
Abstract
A 55-year-old woman presented with a 9-month history of progressively painful, disabling bilateral leg and foot swelling. Her medical history was essentially unremarkable with the exception of longstanding lichen planus and an ongoing 25 pack-year history of tobacco use. She was not taking any edematogenic medications.
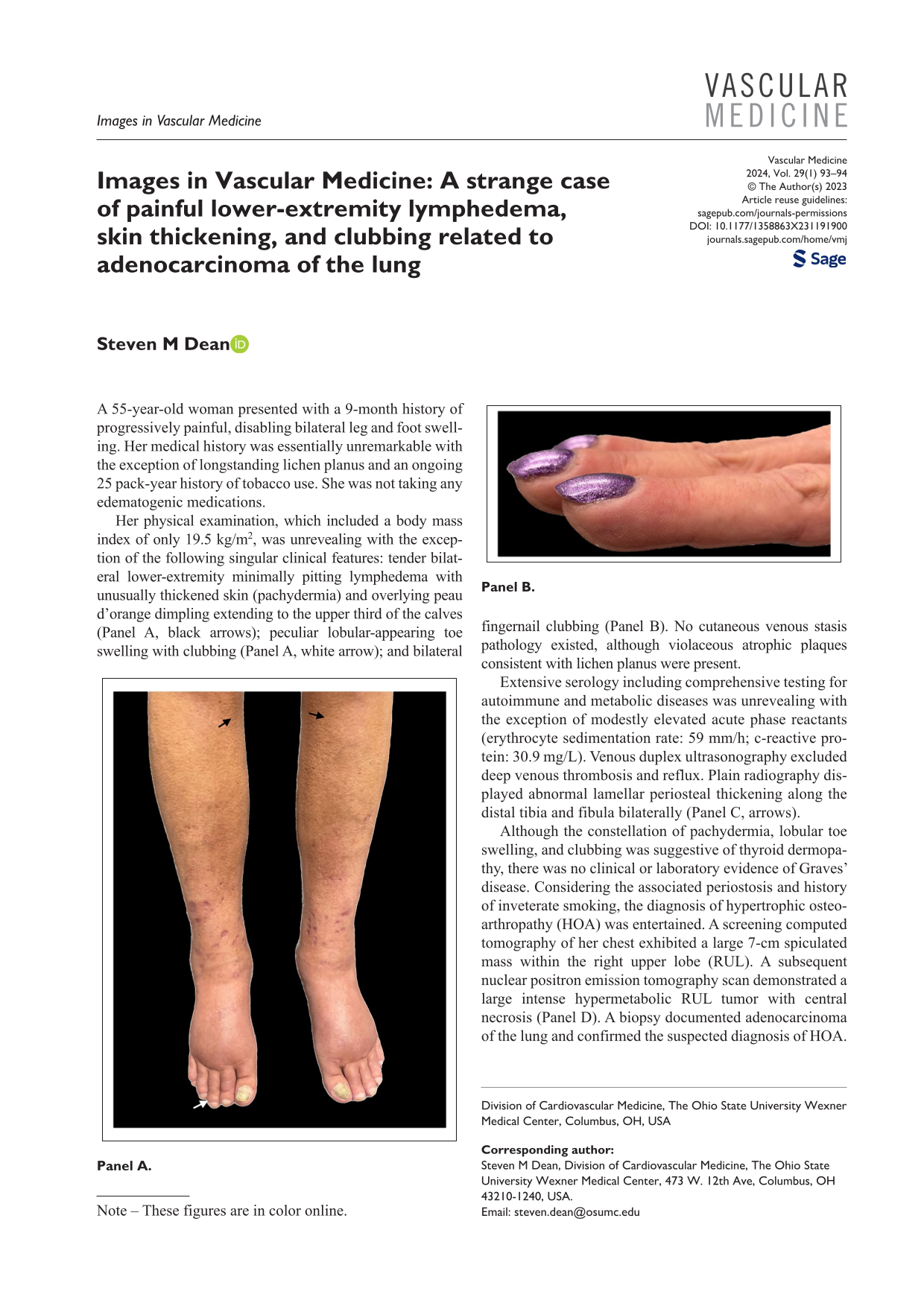
Her physical examination, which included a body mass index of only 19.5 kg/m2, was unrevealing with the exception of the following singular clinical features: tender bilateral lower-extremity minimally pitting lymphedema with unusually thickened skin (pachydermia) and overlying peau d’orange dimpling extending to the upper third of the calves (Panel A, black arrows); peculiar lobular-appearing toe swelling with clubbing (Panel A, white arrow); and bilateral fingernail clubbing (Panel B). No cutaneous venous stasis pathology existed, although violaceous atrophic plaques consistent with lichen planus were present.


