of differential loss to follow-up with inverse probability of censoring weights conditional on all baseline covariates defined above and weeks since procedure. 24
To estimate whether the effect of guideline-directed provision of antiplatelets and statins differed by race/ethnicity, we estimated risk differences (RD) for having been prescribed both a preoperative antiplatelet and statin compared to only one or neither medication, stratified by race/ethnicity.
To estimate the impact of universal provision of preoperative antiplatelets and statins on racial/ethnic disparities, we used the framework described in Howe et al. 25 We first estimated the total association (‘total effect’ [TE]), although we do not interpret this association causally) between race/ethnicity and 30-day and 1-year cumulative incidence of major amputation comparing non-Hispanic Black and Hispanic patients with non-Hispanic White patients (the referent group). These estimates were only adjusted for possible selection bias due to nondifferential loss to follow-up with inverse probability of censoring weights.24,26
We next estimated the 30-day and 1-year risks of major amputation that we would expect to see if all patients had been prescribed preoperative antiplatelets and statins. To get these risks, we estimated the cumulative incidence function of amputation following revascularization procedures restricted to patients who received both a preoperative antiplatelet and statin, again stratified by race/ethnicity, and weighted the subsample who received both medications to represent the entire sample (whether or not they received either medication). We estimated these weights from generalized logistic models for the probability that both antiplatelets and statins were prescribed preoperatively, relative to one drug only, or neither drug, conditional on race/ethnicity and all covariates described above (race, ethnicity, sex, age, insurance, smoking history, diabetes mellitus, COPD, hypertension, obesity, coronary artery disease, congestive heart failure, and dialysis-dependence). We stabilized these weights on race/ethnicity. We call the RDs associated with race/ethnicity based on these risks the ‘controlled direct effect’ (CDE) of race on amputation under a hypothetical intervention to ensure a preoperative antiplatelet and statin was provided to all patients (although again, we do not interpret this association causally as an ‘effect’ of race).
The proportion of the racial/ethnic disparity eliminated (PE) under a hypothetical intervention to ensure a preoperative antiplatelet and statin was provided to all patients was estimated as (TE – CDE)/TE. Although we do not interpret the TE and CDE alone as an ‘effect’ of race, we can interpret the PE causally (again, as the effect of the hypothetical intervention on antiplatelet and statin prescription on the disparity) if we assume that we have measured all confounders of the effect of antiplatelets and statins on major amputation.
To account for uncertainty in the weights, and also possible correlation between major amputations for limbs belonging to the same individual, we estimated 95% CIs for all estimates described above by selecting the 2.5th and 97.5th percentiles from the distribution of such estimates from 500 bootstrap resamples of the data.
As a secondary analysis, we also estimated the PE in subpopulations of revascularization procedures that were indicated for claudication and CLTI.
Bootstrap resamples were conducted through the Palmetto Cluster for high performance computing at Clemson University. All analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Study population
We identified 100,579 revascularizations (limbs) among 88,599 patients. The median follow-up time was 365 days (84% of limbs were followed for a full year). There were 15,442 Non-Hispanic Black patients (17%), and 5506 Hispanic patients (6%). Diabetes (54%) and hypertension (89%) were the most prevalent comorbidities and were more prevalent in Black and Hispanic patients than non-Hispanic White patients, as was dialysis dependency, whereas White patients were more likely to have COPD (Table 1).
Characteristics of patients a who underwent revascularization for peripheral artery disease, stratified by race/ethnicity.