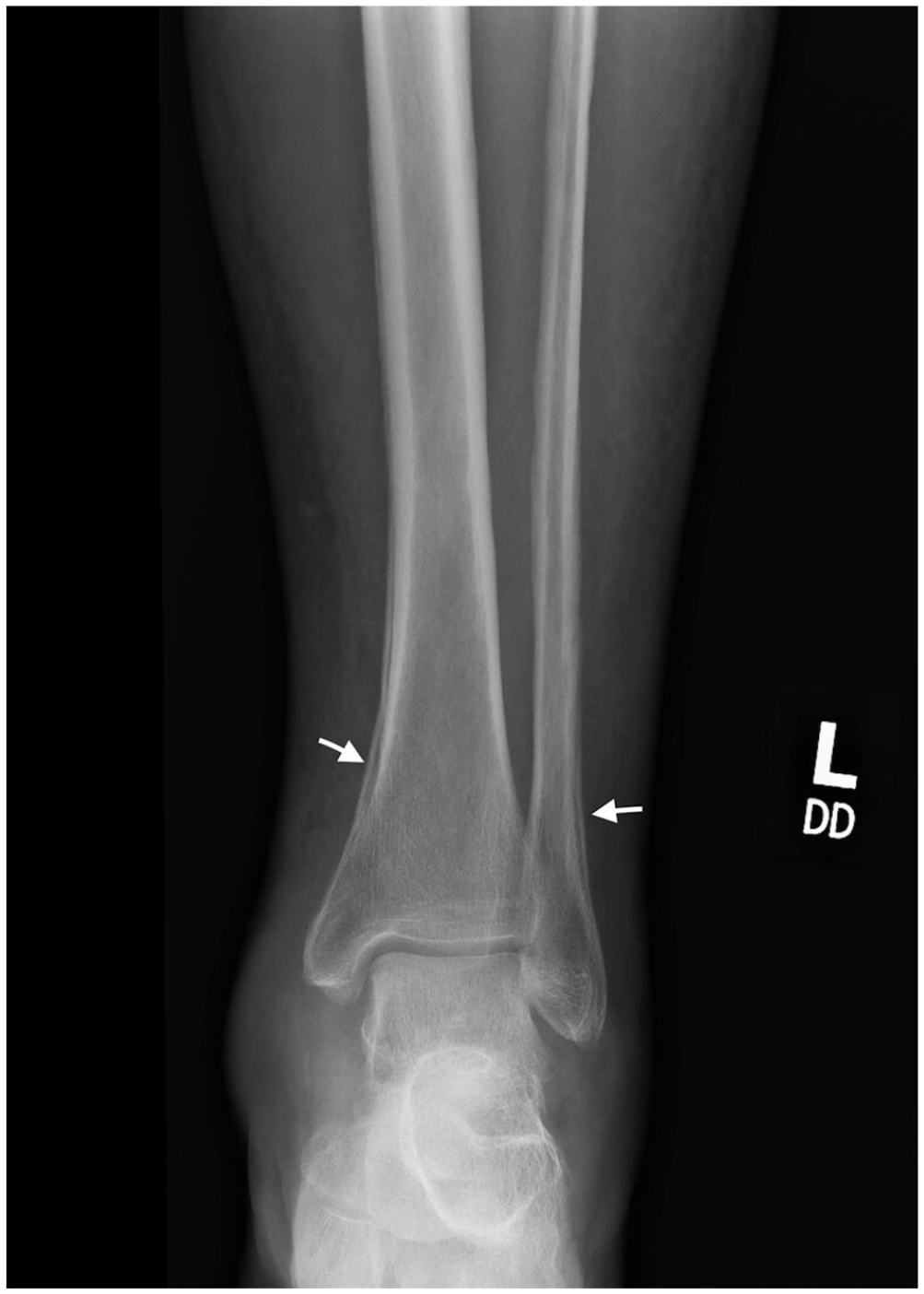
Extensive serology including comprehensive testing for autoimmune and metabolic diseases was unrevealing with the exception of modestly elevated acute phase reactants (erythrocyte sedimentation rate: 59 mm/h; c-reactive protein: 30.9 mg/L). Venous duplex ultrasonography excluded deep venous thrombosis and reflux. Plain radiography displayed abnormal lamellar periosteal thickening along the distal tibia and fibula bilaterally (Panel C, arrows).