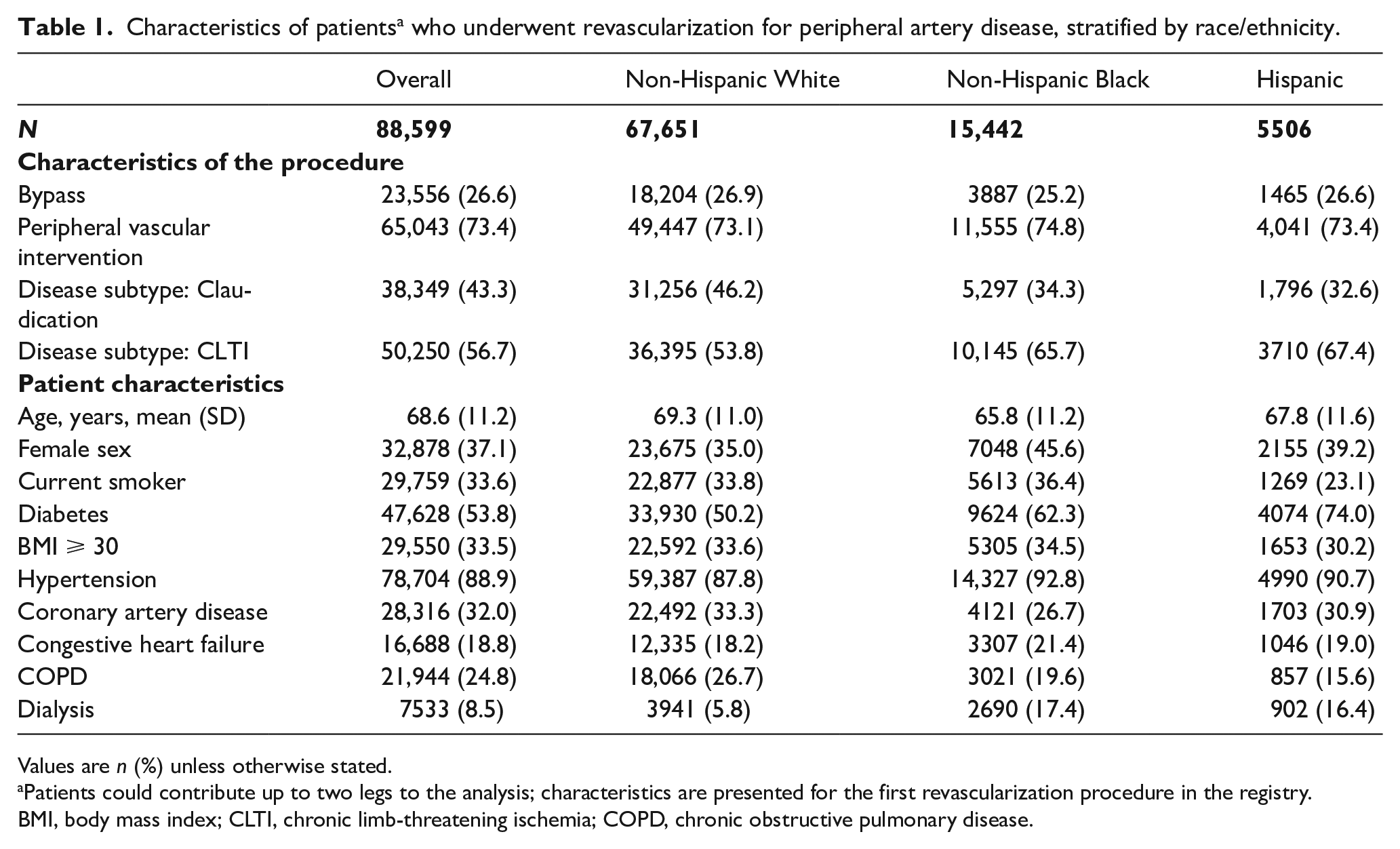
Values are n (%) unless otherwise stated.
Patients could contribute up to two legs to the analysis; characteristics are presented for the first revascularization procedure in the registry.
BMI, body mass index; CLTI, chronic limb-threatening ischemia; COPD, chronic obstructive pulmonary disease.
The cumulative incidence of limb amputation among non-Hispanic White patients was 2.5% (95% CI: 2.4, 2.6) at 1 year (adjusted only for loss to follow-up). Non-Hispanic Black patients and Hispanic patients had higher cumulative incidence rates of amputation than non-Hispanic White patients at 1 year, 5.3% (95% CI: 4.9, 5.6) and 5.3% (95% CI: 4.7, 5.9), respectively.
Prescription patterns
Patients received preoperative antiplatelet and statin medications before 60.2% of revascularizations. The proportion of revascularizations with a preoperative antiplatelet and statin was slightly higher for non-Hispanic White patients (60.9%) than for non-Hispanic Black patients (57.5%) and Hispanic patients (58.7%). These patterns held true across disease subtypes of CLTI and claudication (Table 2).
Presence of guideline-recommended medication prescriptions, statified by race/ethnicity and disease subtype.
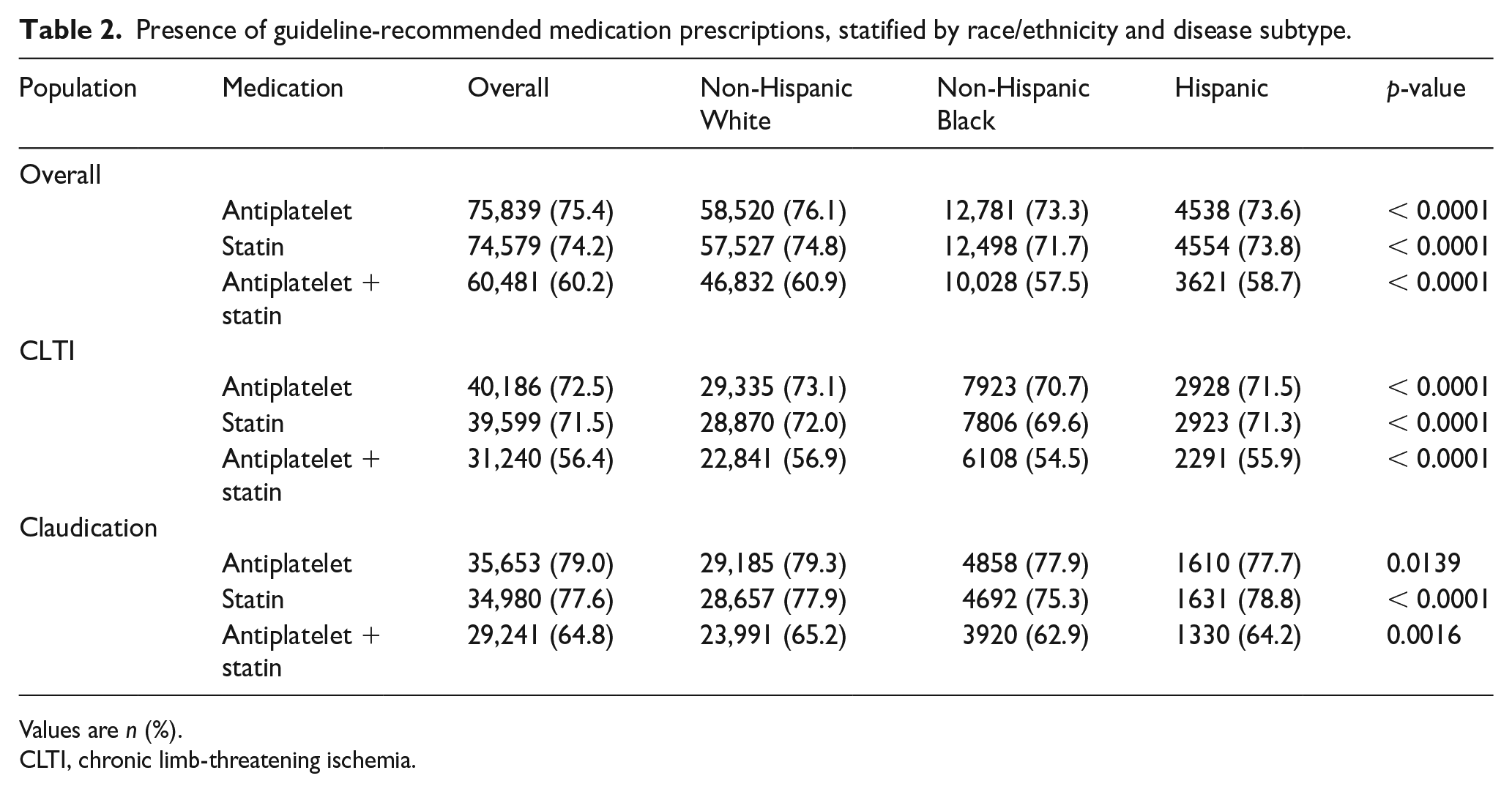
Values are n (%).
CLTI, chronic limb-threatening ischemia.
Impact of preoperative antiplatelet and statin
In comparing amputation for those receiving a preoperative prescription of antiplatelet + statin versus neither across race/ethnicity groups, the risk of amputation at 1 year was reduced among all groups. However, the reduction in amputation risk was more pronounced in Black (RD: 2.2%; 95% CI: 0.7, 3.8) and Hispanic (RD: 1.9%; 95% CI: –0.3, 4.2) patients compared to White (RD: 0.5%; 95% CI: −0.0, 0.9) patients (Table 3).
Standardized a cumulative incidence and risk differences for major amputation associated with preoperative (within 36 h) antiplatelet and statin nonuse versus use, stratified by race/ethnicity groups.
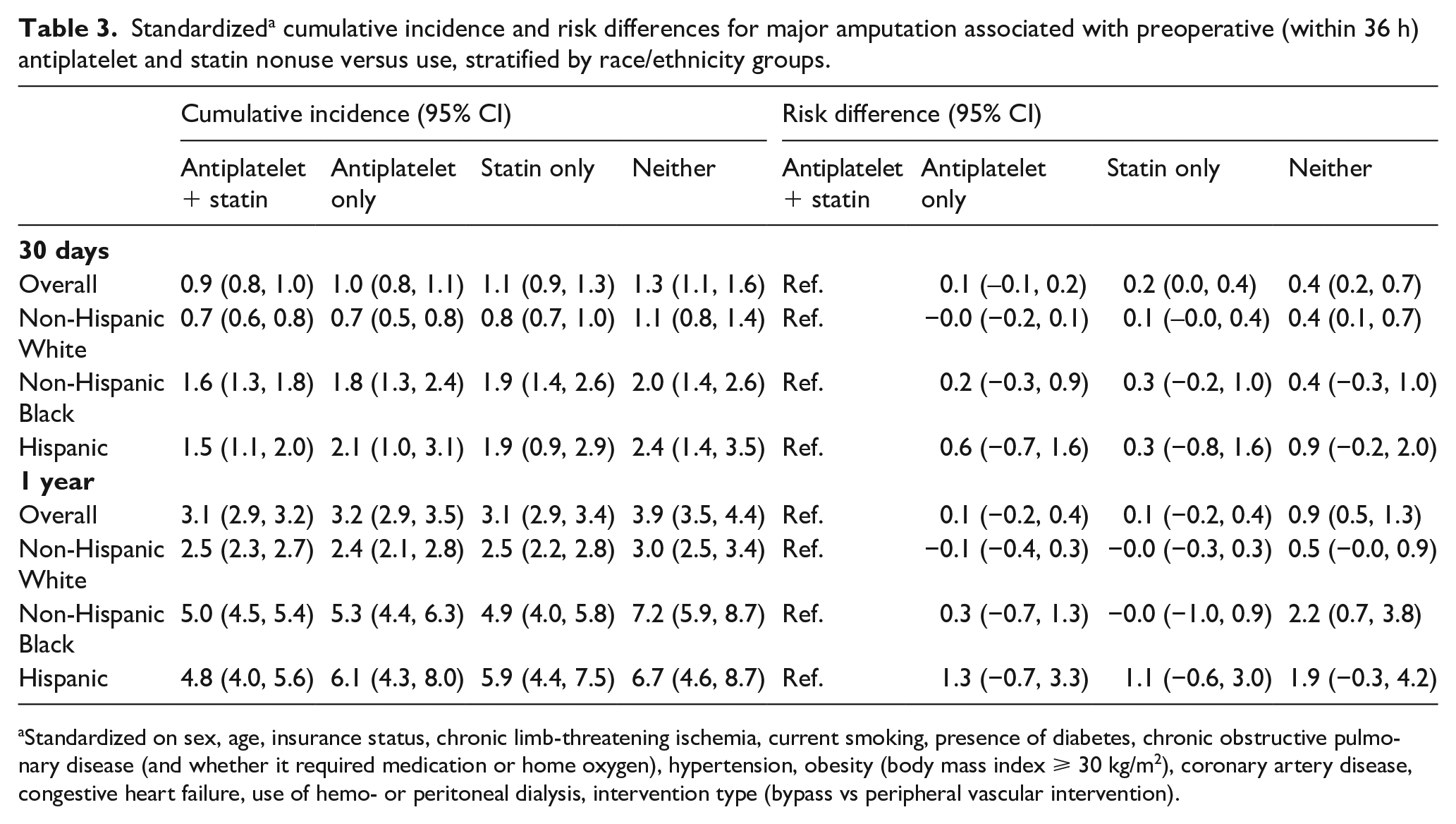
Standardized on sex, age, insurance status, chronic limb-threatening ischemia, current smoking, presence of diabetes, chronic obstructive pulmonary disease (and whether it required medication or home oxygen), hypertension, obesity (body mass index ⩾ 30 kg/m2), coronary artery disease, congestive heart failure, use of hemo- or peritoneal dialysis, intervention type (bypass vs peripheral vascular intervention).
Impact of antiplatelet and statin on racial disparities
Had all patients received the appropriate preoperative medication, the amputation risk would have been lower across all three race/ethnicity groups at both 30 days and 1 year (Table 3). Compared to non-Hispanic White patients, the proportion of disparities that could be eliminated (i.e., the percent reduction in the risk difference observed under no intervention) for non-Hispanic Black patients was 8.9% (95% CI: –2.9, 21.9) at 1 year. For Hispanic patients, the proportion of disparities eliminated compared to non-Hispanic White patients was 17.6% (95% CI: –0.7, 38.6) at 1 year (Table 4).
Cumulative incidence and racial/ethnic disparities of major amputations before and after a hypothetical intervention to ensure universal preoperative (within 36 h) antiplatelet and statin use.
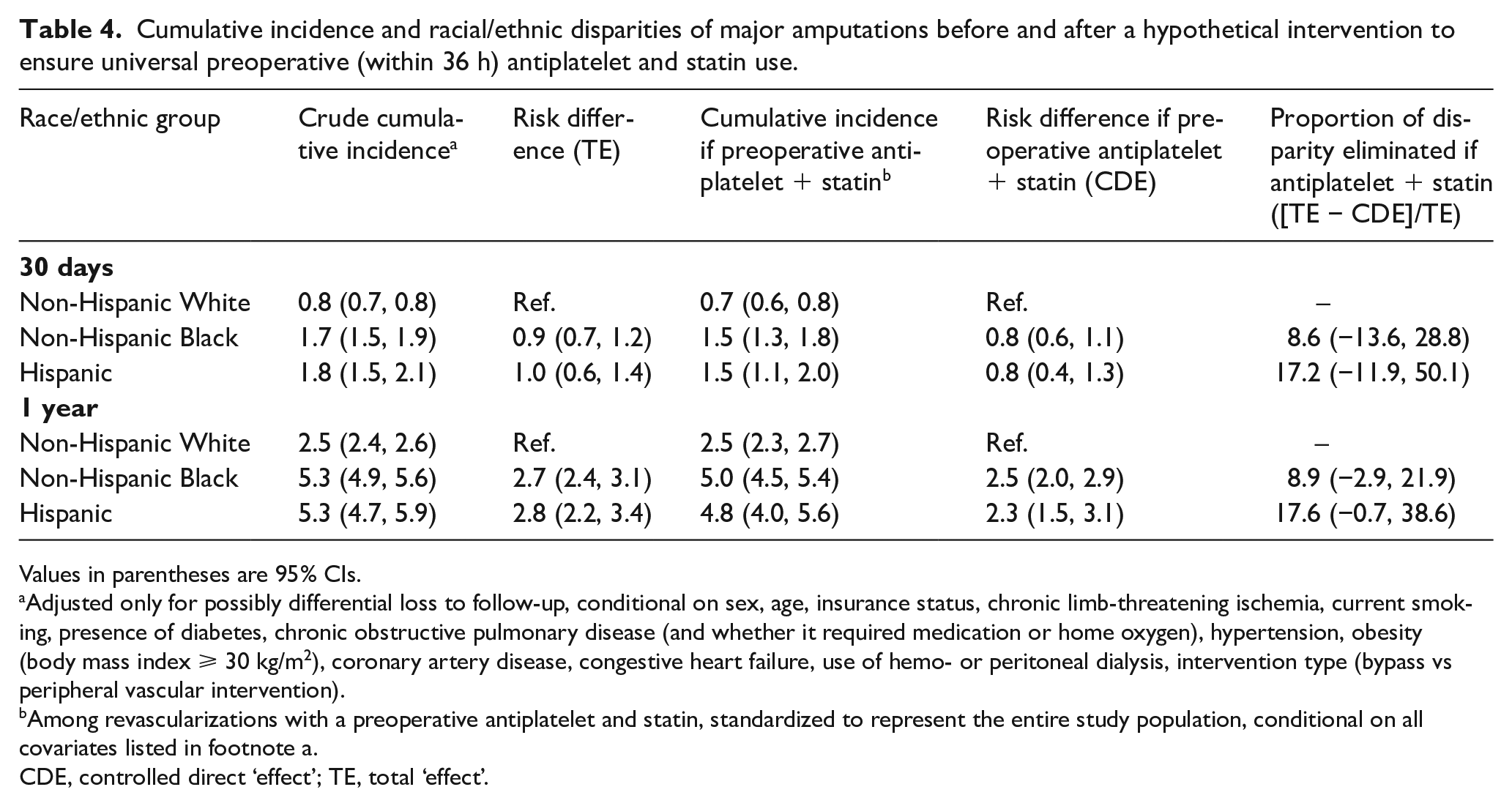
Values in parentheses are 95% CIs.
Adjusted only for possibly differential loss to follow-up, conditional on sex, age, insurance status, chronic limb-threatening ischemia, current smoking, presence of diabetes, chronic obstructive pulmonary disease (and whether it required medication or home oxygen), hypertension, obesity (body mass index ⩾ 30 kg/m2), coronary artery disease, congestive heart failure, use of hemo- or peritoneal dialysis, intervention type (bypass vs peripheral vascular intervention).
Among revascularizations with a preoperative antiplatelet and statin, standardized to represent the entire study population, conditional on all covariates listed in footnote a.
CDE, controlled direct ‘effect’; TE, total ‘effect’.
Revascularizations for CLTI