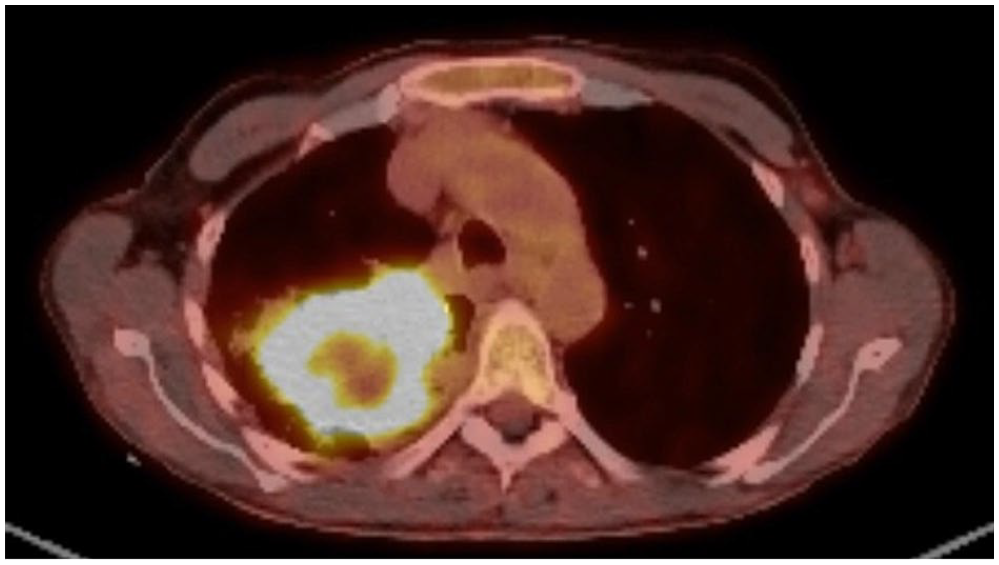
Although the constellation of pachydermia, lobular toe swelling, and clubbing was suggestive of thyroid dermopathy, there was no clinical or laboratory evidence of Graves’ disease. Considering the associated periostosis and history of inveterate smoking, the diagnosis of hypertrophic osteoarthropathy (HOA) was entertained. A screening computed tomography of her chest exhibited a large 7-cm spiculated mass within the right upper lobe (RUL). A subsequent nuclear positron emission tomography scan demonstrated a large intense hypermetabolic RUL tumor with central necrosis (Panel D). A biopsy documented adenocarcinoma of the lung and confirmed the suspected diagnosis of HOA. With an ongoing regimen of chemoradiation and celecoxib, her painful lymphedema has modestly improved.
HOA is syndrome of digital clubbing, pachydermia, and symmetric periostosis with painful joint and/or leg swelling. Although it is associated with a multitude of diverse etiologies, 90% of cases in adults are due to malignancy. 1 Similar to this case, nonsmall cell lung cancer, especially adenocarcinoma, is the most common cause of HOA. 2 The pathogenesis is believed to be humoral with elevated prostaglandin E2, vascular endothelial growth factor, and/or mechanical with fragmented megakaryocytes and platelets that interact with peripheral endothelial cells. 3 The diagnosis is clinical and supplemented with plain radiography, bone scintigraphy, and magnetic resonance imaging. The most effective therapy involves treating the underlying etiology, although COX-2 inhibitors and bisphosphonates have also demonstrated benefit. 4
Footnotes
Note – These figures are in color online.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.