During our study, 55,451 limbs in 50,250 patients were treated with revascularization for CLTI. The 1-year risk of major amputation was 4.3% (95% CI: 4.1, 4.5) in non-Hispanic White patients, 7.6% (95% CI: 7.0, 8.1) in non-Hispanic Black patients, and 7.6% (95% CI: 6.8, 8.4) in Hispanic patients. We estimated that universal preoperative antiplatelet and statins would have reduced the disparity gap for non-Hispanic Black patients compared to non-Hispanic White patients by 7% (95% CI: –11, 23) at 1 year; disparities in amputation risk for Hispanic patients compared to non-Hispanic White patients would have been reduced by 22% (95% CI: –1, 46) at 1 year (Table 5).
Cumulative incidence and racial/ethnic disparities of major amputations before and after a hypothetical intervention to ensure universal preoperative (within 36 h) antiplatelet and statin use for chronic limb-threatening ischemia.
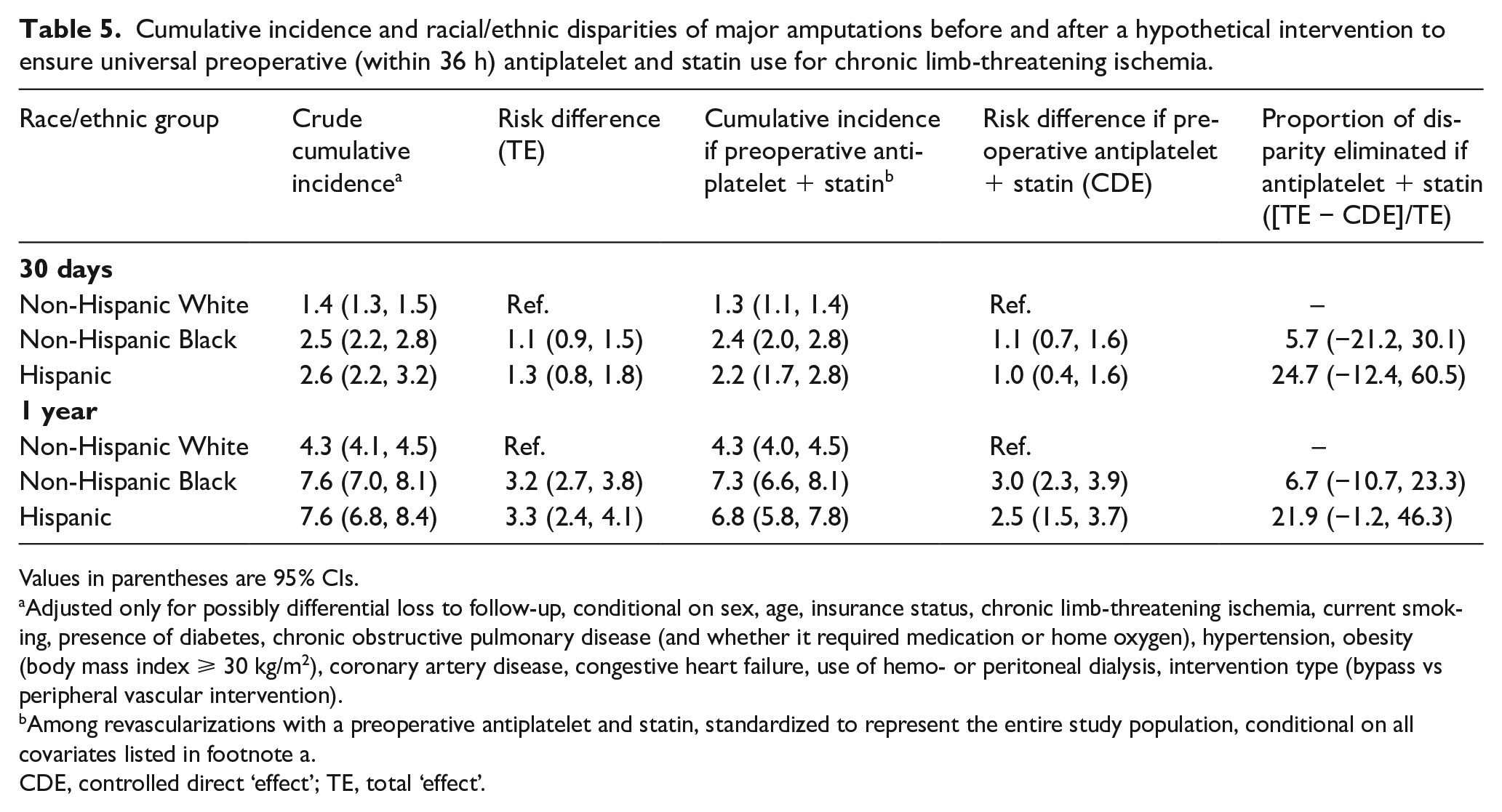
Values in parentheses are 95% CIs.
Adjusted only for possibly differential loss to follow-up, conditional on sex, age, insurance status, chronic limb-threatening ischemia, current smoking, presence of diabetes, chronic obstructive pulmonary disease (and whether it required medication or home oxygen), hypertension, obesity (body mass index ⩾ 30 kg/m2), coronary artery disease, congestive heart failure, use of hemo- or peritoneal dialysis, intervention type (bypass vs peripheral vascular intervention).
Among revascularizations with a preoperative antiplatelet and statin, standardized to represent the entire study population, conditional on all covariates listed in footnote a.
CDE, controlled direct ‘effect’; TE, total ‘effect’.
Revascularizations for claudication
During our study, 45,128 limbs in 38,349 patients were treated with revascularization for claudication. The 1-year risk of amputation for non-Hispanic Black patients (1.1%; 95% CI: 0.8, 1.4) was higher than for non-Hispanic White patients (0.6%; 95% CI: 0.5, 0.6); the 1-year risk for Hispanic patients was 0.9% (95% CI: 0.5, 1.3). We estimated that the proportion of racial/ethnic disparities eliminated by preoperative antiplatelet and statin would be 73% (95% CI: 39, 139) for non-Hispanic Black patients and 47% (95% CI: –315, 502) for Hispanic patients (Table 6).
Cumulative incidence and racial/ethnic disparities of major amputations before and after a hypothetical intervention to ensure universal preoperative (within 36 h) antiplatelet and statin use for claudication.
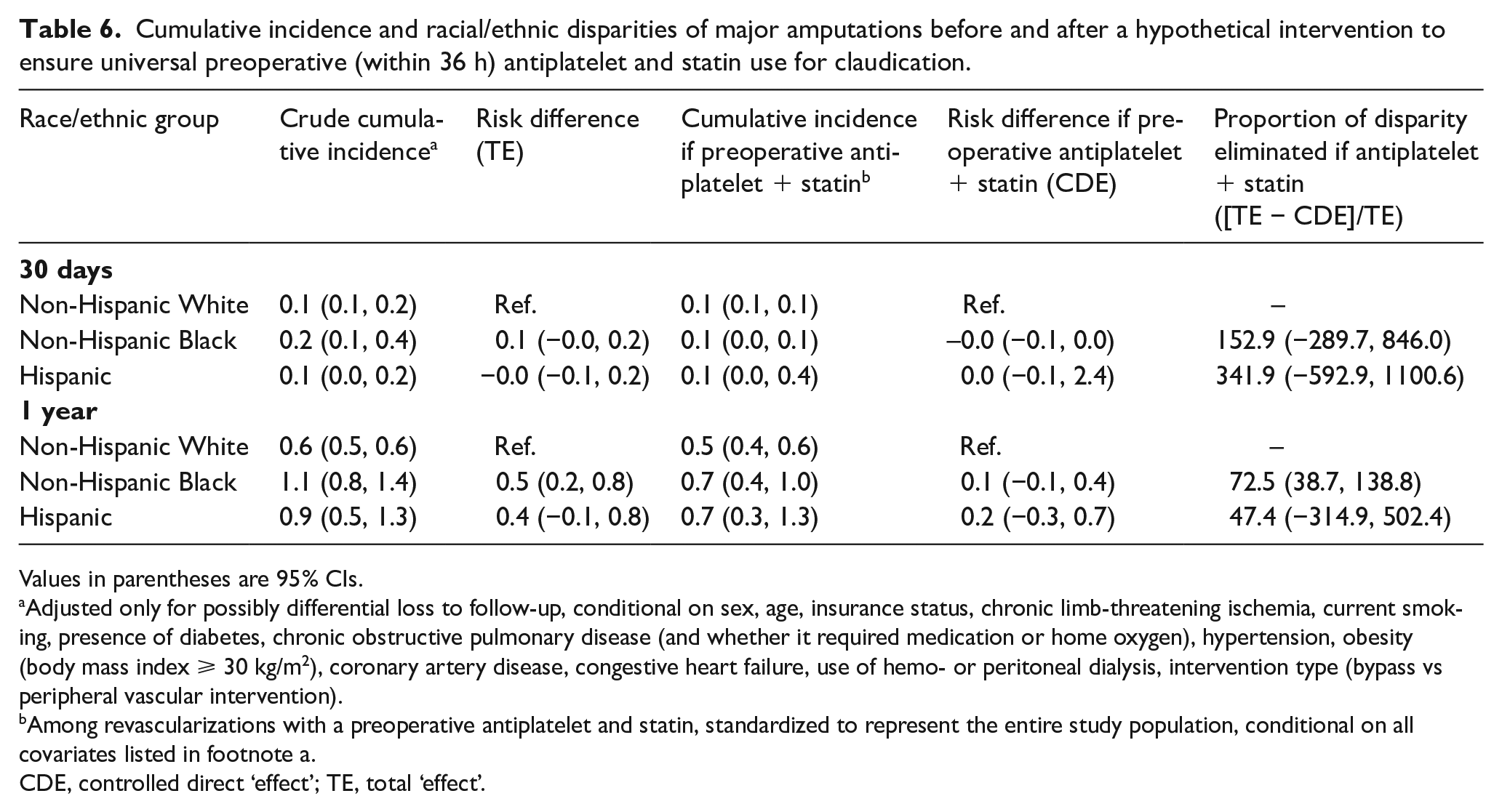
Values in parentheses are 95% CIs.
Adjusted only for possibly differential loss to follow-up, conditional on sex, age, insurance status, chronic limb-threatening ischemia, current smoking, presence of diabetes, chronic obstructive pulmonary disease (and whether it required medication or home oxygen), hypertension, obesity (body mass index ⩾ 30 kg/m2), coronary artery disease, congestive heart failure, use of hemo- or peritoneal dialysis, intervention type (bypass vs peripheral vascular intervention).
Among revascularizations with a preoperative antiplatelet and statin, standardized to represent the entire study population, conditional on all covariates listed in footnote a.
CDE, controlled direct ‘effect’; TE, total ‘effect’.
Discussion
Among patients treated with infrainguinal revascularization for symptomatic PAD, Black and Hispanic patients had a 1-year risk of amputation approximately two times the risk among non-Hispanic White patients. As one potential explanation for disparities in amputation risk, we investigated the role of suboptimal prescription of preoperative antiplatelet and statins. We found that only 60% of patients had been prescribed preoperative antiplatelet and statin medications. We found only minimal differences in the prescription of these medications across race/ethnicity. However, we found the effect of antiplatelets and statins was greater in Black and Hispanic patients such that, had all patients received the appropriate guideline-directed medications, (1) the risk of amputation would have been lower for all patients and (2) a significant portion of the disparities in outcomes experienced by Black and Hispanic patients relative to White patients would have been eliminated. Our analyses suggest an actionable way to reduce the major limb amputation disparities that have been documented for decades.
We estimated the largest proportion of disparities could be eliminated by properly administering antiplatelet and statin medications to patients with claudication, a supposedly nonlimb-threatening condition. First-line therapy for claudication should be cardiovascular risk reduction with medical therapy and revascularization procedures should be reserved for those with very short distance claudication who have failed noninterventional management, including supervised exercise therapy to improve walking distances. More research is needed into why all patients, and especially Black and Hispanic patients, are not treated with best medical practices when they present for a revascularization procedure. It will also be important to study the circumstances that cause these individuals to be referred for vascular specialty care and to increase awareness of claudication in primary care settings where antiplatelet and statin medication could be initially prescribed.
Although differences in the overall low rate of a preoperative antiplatelet and statin across our three race/ethnicity groups were minimal, Black and Hispanic patients did have a lower prevalence of antiplatelet and statin use. This finding of poor care aligns with literature on diseases such as lung cancer, where Black women have been shown to have less access to screening and early-stage surgery. 27 However, the difference in antiplatelet and statin prescription prevalence across race/ethnicity groups is not enough to account for the reductions in disparities we predicted if antiplatelet and statin prescription prevalence was increased to 100% for all groups. Although our method did not require us to estimate the effect of antiplatelet and statin medications directly, we can infer that Black and Hispanic patients experience a greater benefit from antiplatelet and statin prescription compared to White patients, perhaps because of the prevalence of other comorbidities pertinent for PAD such as diabetes and dialysis.
To explain higher rates of amputation in Black patients, some studies have suggested that Black patients have a genetic predisposition to PAD and present at advanced stages with more anatomically complex disease.28,29 History tells us that most of the time that racial disparities in health outcomes are hypothesized to be due to ‘genes,’ better explanations rooted in systemic racism emerge. Worse, a quest for an explanation that blames the patient either indirectly (by faulting their genes) or directly (by suggesting they seek care late) ignores the role of systemic racism in determining whether they develop PAD (e.g., access to a healthy diet and safe spaces and leisure time for exercise, access to earlier medical therapy), when they present for care, how quickly their condition is diagnosed, what primary and secondary preventive care is available to them, and (the intervention of next-to-last-resort) the circumstances under which they receive vascular intervention for symptomatic PAD. Additionally, as in other conditions where pain is the primary symptom,30,31 it is possible that the severity of claudication is underestimated in Black and Hispanic patients, and they are not referred until their claudication is more severe than in White patients. Although we describe a potential opportunity to reduce health disparities by increasing the prescription and uptake of antiplatelets and statins among patients undergoing a revascularization procedure, limiting ourselves to interventions at such late stages of PAD care will always fall short of eliminating health disparities. However, the point at which patients present for vascular surgery represents an inflection point where we have an opportunity, at the very least, not to further propagate disparities.
There are other ACC/AHA Class I recommendations that define best practices for medical management, imaging methods to assess anatomy, and specific operative techniques. We found that provision of a preoperative antiplatelet and statin may reduce amputation disparities. Optimized management of hypertension, diabetes, and smoking represent other critical areas of preventive care that should be explored. Assuming our estimate for the proportion of disparities reduced by universal uptake of preoperative antiplatelet/statin was correct, small incremental differences in each measure of optimized care may lead to the major disparities we see in outcomes.
Limitations
Our results are limited to patients who underwent lower-extremity revascularization for symptomatic PAD. There are selection processes that drive the patient population who were eligible for this study; for example, access to health care for diagnosis of PAD and initial revascularization surgery. These selection processes are associated with race and ethnicity, such that Black and Hispanic patients who undergo revascularization may be a healthier subset of all disadvantaged patients who would be eligible for this procedure, as compared to White patients. There also remains the possibility that being prescribed these medications is a marker of being treated by ‘better’ vascular providers whose patients have better outcomes (i.e., the provider is the source of the outcome disparity rather than effects of the medication). If these selection-related disparities were remedied early in the prevention and treatment pathways, we might hypothesize that the observed disparities after revascularization would be more dramatically reduced (even prior to additional interventions such as increasing adherence to guideline-directed care).
Registry information is updated manually and is subject to human error. The VQI registry was not designed specifically for research purposes and follow-up past 1 year is limited. The registry does not include information on the timing of medication initiation or dosage of medications. If there are important differences in the effects of antiplatelets and statins based on how long prior to revascularization they were prescribed, we have averaged over them and our estimate of the impact that prescription of antiplatelets and statins within 2 days of surgery would have on amputation outcomes. We are also limited in that this is an observational study and the validity of our results rests on the assumption that we have measured and accounted for all confounders of the effect of antiplatelets and statins on major amputation, although we have adjusted for a robust set of covariates. However, we report longer-term outcomes (1 year) than many previous publications. Additionally, the VQI is a ‘real world’ data source that provides a view of current outcomes in a large population of patients undergoing lower-extremity revascularization procedures for symptomatic PAD in both tertiary and community hospitals. Thus, our results are likely more generalizable to PAD patients undergoing revascularization in the United States than prior reports.
Conclusion
There are a range of patient, physician, and health care system factors that impact the provision of cardiovascular care. 32 Our study examined one facet of this conceptual model. We found that a substantial proportion of patients in this study did not receive guideline-directed medications prior to their revascularization attempt. We are not the first to find that uptake of optimal medical care is low among patients with PAD 33 or that nonoptimized medical care is connected to poor outcomes.18,34 However, our study quantifies the potential impact that lack of adherence to guideline-directed medication provision might have had on amputation disparities. Adherence to recommendations for the prescription of antiplatelet and statin medication, an ACC/AHA Class I recommendation, would improve outcomes for all patients with PAD. We have also demonstrated its potential to close outcome gaps for vascular patients from disadvantaged racial/ethnic groups.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X231196139 – Supplemental material for Investigating the impact of suboptimal prescription of preoperative antiplatelets and statins on race and ethnicity-related disparities in major limb amputation
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X231196139 for Investigating the impact of suboptimal prescription of preoperative antiplatelets and statins on race and ethnicity-related disparities in major limb amputation by Corey A Kalbaugh, Brian Witrick, Kerry A Howard, Laksika Banu Sivaraj, Katharine L McGinigle, William P Robinson, Samuel Cykert, Caitlin W Hicks and Catherine R Lesko in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Corey A Kalbaugh received a Career Development Award from the American Heart Association (19CDA34760135) and National Institute of Health/National Heart Lung and Blood Institute (K01HL146900).
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.